Embed Size (px)
Citation preview

Fisiopatologia Respiratoria e Disturbi nel Sonno: proposta di
rete
Antonio ForesiDirettore
U.O.C. di Pneumologia e Fisiopatologia RespiratoriaPresidio Ospedaliero di Sesto San Giovanni
@AForesi 1

full hub/spoke/satellite service
@AForesi 2
@AForesi 3

Specialità Strutture di degenza Servizi senza posti letto
Bacino Max Min*
Bacino Max Min*
Pneumologia 0,8 0,4 ? ?
* (x milioni di abitanti)
Bozza Decreto su “Definizione degli standard qualitatitivi, strutturali, tecnologici, e quantitativi relativi all’assistenza ospedaliera…” 9 Luglio 2014
@AForesi 4

Sleep Medicine is a very prevalent disorders with effective treatments that change patients lives
Sleep Unit with polisomnograpy needs higly specialised personnel and complicated
technology. Sleep technology is a rapidly growing, advancing, and evolving field
Sleep Medicine is chronic care management discipline, not a diagnostic one
@AForesi 5

@AForesi 6

Classification of Sleep Disorders - ICSD-2
Thorpy MJ - Neurotherapeutics (2012) 9:687–701@AForesi 7

Patologie sonno-correlate di maggiore interesse pneumologico
• OSA(S)• BPCO• Overlap syndrome • Apnee centrali• CSR-CSA• S. obesità-ipoventilazione (OHS)• DRS in corso di patologie neuromuscolari o
restrittive toraciche
@AForesi 8

Functions and obligations of primary care and sleep units with respect to the handling of patients with OSA, or suspected of having OSA
Martínez-García M.A. – Breathe Review 2010
@AForesi 9

Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 10

risk factors commonly associated with OSA: obesity, gender (more common in men than women), age (more common in older age), hypertension and diabetes.
@AForesi 11

Percent of UK hospitals delivering each service
ARTP Working Groups on Standards of Care and Recommendations for Lung Function Departments (2007)
@AForesi 12

Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 13

OSAS: Sonnolenza o fatica?
Su 197 soggetti :•Astenia : 62%•Fatica : 57%
•Stanchezza : 61%•Sonnolenza : 47%
Chervin RD. Sleepiness, fatigue, tiredness, and lack of energy in obstructive sleep apnea. Chest 2000;118:372–9

Cosa fare per inquadrare il paziente
Scala della sonnolenza di Epwort (ESS)Scala di autovalutazione della Fatica (FAS)Questionario SWIFT?
Questionario di valutazione funzionale del sonno

Ann Intern Med. 2014;161:210-220.

Masa JF, et al. Effectiveness of home single-channel nasal pressure for sleep apnea diagnosis. SLEEP 2014
@AForesi 17

AUCs from ROC curves for the manual and automatic HNP home single-channel nasal pressure scorings,
based on AHI polysomnographic cutoff points
@AForesi 18
Masa JF, et al. Effectiveness of home single-channel nasal pressure for sleep apnea diagnosis. SLEEP 2014

A simplified model of screening questionnaire and home monitoring for obstructive sleep apnoea in primary care
Chai-Coetzer C.L. - Thorax 2011;66:213-219 @AForesi 19
157 pts aged 25-70 years attending their primary care physician for any reason
patients with < o > AHI 30
performance of the OSA50
screening

@AForesi 20
When GPs take an active role in screening and referral pathways then this is beneficial to the patient, the GP and the sleep clinic
BLF 2014

Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 21

•Up to 80 per cent of people with OSA have not been diagnosed
BLF 2014

@AForesi 23BLF 2014
timely access to diagnostic services

Ann Intern Med. 2014;161:210-220. doi:10.7326/M12-3187

Night-to-night variability of apnea-hypopnea index in individuals having 2 in-laboratory polysomnograms
Respir Care 2010;55(9):1196–1212
@AForesi 25
PSG

Respiratory polygraphyin sleep apnoea diagnosis
SWISS MED WKLY 2007;137:97–102 ·@AForesi 26


Phenotypes of patients with mild to moderate OSA as confirmed by cluster analysis
1184 consecutive patients AHI of 5-30/h, collected over 24 months
• REM predominant OSA, 44.6%• non-REM predominant OSA, 18.9%• supine predominant OSA, 61.9%• intermittent OSA, 12.4%
Joosten SA, et al. Respirology. 2012 Jan;17(1):99-107
@AForesi 28

Comparison of supine-only and REM-only OSA
Gillman A et al. Sleep Medicine 13 (2012) 875–878
prevalence of supine-OSA varied from 23% (strict
definition) to 63% (lenient definition);
prevalence of REM-related OSA was 10%
@AForesi 29

Sleep Med Clin 6;309–333;2011 @AForesi 30

PSG

Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 32

A Clinical Decision Rule to Prioritize PSG in Patients with Suspected Sleep Apnea
Rodsutti J; SLEEP 2004;27(4):694-9.

