-
7/29/2019 Gist Bedah Digestif
1/36
Medical and Targeted Therapies
of GIST
-
7/29/2019 Gist Bedah Digestif
2/36
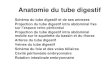
Foo WC, Liegl-Atzwanger B, Lazar AJ. Pathology of
Gastrointestinal Stromal Tumors.Pathology 2012;5:23-33
Anatomical Sites of GIST
Stomach
(60%)
Jejunum & ileum
30%
Duodenum
(5%)
Colorectum
(4%)
Appendix
-
7/29/2019 Gist Bedah Digestif
3/36
CLINICAL PRESENTATION
Varies depending on:
anatomic location of tumor
tumor size
aggressiveness
most common presentation:
GI bleeding (acute)
Chronic anemia
-
7/29/2019 Gist Bedah Digestif
4/36
CLINICAL PRESENTATION
GIST patients may also present with:
acute abdomen (tumor rupture)
GI obstruction
appendicitis-like pain
others: fatigue, dysphagia, satiety
-
7/29/2019 Gist Bedah Digestif
5/36
PATHOGENESIS:
-
7/29/2019 Gist Bedah Digestif
6/36
GIST: express CD 117 antigen*
(95%)
Evolution in stromal cell neoplasms
of GI tract: classification,
diagnosis, management
CD117 molecule: part of KIT (c-kit) tirosine-
kinase receptor, produced by KIT-oncogen
Express by ICC (interstitial cell of Cajal)
-
7/29/2019 Gist Bedah Digestif
7/36
Other spindle cell neoplasms of GI tract :
(lipoma, schwannoma, hemangioma,
leiomyoma dan leiomyosarcoma)
CD117-negative5% GIST CD 117
negative
-
7/29/2019 Gist Bedah Digestif
8/36
-
7/29/2019 Gist Bedah Digestif
9/36
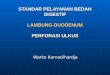
Foo WC, Liegl-Atzwanger B, Lazar AJ. Pathology of
Gastrointestinal Stromal Tumors.Pathology 2012;5:23-33
Diagram of KIT and PDGFRA receptor tyrosine kinases with
location and relative frequencies of mutations.
-
7/29/2019 Gist Bedah Digestif
10/36
Tyrosine kinases and cancer
Tyrosine phosphorylation
A central mechanism for controlling cell signaling, leading
to:
DifferentationMigrationProliferation
Enzyme Tyrosine kinases Tyrosine phosphatases
-
7/29/2019 Gist Bedah Digestif
11/36
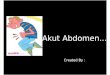
Normal KIT Signaling
1. SCF ligand binding induces
2 KIT protein1,2
homodimerization2. Activation of the KIT
kinase domain1,2
3. ATP binding allows
binding of a substrate that
can now be
phosphorylated andactivated1,2
4. Activated substrate
initiates a signaling
cascade thought to be
crucial for1,2
Proliferation
Adhesion
Apoptosis
Differentiation PP P
ADP
PP PP
ATP
SIGNALING
KIT kinase
domain
Substrate
P
1 . D ue ns ing A e t a l. Cancer Invest. 2004;22:106-116.2.
Rubin BP et al. Lancet. 2007;369(9574):1731-1741.
Proliferation
and survival
-
7/29/2019 Gist Bedah Digestif
12/36
Targeted Therapies:
a new generation of cancer drugs,
designed to interfere with specific proteins,
that have a critical role in tumor growth
andprogression
-
7/29/2019 Gist Bedah Digestif
13/36
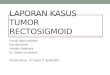
Inhibition of KIT Signaling by Imatinib1. Imatinib binds to
the ATP-binding
pocket of the KIT
kinase domain1,2
2. This prevents
substrate
phosphorylation
and
signaling1,2
3. A lack of signaling
inhibitsproliferation
and survival1,2
SIGNALING
KIT kinase
domain
Imatinib
ATP
P P P
X
Substrate
Proliferation and survivalX1. Rubin BP et al. Lancet.
2007;369(9574):1731-1741.
2. Sav age DG et al. N Engl J Med. 2002;346:683-693.
-
7/29/2019 Gist Bedah Digestif
14/36
Targeting KIT
Imatinib and other TKIs in the treatment of
GIST has dramatically improve the outcome.
Especially in metastatic phase (no effective
treatment before TKI).
