Embed Size (px)
DESCRIPTION
Lecture on GI
Citation preview

Basic Mechanism of Secretion1. Secrete substance – nervous or hormonal
stimuli increase iCa2+ → exocytosis2. Secrete water and electrolytes to move
substance into target area (osmosis)

Chemical & Electrical Gradients Drive Secretionof Water
cAMP causes Cl- channels to
open
Na+ follows electrical gradient
H2O moves along osmoticgradient
Cl -Na+
Cl - Na+
PNa+ Na+
K+ K+
Na+
H2 0
Na+
H2 0
Cl -
CFTR
cAMP
-----
-----
lumen blood
++
++
++
Types of Secretory Glands
• Single Cell - mucous cells or goblet cells
• Simple - indentations in epithelium in S.I.and colon
(e.g. crypts of Lieberkühn inS.I.)
• Tubular - stomach, duodenum
• Complex - salivary, pancreas, liver
Control of Secretion• Local - tactile, distention, irritation that comes
from direct contact with food/chyme
• Reflex - nervous input, activated by local inputor sensory input
• Hormonal - G.I. hormones (more so in stomach& S.I.)
PNS Stim. - secretion of substance & waterSNS Stim. - blood flow to gland & cAMP
in acinar cells

Mucus Composition - Properties
• Thick secretion that is mainly water,
electrolytes and glycoproteins -
• Essential for digestion because -Adherent - sticks to foodBody - coats wellLow resistance - lubricationSelf adherent - sticks togetherResistant to digestionBuffering capacity

Functions of Saliva
• Lubrication and binding of foodtogether
• Solubilizes dry food
• Initiates starch digestion
• Oral hygieneDestroys bacteria - proteolytic enzymes (lysozyme)
- thiocyanate- antibodies

Saliva
• Two types of secretion -
- Serous - watery secretion, contains an
-amylase (ptyalin)
- Mucous - contains mucin - lubrication
• Secrete 800-1000 mL/day of saliva• Maximum rate of secretion: 4 ml/min
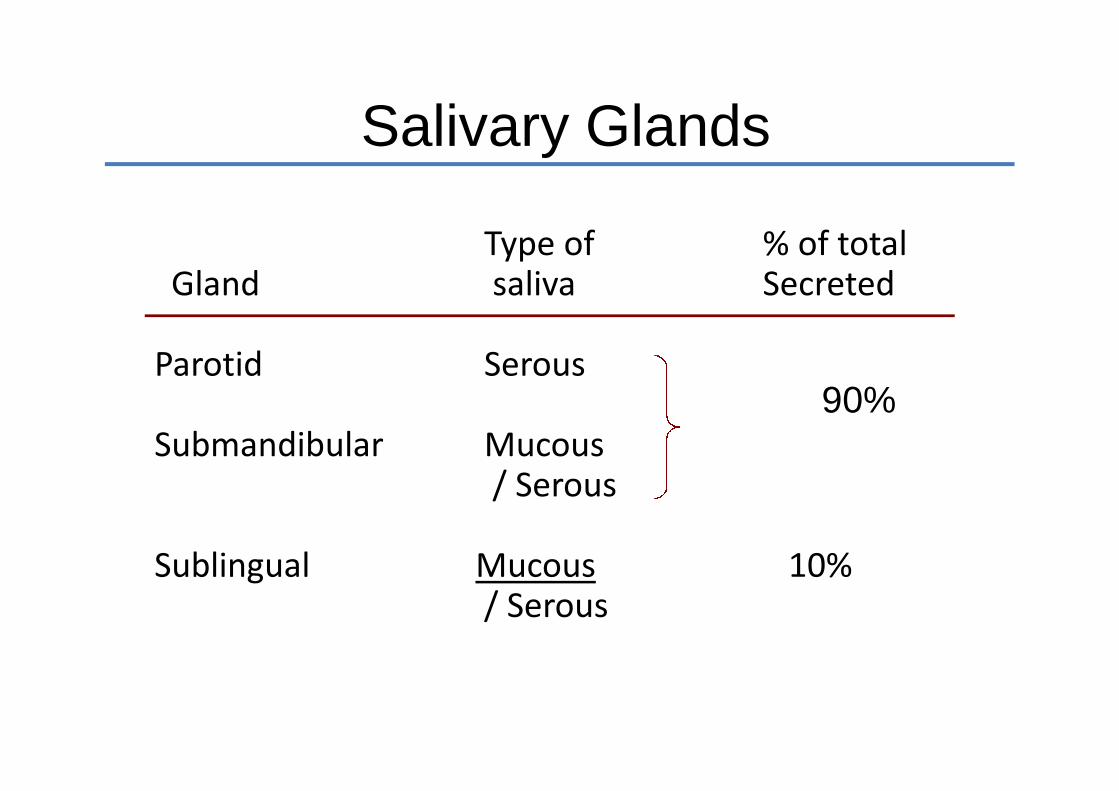
Salivary Glands
Type of % of totalGland saliva Secreted
Parotid Serous
Submandibular Mucous/ Serous
Sublingual Mucous 10%/ Serous
90%

Formation and Secretion of Saliva
• Two Stages -
- Acini: - primary secretion similar toplasma
- Salivary Ducts: modified as it passesthrough ducts
- Na+ is actively reabsorbed- K+ is secreted, but not equal to
the Na+ that’s reabsorbed- increased electronegative forceleads to passive Cl- reabsorption- HCO3- secreted

Ionic Composition of Saliva
• Hypotonic
• Ionic composition depends upon rate ofsecretion. Resting composition is:
- Na+ - 0.1 x plasma (15 mEq/L)- Cl- - 0.15 x plasma (15 mEq/L)- K+ - 7 x plasma (30 mEq/L)- HCO
-3 - 3 x plasma (70 mEq/L)
• Increased secretion increases the [Na+] and[Cl-] & decreases the [K+] & [HCO3-]
• Aldosterone increases K+ secretion
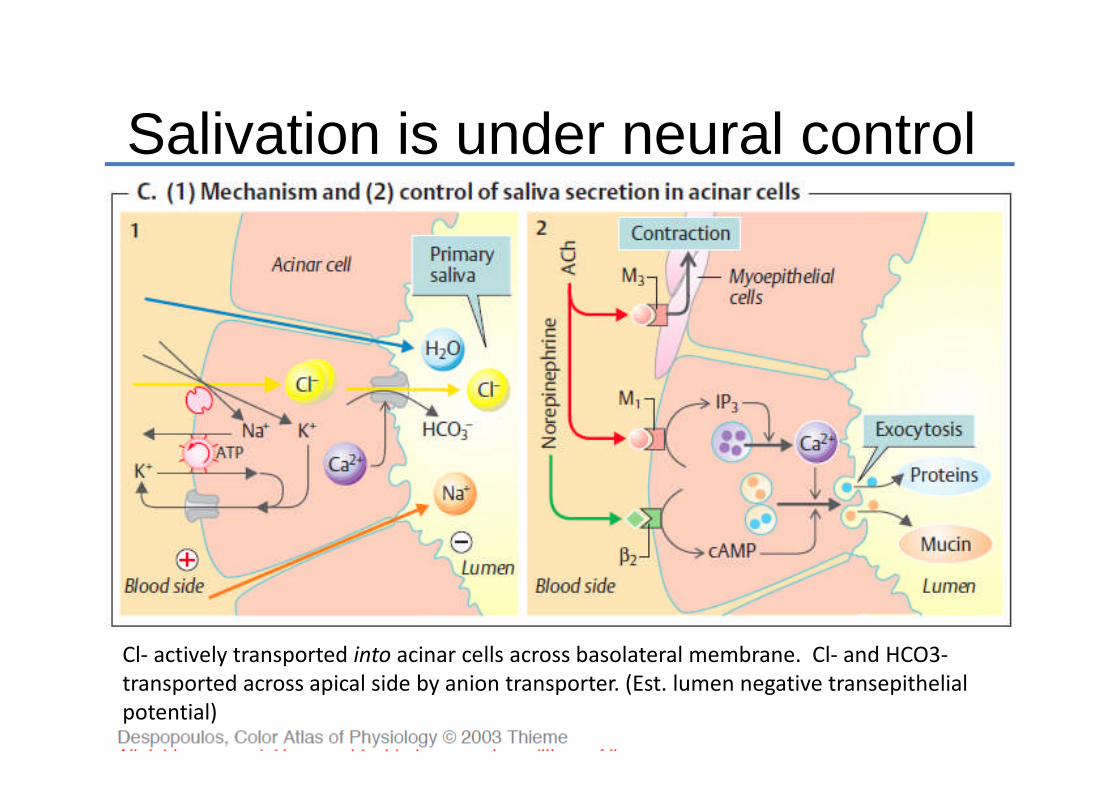
Salivation is under neural control
Cl- actively transported into acinar cells across basolateral membrane. Cl- and HCO3-transported across apical side by anion transporter. (Est. lumen negative transepithelialpotential)
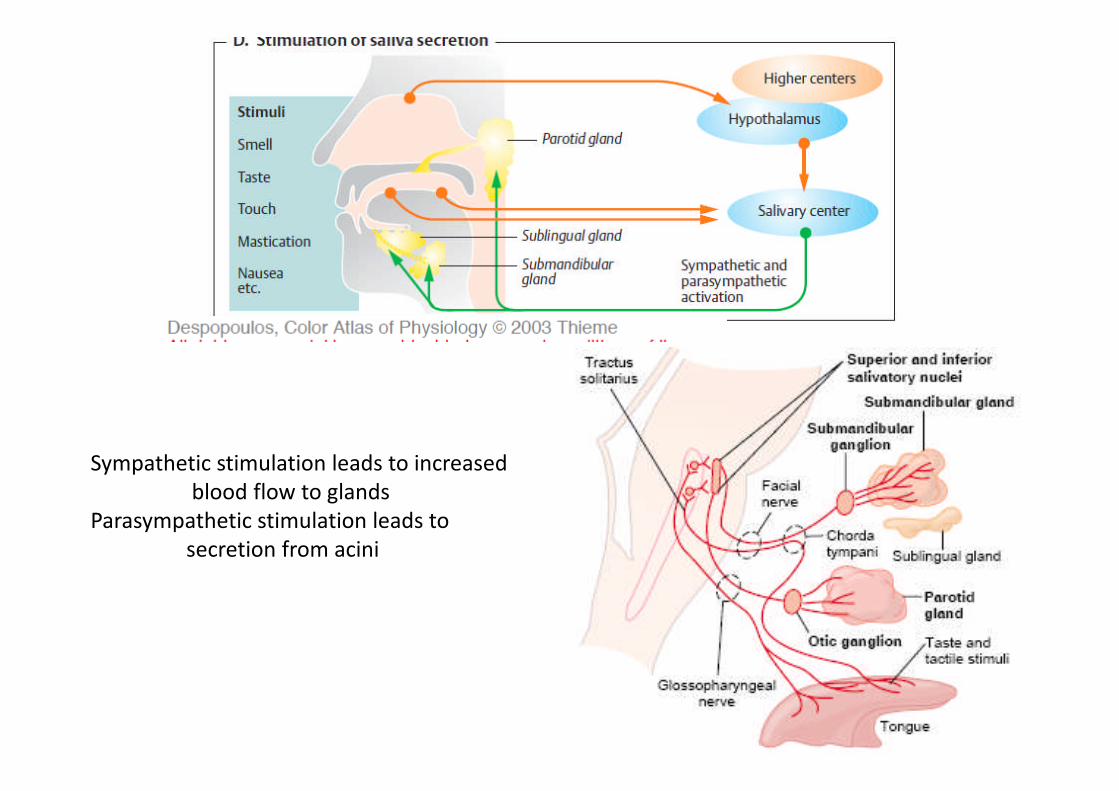
Sympathetic stimulation leads to increasedblood flow to glands
Parasympathetic stimulation leads tosecretion from acini
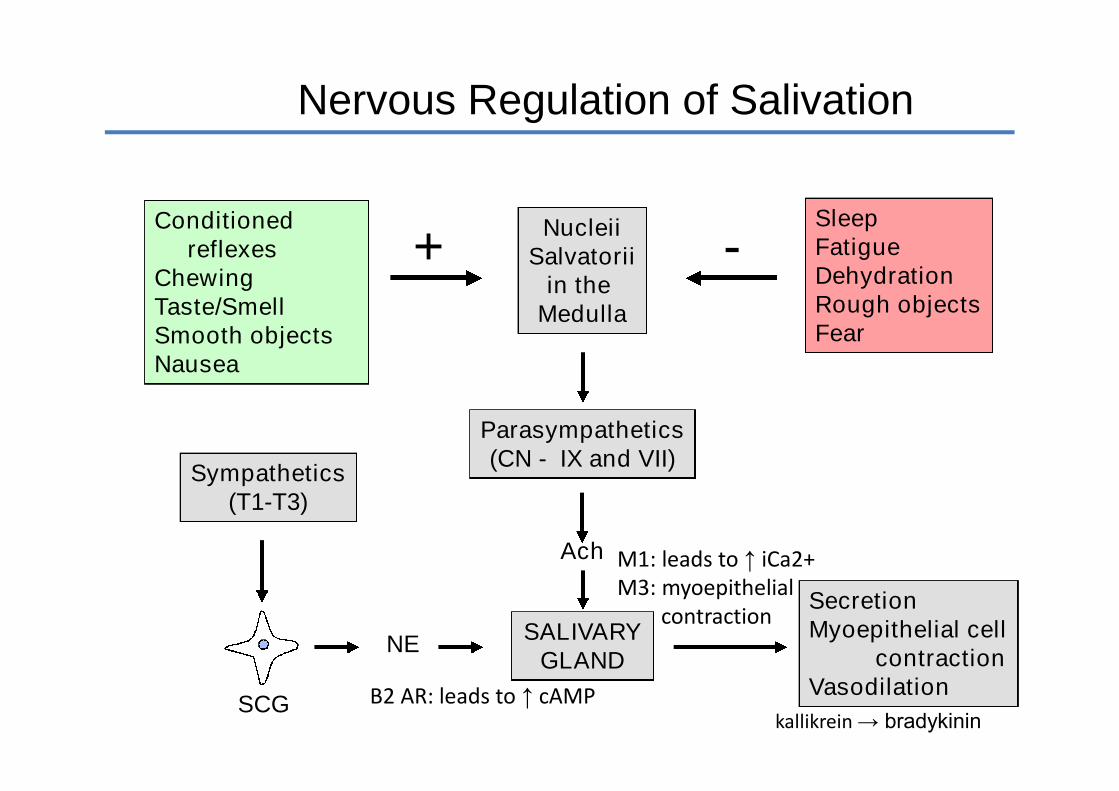
NucleiiSalvatorii
in theMedulla
SleepFatigueDehydrationRough objectsFear
Conditionedreflexes
ChewingTaste/SmellSmooth objectsNausea
+ -
Parasympathetics(CN - IX and VII)
SALIVARYGLAND
Ach
Sympathetics(T1-T3)
SCG
NE
SecretionMyoepithelial cell
contractionVasodilation
Nervous Regulation of Salivation
B2 AR: leads to ↑ cAMP
M1: leads to ↑ iCa2+M3: myoepithelial
contraction
kallikrein → bradykinin
Clinical
• Xerostomia - dry mouth.- Causes: -- lack of sleep or dehydration- drug related, e.g. diuretics
- insufficient capillary perfusion- radiation treatment (aplasia of glands)
- destruction of glands- autoimmune disease
• Drooling- Treatment: - anticholinergics
- surgical removal of the sublingualglands and retropositioning
submandibular ducts.

