Embed Size (px)
Citation preview

Gregory A. Jicha, M.D. Ph.D.Assistant Professor of NeurologyUK Alzheimer’s Disease CenterUK Alzheimer s Disease CenterSanders‐Brown Center on Aging

There are now more than 5 million people in the United States living with Alzheimer’s, almost 8 h i KY80,000 here in KY
Every 72 seconds, someone develops Alzheimer’s, i h d i KY l with 3 to 4 new cases per day in KY alone
Kentucky ranks 8th in state death rates/100,000 l f l hpopulation for Alzheimer’s
Kentucky ranks 13th in state rates for nursing home residents with cognitive impairment


22
23
atio
n
260
265
atio
n Heart disease
18
19
20
21
22
per 1
00K
pop
ula
245
250
255
260
per 1
00K
pop
ula
AD
15
16
17
18
1999 2000 2001 2002 2003
Dea
th ra
tes
230
235
240
1999 2000 2001 2002 2003
Dea
th ra
tes
1999 2000 2001 2002 2003 1999 2000 2001 2002 2003
196
197
198
pula
tion
59
60
pula
tion
193
194
195
196
es p
er 1
00K
pop
55
56
57
58es
per
100
K p
op
Neoplasm CVD
190
191
192
1999 2000 2001 2002 2003
Dea
th ra
t
53
54
55
1999 2000 2001 2002 2003
Dea
th ra
tNeoplasm CVD

The direct and indirect costs of Alzheimer’s and other dementias amount to more than $148 billion annually
d b ll d In 2005, Medicare spent $91 billion (compared to $117 billion on the Iraq war) for persons with Alzheimer’s and other dementias projected to Alzheimer s and other dementias, projected to increase to $160 billion by 2010 and $189 billion by 2015y 5
Congress spent only $647 million on AD research in 2005

DSM IV CriteriaDSM‐IV Criteria
Memory and at least one other cog domain involvedinvolved
Impaired general cognitive function
Social, educational, occupational function impairedp
No medically reversible cause found

Good Brain Bad Brain

Alzheimer’s disease (NINDS ADRDA)Alzheimer s disease (NINDS‐ADRDA)
•Dementia by DSM‐III‐R/V criteria
•Deficits in two or more areas of cognition•Deficits in two or more areas of cognition
•Progressive worsening of memory and cognitive dysfunction
•Onset age 40 90•Onset age 40‐90
•Absence of other systemic/brain disorders

HypertensionDi i Diagnosis
Treatment Adaptation to disease process Adaptation to disease process Prevention of complications End stage of the disease process End stage of the disease process
Di i Diagnosis This is easy…