Imatinib was the first TKI to be approved for
the treatment of GIST.
-
7/29/2019 Gist Bedah Digestif
15/36
Targeting KIT
Imatinib-treated patients tend to relapse
because of secondary KIT mutation.
Dasatinib (second generation) are being
tested for their efficacy against KIT mutant
forms.
-
7/29/2019 Gist Bedah Digestif
16/36
Targeting KIT
Dasatinib is currently under investigation in
patientswith imatinib/sunitinib-refractory
GIST.
Nilotinib is inphase III first-line therapy in
inoperable/unresectable, metastatic disease.
-
7/29/2019 Gist Bedah Digestif
17/36
TREATMENT
Multidisciplinary treatment planning
involving:
pathologist
radiologist
surgeons (digestive)
medical oncologist
-
7/29/2019 Gist Bedah Digestif
18/36
ADJUVANT THERAPY
Relapse can be substantial. Risk classification and mutational
analysis is
critical to making a clinical decision about
adjuvant therapy.
-
7/29/2019 Gist Bedah Digestif
19/36
Stage Classification and Risk
Assessment
TNM classification is not recommended (ESMO)
Prognostic factors:
Mitotic rate
Tumor size
Tumor site: gaster better than small bowel or
rectal GIST
Surgical margins
Tumor rupture
-
7/29/2019 Gist Bedah Digestif
20/36
Table : Rates of metastases or tumor-related death in GISTs of
the stomach and small intestine by tumors grouped by
the mitotic rate and tumor size.
Group Tumor parameters Percentage of patients due to relapse
Size Mitotic rate Gastric GISTs Jejunal and ileal GISTs Duodenal
GISTs Rectal GISTs
1 2 cm 5 per 50 HPFs 0 none 0 none 0 none 0 no ne
2 >2 5 cm 5 per 50 HPFs 1.9 very low 4.3 low 8.3 low 8.5 %
low
3 a >5 10 cm 5 per 50 HPFs 3.6 low 24 moderate3b >10 cm 5
per 50 HPFs 12 moderate 52 high 34 higha 57c highb
4 2 cm >5 per 50 HPFs 0c 50c d 54 high
5 >2 5 cm >5 per 50 HPFs 16 moderate 73 high 50 high 52
high
6a >5 10 cm >5 per 50 HPFs 55 high 85 high
6b >10 cm >5 per 50 HPFs 86 high 90 high 86 highb 71
highb
a
Based on previously published long-term follow-up studies on
1055 gastric, 629 small intestinal, 144 duodenal and111 rectal
GISTs [12, 15, 18, 30].bGroups 3a and 3b or 6a and 6b are combined
in duodenal and rectal GISTs because of the small number of cases.c
Denotes the tumor categories with very small numbers of cases.dNo
tumors of such category were included in the study. Note that small
intestinal and other intestinal GISTs show a
markedly worse prognosis in many mitotic rate and size
categories than gastric GISTs.
GIST: Gastrointestinal stromal tumor; HPF: high-power field.
The ESMO / European Sarcoma Network Working Group. Clinical
Practice Guidelines. Gastrointestinal Stromal Tumors: ESMO Clinical
PracticeGuidelines for diagnosis, treatment and follow-up. Annals
of Oncology 23 (Supplement 7): vii49vii55, 2012
Rate of metastases or tumor-related
death in GIST
-
7/29/2019 Gist Bedah Digestif
21/36
NCCN Guidelines
1. NCCN Clinical Practice Guidelines in Oncology. Soft Tissue
Sarcoma. V.2.2011.
-
7/29/2019 Gist Bedah Digestif
22/36
Adjuvant imatinib therapy is safe and compared to placebo
treatments
appears to prolong RFS following the resection of primary
GIST.OS is not different at this time
-
7/29/2019 Gist Bedah Digestif
23/36
Preoperative imatinib can decrease tumor volume and is
associatedwith complete surgical resection in locally advanced
GISTs.
-
7/29/2019 Gist Bedah Digestif
24/36
IMATINIB
Dose of imatinib 400mg/d.
Patients with KIT exon 9
mutations fare better in
PFS on dose 800mg/d.
Treatment should becontinued indefinitely.
-
7/29/2019 Gist Bedah Digestif
25/36
Imatinib
Patients should be alerted to the importance
of compliance with therapy.