Clinical complications
• Cystic Fibrosis - salivary Ca++, Na+, and protein are elevated(also true for bronchial secretions, pancreatic juice, andsweat).- Cl- secretion is essential for cell secretion- CF patients have dysfunctional or no (CFTR )
CFTR = cystic fibrosis transmembrane
conductance regulator
• Primary aldosteronism - (Conn’s syndrome)
- salivary NaCl close to zero
- salivary K+ increases to high levels
Esophageal Secretion
• Mucosal
• Simple mucos glands
• Compound mucos glands in proximal &distal ends secrete mucos that– Prevents food from scraping epithelia
– Protects in case of stomach reflux

Functions of Stomach
• Short-term storage reservoir
• Secretion of intrinsic factor
• Chemical and enzymatic digestion isinitiated, particularly of proteins
• Liquefaction of food
• Slowly released into the small intestine forfurther processing
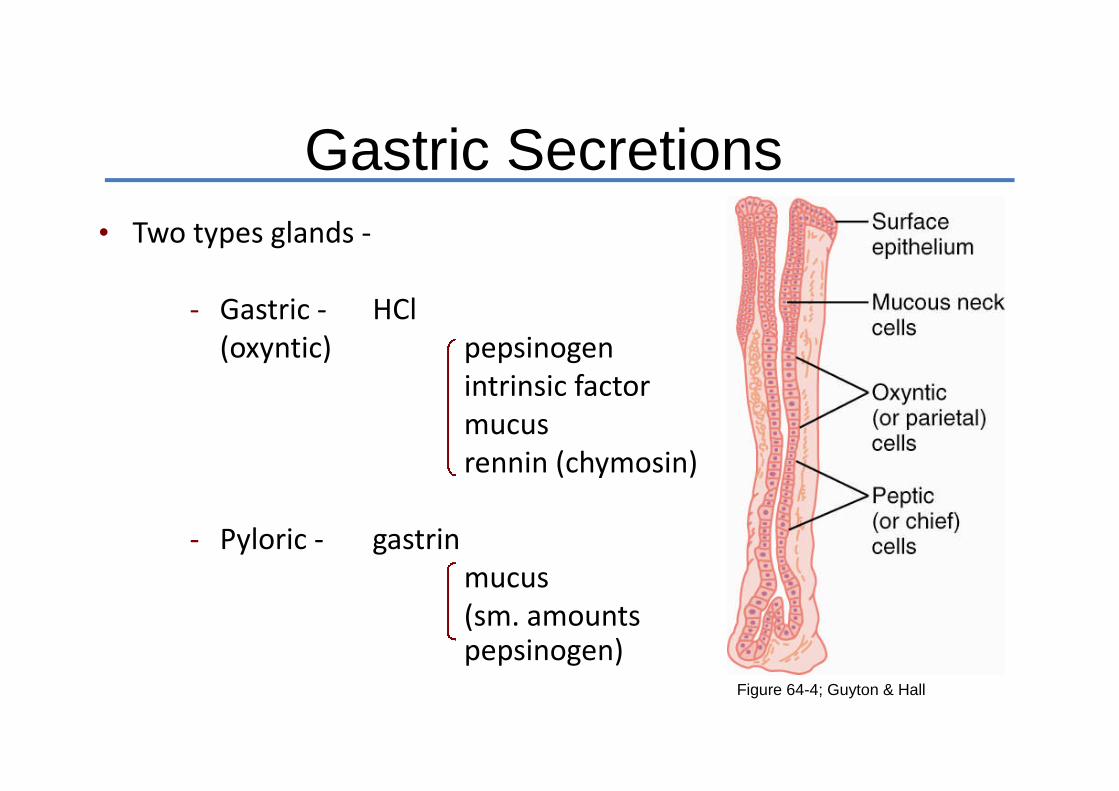
Gastric Secretions• Two types glands -
- Gastric - HCl(oxyntic) pepsinogen
intrinsic factormucusrennin (chymosin)
- Pyloric - gastrinmucus(sm. amountspepsinogen)
Figure 64-4; Guyton & Hall
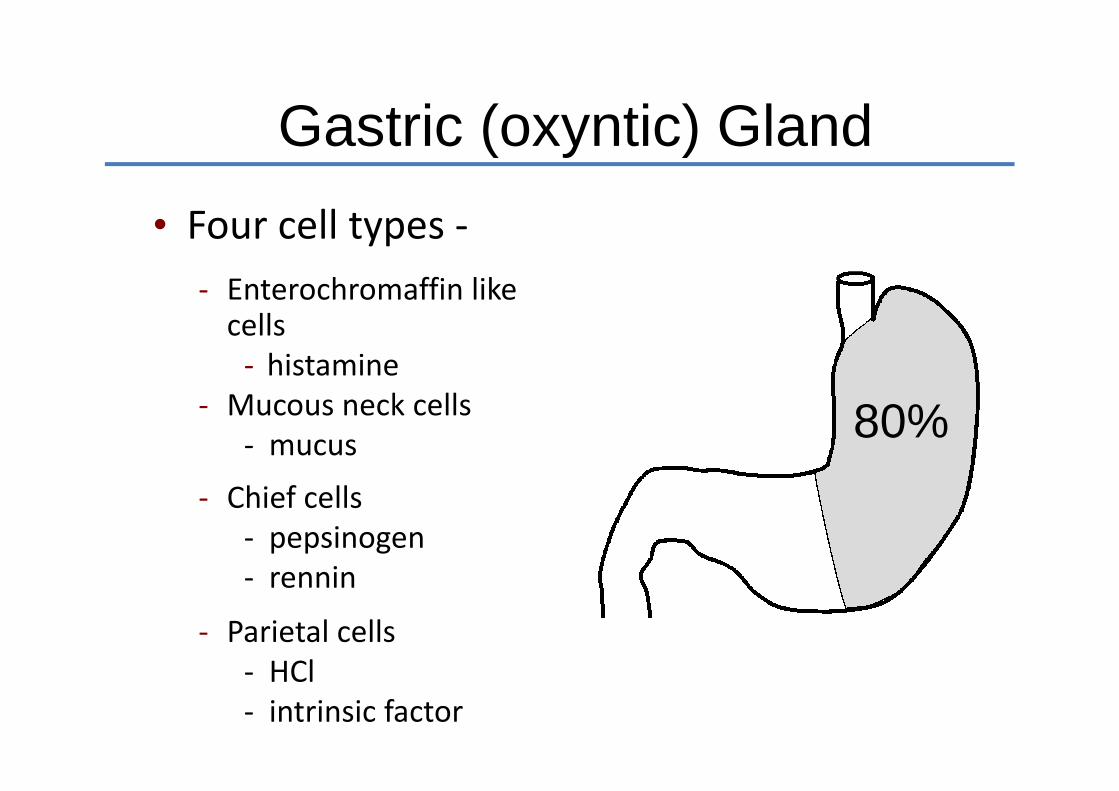
Gastric (oxyntic) Gland
• Four cell types -
- Enterochromaffin likecells
- histamine- Mucous neck cells
- mucus
- Chief cells- pepsinogen- rennin
- Parietal cells- HCl- intrinsic factor
80%
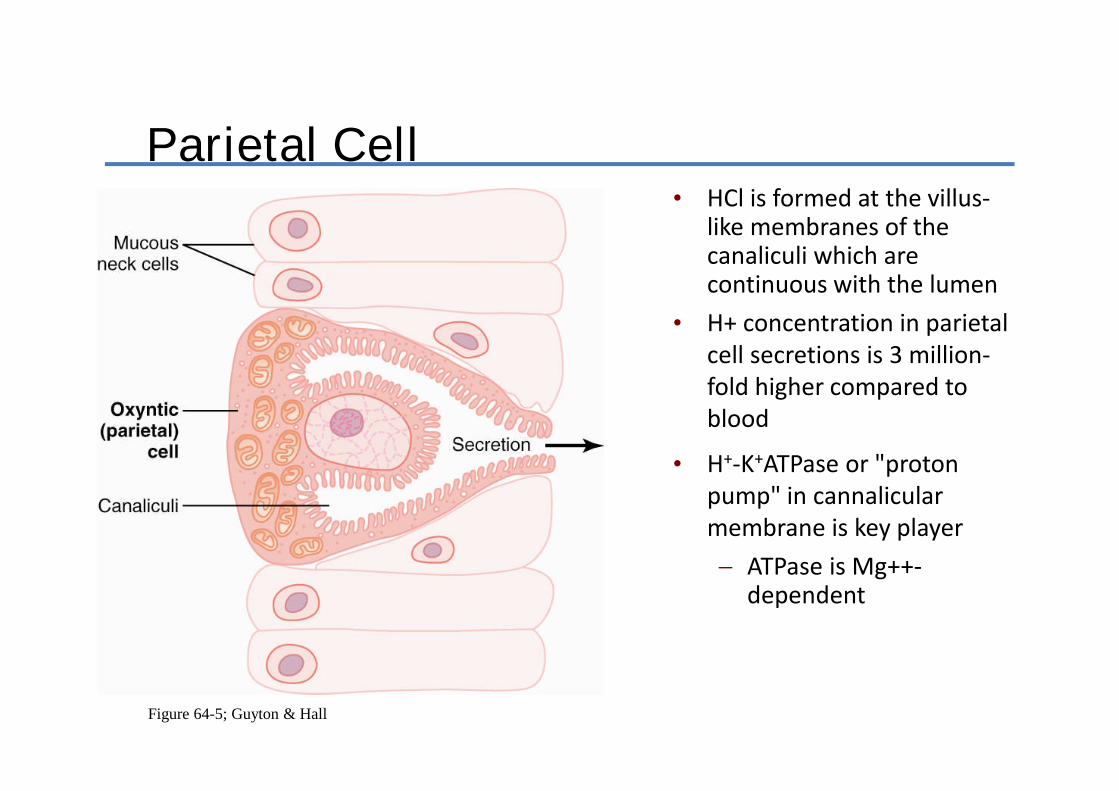
Figure 64-5; Guyton & Hall
Parietal Cell• HCl is formed at the villus-
like membranes of thecanaliculi which arecontinuous with the lumen
• H+ concentration in parietalcell secretions is 3 million-fold higher compared toblood
• H+-K+ATPase or "protonpump" in cannalicularmembrane is key player
ATPase is Mg++-dependent

