Embed Size (px)
Citation preview

FORMULE per
LATTANTI
PRETERMINE PRETERMINE
POST
DISCHARGE
Carla Pittini
SOC Neonatologia
Appunti di alimentazione nei primi due anni di età – Udine 2 febbraio 2018
SOC Neonatologia
ASUIUD
non ho conflitti di interesse attuali o potenziali in
DICHIARAZIONE:
non ho conflitti di interesse attuali o potenziali in
merito all’argomento della relazione
IL MIGLIOR ALIMENTO per IL NEONATO PRETERMINE
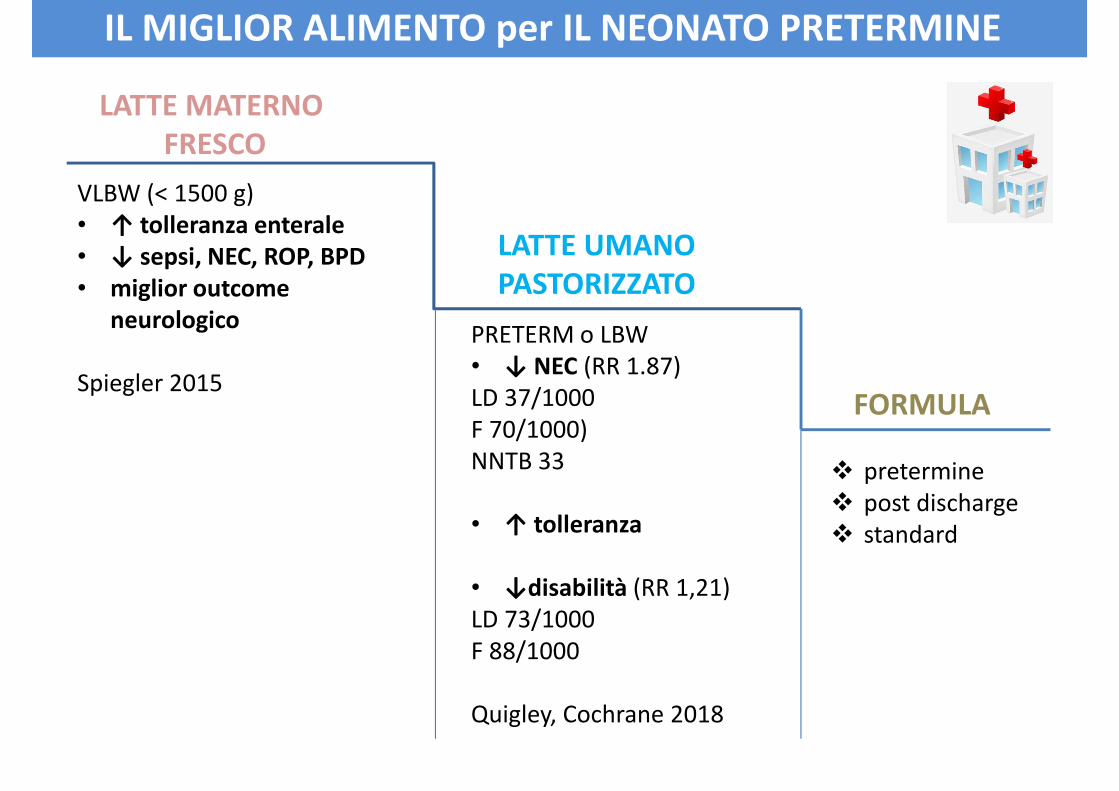
IL MIGLIOR ALIMENTO per IL NEONATO PRETERMINE
VLBW (< 1500 g)
• ↑ tolleranza enterale
• ↓ sepsi, NEC, ROP, BPD
LATTE MATERNO
FRESCO
LATTE UMANO
PASTORIZZATO• ↓ sepsi, NEC, ROP, BPD
• miglior outcome
neurologico
Spiegler 2015
LATTE UMANO
PASTORIZZATO
FORMULA
� pretermine
� post discharge
� standard
PRETERM o LBW
• ↓ NEC (RR 1.87)
LD 37/1000
F 70/1000)
NNTB 33
• ↑ tolleranza� standard• ↑ tolleranza
• ↓disabilità (RR 1,21)
LD 73/1000
F 88/1000
Quigley, Cochrane 2018
Recommendations on Breastfeeding Management
for Preterm Infants
1. All preterm infants should receive human milk
- human milk should be fortified, with protein, minerals and vitamins to
ensure optimal nutrient intake for infants weighing < 1500 g at birthensure optimal nutrient intake for infants weighing < 1500 g at birth
- pasteurized donor human milk, appropriately fortified, should be used
if mother’s own milk is unavailable or its use is contraindicated
2. Methods and training protocols for manual and mechanical milk expression must
be available to mothers
3. Neonatal intensive care units should possess evidence-based protocols for
collection, storage and labeling of human milk
4. Neonatal intensive care units should prevent the misadministration of human
milk
5. There are no data to support routinely culturing human milk for bacterial or5. There are no data to support routinely culturing human milk for bacterial or
other organisms
POLICY STATEMENT
Breastfeeding and the Use of Human Milk. 2012
The Committee advocates the use of human milk for preterm infants as standard
practice, provided it is fortified for added nutrients where necessary to meet
requirements
Parents and health care providers should be aware thet human milk composition
may vary for the duration of lactation, within the day, and even during 1 expressionmay vary for the duration of lactation, within the day, and even during 1 expression