Reduction of AHI after automatic titration andmanual titration in 491 patients
Gao W et al. Sleep Breath (2012) 16:329–340
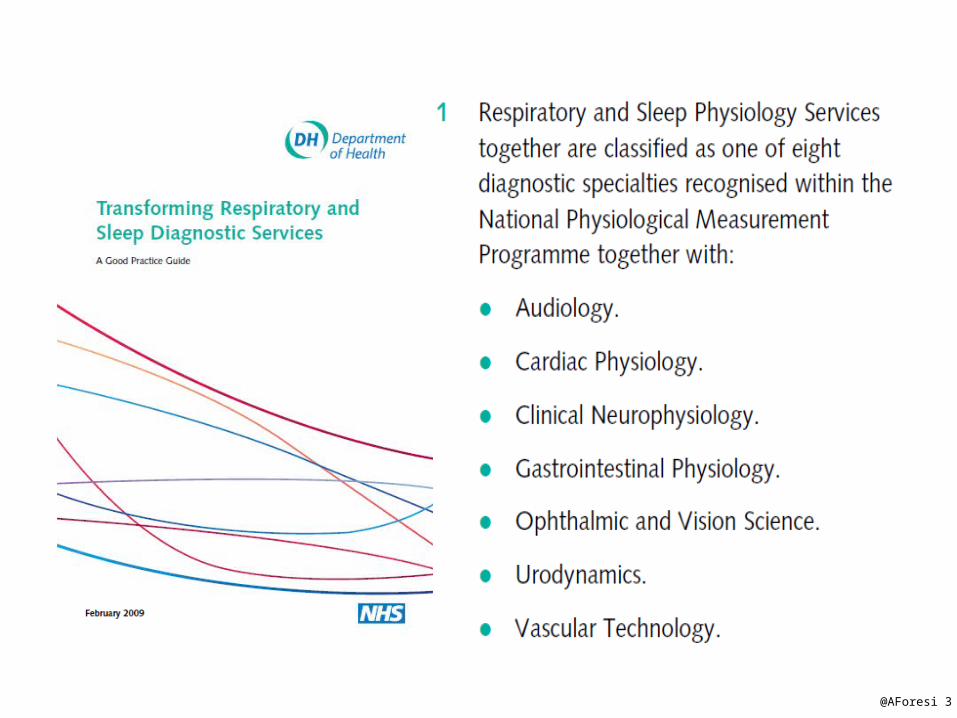
The CPAP after automatic titration and manual titration pressuredetermined by two titration methods involving
808 patients
Gao W et al. Sleep Breath (2012) 16:329–340


Residual sleepiness in obstructive sleepapnoea: phenotype and related symptoms
Vernet C. et al. Eur Respir J 2011; 38: 98–105@AForesi 37

CompSA has been reported to occur in 6% to 15% of
CPAP-treated OSAS patients
Can Respir J Vol 18 No 1 January/February 2011

Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 39

Aderenza alla terapia con CPAP
Aderenza alla terapia insufficiente se uso della CPAP inferiore a 4 ore/notte per il 70% (o meno) delle notti del periodo considerato
A livello mondiale tra il 5 e 25% dei pazienti con OSAS rifiuta l’opzione del trattamento con CPAP o ne abbandona l’uso entro la prima settimana di trattamento
Si stima che tra il l 12- 25% dei pazienti restanti abbandoni il trattamento entro i 3 anni dall’inizio .
L’aderenza del paziente al trattamento con la CPAP è il principale fattore che determina l’efficienza del trattamento stesso

@AForesi 41
BLF 2014

An Official American Thoracic Society Statement: Continuous Positive Airway Pressure Adherence Tracking Systems. The Optimal Monitoring Strategies and Outcome Measures in Adults.
Clinical algorithm for using continuous positive airway pressure adherence tracking systems.
Published in: Richard J. Schwab; Safwan M. Badr; Lawrence J. Epstein; Peter C. Gay; David Gozal; Malcolm Kohler; Patrick Lévy; Atul Malhotra; Barbara A. Phillips; Ilene M. Rosen; Kingman P. Strohl; Patrick J. Strollo; Edward M. Weaver; Terri E. Weaver; Am J Respir Crit Care Med 188, 613-620.


CPAP Adherence Factors
RussellT. - Semin Respir Crit Care Med 2014;35:604–612.

• subjective adherence was 85.1% and objective adherence was 64.5%.
Respir Care 2013;58(9):1467–1473

Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 46

• In the United States, the Center for Medicare and Medicaid Services (CMS) requires at least one face-to-face contact between the 31st and 91st days of therapy with visual inspection of adherence data verifying use > 4 hours per night 70% of the time.
Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 48

@AForesi 49
BLF 2014
“coping with the CPAP mountain”


Prima
Oggi
Configurazione del moduloe abbinamento fra
paziente e S/N
Raccolta del consenso del paziente
Chiamata del tecnico allasede per attivare
la telesorveglianza
La soluzione tecnologica a domicilio

Schema di monitoraggio paziente OSAS

Patologie respiratorie nel sonno: modelli organizzativi
• Pre-test evaluation• Screening/Referral
• Diagnosis• Treatment
• Compliance/Adherence• Follow-up
• Long term care• Costs
@AForesi 53

Full-night PSG for diagnosis and CPAP treatment of OSA are highly cost-effective are robust within the ranges of input
parameter uncertainty. Diagnosis and treatment of OSA contributes to significant
increases in patient quality of life and substantial reductions in the risk of motor vehicle collisions, heart attacks, and strokes.
Pietzsch JB et al. SLEEP 2011;34(6):695-709.