Gastric Acid
• Three major functions -
- Bacteriostatic- Converts pepsinogen to pepsin- Begins protein digestion (with pepsin)
• Composition-
- HCl 155 mEq/L pH = 0.8!- KCl 15 mEq/L to concentrate this- NaCl 3 mEq/L much acid requires
- 1500 cal/L gastricjuice
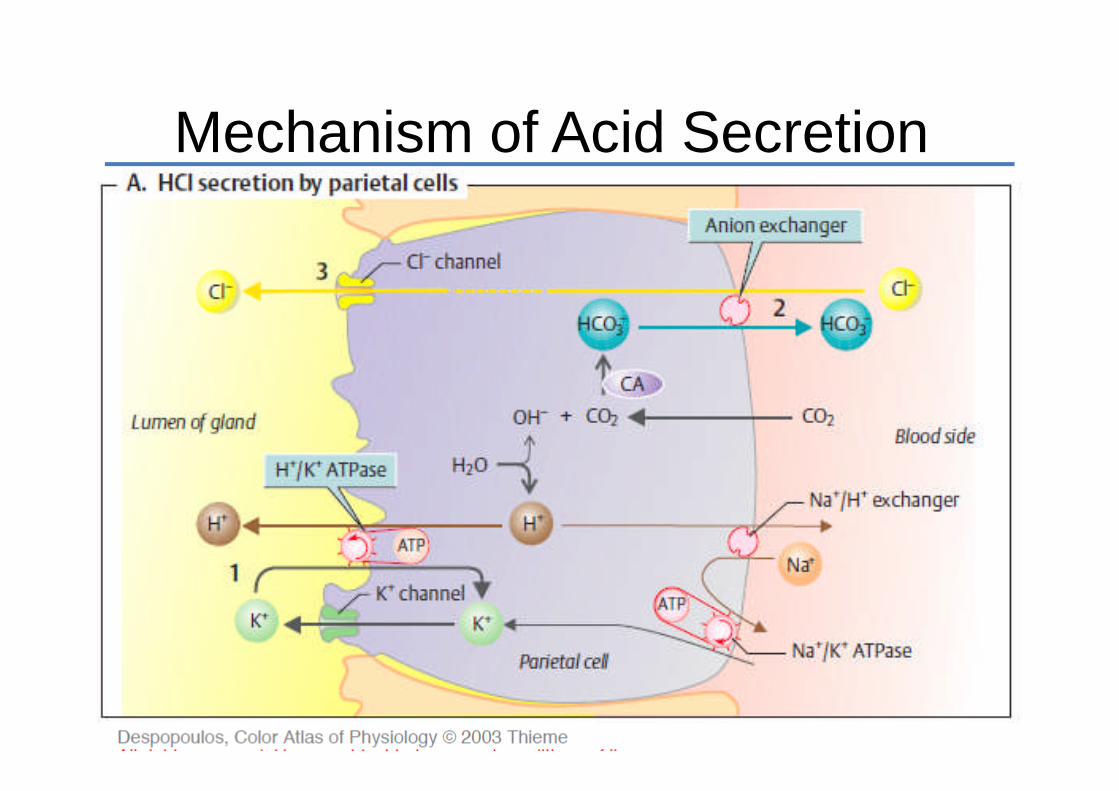
Mechanism of Acid Secretion

Regulation of Gastric Secretion
• Secretion occurs in 3 phases: cephalic, gastric,intestinal
• Gastric secretion is stimulated by neural,paracrine and endocrine mechanisms- Acetylcholine - HCl secretion
- mucus, pepsinogen, and gastrin
- Histamine - HCl secretion
- Gastrin - HCl secretion (1500x more
powerful compared to histamine)

Phases of Gastric Secretion
Figure 64-7; Guyton & Hall
Cephalic Phase
• Seeing, smelling and anticipating food is perceived in brain. Brain tells stomach toprepare for receipt of meal
• Accounts for 30% of acid response to meal -
Stimuli - MechanoreceptorsChemoreceptors (smell and taste)Central pathway (thought)Hypoglycemia
Blocked entirely by vagotomy
Gastric Phase
• Accounts for 60% of acid response to a meal• When meal enters stomach, several factors
come into play•
Increased pH - gastrin release ** Distention - gastrin release **
Ach stimulation of HCl * Peptides / AA - gastrin release **
* blocked by atropine** blocked by acidification of antrum

Intestinal Phase
• Accounts for 10% of acid response to a meal
Distention of small intestine - stimulates acid secretion(enterooxyntin - postulated hormone)
Amino acids - circulating amino acids stimulate acidsecretion via direct effect on parietal cell

Table 16-4, p. 609
Stimulation of Gastric Secretion
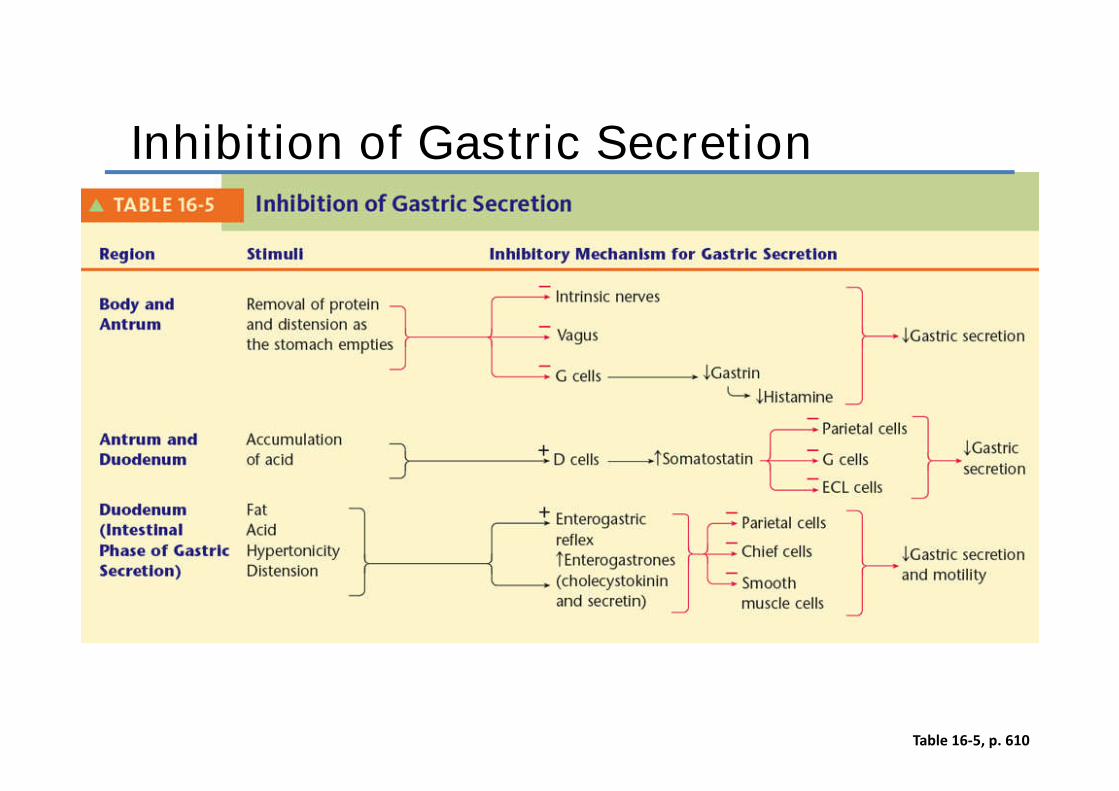
Table 16-5, p. 610
Inhibition of Gastric Secretion