The treatment following expression (storage, pasteurization) may influence
composition
As an alternative to human milk, preterm formula may be used
Enteral nutrient supply for preterm infants: commentary from the
European Society for Peaditric Gastroentereology, Hepatology, and
Nutrition Commitee on Nutrition .
2010
Obiettivi della nutrizione dopo la DIMISSIONE
� recuperare il ritardo di crescita extrauterino del neonato VLBW (< 1500 g)
� garantire il miglior sviluppo somatico e neurocognitivo
� porre attenzione all’outcome in età adulta: rischio metabolico e cardio-vascolare
… stessi obiettivi in
OSPEDALE
“La crescita del neonato pretermine dovrebbe
seguire quella del FETO umano normale”
AAP, Pediatrics 1977
QUANTO DEVE CRESCERE un PRETERMINE ?
una volta recuperato il PN
14 – 16 g/Kg/die
Ehrenkranz 1999
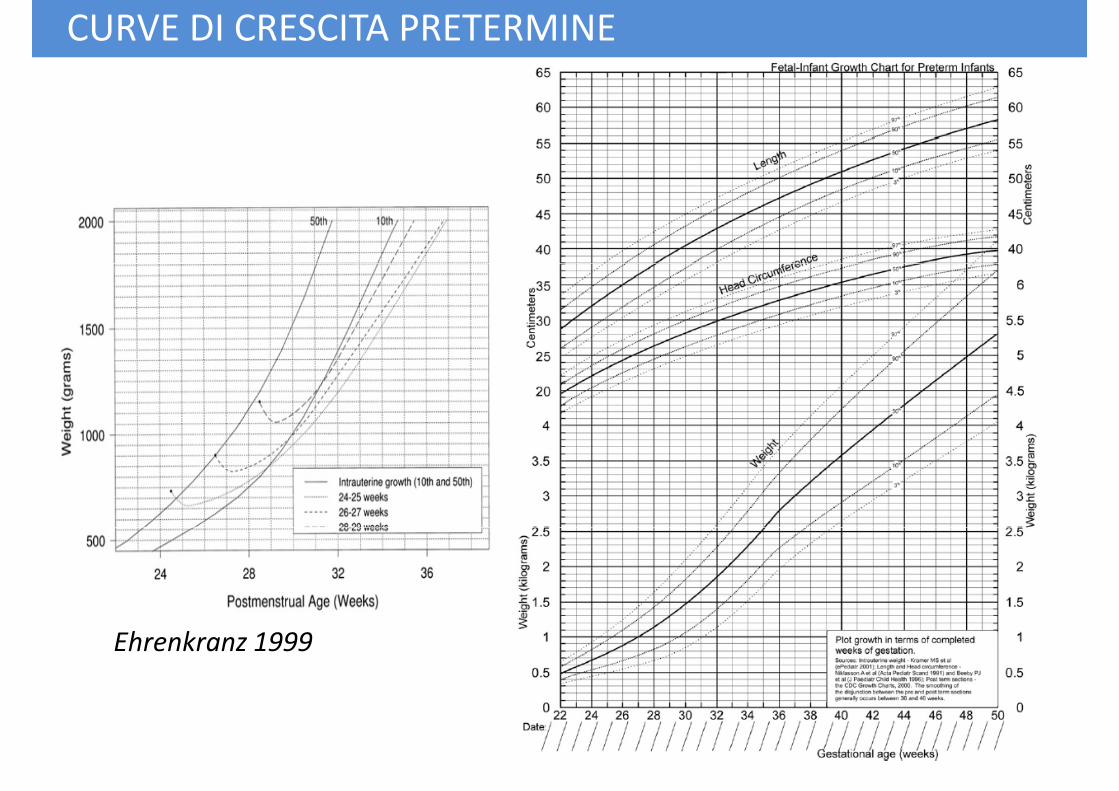
CURVE DI CRESCITA PRETERMINE
Ehrenkranz 1999
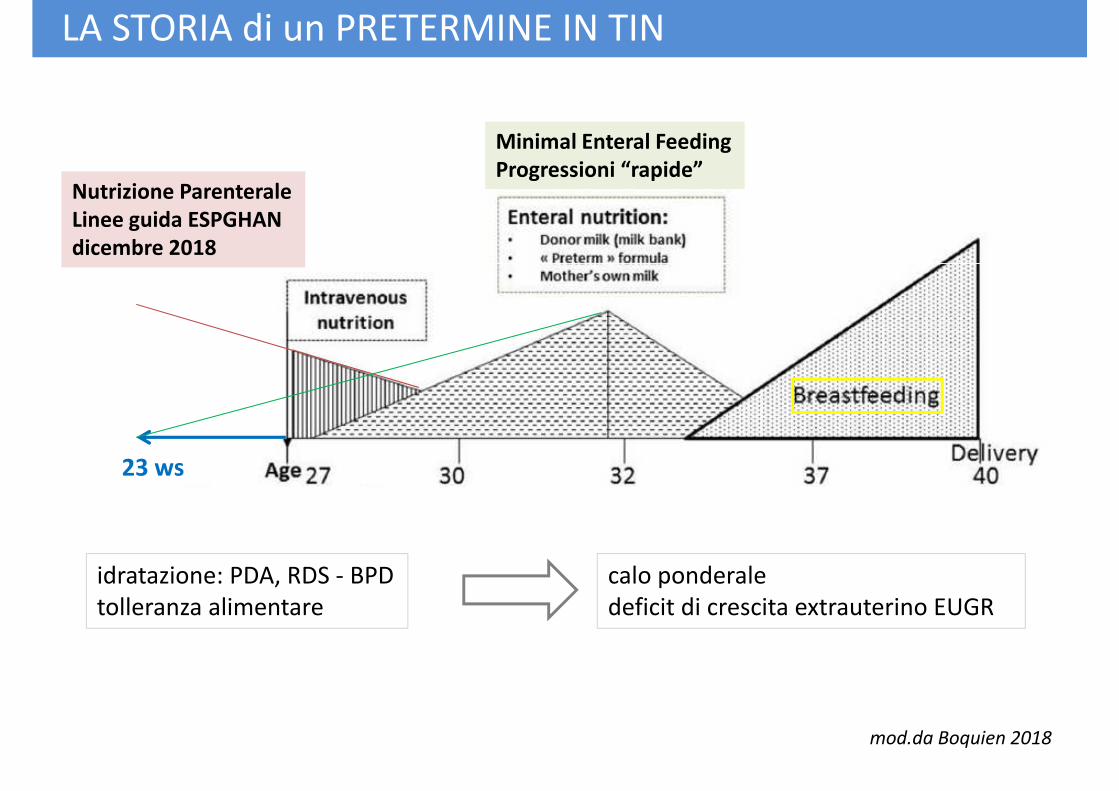
Nutrizione Parenterale
Linee guida ESPGHAN
dicembre 2018
Minimal Enteral Feeding
Progressioni “rapide”
LA STORIA di un PRETERMINE IN TIN
23 ws
mod.da Boquien 2018
idratazione: PDA, RDS - BPD
tolleranza alimentare
calo ponderale
deficit di crescita extrauterino EUGR
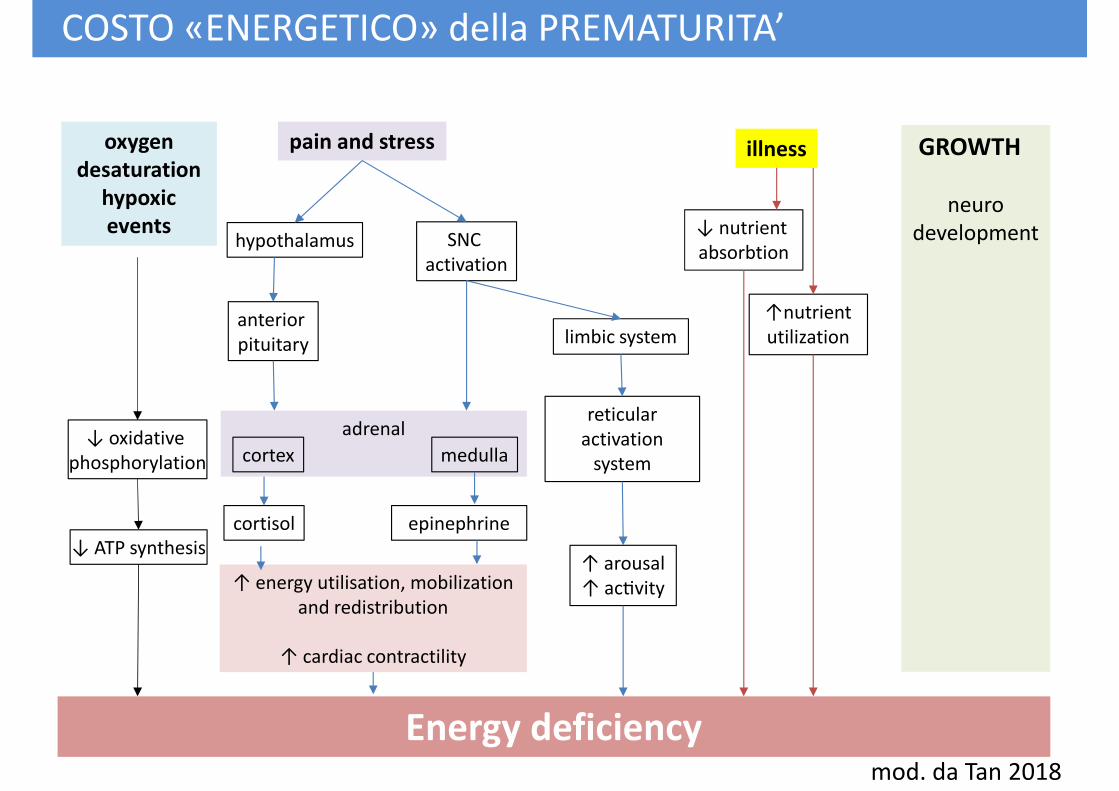
oxygen
desaturation
hypoxic
events
pain and stress
hypothalamus SNC
activation
GROWTH
neuro
development
illness
↓ nutrient
absorbtion
COSTO «ENERGETICO» della PREMATURITA’
↓ oxidative
phosphorylation
activation
anterior
pituitary
adrenal
cortex medulla
cortisol epinephrine
limbic system
reticular
activation
system
absorbtion
↑nutrient
utilization
↓ ATP synthesis
cortisol epinephrine
↑ energy utilisation, mobilization
and redistribution
↑ cardiac contractility
↑ arousal
↑ acNvity
Energy deficiencymod. da Tan 2018
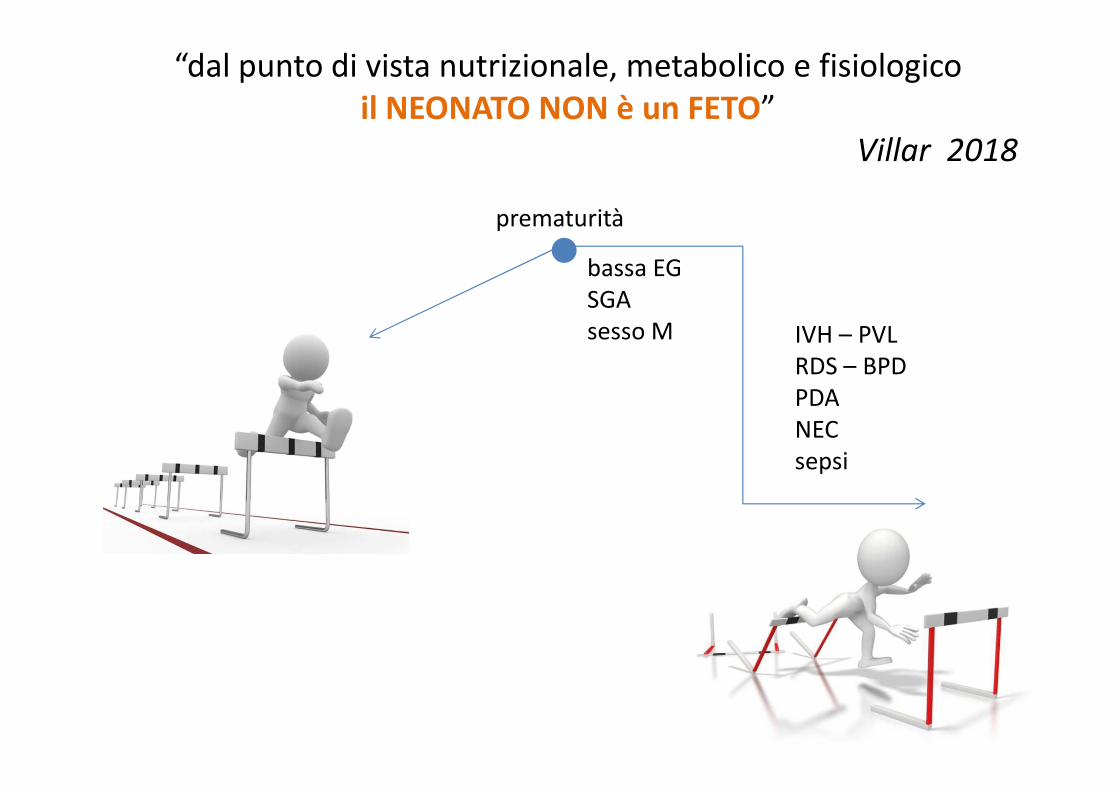
“dal punto di vista nutrizionale, metabolico e fisiologico
il NEONATO NON è un FETO”
Villar 2018
prematurità
bassa EG
IVH – PVL
RDS – BPD
PDA
NEC
sepsi
bassa EG
SGA
sesso M
The INTERGROWTH-21st project was a multi-centre, multi-ethnic, population-based
project, conducted between 2009 and 2014, in eight demarcated urban areas:
Pelotas, Brazil; Shunyi County, Beijing, China; Central Nagpur, India; Turin, Italy;
Parklands Suburb, Nairobi, Kenya; Muscat, Oman; Oxford, UK, and Seattle, USA.
