Embed Size (px)
Citation preview

Getting the GIST of it: Why Molecules Matter to Surgeons
Martin McCarter, M.D.Associate Professor of SurgeryGI Tumor & Endocrine SurgeryUniversity of Colorado Denver
Surgery Grand RoundsNovember 21, 2011

Conflict of Interest
Employee of University of Colorado School of Medicine

Outline: GIST as a paradigm• What is GastroIntestinal Stromal Tumor• Natural history of GIST• Molecular classification• Signaling kinases• The imatinib story• Metastatic and adjuvant treatment• GIST post imatinib• What’s next for GIST
Getting the GIST of it: Why Molecules Matter to Surgeons

GIST – Formerly Known As:Leiomyoma Leiomyosarcoma Leiomyoblastoma

GIST: Identification of KITGain-of-Function Mutations
• KIT staining was positive in 46 of 49 GIST (94%)• 5 of 6 GIST had mutations in KIT gene• Mutant forms of KIT are constitutively active• Proposed that GIST may originate from Interstitial
cells of Cajal• KIT is receptor for Stem Cell Factor
Hirota et al. Science. 1998;279:577.

GIST: Interstitial Cells of Cajal
• Originally described by Ramon Cajal• KIT-positive fibroblast-like cells• Pacemaker cells of the gut
– Intercalated between intramural neurons and smooth muscle cells
– Generate electrical slow waves• Loss of ICC function has been
implicated in diabetic gastroenteropathy and gastroentericarrhythmia
Takayama et al. Arch Histol Cytol. 2002;65:1.

Scope of the Problem
• ~ 10,000 new soft tissue sarcomas per year• ~ 3000 GIST per year in the United States• Estimated annual incidence ~ 10 cases
per million

Staging of GIST
AJCC Staging Manual 7th ed.
T1 = <2 cmT2 = 2-5 cmT3 = 5-10 cmT4 = >10 cm
Mitotic RateLow <5/50HPFHigh >5/50HPF

Pathologic Features of GIST
Joensuu H and DeMatteo RP. Annu Rev Med. 2011 Jan 26. [Epub ahead of print]
• Median age at presentation is 63• Size about 5-7 cm• Location
• Stomach 55%• Small Intestine 35%• Rectum 5%• Other 5%

Natural History of GIST
DeMatteo RP et al. Ann Surg 2000 Jan;231(1):51-8.

GIST: Recurrence-Free Survival Following Surgical Treatment of
Primary GIST
Singer et al. J Clin Oncol. 2002;20:3898.
0
0.25
0.50
0.75
1.0
0 20 40 60 80
<5 cm<5-10 cm
>10 cm
P=0.03
Length of study (mo)
Prop
ortio
n su
rviv
ing
free
of r
ecur
renc
e
0
0.25
0.50
0.75
1.0
20 40 60 80Length of study (mo)
Prop
ortio
n su
rviv
ing
free
of
recu
rren
ce
≤3 mitoses/30 hpf
>3 to ≤15 mitoses/30 hpf
>15 mitoses/30 hpfP=0.0001
0

Joensuu H , DeMatteo RP. Annu Rev Med. 2011 Jan 26. [Epub ahead of print]
KIT and PDGFRα Mutations in GIST

Signaling Protein Kinases
• Transient signal from surface membrane receptor through to intracellular and nuclear machinery• Regulate cell functions• Dependant on a phosphorylation step• Potential target IF cancer cell is largely dependant on it for growth

Development of Imatinib
• CML was the target• Known (Philadelphia 9/22) chromosomal translocation • Resulted in BCR-ABL fusion protein• Screened designer drugs to fit BCR-ABL phosphate
pocket and inhibit tyrosine kinase

Imatinib and GIST An International Story
1 BCR-ABL protein described 1973
1

Imatinib and GIST An International Story
1 BCR-ABL protein described 19732 Imatinib developed for BCR-ABL 1990’s
12

Imatinib and GIST An International Story
1 BCR-ABL protein described 19732 Imatinib developed for BCR-ABL 1990’s3 KIT mutation described 1998
12 3

Imatinib and GIST An International Story
1 BCR-ABL protein described 19732 Imatinib developed for BCR-ABL 1990’s3 KIT mutation described 19984 First GIST patient treated with Imatinib 2000
12
4
3

Imatinib Mesylate (Gleevec):Proposed Mechanism of Action
P
PP PATP
SIGNALING
Imatinibmesylate
Kinasedomains
• Inhibits KIT, Bcr-Abl, PDGFR
• Occupies the ATP binding pocket of the KIT kinase domain
• This prevents substrate phosphorylation and signaling
• A lack of signaling inhibits proliferation and survival
Adapted from Savage and Antman. N Engl J Med. 2002;346:683.Scheijen and Griffin. Oncogene. 2002;21:3314.