Fig. 16-10, p. 608
Mechanism ofpepsin production
Pepsinogen
• Pepsinogen is an inactive, secreted form ofpepsin -
Acid converts pepsinogen to pepsin
Pepsin (35 kDa) converts more pepsinogen to pepsin
- proteolytic enzyme- optimal pH 1.8 - 3.5- reversibly inactivated > pH 5.0- irreversibly inactivated > pH 7-8

Pepsinogen Secretion
• Signals stimulating secretion of pepsinogen-
- Vagal stimulation as mediated byacetylcholine
- Direct response to gastric acid- Stimulation by secretin, CCK
Intrinsic Factor
• Stomach - Dietary vitamin B12 bound by B12-binding proteins present in gastric juice
• Duodenum - pancreatic proteases digest bindingproteins, releasing vitamin B12 which binds tointrinsic factor
• Ileum - intrinsic factor- vitamin B12 complexabsorbed
• Only indispensable substance in gastric juice
• Ileal disease, resection, atrophic gastritis- Lack of B12 - pernicious anemia

Rennin (Chymosin)
• Proteolytic enzyme - causes milk to curdle instomach
• Milk retained in stomach and released moreslowly
• Rennin secretion - maximal first few days afterbirth. Replaced by secretion of pepsin as majorgastric protease
• Secreted as inactive proenzyme (prochymosin)that is activated on exposure to acid

Pyloric Gland
• Three cell types -
G-cells - release gastrin D-cells – release somatostatin Mucus neck cells
- mucous- Few peptic cells
20%
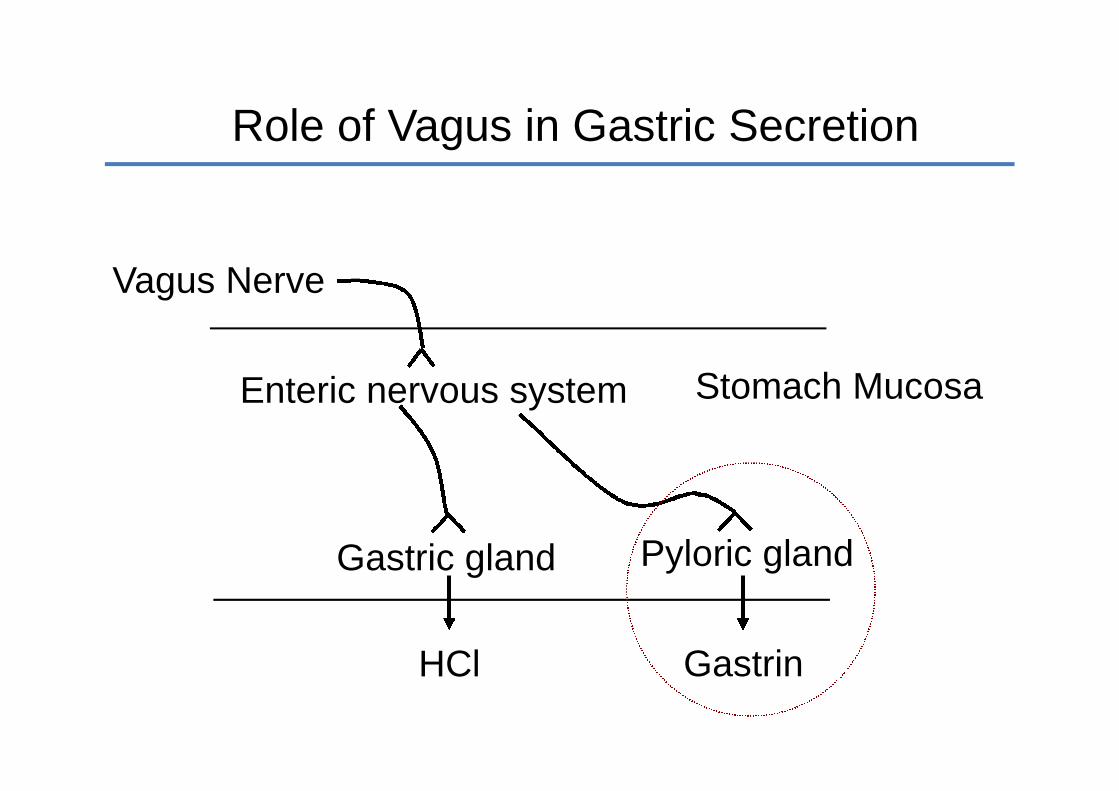
Role of Vagus in Gastric Secretion
Stomach MucosaEnteric nervous system
Vagus Nerve
Gastric gland
HCl
Pyloric gland
Gastrin

Regulation of Gastrin Secretion
• Vagal control Gastrin secretion not blocked by atropine Gastrin releasing peptide - stimulates gastrin release
from G-cell Somatostatin - inhibits gastrin release
from G-cell
• Antrum acidification - pH <3 inhibits gastrinrelease
• Sm peptides and amino acids - directlystimulate gastrin release from G-cell

Regulation of Gastrin SecretionVagus Nerve
AChACh
GRP ACh
Somatostatin CellGastrin CellSS
Gastrin
peptides, amino acids H+
+ -
Regulation of Histamine Secretion
• Gastrin and acetylcholine stimulate histaminerelease from enterochromaffin-like (ECL) cells
• ECL cells are a specialized endocrine cell ingastric mucosa
• Proliferation of ECL cells occurs in associationwith hypergastrinemic states -
Gastrin-secreting tumors Long term therapy with drugs that block acid secretion

Multiplicative Effect of Secretagogues
• Gastrin, acetylcholine and histamine potentiate the effects of theothers- Histamine potentiates effects of gastrin and acetylcholine. H2 blockers
attenuate secretory responses to both acetylcholine and gastrin.
- Acetylcholine potentiates effects of gastrin and histamine. Atropineattenuates secretory effects of histamine and gastrin.
H+
Histamine
Cm
Cm CmAt
Cm, CimetidineAt, Atropine

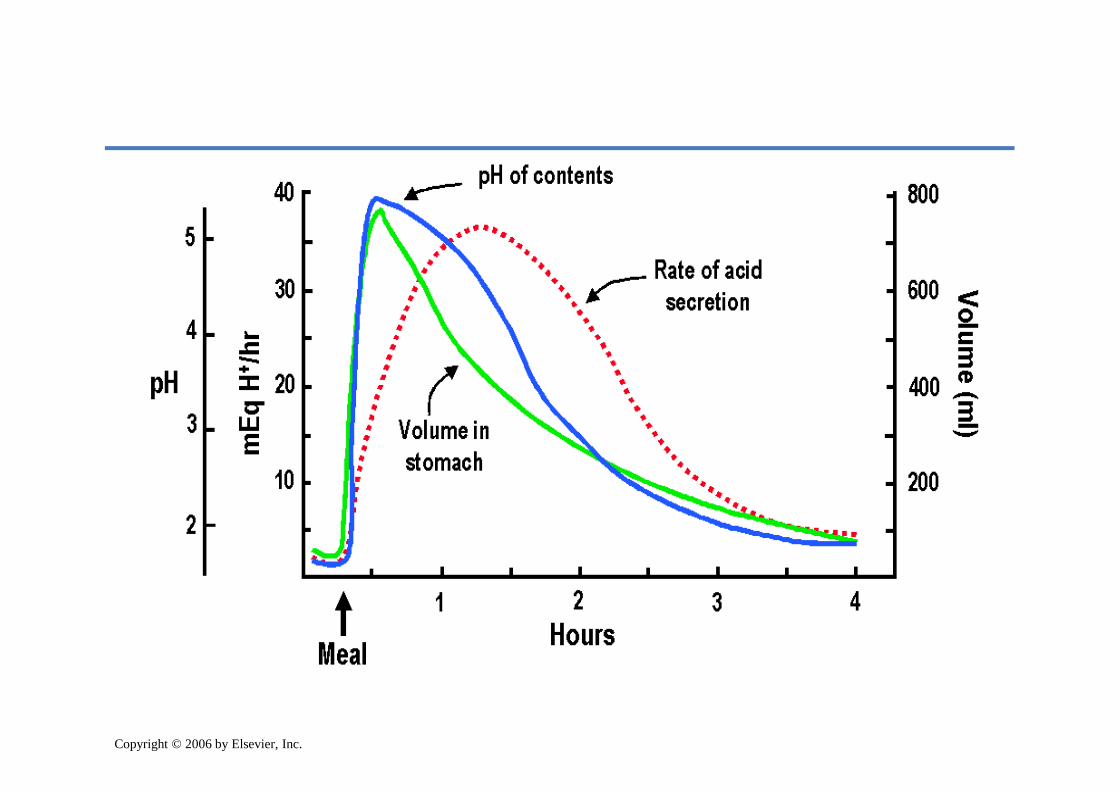
Acid Response to a Meal
• Duration of gastric acid response to mealis a function of -
1. Intragastric pH2. Nature of chyme entering duodenum
• Before meal - pH is low - acid secretion issuppressed Acid stimulates somatostatin release (which
decreases gastrin secretion)
Acid has direct effect to suppress parietal cellsecretion

Acid Response to a Meal (cont’d)
Meal (early) - acid secretion increases because - Cephalic phase (vagal) Gastric pH rises (disinhibition of somatostatin effect) Chemical nature of food (protein, etc.)
Meal (late) - acid secretion decreases because - Buffering capacity of food is saturated As pH falls, acid inhibits further secretion of gastrin and acid
secretion wanes (negative feedback) Chyme entering duo further inhibits acid secretion (acid, osmolarity,
fat - same as inhibits gastric emptying)
Copyright © 2006 by Elsevier, Inc.

