Embed Size (px)
Citation preview

Flight Log
A BOOK ABOUT LIFE
AND SOMETIMES DEATH
JeffreyW. Gaver, DVM, MD, FACEP

I served as a Med Flight Physician from 1991‐2011

I also served as a Flight For Life Physician from 1988‐1992
In that capacity I had the opportunity to log approximately 5500 flights over a twenty three year period.Besides a treasure trove of great memories, the one possession I hold most dear from my Med Flight career is a half blade from a helicopter tale rotor that was presented to me on my retirement.

FLIGHT LOG:A BOOK ABOUT LIFE AND SOMETIMES DEATH
BY JEFFREY W. GAVER D.V.M. M.D.FLIGHT PHYSICIAN
EMALTERN
ATIVES INC
In 1993 I wrote a book entitled Flight Log:
A Book About life, and Sometimes Death
I would like to read the dedication to you.

DedicationThis book is dedicated to the community based Emergency Medical Systems who provide the initial care to injured patients and to the community hospital emergency departments who evaluate and stabilize their patients before transferring them to tertiary care centers.
The care that these teams offer is often the reason that many patients survive, and their compassion and concern for their patient’s comfort is reenacted across Wisconsin and the United states hundreds of times each day.
It is the author’s hope that the reader will appreciate through the chapters that follow, the joy and the anguish of being a member of one of these teams.

ACKNOWLEDGMENTSThis book also acknowledges the aeromedical transport teams who provide emergency medical services and rapid evacuation for severely ill and injured patients, sometimes at considerable risk to themselves. These nurses, paramedics, doctors, pilots, ground crews, dispatchers, and mechanics comprise an efficient organization which directs each patient into the appropriate branch of the medical system after a trauma incident or a debilitating illness.

Additional Dedication
Over the two decades that have passed since this book was written, we have lost several members of flight teams and EMS members through‐out the state. These people have made the ultimate sacrifice for their patients as have their families. Even the mention of their names is still painful for those of us who knew and worked with them. I additionally dedicate this book as a memorial to them.

So why am I sharing with you some of my EMS experiences?
•Are my stories any more meaningful than yours? •Do I feel my thoughts and feelings about my patients are somehow different or more genuine than yours?
•Do I brood about my catastrophes and failures any more than you do?
•Do I feel any more or any less stress than you do?
Of Course Not!

What is Stress?• I have a coffee cup at my offices that reads: •Stress –The irresistible urge to choke the living S___ out of some A__hole that really needs it!
•Probably a better definition is: •Stress is an individual’s total response to environmental demands or pressures.
•Stress in humans results from interactions between persons and their environment that are perceived as straining or exceeding their adaptive capacities and threatening their well‐being
•These factors include lack or loss of control over one's physical environment, and lack or loss of social support networks

Stress Reduction & Stress Causation•Obviously , one of the best stress reducers is a good outcome for the patient.
•But what if there is a bad outcome?
•What if you feel partially at fault for that bad outcome?
•What if you wish you could redo the incident all over again and make some changes in what you did?
•What if the patient’s family blames you for a bad outcome?
•What if the patient dies.
•What if you just can’t get the incident out of your mind?

My question to you then is how will you cope with your EMS stress?
•Will you nervously eat? Use drugs? Use alcohol?
•Will you fitfully sleep?
•Will you talk it through with your colleagues?
•Will you attend a critical incident stress debriefing?
•Will you use humor to deal with it?
•Will you use denial? Will you use anger?
•Will you cry?
•Will it strengthen your Faith or cause you to lose it?

Likely you may use some combination of the coping measures I listed, and probably several more I haven’t.
•You may notice that some of these coping modalities are maladaptive, and you should try to replace them with healthy ones if you can.
•An additional coping strategy that you might consider is writing about some of your experiences.
•You don’t have to write a book, but maybe you can keep a journal.
• It is a good way to deal with some of the emotions you experience after a stressful EMS run, and it helps your separate out the various components of the event that might by bothering you.

I initially wrote Flight Log to deal with some of the pain and tragedy that I saw during my early career as a flight physician. •But, I also wrote the book to demonstrate the skill and the compassion shown by my fellow EMS workers toward their patients.
•Additionally, I have tried to highlight the resilience, courage, and strength that the patients themselves display.
•Along with the sadness, I do describe some humorous events as well.
•Over the several minutes, I would like to share a few of my flight experiences with you.

First FlightIt was one of those rare spring Mondays when the Emergency Department wasn’t busy. It had rained most of the day, but now, about four o’clock in the afternoon, the sun was starting to peek through the clouds.
I heard the flight pager’s high pitched whine as I came out of Paramedic Base after finishing my radio call.
Cathleen, the flight doctor, was a resident in her final year of training. She must have noticed the longing look on my face, because she called out to me as she headed toward the hanger.
PARAMEDIC BASE

“Hey G‐man” She said. “Why don’t you ask the attending if you can come along?”
I ran into the ED with my heart pounding in anticipation. The supervising doctor in the department said, “Go ahead, it’s slow, have a nice flight.”
During the next few minutes I put on my flight suit and listened to the last minute safety instructions given by the pilot and flight nurse.
It was a joyous moment for me as I attached the leather name badge that read Flight Physician.

LIFT OFF
I secured my shoulder harness, put on my helmet, and we lifted off. I listened to the pilot talking to the tower. It was marvelous!

The base gave us the medical report.
Our patient was a young man who had an influenza like illness over the weekend, and was still quite ill on Monday.
He had consulted his doctor earlier in they day, and because he had a high WBC, he was hospitalized.
Over the next few hours, his blood pressure dropped and he had difficulty breathing.
He had been moved to the ICU and intubated, but because his condition was deteriorating, his doctor wanted him transferred to the tertiary care center.

We flew north along lake Michigan.
The trip was beautiful and the signs of spring were everywhere.
The pilot set the ship down gently on the pad while we watched out the window for foreign objects, trees, wires, and people.
The engines cooled down, then came to a stop, and we went in to the small modern hospital

We found the patient in his ICU bed attended by his physician, a kind man with a very concerned look on his face. The patient’s wife was a nurse at the hospital and was at his bedside.
His parents were in the waiting room.
Everyone appeared to be anxious, but they seemed relieved to have us there.


We loaded him into the helicopter and took off for the hospital. I don’t remember much about the flight back, because we too were busy trying to maintain his oxygen saturation and blood pressure.
However, It did seem to take a long time to get back to the medical center, and even the engine cool down seemed to last forever.
We quickly transferred the patient from the helicopter into the hospital and from the transport cot into his ICU bed, gave report and returned to the ED.
He was hypotensive, and his skin was cool and clammy. He was obviously in septic shock. Cathy, the flight physician, did a rapid evaluation of the patient while the nurse and I changed over his monitor and IV drips

The next morning when I came in, Cathy handed me some pills and said. “That patient died about an hour after we left him last night. “
“He had meningococcal sepsis and we’re supposed to take these pills so we don’t get sick.” “They will turn your urine orange, and they are hard on your stomach.”“By the way, part of being a good flight doc is understanding that you can’t save everyone. “You hope for the best and cope with the rest!”This was not the way I’d hoped my first flight would end.

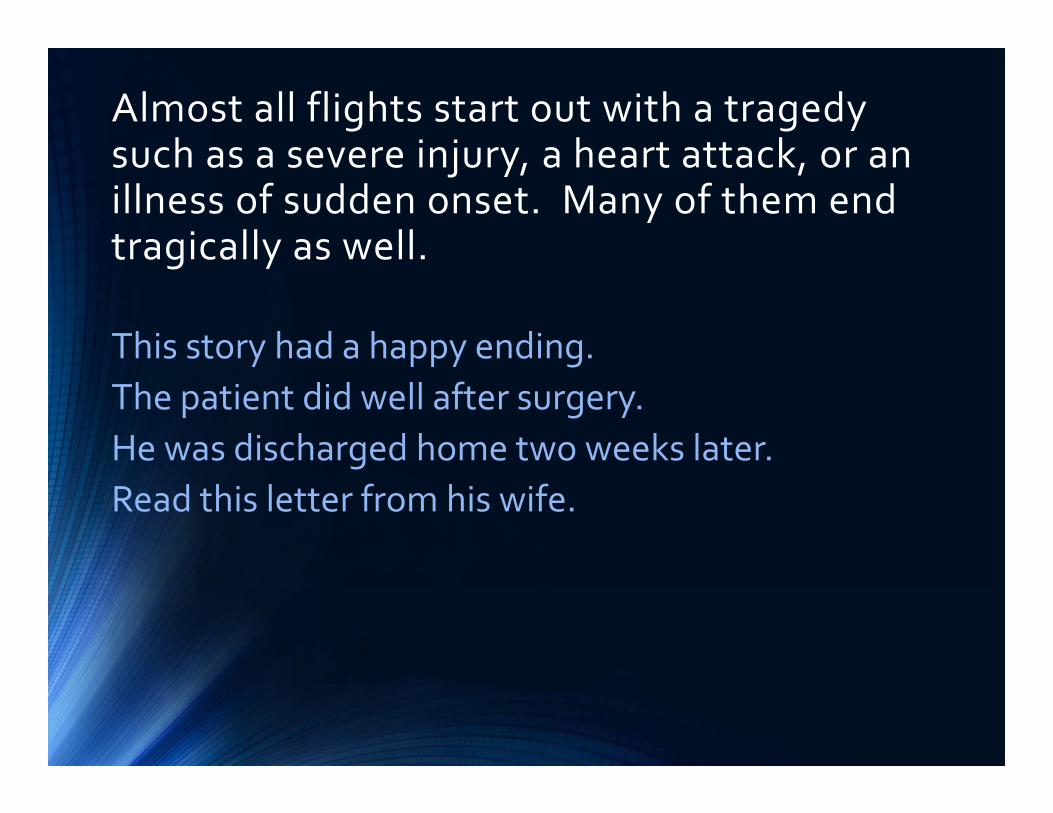
Medical Report Flight: 1988225The patient is a forty‐seven year old man who was just “trying out” a motorcycle.He was not wearing a helmet and crashed a few blocks from his home.
He was unresponsive at the scene and had obvious head trauma.

He required rapid sequence intubation, transport to the trauma center, and immediate neurosurgical consultation.

Diagnosis:Epidural hematoma
Treatment: Neurosurgical decompression of the brain
Almost all flights start out with a tragedy such as a severe injury, a heart attack, or an illness of sudden onset. Many of them end tragically as well.
This story had a happy ending. The patient did well after surgery.He was discharged home two weeks later. Read this letter from his wife.

Dear Flight Doctor and Nurses, This card is for the wonderful crew on the helicopter on September 27.There are not enough words to express how very grateful we are to you all for your caring and very professional care of my husband on the flight from out hospital to the Trauma Center. You saved his life and gave me my husband and father of our four boys back to us and for that I’ll never forget each and every one of you. A special thank you to the nurse for taking my husband out to see the helicopter he rode in. The flight pin you put on him is treasured by all of us. God Bless you all your are always in our prayers. Thank you from the bottom of my heart. Your thoughtfulness will always be remembered. With love,The Family of DJ

SOLO
It is July 9, 1989. I have been a qualified flight doctor for nine days, but I have yet to fly my first solo mission.
Finally about one o’clock in the afternoon, my flight pager whines its alert tone and announces a flight request to a city fifty miles south along lake Michigan. I am ready.
When I look back at the flight summary, I am amazed at how much it doesn’t tell me.
The medical information is there, but there is none of the passion.
The report begins as follows:

This patient is a seven year old male child who was transferred to CHOW by FFL Helicopter from the referring hospital subsequent to a near drowning episode.
He was swimming in Lake Michigan with his family when a wave knocked him over.
No one could get to him for 10 minutes.
When he was pulled from the water he was cyanotic, pulseless, and non‐breathing.
After a short course of CPR, the patent developed a pulse, blood pressure and respiration, but he was neurologically unresponsive when transferred to the hospital by ambulance.


Imagine this. A family is together for an outing on a beautiful July day.
Suddenly they see their child swept under the water and they can’t get to him!
In seconds their life has changed from a happy care free existence to terror!
When they finally do reach him, he is blue and not breathing.
He may be dead!
The paramedics arrive and are able to regain a pulse, and BP, but the child is making no respiratory efforts, and is completely unresponsive.

The family watches helplessly in numbed horror as their son is whisked away by ambulance to the hospital.When the family arrives at the hospital, they learn that their child is on a ventilator and will soon be transferred by helicopter to a children’s hospital 50 miles away.
Can you imagine the worry grief, and guilt that surrounds them while they attempt to answer questions about their address, the details of the accident, and what is their insurance?
On the way to the helicopter, we stop and let the family say goodbye.

We are in a small Catholic Hospital and I notice that the family has a Nun accompanying them.
She asks me if I am a Christian and when I answer yes, the family visibly relaxes.
I explain that I am also a daddy and will treat this child as if is my very own son.
I ask them If they would like me to say a prayer before we go and they nod yes through their tears.
I ask God to protect this child, and to let him live and to send him home to his family safe and sound.

I finish the prayer, and in a moment we are off in the helicopter.
The flight back to the medical center goes smoothly.
I hand ventilate the child with the ambu bag and watch while the flight nurse gently strokes his hair.
I am filled with memories of my own son when he was that age.
Upon our arrival, the child is a direct admit to the pediatric ICU and I endorse his care over the pediatric critical care fellow.

I finished my ED shift at 7 pm and went to check in on the patient back at the pediatric ICU
The critical care attending tells me the child appears to be awakening.
He is quite hopeful that the child will recover.
He may even be extubated later that evening.
It is too early to tell for sure, but he and the ICU fellow have a good feeling about this child.

The next morning, I arrive early before my ED shift begins so I can visit my patients.
The child is no longer in the ICU and has moved to a general nursing floor.
He appears normal and asks for something to eat.
He has no recollection of any of the events before his drowning and he has absolutely no idea who I am.
Three days later he is discharged home with his happy family with no disabilities what‐so‐ever.
I breathe a prayer of thanks. Another day at the ED begins.

Road America
Road America is a 4 mile road race course near Elkhart Lake, Wisconsin

Race Day at Road AmericaA race day at Road America is a glorious collage of colors, sounds, and smells. The brilliant hues of the cars, the drivers in their brightly colored helmets and racing suits, the sounds of revving racing engines, and ah yes, the fragrances. This wonderful pungent odor encompasses a mixture of racing fuels, outdoor grills, and burning rubber wafting over the track to form an elegant aromatic olfactory symphony.

One of the track’s technical inspectors has developed a program in which he invites kids with leukemia and other childhood cancers to the races.
The kids just love the cars and the excitement.

For some of them it may be their last outing anywhere before they succumb to their disease.
During the noon break, the kids are given a tour around the track in vans and convertibles.
They get to meet the drivers and get to take home posters, hats, pins, and racing patches.

Each of the 14 corners has a group of flagmen who signal the race drivers about possible track hazards ahead.
As the children passed through each turn, that corner would erupt in a sea of color.The workers, in a spontaneous show of encouragement and affection, waved every flag they had at the kids. The kids were overjoyed!

The crowd roared its approval and I don’t think there were many dry eyes in the viewing stands that day.
• It was a wonderful moment for all of us.
•Everyone, at least briefly, exuded a spirt of harmony and brotherhood.
•As we flew over this tremendous scene in the helicopter, my heart nearly leapt with joy.
•On the way home, my son Justin told me it was a day he’d never forget.

Triage is a French word which means “to sort”• In multiple trauma injuries, the word is used two ways.
•The first use is when there are adequate resources to handle all the patients.
•Triage in this case means to treat those patients first who are the most severely ill or injured.
•The second use of the word triage is when the number of causalities exceeds the resources that are available to care for them.
•Triage in this sense means to treat those with injuries who have the greatest chance of survival with the resources you have to work with.
•Triage was initially used to sort war causalities, but it has been widely adapted to the EMS system when multiple patients are injured.
•Observe on this flight how the meaning of triage sadly becomes true.

Thanksgiving is a time when families get together. It is also when the college students come home for the long weekend.
It is the beginning of the Christmas season.
Roads are crowded with families returning home or returning their children to their college campuses.
The Sunday after Thanksgiving is an especially busy day in the ED.
A family was bringing their daughter from Illinois to Oshkosh, Wisconsin where she attended the University.
A driver from the opposite direction suddenly crossed the median and crashed into their car.
The local EMS squads arrive. There are multiple victims, some with serious injuries.

The trauma center’s helicopter flight team is activated and arrives at the scene about 2o minutes later.

The flight physician and nurse begin to triage the patients. There are six victims. The flight dictation reads as follows:
The first patient is a male in his early forties. CPR has been in progress for 15 minutes. He has sustained multiple blunt trauma. There are no heart tones and there is no electrical heart activity on the monitor. The patient is pronounced dead at 1405.
The second patient is a female in her forties and appears to be the first patient’s wife. CPR has been in progress for eighteen minutes. She has also sustained multiple blunt trauma. There are no heart tones and no electrical activity on the cardiac monitor. She is pronounced dead at 1410.

The third victim is a female in her late teens or early twenties. CPR has been in progress for twenty minutes with no response, no heart tones and no electrical heart activity on the monitor. She is pronounced dead at 1415.
The fourth patient is a teenaged female who is talking and has sustained only minor injuries. She says that she is fifteen years old. An EMT is assigned to continue evaluating her while the flight physician and nurse attend to the other injured patients. Her vital signs are stable at 1420.
The fifth patient is a female in her early thirties with minor injuries. She appears normal, but may be post ictal and does not remember the crash. Vital signs are stable at 1425.

The last victim is a female child about ten years old.She has obvious severe chest injuries, is hypotensive, and is unable to speak. The little girl hands the physician a folded piece of paper and then becomes unresponsive. The physician stuffs the paper in to his pocket and while the flight nurse starts two intravenous lines, the doctor intubates the little girl, and attaches her to the monitor. It reveals a slow heart rate in an agonal rhythm. Chest compressions are initiated and ACLS drugs are given. After half an hour, the patient has not responded, and is pronounced dead at 1500.

The teenaged girl, and the lady who came across the median and caused the crash, are transported to the local hospital.
The flight team returns to the trauma center with no patients. On the trip back home, the flight nurse asks the doctor, “What was that paper that the little girl gave you?”The doctor pulls the paper out of his pocket, reads it and hands it to the nurse.It is the child’s letter to Santa Claus!Not one word is spoken on the way back to the hospital.
Postscript
The lady driver of the car that hit the family recovered uneventfully. She had a seizure disorder which caused her to lose consciousness and cross the median causing the accident.
The fifteen year old went to live with relatives in Illinois.
Two years later, on the way home from her prom, she and her date were killed by a tree falling across their car in a storm.
She is with her family now!

As physicians at a large regional medical center, we treat patients from a diversity of socio‐economic and cultural backgrounds. They have their own language to describe their illnesses.For instance if a patient tells me a family member has passed, they mean they died.
If they say they have the sugar, that means they have diabetes.
When I was a first year resident, several patients told me that their booty hurt. It took me six weeks to stop radiographing their feet and realize that the meant their bottoms!
We kept a note book in the ED for a couple of years to record some of the more colorful terminology that patients use to describe disease.