First Patient With GIST to Receive Imatinib Mesylate: Proof-of-Concept
• Exploratory study with oral imatinib mesylate at 400 mg/d• Dramatic clinical response
– Disappearance of excess metabolic activity at 4 weeks by 18FDG-PET
– 75% reduction in tumor size at 8-month follow-up– Tumor biopsies showed histologic evidence of myxoid
degeneration and lack of mitotic activity– Symptomatic relief
Joensuu et al. N Engl J Med. 2001;344:1052.

Imatinib Induced Pathologic Changes
Demetri GD, et al. N Engl J Med. 2002;347:472-80
CD 117
H&E

Key Studies in GISTMetastatic Disease – B2222 Trial
Demetri GD, et al. N Engl J Med. 2002;347:472-80

• Nine-year OS rate all patients was 35% (38% for patients with CR/PR; 49% for patients with SD)
• Nine-year OS by tumor bulk at baseline was: 58% in group 1, 40% in group 2, 20% in group 3, and 23% in group 4
Significant correlation between tumor bulk and OS (P=0.0043)
Key Studies in GISTLong Term F/U of B2222 Trial
von Mehren et al. ASCO June 2011

Key Studies in GISTAdjuvant Treatment Following Resection
DeMatteo RP et al. Lancet. 2009 Mar 28;373(9669):1097-104. Epub 2009 Mar 18.
Recurrence Free Survival Overall Survival
ACOSOG Z-9001 • Completely resected GIST >3 cm• Randomized to placebo vs. imatinib for 12 months• Primary endpoint is recurrence free survival

Key Studies in GISTAdjuvant Treatment Following Resection
DeMatteo RP et al. Lancet. 2009 Mar 28;373(9669):1097-104. Epub 2009 Mar 18.

Key Studies in GISTAdjuvant Treatment Following Resection
Joensuu et al. Presented at ASCO June 2011
Recurrence Free Survival Overall Survival
SSGXVIII/AIO• Completely resected High Risk GIST (>5 mitosis/50HPF)• Randomized to 12 vs. 36 months of imatinib• Primary endpoint is recurrence free survival

Subgroup No. of patients Hazard ratio (95% CI), RFS P-value
Age≤65 256 0.47 (0.30–0.74) 0.001>65 141 0.49 (0.28–0.85) 0.01
SexMale 201 0.46 (0.28–0.76) 0.002Female 196 0.46 (0.28–0.76) 0.002
Tumor siteStomach 202 0.42 (0.23–0.78) 0.005Other 195 0.47 (0.31–0.73) <0.001
Tumor size≤10 cm 219 0.40 (0.23–0.69) <0.001>10 cm 176 0.47 (0.29–0.76) 0.002
Mitoses/50 HPF (local)≤10 mitoses 209 0.76 (0.43–1.32) 0.33>10 mitoses 154 0.29 (0.17–0.49) <0.001
Mitoses/50 HPF (central)≤10 mitoses 238 0.58 (0.34–0.99) 0.04>10 mitoses 133 0.37 (0.23–0.61) <0.001
Tumor ruptureNo 318 0.43 (0.28–0.66) <0.001Yes 79 0.47 (0.25–0.89) 0.02
Tumor mutation siteKIT exon 9 26 0.61 (0.22–1.68) 0.34KIT exon 11 256 0.35 (0.22–0.56) <0.001Wild type 33 0.41 (0.11–1.51) 0.16Other 51 0.78 (0.22–2.78) 0.70
0.1 1.0 10
36 mo better 12 mo better
Results of SSGXVIII/AIO: Subgroup Analysis
Joensuu et al. Presented at ASCO June 2011