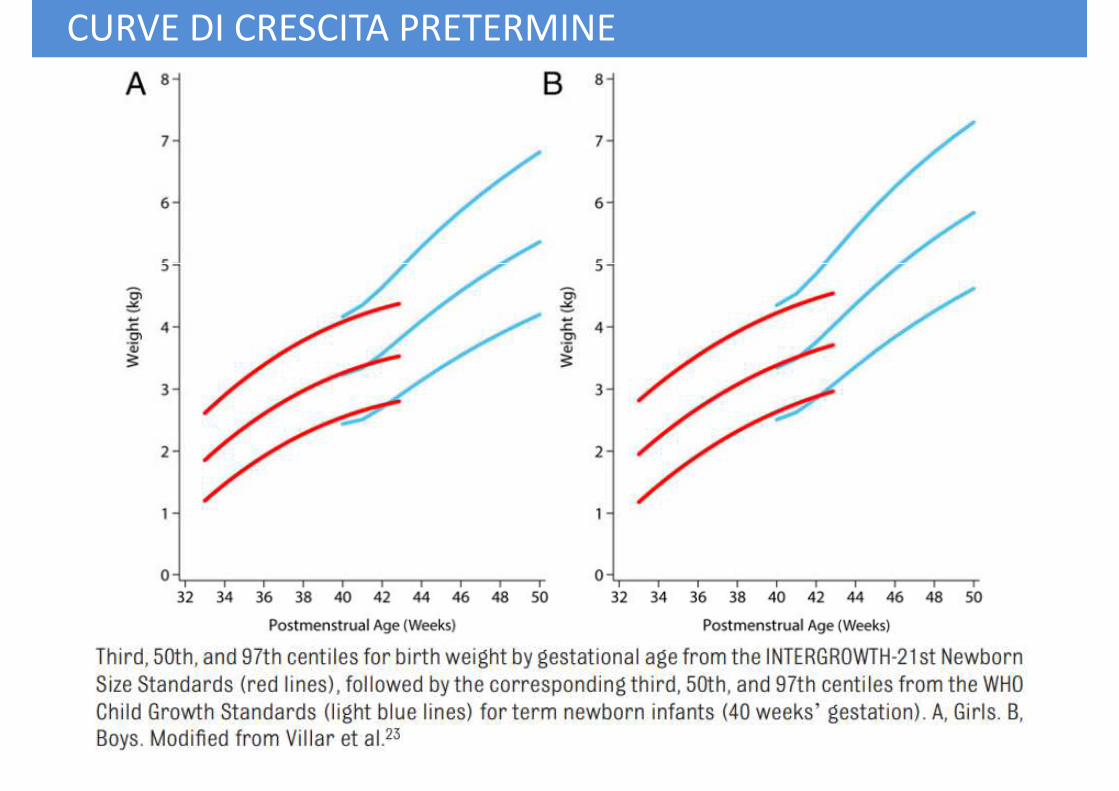
CURVE DI CRESCITA PRETERMINE
Parklands Suburb, Nairobi, Kenya; Muscat, Oman; Oxford, UK, and Seattle, USA.
Its primary aim was to study growth, health, nutrition and neurodevelopment from
<14weeks of gestation to 2 years of age, using the same conceptual framework as the
WHO Multicentre Growth Reference Study, so as to produce international prescriptive
standards for pregnancy dating, maternal weight gain, fetal growth, newborn size, the
postnatal growth of preterm infants and cognitive development at 2 years of age.
These scientifically robust clinical tools may be used to monitor and evaluate maternal
and fetal wellbeing, as well as infant health and nutrition at an individual and and fetal wellbeing, as well as infant health and nutrition at an individual and
population level
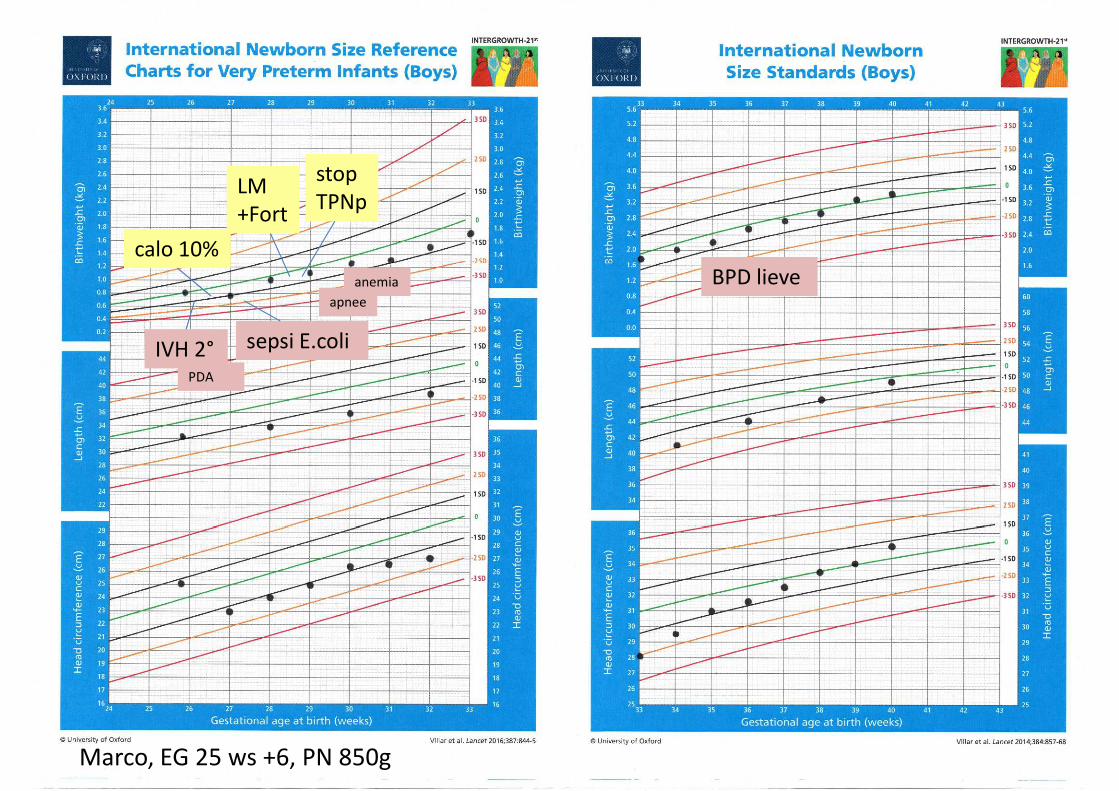
BPD lieve
calo 10%
LM
+Fort
stop
TPNp
BPD lieve
sepsi E.coliIVH 2°
apnee
anemia
PDA
Marco, EG 25 ws +6, PN 850g
CURVE DI CRESCITA PRETERMINE
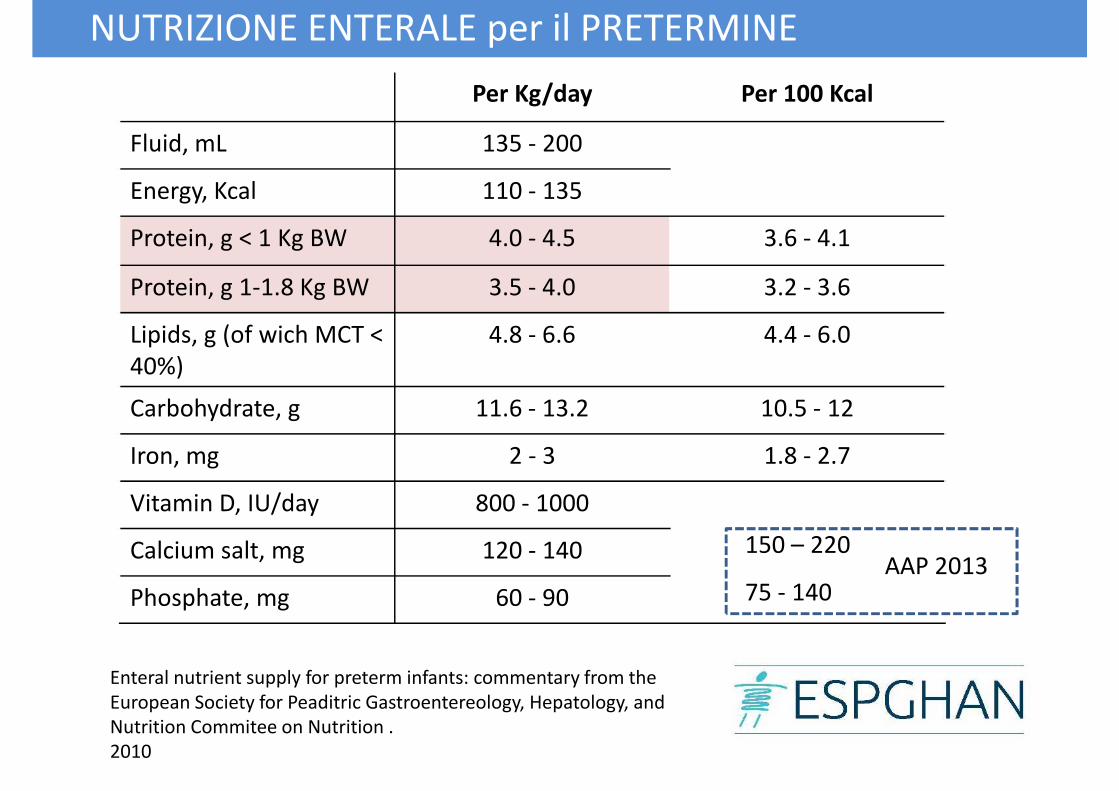
Per Kg/day Per 100 Kcal
Fluid, mL 135 - 200
Energy, Kcal 110 - 135
Protein, g < 1 Kg BW 4.0 - 4.5 3.6 - 4.1
NUTRIZIONE ENTERALE per il PRETERMINE
Protein, g 1-1.8 Kg BW 3.5 - 4.0 3.2 - 3.6
Lipids, g (of wich MCT <
40%)
4.8 - 6.6 4.4 - 6.0
Carbohydrate, g 11.6 - 13.2 10.5 - 12
Iron, mg 2 - 3 1.8 - 2.7
Vitamin D, IU/day 800 - 1000
Calcium salt, mg 120 - 140
Phosphate, mg 60 - 90
Enteral nutrient supply for preterm infants: commentary from the
European Society for Peaditric Gastroentereology, Hepatology, and
Nutrition Commitee on Nutrition .
2010
150 – 220
75 - 140AAP 2013
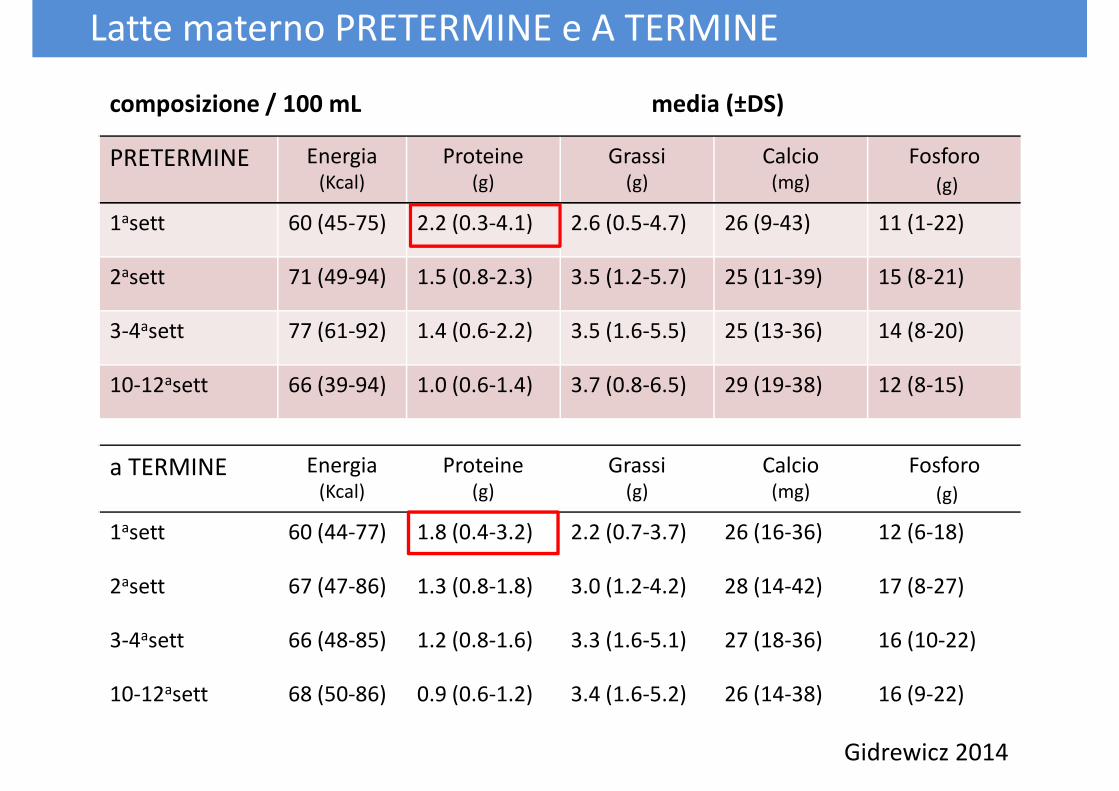
composizione / 100 mL media (±DS)
PRETERMINE Energia (Kcal)
Proteine(g)
Grassi (g)
Calcio (mg)
Fosforo
(g)
1asett 60 (45-75) 2.2 (0.3-4.1) 2.6 (0.5-4.7) 26 (9-43) 11 (1-22)
2asett 71 (49-94) 1.5 (0.8-2.3) 3.5 (1.2-5.7) 25 (11-39) 15 (8-21)
Latte materno PRETERMINE e A TERMINE
2asett 71 (49-94) 1.5 (0.8-2.3) 3.5 (1.2-5.7) 25 (11-39) 15 (8-21)
3-4asett 77 (61-92) 1.4 (0.6-2.2) 3.5 (1.6-5.5) 25 (13-36) 14 (8-20)
10-12asett 66 (39-94) 1.0 (0.6-1.4) 3.7 (0.8-6.5) 29 (19-38) 12 (8-15)
a TERMINE Energia (Kcal)
Proteine(g)
Grassi (g)
Calcio (mg)
Fosforo
(g)
1asett 60 (44-77) 1.8 (0.4-3.2) 2.2 (0.7-3.7) 26 (16-36) 12 (6-18)
Gidrewicz 2014
1asett 60 (44-77) 1.8 (0.4-3.2) 2.2 (0.7-3.7) 26 (16-36) 12 (6-18)
2asett 67 (47-86) 1.3 (0.8-1.8) 3.0 (1.2-4.2) 28 (14-42) 17 (8-27)
3-4asett 66 (48-85) 1.2 (0.8-1.6) 3.3 (1.6-5.1) 27 (18-36) 16 (10-22)
10-12asett 68 (50-86) 0.9 (0.6-1.2) 3.4 (1.6-5.2) 26 (14-38) 16 (9-22)
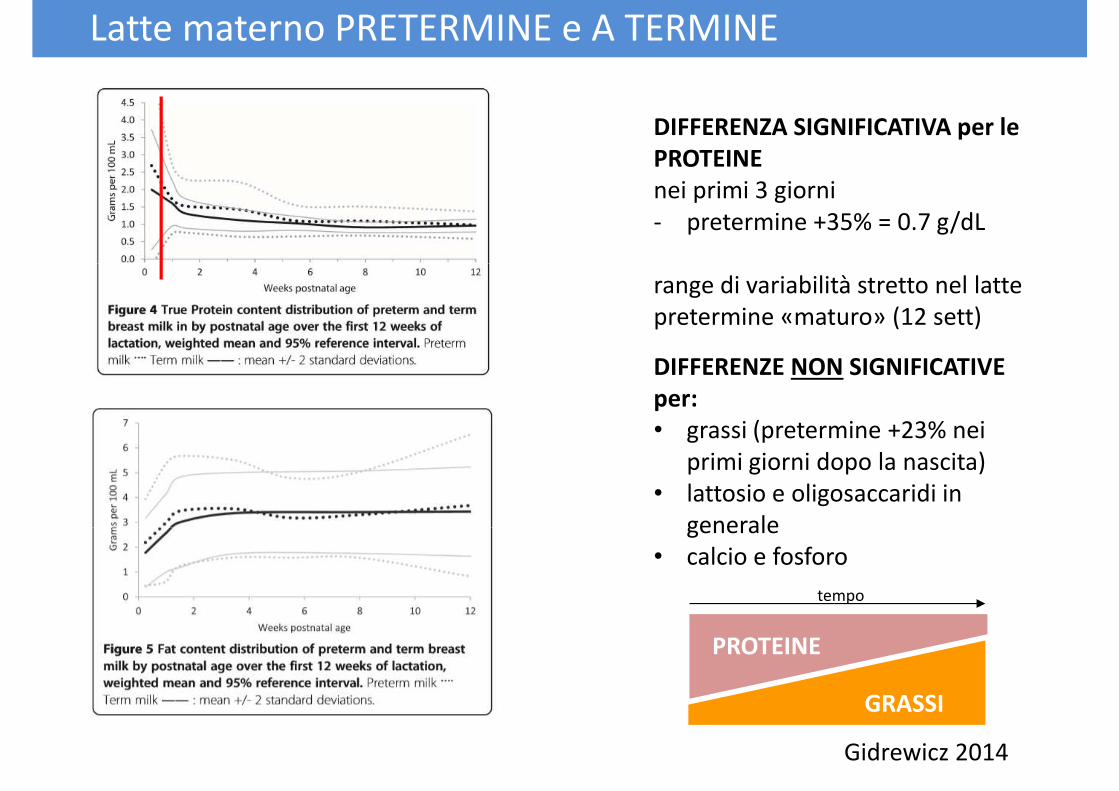
DIFFERENZA SIGNIFICATIVA per le
PROTEINE
nei primi 3 giorni
- pretermine +35% = 0.7 g/dL
Latte materno PRETERMINE e A TERMINE
range di variabilità stretto nel latte
pretermine «maturo» (12 sett)
DIFFERENZE NON SIGNIFICATIVE
per:
• grassi (pretermine +23% nei
primi giorni dopo la nascita)
• lattosio e oligosaccaridi in
generalegenerale
• calcio e fosforo
PROTEINE
GRASSI
tempo
Gidrewicz 2014
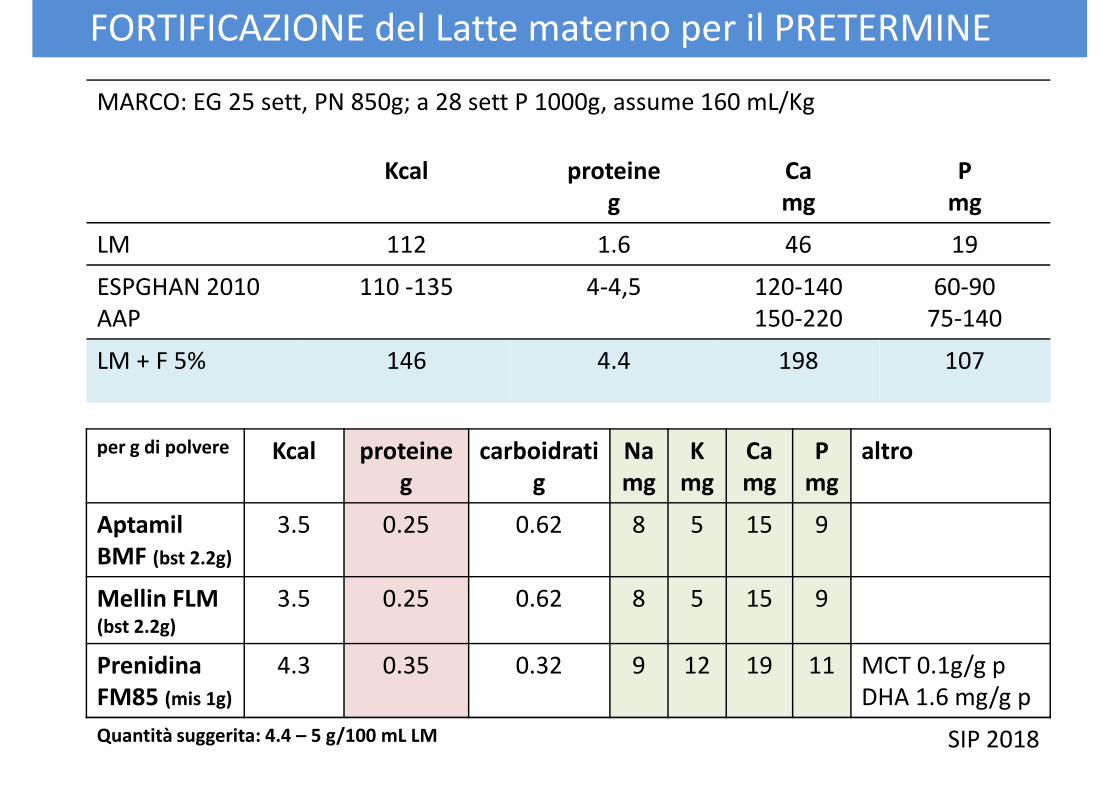
FORTIFICAZIONE del Latte materno per il PRETERMINE
MARCO: EG 25 sett, PN 850g; a 28 sett P 1000g, assume 160 mL/Kg
Kcal proteine
g
Ca
mg
P
mg
LM 112 1.6 46 19
per g di polvere Kcal proteine
g
carboidrati
g
Na
mg
K
mg
Ca
mg
P
mg
altro
Aptamil 3.5 0.25 0.62 8 5 15 9
ESPGHAN 2010
AAP
110 -135 4-4,5 120-140
150-220
60-90
75-140
LM + F 5% 146 4.4 198 107
Aptamil
BMF (bst 2.2g)
3.5 0.25 0.62 8 5 15 9
Mellin FLM (bst 2.2g)
3.5 0.25 0.62 8 5 15 9
Prenidina
FM85 (mis 1g)
4.3 0.35 0.32 9 12 19 11 MCT 0.1g/g p
DHA 1.6 mg/g p