Mechanisms Inhibiting Acid Secretion
Inhibits DirectlyRegion Stimulus Mediation gastrin inhibits acid
release secretion
Oxynticgland area
Antrum
Acid(pH < 3.0) Somatostatin YES YES
SecretinNervous reflex
Unidentifiedenterogasterone
Unidentifiedenterogasterone
GIP
YESYES
YES
YES
YES
YES
YES
Acid
Hyper-osmoticsolutions
Fattyacids
Duodenum
Duodenumand
Jejunum
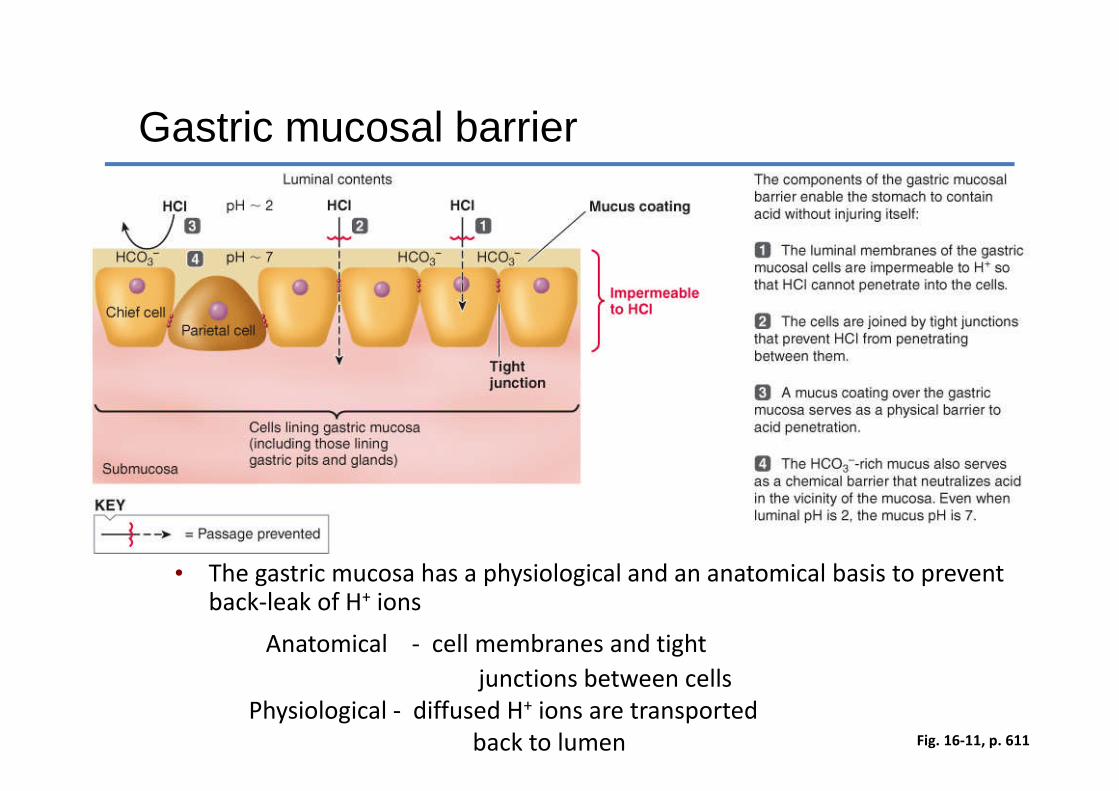
Fig. 16-11, p. 611
Gastric mucosal barrier
• The gastric mucosa has a physiological and an anatomical basis to preventback-leak of H+ ions
Anatomical - cell membranes and tight
junctions between cellsPhysiological - diffused H+ ions are transported
back to lumen

Integrity of Mucosal Barrier
Barrier HealthyNo Ulcers
BarrierDamagedGastritis,Ulcers
Strengthensmucus, HCO3
-
secretion, gastrin,PGs, epidermalgrowth factor
WeakensH. pylori, aspirin,
ethanol,NSAIDs,bile salts

Damaged Gastric Mucosal Barrier
• H+ back-leaks into mucosa in exchange forNa+. This is a forerunner to gastric ulcer -
Decreased cell pH leads to cell death
Damaged mast cells (ECL cells) leak histamine
Viscous cycle - Histamine .. vascular damage ..
local ischemia .. greater leakage
of H+.. more cell death ...