Drug Trade Name Diuretics (partial list)Chlorthalidone (G)‐HygrotonHydrochlorothiazide (G)‐Hydrodiuril, Microzide, EsidrixIndapamide‐ LozolMetolazone‐Mykrox, Zaroxolyn
Loop diureticsBumetanide (G)‐ Bumex
Calcium antagonistsNondihydropyridinesDiltiazem hydrochloride‐ Cardizem SR, CardizemCD, Dilacor XR, TiazacVerapamil hydrochloride‐ Isoptin SR, Calan SR Verelan, Covera HS
DihydropyridinesAmlodipine besylate‐ Norvasc
ACE inhibitors and diureticsBenazepril hydrochloride and hydrochlorothiazide‐Lotensin HCTCaptopril and hydrochlorothiazide‐ CapozideEnalapril maleate and hydrochlorothiazide‐VasereticLisinopril and hydrochlorothiazide‐ Prinzide, Zestoretic
Bumetanide (G) BumexEthacrynic acid‐ EdecrinFurosemide (G)‐ LasixTorsemide‐ Demadex
Potassium‐sparing agentsAmiloride hydrochloride (G)‐MidamorSpironolactone (G‐ AldactoneTriamterene (G)‐Dyrenium
Amlodipine besylate NorvascFelodipine‐ PlendilIsradipine‐DynaCirc, DynaCirc CRNicardipine‐Cardene SRNifedipine‐Procardia XL, Adalat CCNisoldipine‐ Sular
ACE inhibitorsBenazepril hydrochloride‐ LotensinCaptopril (G)‐ Capoten
l l l
Angiotensin II receptor antagonists and diurecticsLosartan potassium and hydrochlorothiazide‐Hyzaar
Calcium antagonists and ACE inhibitorsAmlodipin besylate and benazepril hydrochloride‐LotrelDiltiazem hydrochloride and enalapril maleate‐Teczem
Adrenergic inhibitorsPeripheral agentsReserpine (G)‐ SerpasilCentral alpha‐agonistsClonidinehydrochloride (G)‐ CatapresGuanabenz acetate (G)‐WytensinGuanfacine hydrochloride (G)‐ TenexMethyldopa (G)‐Aldomet
Al h bl k
Enalapril maleate‐ VasotecFosinopril sodium‐MonoprilLisinopril‐ Prinivil, ZestrilMoexipril‐UnivascQuinapril hydrochloride‐ AccuprilRamipril‐AltaceTrandolapril‐Mavik
Angiotensin II receptor blockersLosartan potassium‐ Cozaar
TeczemVerapamil hydrochloride (extended release) and trandolapril Tarka‐ Felodipine and enalaprilmaleate‐ Lexxel
Other combinations Triamterene and hydrochlorothiazide‐ Dyazide, Maxide Spironolactone and hydrochlorothiazideAldactazideAmiloride hydrochloride and hydrochlorothiazideModuretic
Alpha‐blockersDoxazosin mesylate‐ CarduraPrazosin hydrochloride (G)‐MinipressTerazosin hydrochloride‐ Hytrin
Beta‐blockersAcebutolol‐ SectralAtenolol (G)‐ TenorminBetaxolol‐ KerloneBisoprolol fumarate‐ ZebetaCarteolol hydrochloride‐ Cartrol
Losartan potassium CozaarValsartan‐ DiovanIrbesartan‐ Avapro
(G) indicates generic available.
DrugTrade Name (Combination Drugs) Beta‐adrenergic blockers and diuretics
Guanethidine monosulfate and hydrochlorothiazideEsimilHydralazine hydrochloride and hydrochlorothiazideApresazideMethyldopa and hydrochlorothiazideAldorilReserpine and hydrochlorothiazideHydropresReserpine hydralazine hydrochloride, and hydrochlorothiazidey
Metoprolol tartrate (G)‐ LopressorMetoprolol succinate‐ Toprol‐XLNadolol (G)‐ CorgardPenbutolol sulfate‐ LevatolPindolol (G)‐ ViskenPropranolol hydrochloride (G)‐ Inderal, Inderal LATimolol maleate (G)‐ Blocadren
Combined alpha‐ and beta‐blockersC dil l C
Atenolol and chlorthalidone‐ TenoreticBisoprolol fumarate and hydrochlorothiazide‐ ZiacMetoprolol tartrate and hydrochlorothiazide‐Lopressor HCTNadolol and bendroflumethiazide‐ CorzidePropranolol hydrochloride and hydrochlorothiazide‐ InderidePropranolol hydrochloride and hydrochlorothiazide (extended release)‐ Inderide LATimolol maleate and hydrochlorothiazide‐ Timolide
ySer‐Ap‐EsClonidine hydrochloride and chlorthalidoneCombipresMethyldopa and chlorothiazideAldochlorReserpine and chlorthalidoneDemi‐RegrotonReserpine and chlorothiazideDiupresPrazosin hydrochloride and polythiazideMinizideCarvedilol‐ Coreg
Labetalol hydrochloride (G)‐Normodyne, Trandate
Direct vasodilatorsHydralazine hydrochloride (G)‐ApresolineMinoxidil (G)‐ Loniten
Minizide