Quantità suggerita: 4.4 – 5 g/100 mL LM SIP 2018
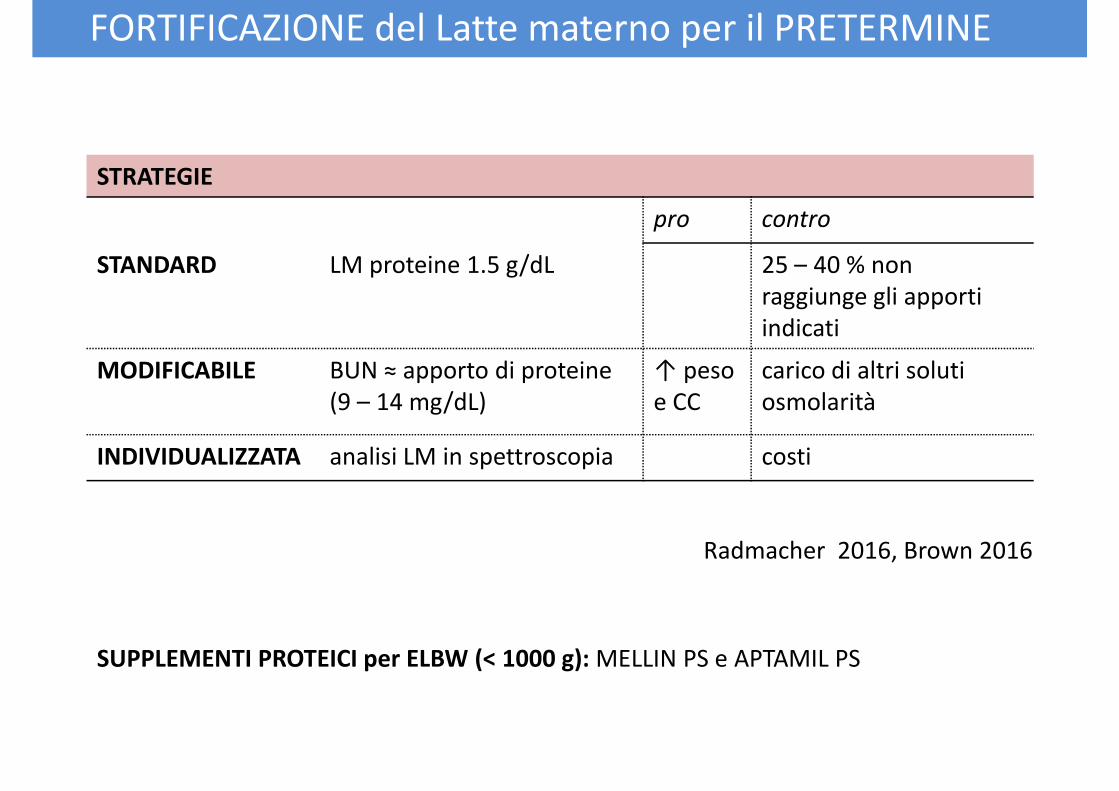
FORTIFICAZIONE del Latte materno per il PRETERMINE
STRATEGIE
pro contro
STANDARD LM proteine 1.5 g/dL 25 – 40 % non STANDARD LM proteine 1.5 g/dL 25 – 40 % non
raggiunge gli apporti
indicati
MODIFICABILE BUN ≈ apporto di proteine
(9 – 14 mg/dL)
↑ peso
e CC
carico di altri soluti
osmolarità
INDIVIDUALIZZATA analisi LM in spettroscopia costi
Radmacher 2016, Brown 2016
SUPPLEMENTI PROTEICI per ELBW (< 1000 g): MELLIN PS e APTAMIL PS
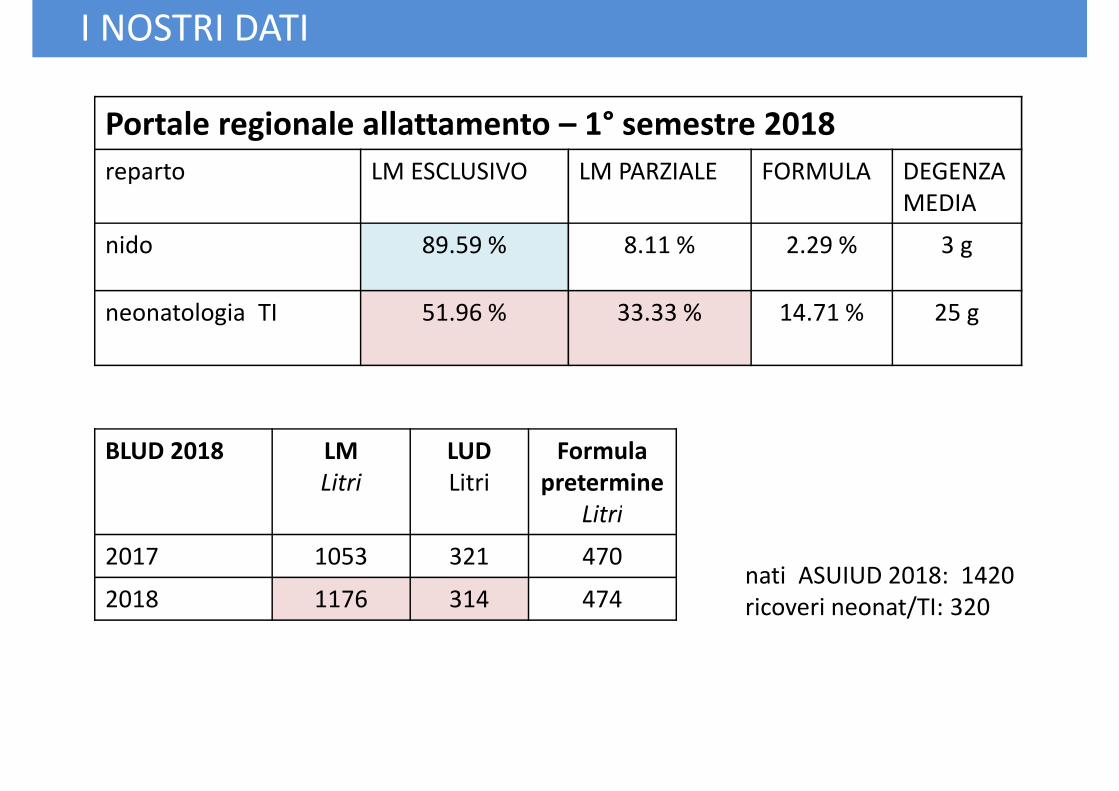
I NOSTRI DATI
Portale regionale allattamento – 1° semestre 2018
reparto LM ESCLUSIVO LM PARZIALE FORMULA DEGENZA
MEDIA
nido 89.59 % 8.11 % 2.29 % 3 g
neonatologia TI 51.96 % 33.33 % 14.71 % 25 g
BLUD 2018 LM
Litri
LUD
Litri
Formula
pretermine
LitriLitri
2017 1053 321 470
2018 1176 314 474nati ASUIUD 2018: 1420
ricoveri neonat/TI: 320
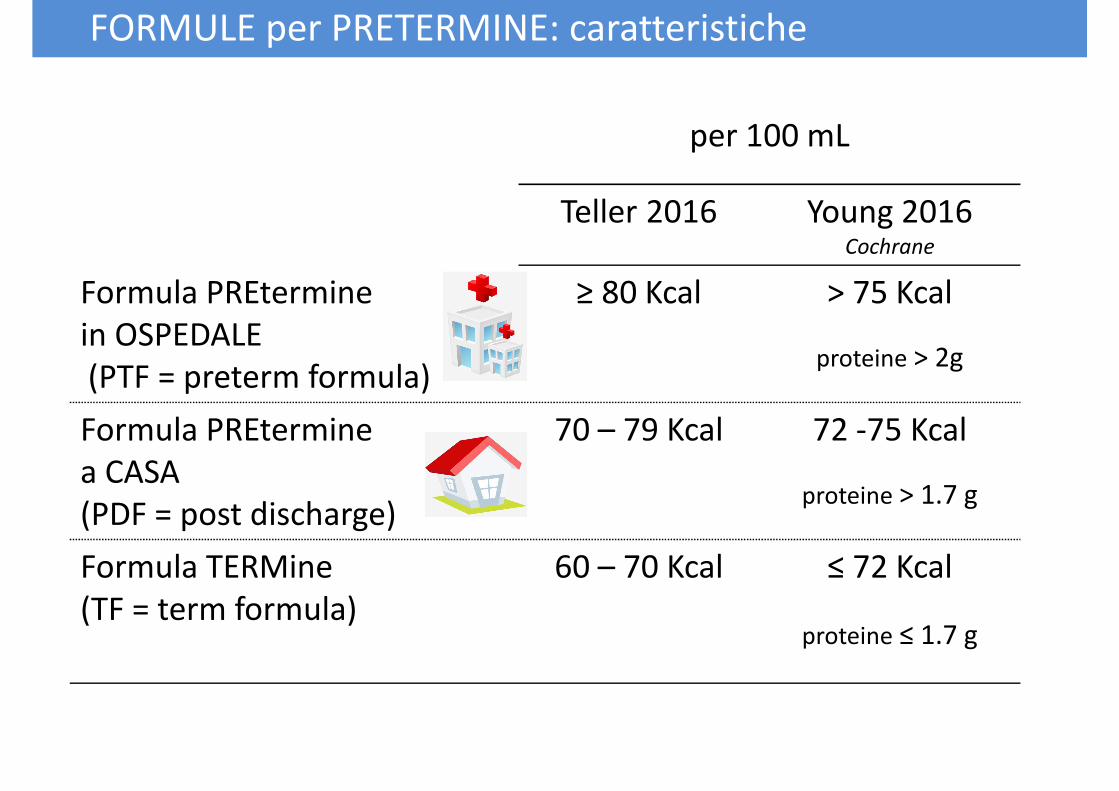
per 100 mL
Teller 2016 Young 2016Cochrane
FORMULE per PRETERMINE: caratteristiche
Formula PREtermine
in OSPEDALE
(PTF = preterm formula)
≥ 80 Kcal > 75 Kcal
proteine > 2g
Formula PREtermine
a CASA
(PDF = post discharge)
70 – 79 Kcal 72 -75 Kcal