Treatments for peptic ulcer diseases
Agents Mechanism
Antacids Neutralization of acidAnticholinergics Inhib. of Ach stimulated acid
secretionH2 receptor antag. Inhib. of histamine-dependent
acid secretionOmeprazole Inhib. of H+ K+ ATPaseCoating agents(sucralfate, CBS) Provide protective layerProstaglandins(E series) Inhibit acid secretion & enhance
cytoprotection
Pancreas• As chyme moves into small intestine; two
things must happen:
1. Acid must be neutralized to prevent damage toduodenal mucosa
2. Nutrients – (proteins, fats and starch) must bebroken down much further so their constituentscan be absorbed
• Critical role in accomplishing both objectives
Digestive enzymes for all food types
Bicarbonate solution to neutralize acid chyme
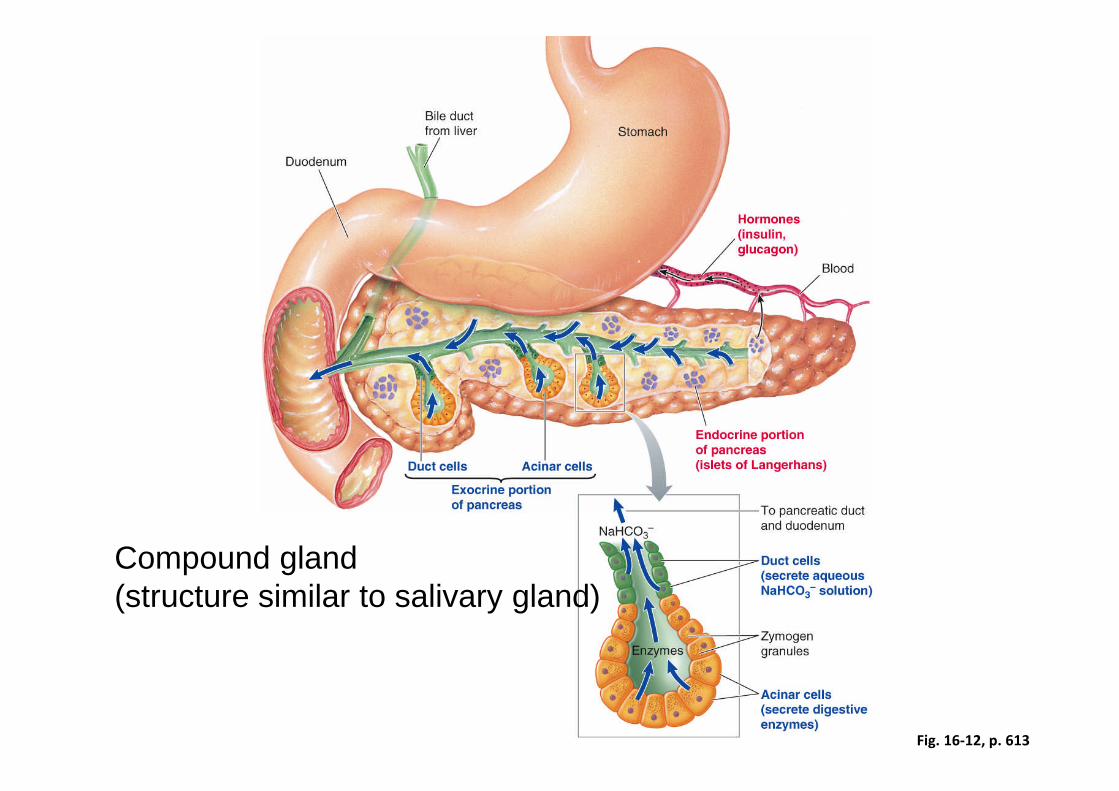
Fig. 16-12, p. 613
Compound gland(structure similar to salivary gland)
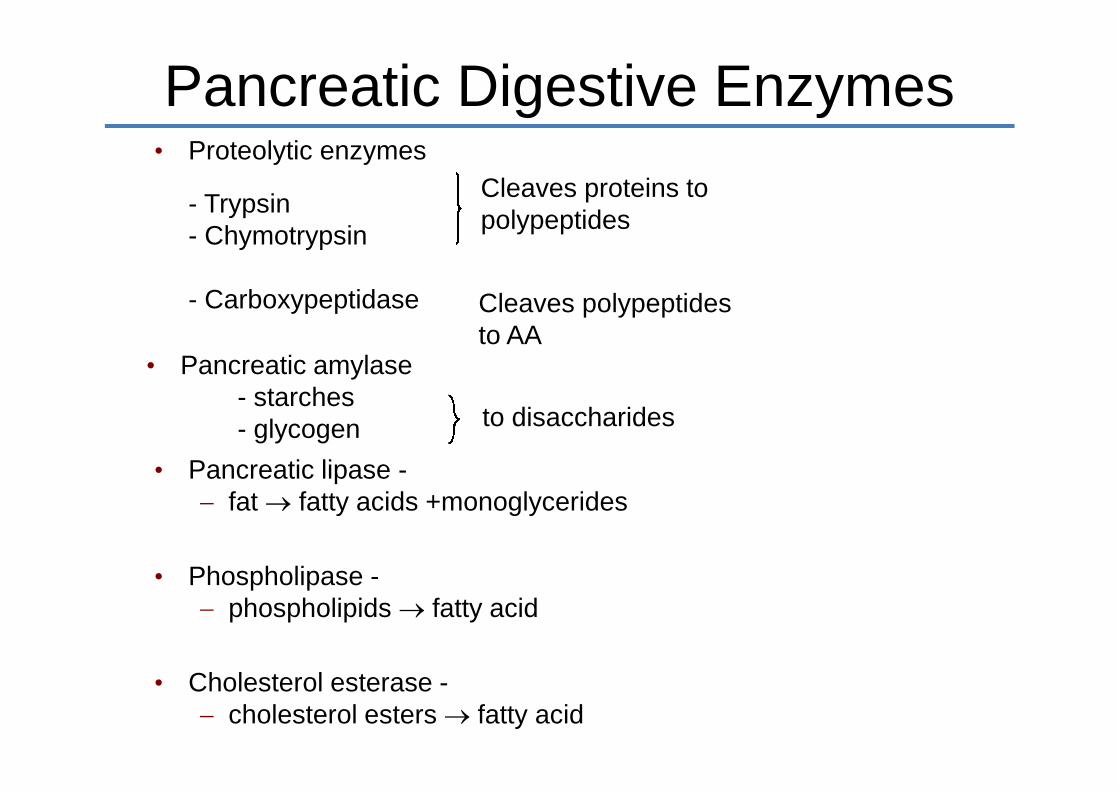
Pancreatic Digestive Enzymes• Proteolytic enzymes
- Trypsin- Chymotrypsin
- Carboxypeptidase
Cleaves proteins topolypeptides
Cleaves polypeptidesto AA
• Pancreatic amylase- starches- glycogen to disaccharides
• Pancreatic lipase - fat fatty acids +monoglycerides
• Phospholipase - phospholipids fatty acid
• Cholesterol esterase - cholesterol esters fatty acid
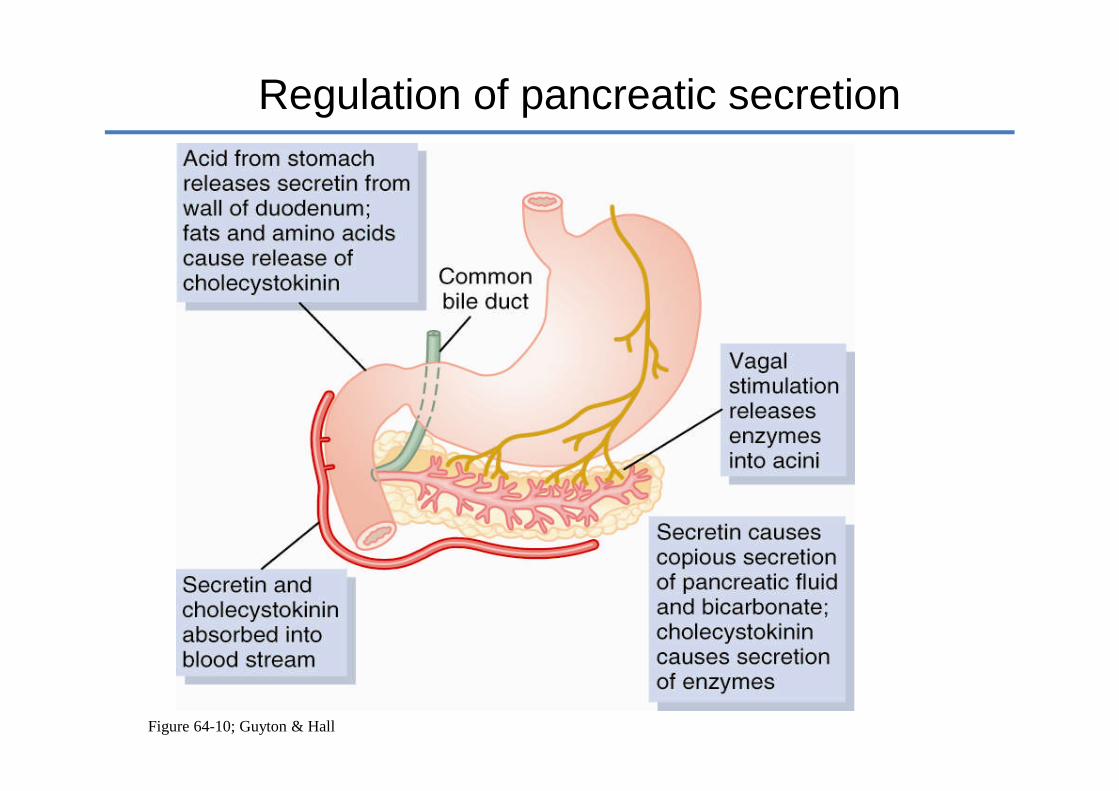
Regulation of pancreatic secretion
Figure 64-10; Guyton & Hall
Vagal stim.
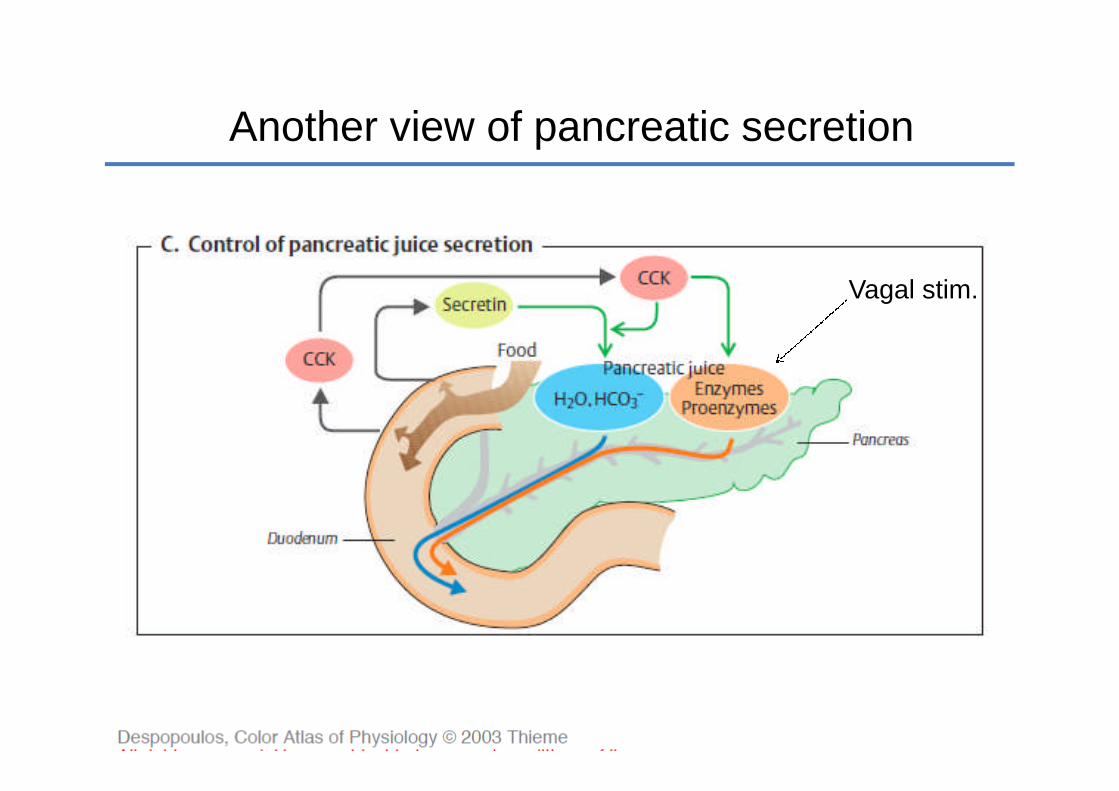
Another view of pancreatic secretion
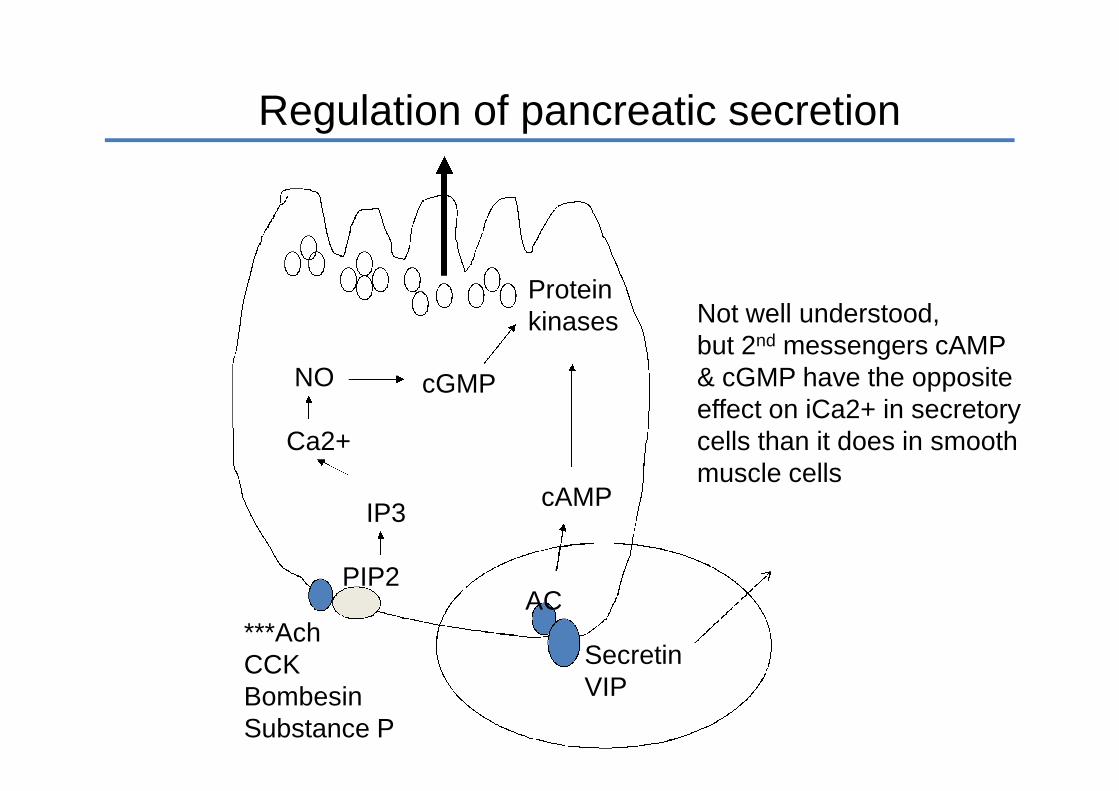
***AchCCKBombesinSubstance P
SecretinVIP
ACPIP2
cAMPIP3
Ca2+
cGMP
Regulation of acinar cell secretion
NO
Proteinkinases Not well understood,
but 2nd messengers cAMP& cGMP have the oppositeeffect on iCa2+ in secretorycells than it does in smoothmuscle cells
Regulation of pancreatic secretion

Why Doesn’t the Pancreas Digest Itself?
• Proteolytic enzymes stored and secreted in aninactive form - (also, a trypsin inhibitor is presentin cells)
• Trypsin inhib. prevents trypsinogen cleavage inacini & ducts (lack of causes acute pancreatitis)
trypsinogen trypsin
chymotrypsinogen chymotrypsin
procarboxypeptidase carboxypeptidase
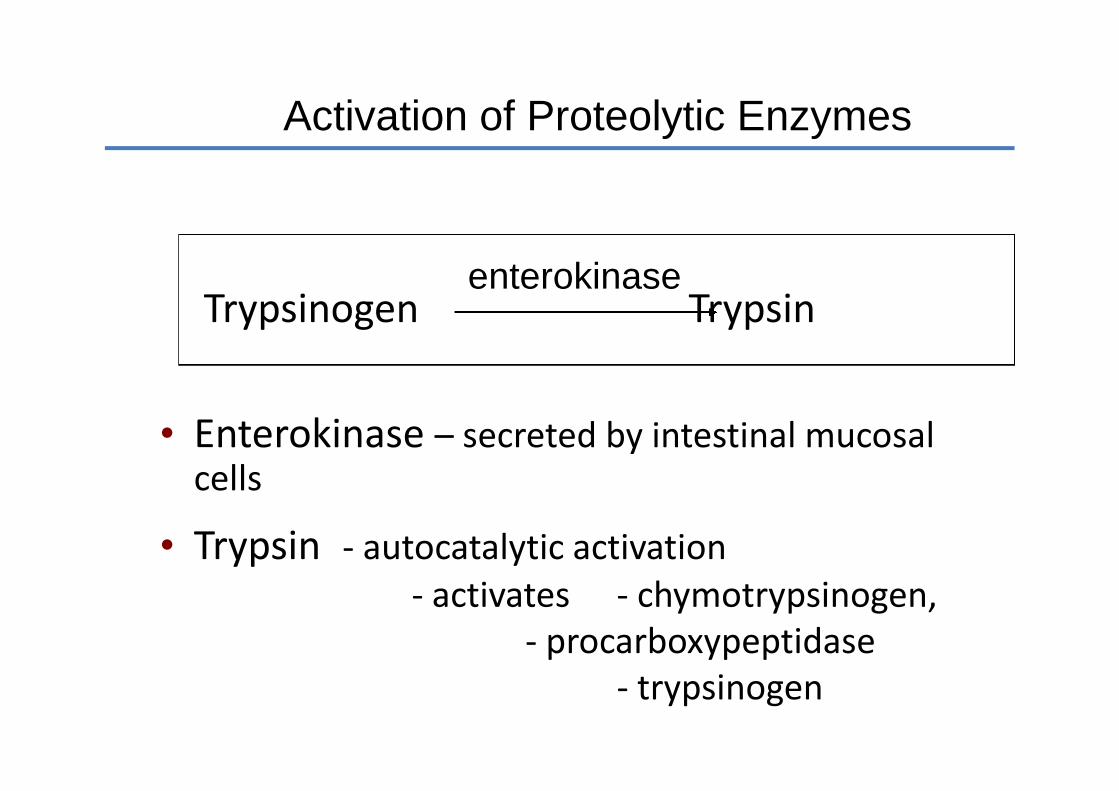
Activation of Proteolytic Enzymes
Trypsinogen Trypsin
• Enterokinase – secreted by intestinal mucosalcells
• Trypsin - autocatalytic activation- activates - chymotrypsinogen,
- procarboxypeptidase- trypsinogen
enterokinase
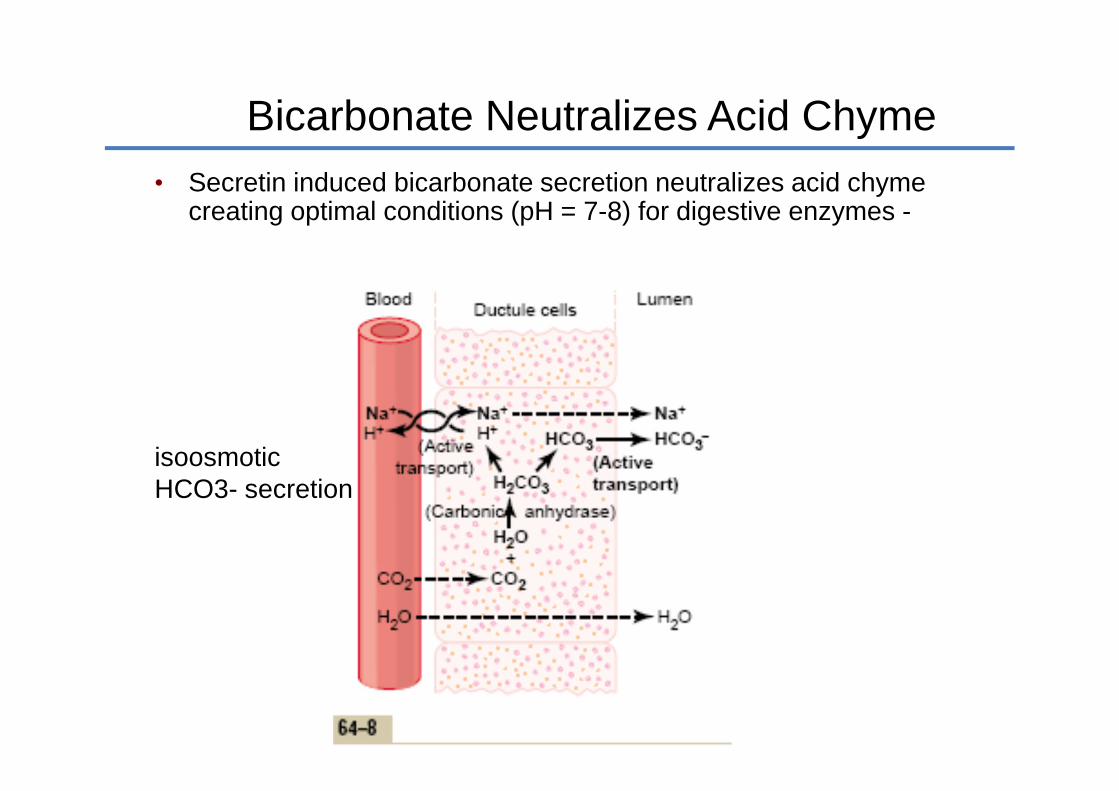
Bicarbonate Neutralizes Acid Chyme
• Secretin induced bicarbonate secretion neutralizes acid chymecreating optimal conditions (pH = 7-8) for digestive enzymes -
isoosmoticHCO3- secretion

Model of Bicarbonate Secretion
1. CO2 combines with H2O in presence of carbonicanyhydrase in cell → H2CO3
2. H2CO3 dissociates into HCO3- and H+
3. H+ exchanged for Na+ across basolateral membrane,active transport (Na+ gradient established by usual Na +K +
ATPase)
4. HCO3- moves out of cell across apical membrane with
Na+
5. Na+ moves down electrochemical gradient. Watermoves into lumen establishing osmotic equilibrium.(Pancreatic juice always isotonic.)

Regulation of Pancreatic Secretion
• Secretion of fluid and HCO3- dependent
upon amount of acid entering duodenum
• Secretion of enzymes dependent uponamount of fat and protein enteringduodenum
Acetylcholine - vagovagal reflexes
Cholecystokinin - fat and protein
Secretin - acid
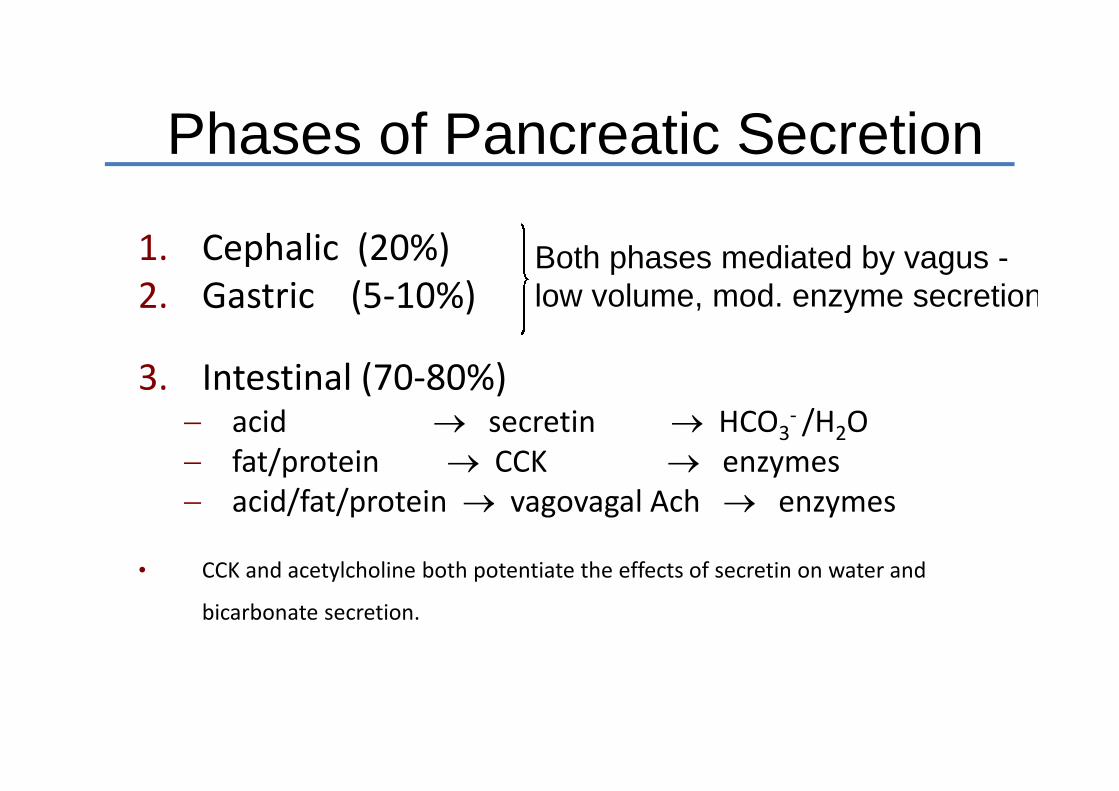
Phases of Pancreatic Secretion
1. Cephalic (20%)2. Gastric (5-10%)
3. Intestinal (70-80%) acid secretin HCO3
- /H2O fat/protein CCK enzymes acid/fat/protein vagovagal Ach enzymes
• CCK and acetylcholine both potentiate the effects of secretin on water and
bicarbonate secretion.
Both phases mediated by vagus -low volume, mod. enzyme secretion
Pancreatic HCO3- Output (Secretin)
Response to Duodenal Acidification
• Secretin released when pH < 4.5.
• Below pH = 3, secretin release ismaximal in segment of duodenum.Further release of secretin dependsupon area of small intestine affected.(Maximal bicarbonate response is 30mEq/hr)
• During meal pH rarely < 3.5 or 4.0.

Distribution of GI Hormones
• Digestive products are equally effective inreleasing secretin when applied to any partof duodenum or jejunum.
Secretin
Fundus Antrum Duo Jejun Ileum Colon

Pancreatic Failure
• Digestion is abnormal when pancreas failsto secrete normal amounts of enzymes
Pancreatitis Removal of pancreatic head - malignancy
• Without pancreatic enzymes - 60% fat not absorbed (steatorrhea) 30-40% protein and carbohydrates not absorbed
Pancreatitis
• Pancreatitis = inflammation of pancreas. Autodigestiontheory can explain condition.
• Chronic pancreatitis - (multiple shared causes) alcohol - most common cause in adults cystic fibrosis - most common cause in children
• Acute pancreatitis - (multiple shared causes) gallstones - most common cause
Secretion Failure in Cystic Fibrosis
•1/29 Caucasians carry mutation in 1 copy of CFTR gene;CF occurs at about 1/2000 Caucasian births
•CF patients lack chloride transporter at apicalmembrane.
• Watery ductal secretion decreases whichconcentrates acinar secretions in ducts.
• Precipitation of proteinaceous secretions blockducts and can destroy gland by autodigestion.
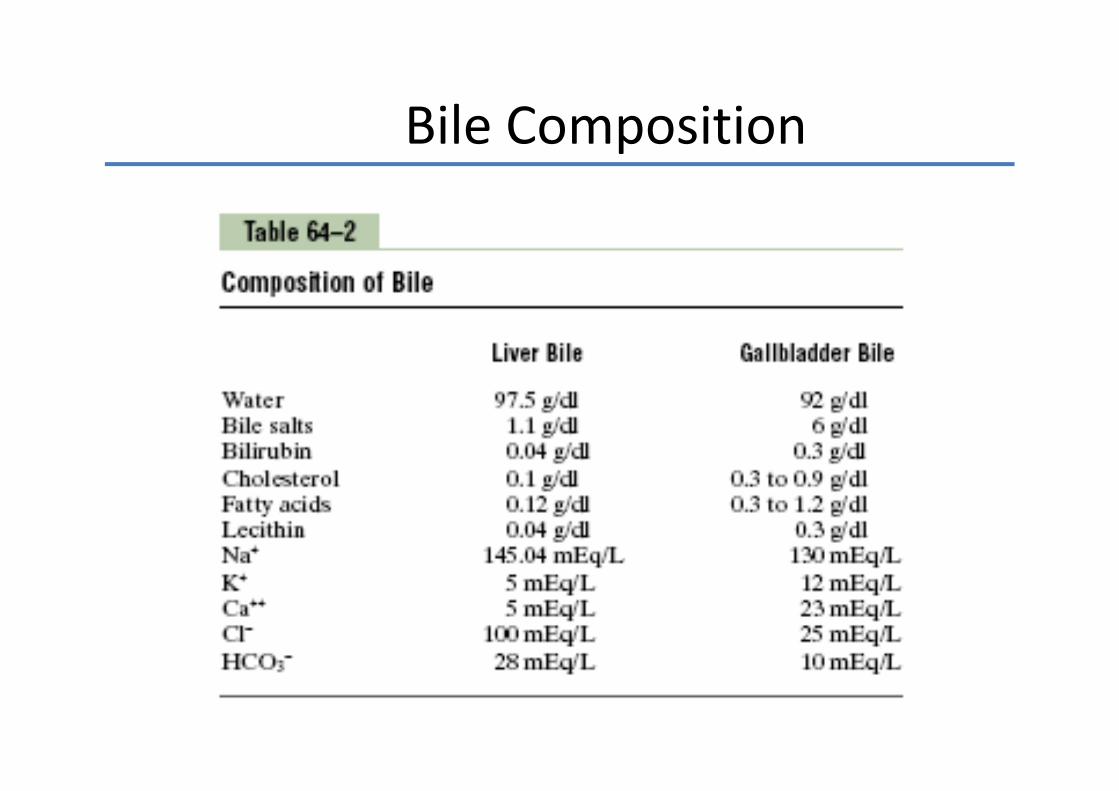
Bile Composition
Bile Secretion
• Secretion in 2 stages1. Hepatocytes secrete bile acids, cholesterol into bile
canaliculi Bile flows in canaliculi to terminal bileducts, then into the hepatic bile duct & finally thecommon bile duct
2. NaHCO3 & water added by bile duct epithelia,(stim. by secretin) ↑ volume
• Bile concentrated when stored in gallbladder 30-60 mL Active Na+ transport across epithelia 2°
transport of Cl- & water Concentrates bile 5-20 fold
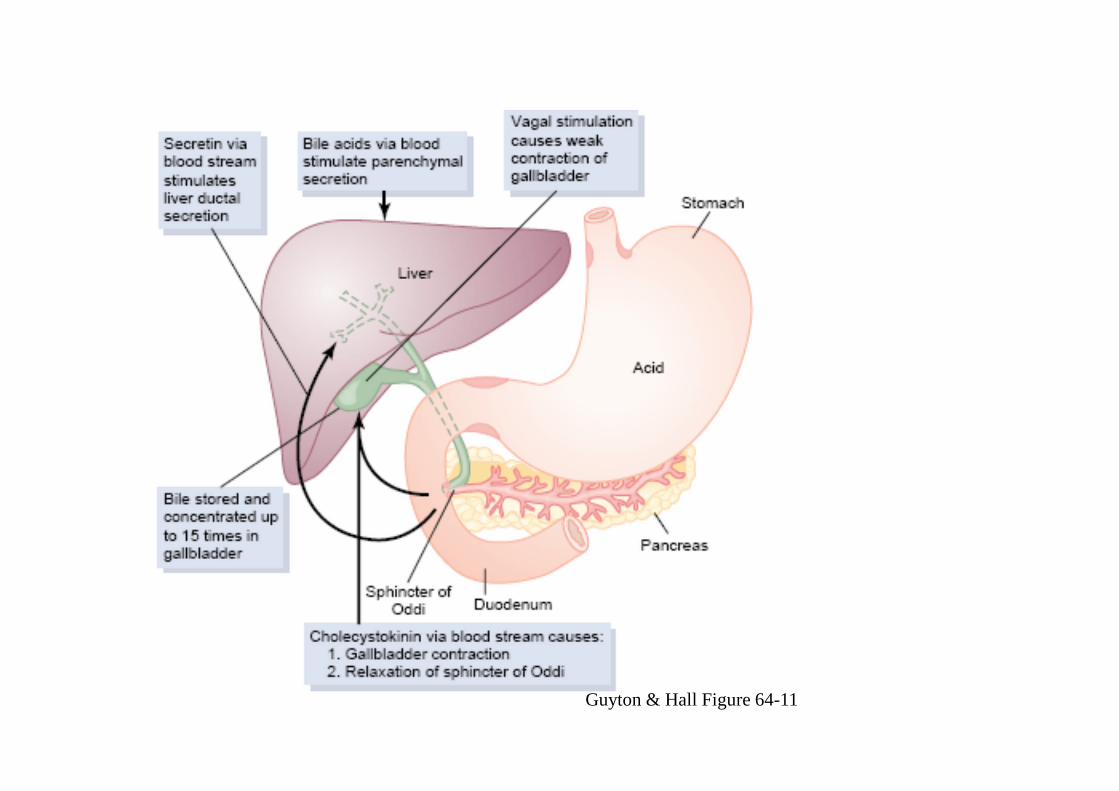
Guyton & Hall Figure 64-11

Fig. 16-16, p. 618
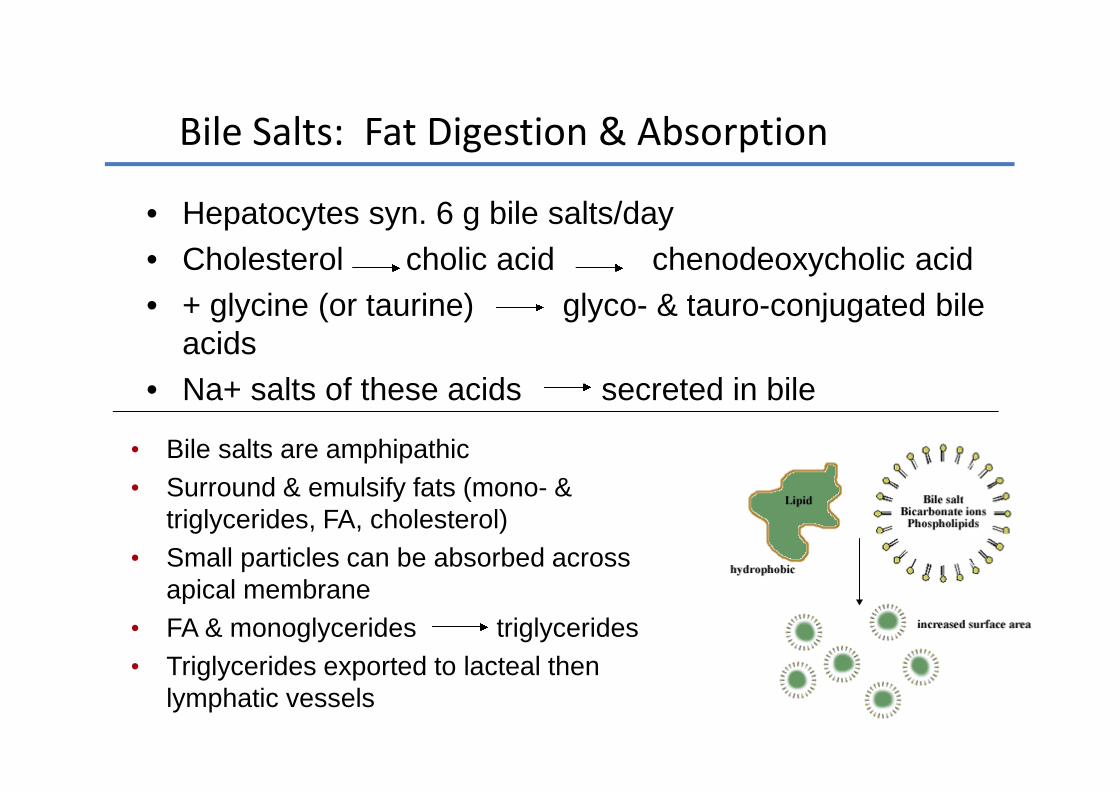
Bile Salts: Fat Digestion & Absorption
• Hepatocytes syn. 6 g bile salts/day
• Cholesterol cholic acid chenodeoxycholic acid
• + glycine (or taurine) glyco- & tauro-conjugated bileacids
• Na+ salts of these acids secreted in bile
• Bile salts are amphipathic
• Surround & emulsify fats (mono- &triglycerides, FA, cholesterol)
• Small particles can be absorbed acrossapical membrane
• FA & monoglycerides triglycerides
• Triglycerides exported to lacteal thenlymphatic vessels

Secretions of Small Intestine
• Brunner’s glands secrete an alkaline mucus. Compound mucus gland in duodenum Protects mucosa from acid chyme Stimulated by local irritation - vagus (Ach) Inhibited by sympathetics (NE)
• Crypts of Lieberkühn - mostly secrete water -like fluid - 1800 ml/day

Crypt of Lieberkuhn in theSmall Intestine
Secretions of the Large Intestine
• Large intestine also contains crypts ofLieberkühn but there are no villi orenzymes.
• Crypts mainly secrete alkaline mucus
• Mucus secretion increased byparasympathetic stimulation

















![[Eng.economics] Lecture #3](https://img.pdfslide.tips/doc/110x75/5695cf9d1a28ab9b028ed24a/engeconomics-lecture-3.jpg)