Future of sleep medicine
• Budgetary constraints on the health care system make it unlikely that we will see any significant expansion of facility-based PSG resources
• Regional Networks to organise services and management strategies at a regional level
• Shifting from a focus on diagnostic testing to chronic disease management
• Focus on quality outcomes of care moving towards a patient-centered and outcomes-based delivery model
@AForesi 57

Building a new model of Sleep-Lab
• Provide for diagnosis and treatment for all sleep disorders
• Balanced capability for in-laboratory and in-home sleep studies
• Define set of outcomes (OSA) sleep apnea symptoms, ESS, FOSQ, Fatigue, PAP compliance, blood pressure, HbA1C (for diabetics), and medication use
@AForesi 58

@AForesi 59
• Lack of awareness of OSA amongst the general population • Lack of undergraduate training for medical and dentistry students • Lack of recognition of the key symptoms by general practitioners • Lack of widespread screening based on the key symptoms • Possible referral bias towards middle-aged overweight men amongst general practitioners • Lack of standardised, accredited training for sleep medicine health care professionals • Lack of standardised, specified service provision • People not coming forward: not thinking there is a problem; embarrassment; fear of losing driving licence; not knowing there is treatment
Barriers to treatment include:
BLF 2014

Brooks R, Trimble M. The future of sleep technology:report from an American Association of Sleep Technologists summit meeting. J Clin Sleep Med 2014;10(5):589-593.

CPAP
• France 500,000• UK 330,000• Italy 120,000-140,000


Sleep Medicine is chronic care management
discipline, not a diagnostic one
@AForesi 63

Fisiopatologia Respiratoria e Disturbi nel Sonno: proposta di
rete
Antonio ForesiDirettore
U.O.C. di Pneumologia e Fisiopatologia RespiratoriaPresidio Ospedaliero di Sesto San Giovanni
@AForesi 64

Fisiopatologia Respiratoria e Disturbi nel Sonno: proposta di
rete
Antonio ForesiDirettore
U.O.C. di Pneumologia e Fisiopatologia RespiratoriaPresidio Ospedaliero di Sesto San Giovanni
@AForesi 65

Hanes et al. / Research in Social and Administrative Pharmacy j (2014) 1–16 @AForesi 66

@AForesi 67
treating 500 patients for five years prevents one fatal accident, 75 injury accidents, and 224 property damage accidents, and that £5.3 million would be saved, with an estimated treatment cost of £0.4 million (12.3 times return on investment).
BLF 2014

Hanes et al. / Research in Social and Administrative Pharmacy j (2014) 1–16 @AForesi 68
1. Referral standards 2. Diagnostic and treatment standards 3. Patient review standards
5. Driving issues
• 1. There is a rise in demand for services • 2. There is variation in service provision
between and within nations in the UK • 3. There is a growing “follow up mountain” of
people on treatment • 4. There is a need to develop ways to
influence and support the commissioning / planning process
BLF 2014

BLF 2014



Alonderis A, Barbe F, Bonsignore M, Calverley P, De BW, Diefenbach K, et al. Medico-legal implications of sleep apnoeasyndrome: driving license regulations in Europe. Sleep Med 2008;9(4):362-75.

• The Canadian Medical Association recommends that if a physician believes their patient has a sleep disorder, and the patient refuses a sleep study or refuses to comply with treatment, the patient should not drive any type of motor vehicle
Canadian Medical Association. Determining medical fitness to operate motor vehicles: CMA driver's guide. 7th ed. Ottawa: Canadian Medical
Association; 2006.

The Canadian Sleep Society is finalizing a position paper on level III sleep studies. This is expectedto be published in the Canadian Respiratory Journal but the date of publication is not yet known[Personal communication, Dr. Helen Driver, Canadian Sleep Society, June 21, 2010].

Summary of cost analysis studies


PSG





• focus in sleep medicine is shifting from procedures to outcomes.
• This will require that the sleep center team integrate with other
• medical professionals, including primary care physicians,
• otolaryngologists, behavioral specialists, and dentists





• Sleepdisordered• breathing is a common public health problem• that affects an estimated 10% of 30- to 49-
year-old men;• 17% of 50- to 70-year-old men; 3% of 30- to
49-year-old• women; and 9% of 50- to 70-year-old women

Can Respir J Vol 20 No 4 July/August 2013
Key potential care gaps

• ASA / NATA web page : http://www.sleep.org.au/membersarea/accreditation
• (last accessed 24-6-13)