Interactions with concomitant medications
/foods.
proper handling side effects.
-
7/29/2019 Gist Bedah Digestif
26/36
www.OncologyEducation.ca
Authors: Joensuu H et al.Reviewed By: Dr. Vincent Tam
Abstract: ASCO 2011 Abstract 1
Date posted: June 2011
Twelve versus 36 months of adjuvant imatinib as
treatment of operable GIST with a high risk of
recurrence: Final results of a randomized trial
(SSGXVIII/AIO)
-
7/29/2019 Gist Bedah Digestif
27/36
N= 400 (1:1 randomization)
Stratification:1) R0 resection, no tumor rupture
2) R1 resection, tumor rupture
Primary Outcome: RFS
R
Treatment A:
IMATINIB 400mg daily x 12 months
Treatment B:IMATINIB 400mg daily x 36 months
Study Design
-
7/29/2019 Gist Bedah Digestif
28/36
Inclusion Criteria
- Diagnosis histology: GIST, KIT-positive
- High Risk for recurrence according Modified
Consensus Criteria:
Diameter tumor > 10cm or
Tumor mitotic count>10/50 HPF or
Tumor >5cm and mitosis count>5/50 HPF or
Spontaneous tumor rupture during surgical
procedure
-
7/29/2019 Gist Bedah Digestif
29/36
RESULTS*
IMATINIB
X 12
Months
IMATINIB
X 36
Months
Hazard
Ratiop-value
5Y-RFS
(%)47.9% 65.6% 0.46 p
-
7/29/2019 Gist Bedah Digestif
30/36
TOXICITY
IMATINIB
X 12 Mon ths
(n = 194)
IMATINIB
X 36 Mon ths
(n = 198)
P
Any adverse event 99% 100% 0.24
Any grade 3/4 event 20% 33% 0.006
Grade 3/4 periorbital
edema1% 1% 1.00
Grade 3/4 fatigue 1% 1% 0.62
Grade 3/4 diarrhea 1% 2% 0.37
Discontinued imatinib,
no GIST recurrence13% 26% 0.001
-
7/29/2019 Gist Bedah Digestif
31/36
Drug side effects and other
consideration:
Fluid retention (periorbital or peripheral edema)
Diarrhea
Nausea (diminished if taken with food)
fatigue
Muscle cramps
Abdominal pain
Rash
Mild macrocytic anemia
-
7/29/2019 Gist Bedah Digestif
32/36
Second line : Sunitinib
Third line: Regorafenib
After failing on Regorafenib: participated in
clinical trial
Anecdotal evidence:
patients who have already progressed onimatinib may occasionally
benefit when
rechallenged with the same drug.
-
7/29/2019 Gist Bedah Digestif
33/36
FOLLOW UP
Relapses most often: liver and/or peritoneum.
Risk assessment: mitotic count, tumor size,tumor site useful in
choosing FU policy.
High risk patients: relapse within 1-2 yearsfrom the end of
adjuvant therapy.
HR pats., FU with CT/MRI every 3-6 mo (for 3
yrs during adjuvant T/), every 3 mo. (for 2 yrson cessation
adjuvant T/), then every 6 mountil 5 yrs, then annually. (MRI
prefer than CT)
The ESMO / European Sarcoma Network Working Group. Clinical
Practice Guidelines. Gastrointestinal Stromal Tumors: ESMO Clinical
PracticeGuidelines for diagnosis, treatment and follow-up. Annals
of Oncology 23 (Supplement 7): vii49vii55, 2012
-
7/29/2019 Gist Bedah Digestif
34/36
ELGEKA
Komunitas Masyarakat Peduli Leukemia
Granulositik Kronik dan GIST di Jawa Tengah.
Berdiri sejak 2009
Obat didapat lewat NOA/NOA+ASKES
Sekretariat: Sub HEMON IPD FK UNDIP/RSDK
-
7/29/2019 Gist Bedah Digestif
35/36
TERIMAKASIH
-
7/29/2019 Gist Bedah Digestif
36/36
Imatinib
Suboptimal plasma levels of imatinib: worse
outcome.
Plasma levels assessment may be useful in:
pats. receiving concomitant medication (risk
major interaction)
unexpected observed toxicities
progression on 400mgto increase dose of
800mg