proteine > 1.7 g(PDF = post discharge)
Formula TERMine
(TF = term formula)
60 – 70 Kcal ≤ 72 Kcal
proteine ≤ 1.7 g
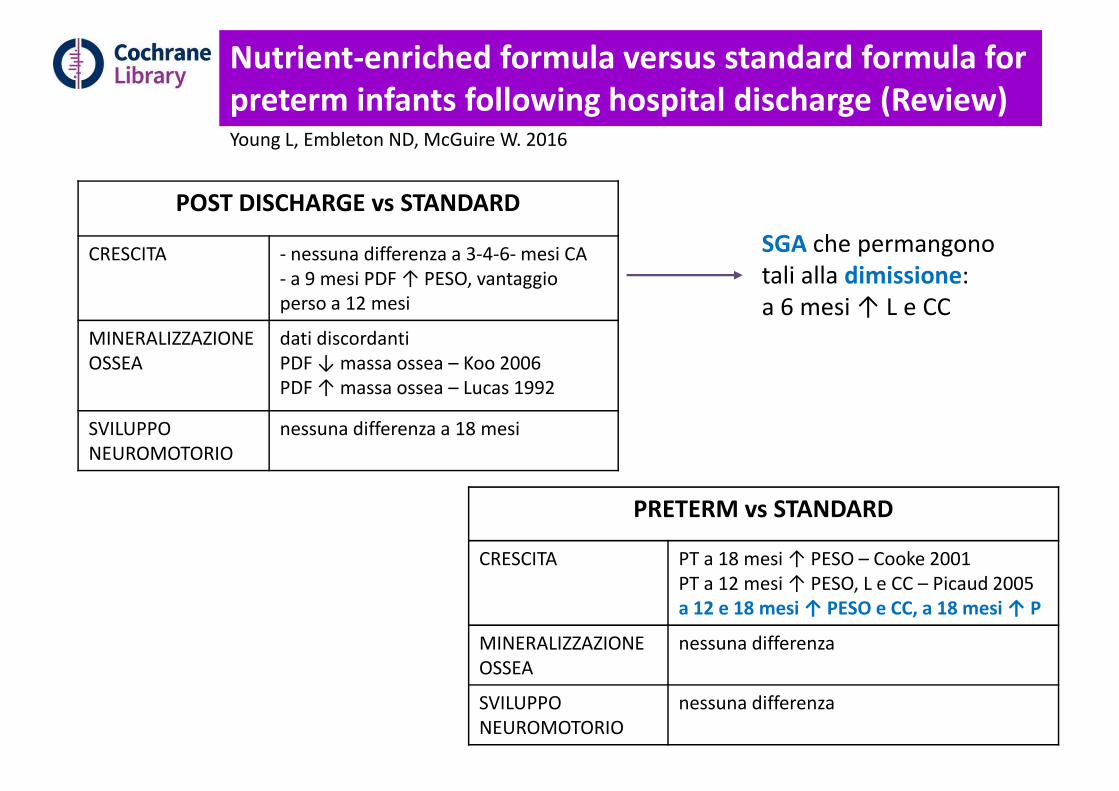
Nutrient-enriched formula versus standard formula for
preterm infants following hospital discharge (Review)Young L, Embleton ND, McGuire W. 2016
POST DISCHARGE vs STANDARD
CRESCITA - nessuna differenza a 3-4-6- mesi CA SGA che permangono
tali alla dimissione:CRESCITA - nessuna differenza a 3-4-6- mesi CA
- a 9 mesi PDF ↑ PESO, vantaggio
perso a 12 mesi
MINERALIZZAZIONE
OSSEA
dati discordanti
PDF ↓ massa ossea – Koo 2006
PDF ↑ massa ossea – Lucas 1992
SVILUPPO
NEUROMOTORIO
nessuna differenza a 18 mesi
PRETERM vs STANDARD
tali alla dimissione:
a 6 mesi ↑ L e CC
CRESCITA PT a 18 mesi ↑ PESO – Cooke 2001
PT a 12 mesi ↑ PESO, L e CC – Picaud 2005
a 12 e 18 mesi ↑ PESO e CC, a 18 mesi ↑ P
MINERALIZZAZIONE
OSSEA
nessuna differenza
SVILUPPO
NEUROMOTORIO
nessuna differenza
FORMULE per PRETERMINE
PRESCRIVERLE o NO?
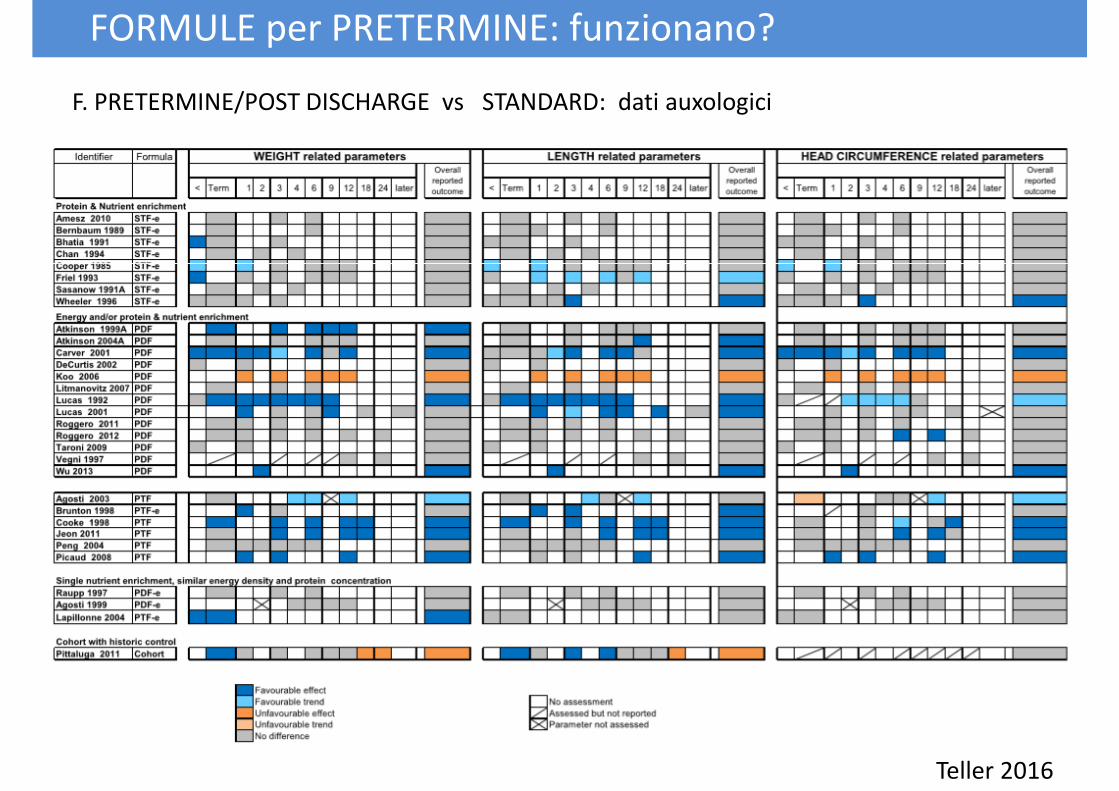
FORMULE per PRETERMINE: funzionano?
F. PRETERMINE/POST DISCHARGE vs STANDARD: dati auxologici
Teller 2016
finire
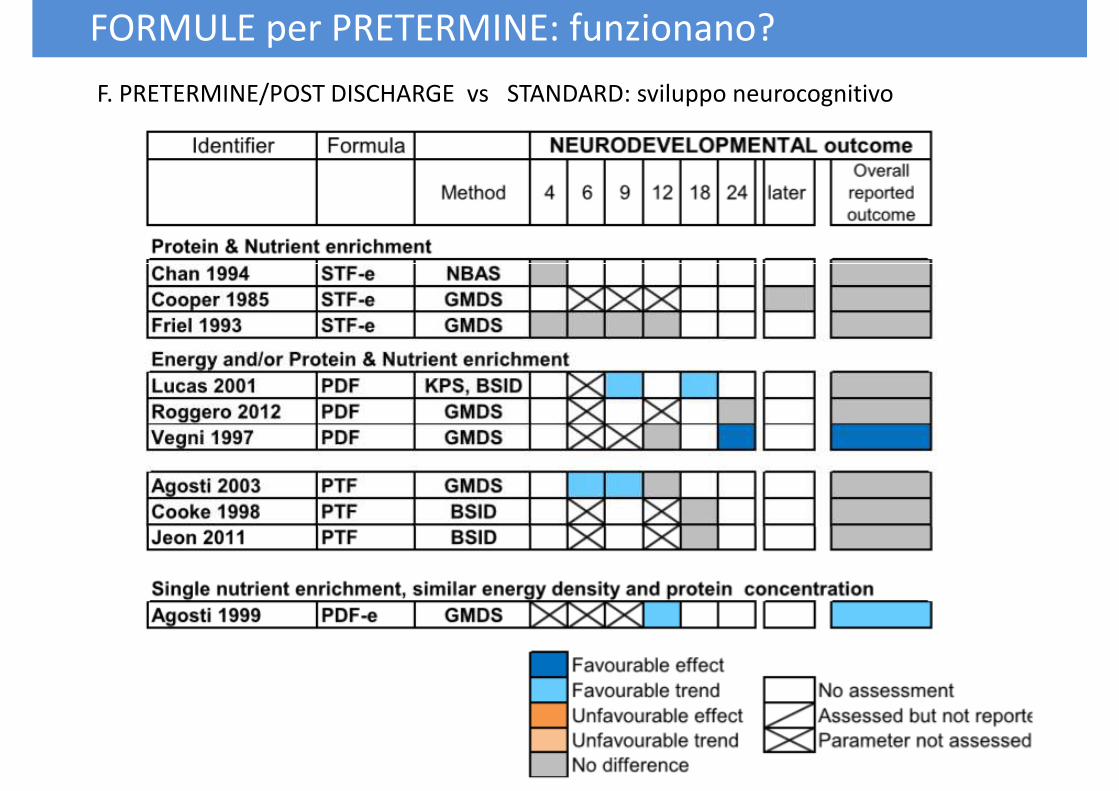
FORMULE per PRETERMINE: funzionano?
F. PRETERMINE/POST DISCHARGE vs STANDARD: sviluppo neurocognitivo
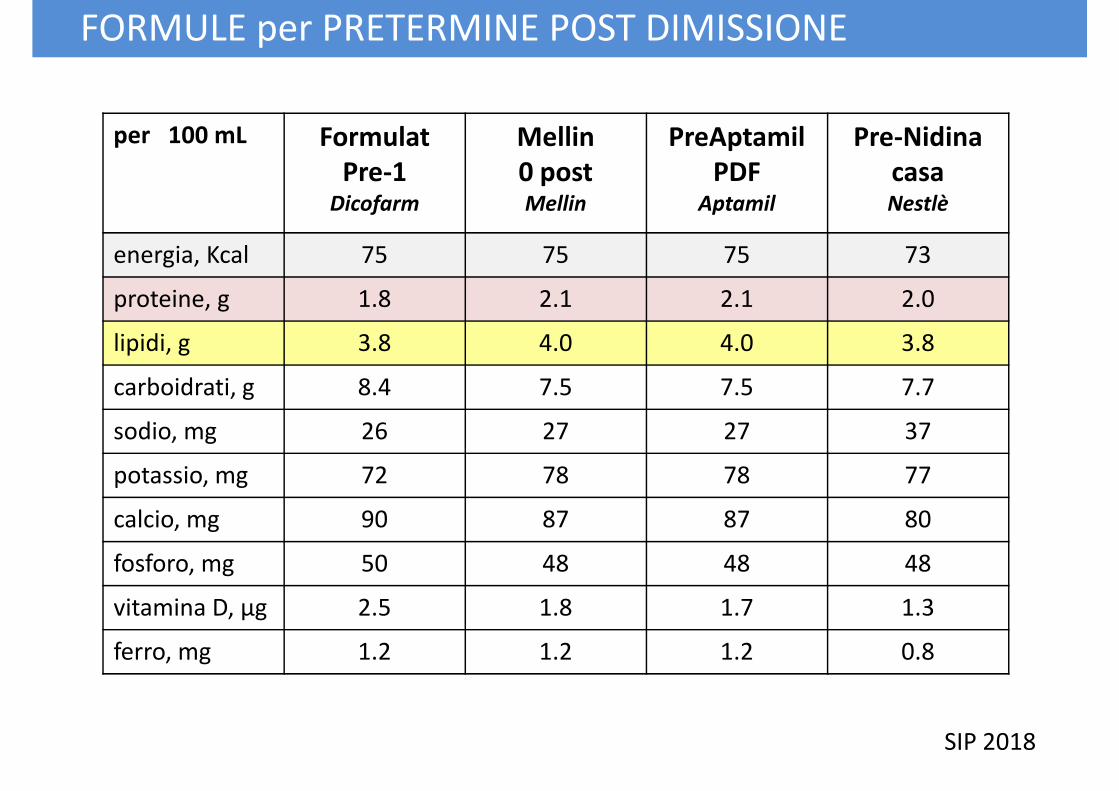
per 100 mL Formulat
Pre-1Dicofarm
Mellin
0 postMellin
PreAptamil
PDFAptamil
Pre-Nidina
casaNestlè
energia, Kcal 75 75 75 73
FORMULE per PRETERMINE POST DIMISSIONE
energia, Kcal 75 75 75 73
proteine, g 1.8 2.1 2.1 2.0
lipidi, g 3.8 4.0 4.0 3.8
carboidrati, g 8.4 7.5 7.5 7.7
sodio, mg 26 27 27 37
potassio, mg 72 78 78 77
calcio, mg 90 87 87 80calcio, mg 90 87 87 80
fosforo, mg 50 48 48 48
vitamina D, µg 2.5 1.8 1.7 1.3
ferro, mg 1.2 1.2 1.2 0.8
SIP 2018
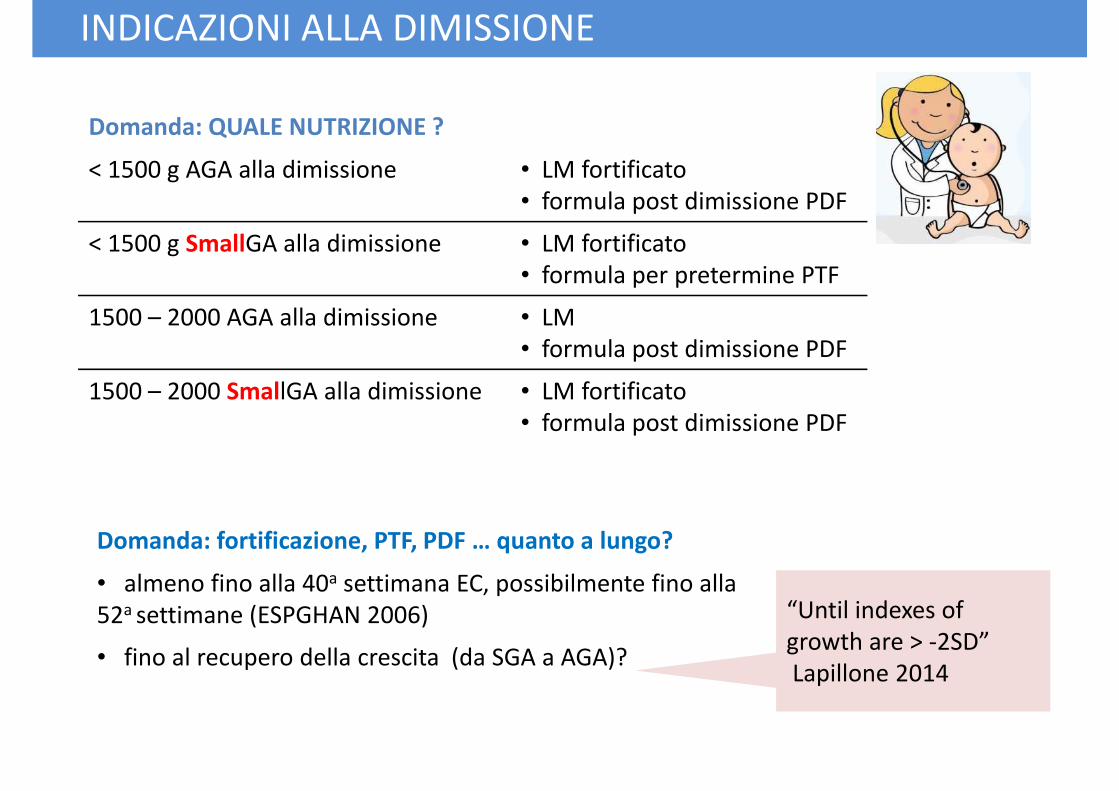
INDICAZIONI ALLA DIMISSIONE
Domanda: QUALE NUTRIZIONE ?
< 1500 g AGA alla dimissione • LM fortificato
• formula post dimissione PDF
< 1500 g SmallGA alla dimissione • LM fortificato
• formula per pretermine PTF• formula per pretermine PTF
1500 – 2000 AGA alla dimissione • LM
• formula post dimissione PDF
1500 – 2000 SmallGA alla dimissione • LM fortificato
• formula post dimissione PDF
Domanda: fortificazione, PTF, PDF … quanto a lungo?Domanda: fortificazione, PTF, PDF … quanto a lungo?
• almeno fino alla 40a settimana EC, possibilmente fino alla
52a settimane (ESPGHAN 2006)
• fino al recupero della crescita (da SGA a AGA)?
“Until indexes of
growth are > -2SD”
Lapillone 2014
INDICAZIONI ALLA DIMISSIONE
PER LA FAMIGLIA
• LM al seno: a richiesta (1.5-3h) con un’unica pausa di sonno 5h
• Se LM al seno: controllo peso 48 ore dalla dimissione
• Se LM fortificato o PDF: istruzione in ospedale sulla preparazioneSe LM fortificato o PDF: istruzione in ospedale sulla preparazione
� crescita «sana e adeguata» di un neonato pretermine dopo la dimissione:
qual’è?
Conclusioni: qualche altro dubbio …
� nutrizione = «pacchetto» di interventi: qual è il migliore?
� periodo di maggior plasticità per l’organismo: quando intervenire?
� comorbidità, difficoltà di alimentazione, scarsa crescita: come modificare
le % dei maconutrienti e il rapporto P:E?
� tecniche, approcci, parametri: come identificare anche minimi
Teller 2016
miglioramenti dell’outcome neurocognitivo?
� outcome: indicatori metabolici, composizione corporea?
� interventi precoci per favorire l’allattamento materno e
quindi al seno
Conclusioni: qualche certezza
quindi al seno
� valutazioni periodiche della crescita in follow up: peso,
lunghezza, circonferenza cranica e sviluppo psicomotorio
� follow metabolico

EG 25 sett
PN 727 g (50-75°p)
IVH 3° bilaterale
RDS -BPD
tracheomalacia -tracheomalacia -
tracheostomia
allattamento materno
esclusivo
grazie