22
23
atio
n
260
265
atio
n Heart disease
18
19
20
21
22
per 1
00K
pop
ula
245
250
255
260
per 1
00K
pop
ula
AD
15
16
17
18
1999 2000 2001 2002 2003
Dea
th ra
tes
230
235
240
1999 2000 2001 2002 2003
Dea
th ra
tes
1999 2000 2001 2002 2003 1999 2000 2001 2002 2003
196
197
198
pula
tion
59
60
pula
tion
193
194
195
196
es p
er 1
00K
pop
55
56
57
58es
per
100
K p
op
Neoplasm CVD
190
191
192
1999 2000 2001 2002 2003
Dea
th ra
t
53
54
55
1999 2000 2001 2002 2003
Dea
th ra
tNeoplasm CVD


22
23
atio
n
260
265
atio
n Heart disease
18
19
20
21
22
per 1
00K
pop
ula
245
250
255
260
per 1
00K
pop
ula
AD
15
16
17
18
1999 2000 2001 2002 2003
Dea
th ra
tes
230
235
240
1999 2000 2001 2002 2003
Dea
th ra
tes
1999 2000 2001 2002 2003 1999 2000 2001 2002 2003
196
197
198
pula
tion
59
60
pula
tion
193
194
195
196
es p
er 1
00K
pop
55
56
57
58es
per
100
K p
op
Neoplasm CVD
190
191
192
1999 2000 2001 2002 2003
Dea
th ra
t
53
54
55
1999 2000 2001 2002 2003
Dea
th ra
tNeoplasm CVD


1906‐ first description of Auguste D. age 51
1976‐ cholinergic deficit in AD discovered
1984‐ b‐amyloid discovered as key component of AD plaques
1986‐ tau protein discovered as key component of NFT

Alzheimer’s Alzheimer s disease pathology

1) APP is a membrane‐bound glycoprotein that
2)APP is normally cleaved by ‐secretase and ‐
3) ‐amyloid is toxic to cells and accumulates in brain g y p
may serve as a growth factor in injury and repair
secretase, but in AD, ‐secretase is active
tissue as amyloid plaques, a hallmark of the diseaseinjury and repair of the disease


Increeasing seeverity oAmyloid plaques
of diseaseNFTs
Amyloid plaquese


Check for reversible causes of dementia MMSE or other bedside cognitive testing? MMSE or other bedside cognitive testing? Imaging studies? MRI PET SPECT PIB MRI, PET, SPECT, PIB
Genetic testing? ApoE status ApoE status
Biomarkers?CSF l id & t CSF amyloid & tau

V‐subdural hematoma, reversible posterior l k h l hleukoencephalopathy
I‐Syphilis, HIV, PML T‐trauma, NPH, drugs A‐SLE, Sjogren’s, MS M‐Thyroid, Wernicke’s, Wilson’s, SCD (B12) I‐Vasculitis, Hashimoto’s N‐neoplasm, limbic encephalitis S‐nonconvulsive status (EPC)

Clinical cause of MCI following Medical evaluation per AAN practice parameter
Probable degenerative
B12 deficiencyB12 deficiency
thyroid dysfunction
vascular
NPH
SDH

Benzodiazepines: valium, ativanp , NSAIDs: ASA, ibuprofen, indomethacin, naproxen, sulindac Antidepressants: TCAs, SSRIs Anticonvulsants: PHT VPA CBZ PHB Anticonvulsants: PHT, VPA, CBZ, PHB Antihypertensives: B‐blockers, Ca‐channel blockers H2 receptor antagonists: cimetidine, ranitidine Antibiotics: Cephalexin, metronidazole, fluoroquinolones Anticholinergics: Benztropine, trihexiphenidyl Antiarrhythmics: disopyramide, quinidine, tocanaide, amiodaroney py , q , , Antiparkinson agents: L‐DOPA, pergolide, bromocriptine Muscle relaxants: Baclofen, cyclobenzaprine, methocarbamol Others: antihistamines/decongestants digoxin steroids narcotics Others: antihistamines/decongestants, digoxin, steroids, narcotics

1. Memory loss. Difficulty performing familiar tasks 2. Difficulty performing familiar tasks.
3. Problems with language. Di i t ti t ti d l4. Disorientation to time and place.
5. Poor or decreased judgment. bl h b h k6. Problems with abstract thinking.
7. