Embed Size (px)
Citation preview

__________________________________________________________________________________________________________________________________
1
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
Get Your Life Back!Get Your Life Back!Get Your Life Back!Get Your Life Back! Reset Your Thyroid HealthReset Your Thyroid HealthReset Your Thyroid HealthReset Your Thyroid Health An organized guide to my health and wellness by Kim Wolinski, MSW “Dr. DeClutter”
This is one of two PDFs: FORMS-PDF-2. These are the FORMS that will help you stay organized with yourself and your healthcare practitioner while you are in your initial treatment for your thyroid problems and long after. The explanation of these FORMS is in the MANUAL-PDF.
PRINT these templates to use for your first consult with your doctor, and all future appointments to track how you are feeling and if the symptoms from your thyroid problem are getting better or worse. 3-HOLE PUNCH and put into a 3-RING BINDER Print a second COVER PLATE from the Manual PDF and insert in the front of your binder.
Print a second This binder belongs toThis binder belongs toThis binder belongs toThis binder belongs to template from the Manual PDF and put in as page 1.
DO NOT FORWARD OR COPY FOR OTHERSDO NOT FORWARD OR COPY FOR OTHERSDO NOT FORWARD OR COPY FOR OTHERSDO NOT FORWARD OR COPY FOR OTHERS Please do not forward PDFs or copy for others. If this system will help someone you know please give them my website link where they can purchase their personal copy! Thank you, Kim. http://thyroidu.com/bookstoreresources/ If your healthcare practitioner is interested in using this system with other patients, have them contact me at [email protected] or 303.485.5280.
Thyroid Health PlanThyroid Health PlanThyroid Health PlanThyroid Health Plan users say,users say,users say,users say,
“The forms in Get Your Life Back Thyroid Health Plan made a
huge difference in how my doctor dealt with me. She could see
exactly where I was each week and how I was feeling, even
when I was unsure how the week or two since our last
appointment was. It was all there in black and white. She said
that it was one of the best patient experiences she’d had in her
18 years of practice because I brought her all the truth about
what I’ve been going through and she could understand and
prescribe my supplements better. Thank you so much. I’m doing
so much better now and still using these forms every day!”
~ Carol, Engineer, Birmingham, AL
“I’m an organized person, but your forms helped make my life
so much easier and calmer while dealing with the overwhelming
symptoms of my thyroid problems. My doctor was really
impressed with my binder! Thank you, Kim for doing this for
me, for all of us. I hope your health continues to get better and
better too.”
~Beverly, Teacher, Dallas, TX

__________________________________________________________________________________________________________________________________
2
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
CCCCONTENTS:ONTENTS:ONTENTS:ONTENTS: FORMS ONLYFORMS ONLYFORMS ONLYFORMS ONLY (Hole punch; put in 3 ring binder for ongoing use)
You can print the whole pdf and review with the Manual, or look through it and leave some that are noted in red not to print as they are instructions only.
HEALTHCARE PRACTITIONER HEALTHCARE PRACTITIONER HEALTHCARE PRACTITIONER HEALTHCARE PRACTITIONER andandandand PHARMACY INFORMATIONPHARMACY INFORMATIONPHARMACY INFORMATIONPHARMACY INFORMATION FORMSFORMSFORMSFORMS
HEALTHCARE PRATITIONER / PHARMACY INFORMATION ........................................................................................................ 3
CURRENT PRESCRIPTIONS / MEDICATIONS ............................................................................................................................... 4 VITAMINS / MINERALS / ALTERNATIVE MEDICINES & SUPPLEMENTS........................................................................................ 5 AUTOIMMUNE DISEASE: FAMILY TREE CHECKLIST ................................................................................................................. 6-8
HYPOTHYROIDISM SYMPTOM CHECKLIST FOR DOCTOR CONSULTATION .......................................................................... 9-13 HYPERTHYROIDISM SYMPTOM CHECKLIST FOR DOCTOR CONSULTATION ...................................................................... 14-17 FYBROMYALGIA SYMPTOM CHECKLIST FOR DOCTOR CONSULTATION ............................................................................ 18-20 HYPOTHYROIDISM DOCTOR APPOINTMENT / SYMPTOM WEEKLY CHECKLIST ................................................................. 21-24 HYPERTHYROIDISM DOCTOR APPOINTMENT / SYMPTOM WEEKLY CHECKLIST ................................................................ 25-27
FOOD & EATING DOCUMENTATION (F.E.D.) Forms: Use for daily documentation and for weekly meal planning .................. 28
HYPOGLYCEMIA SYMPTOM CHECKLIST FOR DOCTOR CONSULTATION ........................................................................... 30-32 HIGH BLOOD SUGAR / INSULIN RESISTANCE CHECKLIST FOR DOCTOR CONSULTATION ..................................................... 33 DAILY MEDICATION AND SUPPLEMENT CHECKLIST ........................................................................................................... 34-35 WATER LOG ............................................................................................................................................................................. 36 EXERCISE PLAN and LOG .................................................................................................................................................... 37-38 PRACTITIONER APPOINTMENT LOG ........................................................................................................................................ 39 MASTER PRACTITIONER APPOINTMENT LOG .......................................................................................................................... 40 LAB TESTS LOG ........................................................................................................................................................................ 41 INSURANCE COMPANY / BILLINGS LOG — OVERALL DOCUMENTATION LOG ........................................................................ 42

__________________________________________________________________________________________________________________________________
3
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HEALTHCARE PRACTITIONER / PHARMACY INFORMATIONHEALTHCARE PRACTITIONER / PHARMACY INFORMATIONHEALTHCARE PRACTITIONER / PHARMACY INFORMATIONHEALTHCARE PRACTITIONER / PHARMACY INFORMATION You can staple business cards here to simplify.
Doctor/Practitioner Doctor/Practitioner Business/Office Name Phone# Phone# Fax# Email Address
Pharmacy Pharmacist Phone# Phone# Fax# Email Address

__________________________________________________________________________________________________________________________________
4
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
CURRENT CURRENT CURRENT CURRENT PRESCRIPTIONSPRESCRIPTIONSPRESCRIPTIONSPRESCRIPTIONS / MEDICATIONS (Thyroid Medications First/ MEDICATIONS (Thyroid Medications First/ MEDICATIONS (Thyroid Medications First/ MEDICATIONS (Thyroid Medications First)))) Some medicines can interfere with the absorption of thyroid medicines. Document everything.
Medicine Date Started Dosage Times Per Day
Purpose Affect on you. Is it helping?

__________________________________________________________________________________________________________________________________
5
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
VITAMINSVITAMINSVITAMINSVITAMINS //// MINERALSMINERALSMINERALSMINERALS //// ALTERALTERALTERALTERNNNNATIVE MEDICINES & SUPPLEMENTSATIVE MEDICINES & SUPPLEMENTSATIVE MEDICINES & SUPPLEMENTSATIVE MEDICINES & SUPPLEMENTS
Some vitamins and supplements can interfere with the absorption of thyroid medicines. Document everything.
Supplement Date Started Dosage Times Per Day
Purpose Affect on you. Is it helping?

__________________________________________________________________________________________________________________________________
6
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
AAAAUTOIMMUNE DISEASEUTOIMMUNE DISEASEUTOIMMUNE DISEASEUTOIMMUNE DISEASE Family TreeFamily TreeFamily TreeFamily Tree ChecklChecklChecklChecklistististist
I haveI haveI haveI have FatherFatherFatherFather MotherMotherMotherMother A GrandparentA GrandparentA GrandparentA Grandparent OthersOthersOthersOthers Related Related Related Related by Bloodby Bloodby Bloodby Blood: Aunts, : Aunts, : Aunts, : Aunts, Uncles, SiblingsUncles, SiblingsUncles, SiblingsUncles, Siblings
1. Achlorhydra AI Active Chronic Hepatitis
2. Addison's Disease
3. Alopecia Areata
4. Amyotrophic Lateral Sclerosis (ALS, Lou Gehrig's
Disease)
5. Ankylosing Spondylitis
6. Anti-GBM Nephritis or anti-TBM Nephritis
7. Antiphospholipid Syndrome
8. Aplastic Anemia
9. Arthritis (over 100 kinds)
10. Asthma
11. Atopic Allergy
12. Atopic Dermatitis
13. Autoimmune Inner Ear Disease (AIED)
14. Autoimmune Lymphoproliferative Syndrome (ALPS)
15. Balo Disease
16. Behcet's Disease
17. Berger's Disease (IgA Nephropathy)
18. Bullous Pemphigoid
19. Cardiomyopathy
20. Celiac Disease/Gluten Intolerant
21. Chronic Fatigue Immune Dysfunction Syndrome
(CFIDS)
22. Churg Strauss Syndrome
23. Cicatricial Pemphigoid
24. Cogan's Syndrome
25. Cold Agglutunin Disease
26. Colitis
27. Cranial Arteritis
28. CREST Syndrome
29. Crohn's Disease

__________________________________________________________________________________________________________________________________
7
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
30. Cushing's Syndrome
31. Dego's Disease
32. Dermatitis
33. Dermatomyositis
34. Devic Disease
35. Diabetes, Type 1
36. Diabetes, Type 2
37. Dressler's Syndrome
38. Discoid Lupus
39. Eczema
40. Essential Mixed Cryoglobulinemia
41. Eosinophilic Fasciitis
42. Epidermolysis Bullosa Acquisita
43. Evan's Syndrome
44. Fibromyalgia
45. Fibromyositis
46. Fibrosing Alveolitis
47. Gastritis
48. Giant Cell Artertis
49. Glomerulonephritis
50. Goodpasture's Disease
51. Grave's Disease (Hyperthyroid)
52. Guillian-Barre Syndrome
53. Hashimoto's Thyroiditis (Hypothyroid)
54. Hemolytic Anemia
55. Henoch-Schonlein Purpura
56. Hepatitis
57. Hughes Syndrome
58. Idiopathic Adrenal Atrophy
59. Idiopathic Pulmonary Fibrosis
60. Idiopathic Thrombocytopenia Purpura
61. Inflammatory Demylinating Polyneuropathy
62. Irritable Bowel Syndrome
63. Kawasaki's Disease
64. Lichen Planus
65. Lou Gehrig's Disease
66. Lupoid Hepatitis
67. Lupus

__________________________________________________________________________________________________________________________________
8
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
68. Lyme Disease
69. Meniere's Disease
70. Mixed Connective Tissue Disease
71. Multiple Myeloma
72. Multiple Sclerosis (MS)
73. Myasthenia Gravis
74. Myositis
75. Ocular Cicatricial Pemphigoid
76. Osteoporosis
77. Pars Planitis
78. Pemphigus Vulgaris
79. Polyglandular Autoimmune Syndromes
80. Polymyalgia Rheumatica (PMR)
81. Polymyositis
82. Primary Biliary Cirrhois
83. Primary Sclerosing Cholangitis
84. Psoriasis
85. Raynaud's Phenomenon
86. Reiter's Syndrome
87. Rheumatic Fever
88. Rheumatoid Arthritis
89. Sarcoidosis
90. Scleritis
91. Scleroderma
92. Sjogren's Syndrome
93. Sticky Blood Syndrome
94. Still's Disease
95. Stiff Man Syndrome
96. Sydenham Chorea
97. Systemic Lupus Erythmatosis (SLE)
98. Takayasu's Arteritis
99. Temporal Arteritis
100. Ulcerative Colitis
101. Vasculitis
102. Vitiligo
103. Wegener's Granulomatosis
104. Wilson's Syndrome (Thyroid Disorder)

__________________________________________________________________________________________________________________________________
9
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HYPOHYPOHYPOHYPOTHYROIDTHYROIDTHYROIDTHYROIDISISISISM SYMPTOM M SYMPTOM M SYMPTOM M SYMPTOM CHECKLISTCHECKLISTCHECKLISTCHECKLIST FOR DOCTOR CONSULTATIONFOR DOCTOR CONSULTATIONFOR DOCTOR CONSULTATIONFOR DOCTOR CONSULTATION
If you’re not sure if you have HYPO- or HYPERthyroidism, you can fill out both lists. Some symptoms are the same for each, but other symptoms are very specific to that condition.
If you already know you have HYPOthyroidism or Hashimoto’s Disease, this will be the list to complete. After completing the following questions and Symptom List, copy and give the copy to your practitioner in your consultation for their use and file.
1. Have you been diagnosed with hypothyroidism? Explain.
2. Have you been diagnosed with Hashimoto’s Disease? Explain.
3. Do you still have your full 2-sided thyroid? If not, explain (include year, why, where, etc.):
4. What thyroid medications, if any, are you taking? The kind/name? Dosage?
5. When did you start taking it?

__________________________________________________________________________________________________________________________________
10
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HYPOHYPOHYPOHYPOTHYROIDTHYROIDTHYROIDTHYROIDISM ISM ISM ISM SymptomSymptomSymptomSymptom CheckCheckCheckCheckllllistististist
Mark 0Mark 0Mark 0Mark 0----10 for your pain or symptom level10 for your pain or symptom level10 for your pain or symptom level10 for your pain or symptom level and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.
0 = no pain or 0 = no pain or 0 = no pain or 0 = no pain or symptoms to 10 symptoms to 10 symptoms to 10 symptoms to 10 = = = = extreme pain or full symptomsextreme pain or full symptomsextreme pain or full symptomsextreme pain or full symptoms ENERGY & SLEEPENERGY & SLEEPENERGY & SLEEPENERGY & SLEEP
1. Chronic fatigue and sluggishness
2. Lethargy
3. Excessive sleepiness
4. Waking up at night/can’t fall back to sleep
5. Decreased concentration/”Foggy” brain
6. Forgetfulness: Poor short-term memory and forgetfulness
7. Difficulty making decisions
STABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESS
8. Dizziness
9. Anxiety
10. Panic
11. Depression/apathy
12. Mood swings/crying unexpectedly
13. Feelings of worthlessness
14. Losing interest in normal daily activities
15. Suicidal thoughts
METABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODY
16. Increased sensitivity to cold/cold intolerance/chills
17. Cold hands and feet

__________________________________________________________________________________________________________________________________
11
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
18. Low body temperature
19. Constipation
20. Unexplained weight gain, most of which is fluid; difficulty losing weight
SKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILS
21. Pale, dry skin
22. Thinning, dull hair
23. Dry, brittle, coarse hair
24. Premature graying of hair
25. Loss of eyebrows from outside in
26. Ridged, brittle/think fingernails
27. Fungal infection of nails
28. Slight rosiness/reddening of face
BODY CHANGESBODY CHANGESBODY CHANGESBODY CHANGES
29. Puffy face
30. Blurred vision
31. Gritty, burning dry eyes
32. Eyes sensitive to light
33. Eyes get jumpy/tics in eyes, which makes me dizzy/vertigo and have headaches
34. Swelled tongue -indentations on sides from teeth
35. Fungal infection of mouth
36. Dowagers Hump
37. Swelled feet, ankles, legs
38. Tinnitus (ringing in ears)

__________________________________________________________________________________________________________________________________
12
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
39. Vague aches and pains
40. Muscle aches, tenderness and stiffness, especially in shoulders and hips
41. Pain and stiffness in joints
42. Swelling of the legs / in knees or the small joints in hands and feet
43. Muscle weakness, especially in lower extremities
44. Tingling in lower legs / below knees
45. Recurrent sinus infections
46. Cramping of toes, stabbing feeling in pads of toes
47. Getting more frequent infections that last longer
48. Sagging eye lids
49. Hoarse voice/rough-deeper
50. Loose skin under upper arms
51. Loose skin under chin
52. Loose, sagging skin at midsection
53. Heart palpitations
54. Loss of libido, lack of sex drive
55. Feel the need to yawn to get oxygen
56. Bloody nose
57. Elevated blood cholesterol level
58. Strange feelings in neck or throat
HORMONALHORMONALHORMONALHORMONAL
59. Women: Heavier than normal periods / Excessive or prolonged menstrual bleeding (menorrhagia) and pain.
60. Women: Loss of menstrual cycle.

__________________________________________________________________________________________________________________________________
13
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
61. Women: Hot flashes
62. Women: Infertility/miscarriage
HYPOGLYCEMIA HYPOGLYCEMIA HYPOGLYCEMIA HYPOGLYCEMIA (Can be directly linked to hypothyroidism)
63. Crave sugary carbohydrates
64. Crave bread, pasta/sour dough bread/butter
65. Crave chocolate and sweets
66. Black outs due to sugar
67. Eyes get light spots /migraines
ADD ADD ADD ADD ANY YOU EXPERIENCE NOT LISTEDANY YOU EXPERIENCE NOT LISTEDANY YOU EXPERIENCE NOT LISTEDANY YOU EXPERIENCE NOT LISTED

__________________________________________________________________________________________________________________________________
14
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HYPHYPHYPHYPERERERERTHYROIDTHYROIDTHYROIDTHYROIDISMISMISMISM SYMPTOM CHECKSYMPTOM CHECKSYMPTOM CHECKSYMPTOM CHECKLISTLISTLISTLIST FOR DOCTOR CONSULTATIONFOR DOCTOR CONSULTATIONFOR DOCTOR CONSULTATIONFOR DOCTOR CONSULTATION If you already know you have HYPERthyroidism or Graves’ Disease, this will be the list to complete. After completing the following questions and Symptom List, copy and give the copy to your practitioner in your consultation for their use and file.
1. Have you been diagnosed with hyperthyroidism? Explain.
2. Have you been diagnosed with Graves' Disease? Explain.
3. Have you been diagnosed with a Goiter? Explain.
4. Do you still have your full 2-sided thyroid? If not, explain (include year, why, where, etc.):
5. What thyroid medications, if any, are you taking? The kind/name? Dosage?
6. When did you start taking it?

__________________________________________________________________________________________________________________________________
15
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HYPERHYPERHYPERHYPERTHYROIDTHYROIDTHYROIDTHYROIDISMISMISMISM Symptom CheckSymptom CheckSymptom CheckSymptom Checkllllistististist
Mark 0Mark 0Mark 0Mark 0----10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.
0 = no pain or 0 = no pain or 0 = no pain or 0 = no pain or symptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptoms ENERGY & SLEEPENERGY & SLEEPENERGY & SLEEPENERGY & SLEEP
1. Irritability
2. Insomnia: difficulty getting to sleep, staying asleep, or going back to sleep after awakening in the middle of the night
3. Excessive sleepiness
4. Feel fatigued, exhausted
STABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESS
5. Nervousness: a lot of nervous energy that I need to burn off
6. Irritable
7. Panic disorder
8. Moods change easily
9. Difficulty concentrating or focusing
10. Can't seem to remember things
11. Depressed
12. Vertigo
13. Some lightheadedness
METABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODY
14. Heat sensitivity: feeling inappropriately hot or overheated
15. Increased perspiration
16. Stomach upset
17. Diarrhea

__________________________________________________________________________________________________________________________________
16
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
18. Bowel movement frequently
19. Unexplained weight loss
20. Losing weight but my appetite has increased
21. Weight gain: hyperthyroidism can cause both weight loss and gain depending on balance of appetite changes vs metabolism changes
SKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILS
22. Warm skin
23. Skin: coarse, dry, scaly, thinning
24. Hair: coarse and dry, breaking, brittle
25. Fine hair
26. Thinning of hair
27. Hair is falling out
BODY CHANGESBODY CHANGESBODY CHANGESBODY CHANGES
28. Goiter
29. Flushing
30. Eye/vision changes
31. Eyes feel sensitive to light
32. Eyes feel gritty and dry
33. Eyes seem to be enlarging, or getting more "bug-eyed" looking
34. Eyes get jumpy/tics in eyes, which makes me dizzy/vertigo and have headaches
35. Itchy skin
36. Rapid heartbeat, racing heart

__________________________________________________________________________________________________________________________________
17
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
37. Heart palpitations
38. Breathlessness: feel shortness of breath and tightness in the chest
39. Pulse is unusually fast
40. Hand tremors, shaky hands
41. Muscular weakness: especially involving the
upper arms and thighs
42. Weak leg muscles
43. Recurrent sinus infections
44. Getting more frequent infections, that last longer
45. Strange feelings in neck or throat
HORMONALHORMONALHORMONALHORMONAL
46. Women: Lighter than normal periods
47. Women: Decreased menstruation
48. Women: Period stops
49. Women: Miscarriages
50. Women: Hard time getting pregnant
51. Severe menstrual cramps
52. Women or men: No sex drive, or am having sexual performance problems
ADD ADD ADD ADD ANY YOU EXPERIENCE NOT LISTEDANY YOU EXPERIENCE NOT LISTEDANY YOU EXPERIENCE NOT LISTEDANY YOU EXPERIENCE NOT LISTED

__________________________________________________________________________________________________________________________________
18
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
FYBROMYALGIAFYBROMYALGIAFYBROMYALGIAFYBROMYALGIA Symptom ChecklSymptom ChecklSymptom ChecklSymptom Checklistististist
Mark 0Mark 0Mark 0Mark 0----10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.
0 = no pain or 0 = no pain or 0 = no pain or 0 = no pain or symptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptoms ENERGY & SLEEPENERGY & SLEEPENERGY & SLEEPENERGY & SLEEP
1. Fatigue, unrefreshing sleep, waking up tired, morning stiffness
2. Insomnia, frequent waking, difficulty falling asleep, or falling asleep immediately
3. Anxiety, depression and "fibrofog"or “fog brain”:The term used to describe the confusion and forgetfulness, inability to concentrate and difficulty recalling simple words and numbers, and transposing words and numbers
4. Difficulty remembering, concentrating, and performing simple mental tasks
5. Difficulty making decisions
STABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESS
6. Moderate or severe fatigue and decreased energy
7. Balance problems
8. Neurally mediated hypotension: When you stand up, your blood pressure drops, which can make you feel faint, dizzy, nauseous, your heart rate drops, and you can even pass out
9. Dizziness
10. Tension or migraine headaches
11. Feeling anxious or depressed

__________________________________________________________________________________________________________________________________
19
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
BODYBODYBODYBODY----MUSCLESMUSCLESMUSCLESMUSCLES----PAINPAINPAINPAIN
12. Headaches, tenderness of the scalp, pain in the back of the skull
13. Jaw and facial tenderness
14. Feeling of pain, burning, aching, and soreness in the body
15. Chronic muscle pain, muscle spasms or tightness, weakness in the limbs, and leg cramps
16. Pain in the neck, shoulder, shoulder blades and elbows
17. Pain in hips, top of buttocks, outside the lower hip, below buttocks, and the pelvis
18. Pain in the knees and kneecap area
19. Reduced tolerance for exercise and muscle pain after exercise
20. Chest pain, palpitations
21. Restless leg syndrome
22. Muscle twitching
23. Numbness or tingling in the face, arms, hands, legs, or feet
METABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODY
24. Raynaud's phenomenon (where your hands feel cold, numb, or turn blue, when exposed to temperature changes)
25. Sense of tissues feeling swollen
26. Sensitivity to one or more of the following: odors, noise, bright lights, medications, certain foods, and cold
27. Shortness of breath

__________________________________________________________________________________________________________________________________
20
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
28. Abdominal pain, bloating, nausea, and constipation alternating with diarrhea (irritable bowel syndrome)
BODY CHANGESBODY CHANGESBODY CHANGESBODY CHANGES
29. Irritable bowel syndrome, diarrhea and constipation, bloating, cramping
30. Numbness, tingling and feeling of cold in the hands and feet
31. Frequent urination
32. Dry mouth
33. Stiffness upon waking or after staying in one position for too long
34. Increase in urinary urgency or frequency (irritable bladder)
HORMONALHORMONALHORMONALHORMONAL
35. Women: Painful periods
ADD ANY YOU EXPERIENCE NOT LISTEDADD ANY YOU EXPERIENCE NOT LISTEDADD ANY YOU EXPERIENCE NOT LISTEDADD ANY YOU EXPERIENCE NOT LISTED

__________________________________________________________________________________________________________________________________
21
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
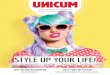
DOCTOR APPOINTMENT / SYMPTOM DOCTOR APPOINTMENT / SYMPTOM DOCTOR APPOINTMENT / SYMPTOM DOCTOR APPOINTMENT / SYMPTOM WEEKLY WEEKLY WEEKLY WEEKLY CHECKCHECKCHECKCHECKLISTLISTLISTLIST (An example: You don’t need to print.) The following is the list of symptoms with spaces to the right for each of your doctor appointments. Even if you don’t see your doctor weekly, it’s good to keep this documentation on a weekly basis so that you really see what’s changing or not and your doctor can treat you accordingly. FILL IN: The appointment dates at the top, including your weight (because, if you are going to be on the thyroid diet, you will most likely be losing
weight!) and then for each symptom mark 0 -10: 0 = no pain or symptoms to 10 = extreme pain or full symptoms. This way, you are keeping track of your symptoms getting better or worse with the treatment plan your doctor prescribes, giving him/her ongoing feedback to help regulate the changes necessary for your best outcome. I find it helpful to fill this in the night before my appointment. COPY IT: Make a copy of your first one filled in and give to the doctor for their chart. Then, every time you go in for an appointment, fill in their copy too and you’ll both be on the same page!
Here is an example sheetHere is an example sheetHere is an example sheetHere is an example sheet....
HYPOHYPOHYPOHYPOTHYROIDISMTHYROIDISMTHYROIDISMTHYROIDISM Symptom Symptom Symptom Symptom ChecklChecklChecklChecklistististist
10 / 28
Wk 1
/
/
/
/
/
/
/
/
/
/
/
/
/
WEIGHTWEIGHTWEIGHTWEIGHT 192
ENERGY & SLEEPENERGY & SLEEPENERGY & SLEEPENERGY & SLEEP
1. Chronic fatigue and sluggishness
2. Lethargy
3. Excessive sleepiness
4. Waking up at night/can’t fall back to sleep
5. Decreased concentration/”Foggy” brain
6. Forgetfulness: Poor short-term memory and forgetfulness
7. Difficulty making decisions
STABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESS
8. Dizziness
Date at top. Example: 10 (October) / 28 Under it is the number of the appointment or session (1 for the first one), keeping it easy to know how many appointments you’ve had. Some Drs have a set amount of appointments, so it’s easy to see and remember this way. I find it best to keep this up weekly, even when I don’t have an appointment. The future dates are left blank for you to pencil in before you get to the appointment —fill in the night before so you don’t forget and get rushed.
Write in each symptom box for that week before you go to see your doctor for that weeks or next appointment. If a symptom is gone (yea!) still put 0 or a line “-“ in the box. Hopefully, you’ll see the symptoms marked 10 going down to 0s in more and
more boxes as you move to the right of the list! The next pages are yours to use.
This list ends at 13 weeks.
Print out another and write in 14 where the “1” is on this one and
keep going.

__________________________________________________________________________________________________________________________________
22
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HYPOHYPOHYPOHYPOTHYROIDTHYROIDTHYROIDTHYROIDISM ISM ISM ISM SymptomSymptomSymptomSymptom ChecklChecklChecklChecklistististist
/
1
/
/
/
/
/
/
/
/
/
/
/
/
WeightWeightWeightWeight
ENERGY & SLEEPENERGY & SLEEPENERGY & SLEEPENERGY & SLEEP
1. Chronic fatigue and sluggishness
2. Lethargy
3. Excessive sleepiness
4. Waking up at night/can’t fall back to sleep
5. Decreased concentration/”Foggy” brain
6. Forgetfulness: Poor short-term memory and forgetfulness
7. Difficulty making decisions
STABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESS
8. Dizziness
9. Anxiety
10. Panic
11. Depression/apathy
12. Mood swings/crying unexpectedly
13. Feelings of worthlessness
14. Losing interest in normal daily activities
15. Suicidal thoughts
METABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODY
16. Increased sensitivity to cold/cold intolerance/chills
17. Cold hands and feet
18. Low body temperature
19. Constipation

__________________________________________________________________________________________________________________________________
23
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
Write in week numbers here-->
20. Unexplained weight gain, most of which is fluid; difficulty losing weight
SKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILS
21. Pale, dry skin
22. Thinning, dull hair
23. Dry, brittle, coarse hair
24. Premature graying of hair
25. Loss of eyebrows from outside in
26. Ridged, brittle/think fingernails
27. Fungal infection of nails
28. Slight rosiness/reddening of face
BODY CHANGESBODY CHANGESBODY CHANGESBODY CHANGES
29. Puffy face
30. Blurred vision
31. Gritty, burning dry eyes
32. Eyes sensitive to light
33. Eyes get jumpy/tics in eyes, which makes me dizzy/vertigo and have headaches
34. Swelled tongue -indentations on sides from teeth
35. Fungal infection of mouth
36. Dowagers Hump
37. Swelled feet, ankles, legs
38. Tinnitus (ringing in ears)
39. Vague aches and pains
40. Muscle aches, tenderness and stiffness, especially in shoulders and hips
41. Pain and stiffness in joints
42. Swelling of the legs / in knees or the small joints in hands and feet

__________________________________________________________________________________________________________________________________
24
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
Write in week numbers here-->
43. Muscle weakness, especially in lower extremities
44. Tingling in lower legs / below knees
45. Recurrent sinus infections
46. Cramping of toes, stabbing feeling in pads of toes
47. Getting more frequent infections that last longer
48. Sagging eye lids
49. Hoarse voice/rough-deeper
50. Loose skin under upper arms
51. Loose skin under chin
52. Loose, sagging skin at midsection
53. Heart palpitations
54. Loss of libido, lack of sex drive
55. Feel the need to yawn to get oxygen
56. Bloody nose
57. Elevated blood cholesterol level
58. Strange feelings in neck or throat
HORMONALHORMONALHORMONALHORMONAL
59. Women: Heavier than normal periods / Excessive or prolonged menstrual bleeding (menorrhagia) and pain.
60. Women: Loss of menstrual cycle.
61. Women: Hot flashes
62. Women: Infertility/miscarriage
ADD ADD ADD ADD ANY YOU EXPERIENCE NOT ANY YOU EXPERIENCE NOT ANY YOU EXPERIENCE NOT ANY YOU EXPERIENCE NOT LISTEDLISTEDLISTEDLISTED

__________________________________________________________________________________________________________________________________
25
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HYPERHYPERHYPERHYPERTHYROIDTHYROIDTHYROIDTHYROIDISMISMISMISM Symptom CheckSymptom CheckSymptom CheckSymptom Checkllllistististist
/
1
/
/
/
/
/
/
/
/
/
/
/
/
WeightWeightWeightWeight
ENERGY & SLEEPENERGY & SLEEPENERGY & SLEEPENERGY & SLEEP
1. Irritability
2. Insomnia: difficulty getting to sleep, staying asleep, or going back to sleep after awakening in the middle of the night
3. Excessive sleepiness
4. Feel fatigued, exhausted
STABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESSSTABILITY & STRESS
5. Nervousness: a lot of nervous energy that I need to burn off
6. Irritable
7. Panic disorder
8. Moods change easily
9. Difficulty concentrating or focusing
10. Can't seem to remember things
11. Depressed
12. Vertigo
13. Some lightheadedness
METABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODYMETABOLISM/BODY
14. Heat sensitivity: feeling inappropriately hot or overheated
15. Increased perspiration
16. Stomach upset
17. Diarrhea

__________________________________________________________________________________________________________________________________
26
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
Write in week numbers here-->
18. Bowel movement frequently
19. Unexplained weight loss
20. Losing weight but my appetite has increased
21. Weight gain: hyperthyroidism can cause both weight loss and gain depending on balance of appetite changes vs metabolism changes
SKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILSSKIN/HAIR/NAILS
22. Warm skin
23. Skin: coarse, dry, scaly, thinning
24. Hair: coarse and dry, breaking, brittle
25. Fine hair
26. Thinning of hair
27. Hair is falling out
BODY CHANGESBODY CHANGESBODY CHANGESBODY CHANGES
28. Goiter
29. Flushing
30. Eye/vision changes
31. Eyes feel sensitive to light
32. Eyes feel gritty and dry
33. Eyes seem to be enlarging, or getting more "bug-eyed" looking
34. Eyes get jumpy/tics in eyes, which makes me dizzy/vertigo and have headaches
35. Itchy skin
36. Rapid heartbeat, racing heart
37. Heart palpitations
38. Breathlessness: feel shortness of breath and tightness in the chest

__________________________________________________________________________________________________________________________________
27
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
Write in week numbers here-->
39. Pulse is unusually fast
40. Hand tremors, shaky hands
41. Muscular weakness: especially
involving the upper arms and thighs
42. Weak leg muscles
43. Recurrent sinus infections
44. Getting more frequent infections, that last longer
45. Strange feelings in neck or throat
HORMONALHORMONALHORMONALHORMONAL
46. Women: Lighter than normal periods
47. Women: Decreased menstruation
48. Women: Period stops
49. Women: Miscarriages
50. Women: Hard time getting pregnant
51. Severe menstrual cramps
52. Women or men: No sex drive, or am having sexual performance problems
ADD ANY YOU EXPERIENCE NOT ADD ANY YOU EXPERIENCE NOT ADD ANY YOU EXPERIENCE NOT ADD ANY YOU EXPERIENCE NOT LISTEDLISTEDLISTEDLISTED

__________________________________________________________________________________________________________________________________
28
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
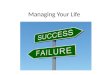
FOOD & EATING DOCUMENTATION (FFOOD & EATING DOCUMENTATION (FFOOD & EATING DOCUMENTATION (FFOOD & EATING DOCUMENTATION (F....EEEE....DDDD....) ) ) ) ---- LogLogLogLog in a spiral notebookin a spiral notebookin a spiral notebookin a spiral notebook Use to write in as you eat and for preplanning your menu.Use to write in as you eat and for preplanning your menu.Use to write in as you eat and for preplanning your menu.Use to write in as you eat and for preplanning your menu.
Day/Date Time awake / Line down the middle of the page.Line down the middle of the page.Line down the middle of the page.Line down the middle of the page. Time actually up for day I do the same on this side of the notebook page. Two to a page.
The next day I flip the page, and on the back do it all again! 9 a.m. Green Smoothie: 2-3 cups of spinach Protein powder Almond milk Banana Flaxseeds
11:30 Hot herbal tea Rice crackers Almond butter 1:30 Ate at China Buffet (YUM!) Shrimp: Grilled and boiled Grilled chicken on a stick Veggies
Bacon wrapped crab Honeydew / Watermelon Lemon water 6:00 Baked chicken breast P Bed of spinach V
Carrots V Onions V Flaxseeds Fb/O Butter O 9:00 Cantaloupe
Almonds
Bottom of page: Ex: (for exercise) Mel: Y/N (for if I took Melatonine)
Note what I did. Bed: (Time went to bed) BM: 0 1 2 3 (Bowel Movement, circle one or just put #)
TIME: The reason I have the time/time is because one of the symptoms of thyroid problems is not being able to sleep, plus, the first one is usually to go to the bathroom! If I stay awake and can’t go back to sleep, I note that too.
I don’t write “breakfast/lunch/dinner,” I just mark the times I eat and what I eat. You certainly can however if it helps you keep or create a healthy eating pattern.
It can also be helpful to put initials next to each food to check and see if you’re getting a balance of fruit, vegetables, protein, etc in for the day. P — Protein M — Meat Fs — Fish N — Nuts L — Legumes (Protein and Fiber) F — Fruit V — Vegetable Fb- Fiber O — Oil
Bowel Movement (BM) Okay, who likes to talk about this! However, one of the nasty symptoms of thyroid disease is constipation. So, when my doctor had me take a “stool sample”* lab test (it’s a good thing!) I noticed that the lab paperwork showed three little illustrations of what should identify one’s poo. Use 0-3 to identify your BM activity. #0: No BM at all; might feel bloated and like you have
to go, but it won’t come out. #1: constipation poo: separate globs that look like
rabbit pellets, roundish balls that are hard to release and can take a while. I hate these!!
#2: a better/healthier poo: softer and smoother but still
had some round rabbit pellets in it. #3: “Normal” healthy poo: softish and, as Dr. Oz says
on Oprah, “Has that little swirl at the end like ice cream from a machine!” And, this would move smoothly and right out of you without pushing or working at it. That’s where we want to be!
*STOOL SAMPLE: Numerous things can affect our immune system in a way that impacts blood sugar and digestion–causing bloating–these include parasites, pathogens, infections and heavy metal and chemical toxicities. A stool sample, saliva tests and other lab tests can help detect these to then eliminate them.

__________________________________________________________________________________________________________________________________
29
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
Date:
Date:
Date:
Breakfast
Breakfast
Breakfast
Snack
Snack
Snack
Lunch
Lunch
Lunch
Snack
Snack
Snack
Dinner
Dinner
Dinner
Snack Water
Snack Water
Snack Water
Water: G G G G G G G G G
Vegetables________
Fruits________ Protein: Meat/Fish________
Milk Substitute: Almond Milk/Rice/Other________ Fat/Oils________ Fiber________
Water: G G G G G G G G G
Vegetables________
Fruits________ Protein: Meat/Fish________
Milk Substitute: Almond Milk/Rice/Other________ Fat/Oils________
Fiber________
Water: G G G G G G G G G
Vegetables________
Fruits________ Protein: Meat/Fish________
Milk Substitute: Almond Milk/Rice/Other________ Fat/Oils________
Fiber________

__________________________________________________________________________________________________________________________________
30
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HYPOGLYCEMIAHYPOGLYCEMIAHYPOGLYCEMIAHYPOGLYCEMIA Symptom CheckSymptom CheckSymptom CheckSymptom Checkllllistististist
Mark 0Mark 0Mark 0Mark 0----10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.
0 = no pain or 0 = no pain or 0 = no pain or 0 = no pain or symptoms to 10 = symptoms to 10 = symptoms to 10 = symptoms to 10 = extreme pain or full symptomsextreme pain or full symptomsextreme pain or full symptomsextreme pain or full symptoms 1. Craving sweets and simple carbohydrates
2. Constant hunger, even right after a meal
3. Irritability if meals are missed
4. Become lightheaded if meals are missed
5. Dependency on coffee for energy
6. Eating to relieve fatigue
7. Feeling shaky, jittery or tremulous (tremors)
8. Unexplained tiredness/Exhaustion
9. Gasping for breath
10. Smothering spell
11. Feeling agitated and nervous
12. Heart palpitations
13. Sighing and yawning
14. Constant worrying
15. Depression
16. Sweating and/or cold sweats
17. Skin conditions

__________________________________________________________________________________________________________________________________
31
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
18. Becoming upset easily: Outbursts of anger, feeling out of control emotionally
19. Unsocial, asocial, or antisocial behavior
20. Phobias
21. Fears
22. Confusion, abnormal behavior or both, such as the inability to complete routine tasks
23. Suicidal impulses
24. Nervous breakdowns
25. Lack of sex drive/libido
26. MALES: Impotency
27. Feeling weepy, crying for no reason, or more emotionally sensitive to everything
28. Light-headed, dizziness, faintness
29. Literally saying a different word in a sentence than you were going to say
30. Lack of coordination
31. Staggering
32. Fog-brain, poor memory, forgetfulness
33. Blackouts — can’t remember that you did something though were completely awake and doing it. (Blackout are usually attributed to alcoholism.)
34. Seizures, though uncommon
35. Convulsions
36. Vertigo

__________________________________________________________________________________________________________________________________
32
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
37. Night terrors
38. Numbness
39. Muscle pain
40. Twitching and jerking muscles
41. Muscle cramps
42. Arthritis
43. Asthma / Allergies
44. Loss of consciousness, though uncommon
45. Visual disturbances, such as double vision and blurred vision
46. Headaches, migraines when sugar, simple carbohydrates are eaten
47. Itching and crawling sensations on the skin; like little pin pricks or bites
48. Obesity
49. Death (just to let you know how serious this is!)
Other:
50.
51.
52.
53.
54.
55.
56.

__________________________________________________________________________________________________________________________________
33
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
HIGH BLOOD SUGAR /HIGH BLOOD SUGAR /HIGH BLOOD SUGAR /HIGH BLOOD SUGAR / INSULIN RESISTANCEINSULIN RESISTANCEINSULIN RESISTANCEINSULIN RESISTANCE Symptom CheckSymptom CheckSymptom CheckSymptom Checkllllistististist
Mark 0Mark 0Mark 0Mark 0----10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level 10 for your pain or symptom level and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.and any notes that will help you doctor.
0000 = no pain or = no pain or = no pain or = no pain or symptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptomssymptoms to 10 = extreme pain or full symptoms 1. Fatigue after meals / General fatigue
2. Craving for sweets that is not relieved by eating them / Must have sweets after meals
3. Waist girth is equal or larger than hip girth
4. Frequent urination
5. Increased appetite and thirst
6. Difficulty losing weight
7. Migrating aches and pains
8. Becoming upset easily: Outbursts of anger, feeling out of control emotionally
9. Confusion, abnormal behavior or both, such as the inability to complete routine tasks
10. Feeling weepy, crying for no reason, or more emotionally sensitive to everything
11. Light-headed
12. Literally saying a different word in a sentence than you were going to say
13. Fog-brain, poor memory, forgetfulness
14. Blackouts — can’t remember that you did something though were completely awake and doing it. (Blackout are usually attributed to alcoholism.)
15. Loss of consciousness, though uncommon
16. Visual disturbances, such as double vision and blurred vision

__________________________________________________________________________________________________________________________________
34
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
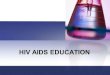
WHEN TO TAKE MEDICATIONSWHEN TO TAKE MEDICATIONSWHEN TO TAKE MEDICATIONSWHEN TO TAKE MEDICATIONS & SUPPLEMENTS& SUPPLEMENTS& SUPPLEMENTS& SUPPLEMENTS (An example: You do not need to print.) Your doctor will instruct you when to take your medications and supplements. It can feel constricting and overwhelming some days when you have a lot to take and keep track of, but it’s not forever. And, if it is forever . . . a list of some sort to check dosages taken will be very important and helpful.
Consistency is the key. I’m a late night person so my times can vary a bit depending on when I get to bed and then up in the morning, but I try to keep these as consistent as possible so that they are working in my body consistently for me. WORK and TRAVEL: If you’re traveling or just going to be out for more than a couple of hours or at work all day, plan ahead to take your pill/supplement supply with you and foods that you can eat. Fill it out once and make copies and you’re set to go!
Daily Medication Daily Medication Daily Medication Daily Medication and Supplement and Supplement and Supplement and Supplement
CheckCheckCheckCheckllllistististist Day:
AM AM AM AM PM PM PM PM
Med Name or just initials that you know what they are
5
Med Name
In-between pill box 7
Big pill box 9
In-between pill box 12
Big pill box 3
In-between pill box 6
Big pill box 9
Medicated Cream A Name
7
Medicated Cream B Name
7 2 9
Medicated Cream C Name
2 9
Drops A 7 6
Drops B 7 2 9
Drops C
Drops D

__________________________________________________________________________________________________________________________________
35
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
Daily Medication Daily Medication Daily Medication Daily Medication and Supplement and Supplement and Supplement and Supplement
ChecklChecklChecklChecklistististist
Day:
AM AM AM AM PM PM PM PM Daily Medication Daily Medication Daily Medication Daily Medication and Supplement and Supplement and Supplement and Supplement
CheckCheckCheckCheckllllistististist
Day:
AM AM AM AM PM PM PM PM

__________________________________________________________________________________________________________________________________
36
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
WATER LOGWATER LOGWATER LOGWATER LOG Choice: Water, Choice: Water, Choice: Water, Choice: Water, herbal teaherbal teaherbal teaherbal tea
Date Date Date Date Date Date Date Date Date Date Date Date Date Date Date Date Date
Using the formula:Using the formula:Using the formula:Using the formula: Weight: __________, divided by 2 =______ divided by 8 =______ ounces per day: ____oz
1 x 8 ounces = 1 cup
2 x 8
3 x 8
4 x 8 1 Quart
5 x 8
6 x 8
7 x 8
8 x 8 ½ Gallon
9 x 8
10 x 8
11 x 8
12 x 8 ¾ Gallon
13 x 8
14 x 8
15 x 8
16 x 8 1 Gallon

__________________________________________________________________________________________________________________________________
37
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
EXERCISE PLANEXERCISE PLANEXERCISE PLANEXERCISE PLAN Date:
TimeTimeTimeTime Kind of ExerciseKind of ExerciseKind of ExerciseKind of Exercise //// DistanceDistanceDistanceDistance
TimeTimeTimeTime Kind of ExerciseKind of ExerciseKind of ExerciseKind of Exercise //// DistanceDistanceDistanceDistance
How I feel today 0 (no symptoms) — 10 (extreme pain in joints, body aches)
Monday, Wednesdays and Fridays
7 a.m.
Walk 1.5 miles (treadmill when busy)
5:30 p.m.
Arm weights, 3 exercises, 12 reps each
Tuesday, Thursday and Saturdays
7 a.m. Stationary bicycle 1.5 miles
5:30 p.m.
Arm weight, 3 exercises, 12 reps each and extra stretching
Sunday No later than 6 p.m.
Preplan beginning of week: Go for a hike with a friend, walk around the block, get outside

__________________________________________________________________________________________________________________________________
38
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
EXERCISE LOGEXERCISE LOGEXERCISE LOGEXERCISE LOG (Twice/day) Date:
TimeTimeTimeTime Kind of ExerciseKind of ExerciseKind of ExerciseKind of Exercise //// DistanceDistanceDistanceDistance
TimeTimeTimeTime Kind of ExerciseKind of ExerciseKind of ExerciseKind of Exercise //// DistanceDistanceDistanceDistance
How I feel today 0 (no symptoms) — 10 (extreme pain in joints, body aches)

__________________________________________________________________________________________________________________________________
39
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
PRACTITIONER PRACTITIONER PRACTITIONER PRACTITIONER APPOINTMENT APPOINTMENT APPOINTMENT APPOINTMENT LOGLOGLOGLOG: : : : Date/Time
Name of PractitionerName of PractitionerName of PractitionerName of Practitioner Reason for AppointmentReason for AppointmentReason for AppointmentReason for Appointment Prescribed TreatmentPrescribed TreatmentPrescribed TreatmentPrescribed Treatment: : : : Medications / Medications / Medications / Medications / Supplements / Etc.Supplements / Etc.Supplements / Etc.Supplements / Etc.

__________________________________________________________________________________________________________________________________
40
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
MASTER MASTER MASTER MASTER PRACTITIONER PRACTITIONER PRACTITIONER PRACTITIONER APPOINTMENT APPOINTMENT APPOINTMENT APPOINTMENT LOG: LOG: LOG: LOG: Date
Name of PractitionerName of PractitionerName of PractitionerName of Practitioner MASTER MASTER MASTER MASTER PRACTITIONER PRACTITIONER PRACTITIONER PRACTITIONER APPOINTMENT APPOINTMENT APPOINTMENT APPOINTMENT LOG: LOG: LOG: LOG: Date
Name of PractitionerName of PractitionerName of PractitionerName of Practitioner

__________________________________________________________________________________________________________________________________
41
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
LAB LAB LAB LAB TESTSTESTSTESTSTESTS LOGLOGLOGLOG Document everything. Print more sheets as needed.
Date Date Date Date PractitionerPractitionerPractitionerPractitioner PurposePurposePurposePurpose: What tests?: What tests?: What tests?: What tests? Insurance SentInsurance SentInsurance SentInsurance Sent Paid? Outcome. Follow upPaid? Outcome. Follow upPaid? Outcome. Follow upPaid? Outcome. Follow up

__________________________________________________________________________________________________________________________________
42
©2011 Kim Wolinski, MSW “Dr. DeClutter” Get Your Life Back! Reset Your Thyroid Health FORMS www.ThyroidU.com [email protected] 303.485.5280
INSURANCE COMPANY / BILLINGS LOGINSURANCE COMPANY / BILLINGS LOGINSURANCE COMPANY / BILLINGS LOGINSURANCE COMPANY / BILLINGS LOG ———— OVERALL DOCUMENTATIONOVERALL DOCUMENTATIONOVERALL DOCUMENTATIONOVERALL DOCUMENTATION Document everything. Print more sheets as needed.
Date Date Date Date PractitionerPractitionerPractitionerPractitioner PurposePurposePurposePurpose Insurance SentInsurance SentInsurance SentInsurance Sent Paid? Outcome. Follow upPaid? Outcome. Follow upPaid? Outcome. Follow upPaid? Outcome. Follow up