GIST: KIT and PDGFRA Mutations Predict Event-Free Survival
KIT exon 11 vs exon 9 (P<0.0001)KIT exon 11 vs no mutation (P<0.0001)KIT exon 9 vs no mutation (P=0.1428)
0 100 200 300 400 500 600 700 8000
102030405060708090
100
Days
Even
t-fre
e su
rviv
al (%
)
KIT exon 9 (n=23)
No kinase mutation(n=9)
KIT exon 11 (n=85)
Heinrich et al. J Clin Oncol. 2003;21:4342.
Lessons Post Imatinib ApprovalMutation Analysis

Lessons Post Imatinib ApprovalRisk Stratification
Miettinen M, Lasota J Semin Diag Pathol 2006;23(2):70-83, NCCN Guidelines 2010 J Natl Compr CancNetw. 2010 Apr;8 Suppl 2:S1-41

Prediction Tools
http://www.mskcc.org/mskcc/html/98103.cfmGold et al. Lancet Oncol. 2009 Nov;10(11):1045-52.

Questions• What are the surgical goals for GIST?• Can we stop or interrupt treatment?• How long to treat – metastatic, adjuvant?• What about imatinib resistance?• What to do with incidental or micro GIST’s?• Should we use imatinib in the neoadjuvant setting?
• If so, how long?• Is surgery ever needed?
• Is there a role for debulking GIST?• What to do with a margin positive (R1) resection?• Is pediatric or familial GIST any different?
The More We Learn About GIST The More Questions We Generate

• Negative margins• Avoid rupture• Preserve function• Nodes generally not necessary
(except in young patients)
Surgical Goals for GIST

How Long to Treat? Can Treatment be Stopped or Interrupted?
von Mehren et al. ASCO June 2011
Years after start of imatinib therapy
0–2 >2–4 >4–6 >6–8 >8–9 >9–10
No. of patients at riska 147 66 29 19 17 14
Progression/Censoredb 71/11 22/3 19/1 1/1 1/2 NA
Rate of progression (Probability of event [%])
48.3 35.4 48.7 5.3 5.9 NA
• 56/147 patients initially enrolled in the B2222 study continued imatinib treatment beyond 3 years, with some patients remaining on treatment for 10yrs • 26 patients (17.7%) have remained on continuous imatinib• Risk of progression drastically decreased after 6 years of imatinib therapy
Probability of progression according to duration of imatinib therapy (life-table method)

Gounder MM , Maki RG. Cancer Chemother Pharmacol. 2011 Jan;67 Suppl 1:S25-43. Epub 2010 Nov 30.
Molecular Basis for Primary and Secondary Tyrosine Kinase Inhibitor Resistance in GIST
• Secondary mutation induce conformational change altering the ATP binding site• Type of secondary mutation may be important in overall survival• May manifest as isolated clonal or polyclonal disease

Micro GIST’s
Joensuu H , DeMatteo RP. Annu Rev Med. 2011 Jan 26. [Epub ahead of print], NCCN Guidelines 2010 J Natl Compr Canc Netw. 2010 Apr;8 Suppl 2:S1-41
• The prevalence is much higher than the clinical incidence
• Micro GIST’s smaller than 1 cm • Found in up to 50% of autopsy series• Many already have KIT mutation• EUS surveillance 13% (3/23) progressed • Potential for malignancy unknown• Resect any >2cm (consensus)

Neoadjuvant Therapy for GIST
Before
After
• Two phase II trials (19 and 30 patients) • Suggest similar response rates• Safe to give pre-op (no need to stop)• Overall recurrence dictated by size

Is there a Role for GIST Tumor Debulking?69 Patients underwent debulking
- pre-operatively determined to have:• Stable disease (n=23) – bulky (>1cm) disease left in 4%• Limited disease progression (n=32) – bulky disease in 16%• Generalized disease progression (n=14) 50% emergent
indication – bulky disease left in 43%
Raut C, et al. J Clin Oncol 2006 May 20;24(15):2325-31.

Considerations for Debulking GIST
• Average duration of response ~ 2 years• Surgical timing around 6 - 24 months• Stable disease – all resectable?• Limited disease progression – selected
resection• Impending obstruction• GI bleeding• Paraneoplastic syndrome

RecurrenceResection MarginR0 R1
Local 8 (4.4%) 4 (16.0%)
Regional 86 (47.5%) 13 (52.0%)
Distant 87 (48.1%) 8 (32.0%)
Sites of First Recorded Recurrence by Margin StatusACOSOG Z-9000 & Z-9001
Chi Square 6.4, p=0.04
Microscopic (R1) Positive Margin
McCarter et al, Western Surgical Association, Nov 2011
• 72/819 Pts (8.8%) had R1 resection• Median f/u 49 months
61% (placebo) to 65% (imatinib) of R1 resections did not experience a recurrence85-95% of recurrences are regional or distant

Recurrence free survival at 3 years is 60% vs. 76% in the R1 vs. R0 group respectively. HR=1.51 (95% CI: 0.76, 2.99) p=0.24
Microscopic (R1) Positive Margin
Recurrence free survival at 3 years is 82% vs. 79% in the R1 vs. R0 group respectively. HR=1.095 (95% CI: 0.66, 1.83) p=0.73
McCarter et al, Western Surgical Association, Nov 2011

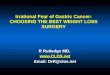
Familial GIST
Joensuu H , DeMatteo RP. Annu Rev Med. 2011 Jan 26. [Epub ahead of print]
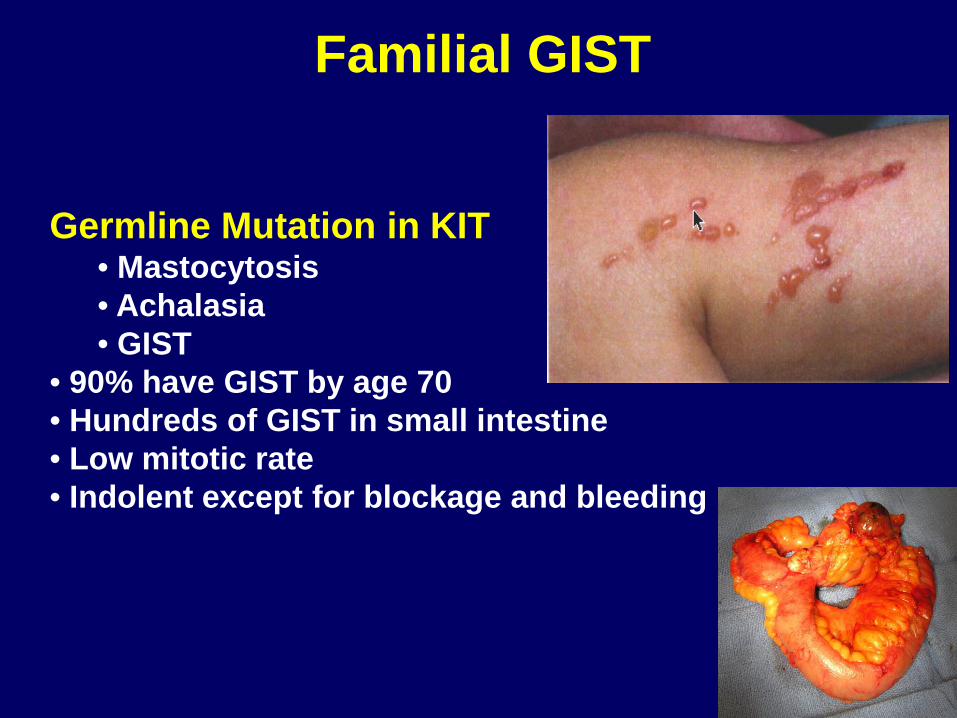
Familial GIST
Germline Mutation in KIT• Mastocytosis• Achalasia• GIST
• 90% have GIST by age 70• Hundreds of GIST in small intestine• Low mitotic rate• Indolent except for blockage and bleeding

Pediatric GIST
• Age <21• Strong CD 117 staining• Wild type – no identifiable mutation• Can involve lymph nodes• Higher recurrence rate• Longer survival (more indolent course)

Cost of Imatinib
• Standard dose is 400mg QD• 100mg tablet costs $20-30• One year of imatinib ~ $64,000

What’s Next for GIST• Serum imatinib concentration and response• Improving prediction of micro GIST• Targeting secondary mutations• Patient initiated tumor banking
Gounder MM , Maki RG. Cancer Chemother Pharmacol. 2011 Jan;67 Suppl 1:S25-43. Epub 2010 Nov 30.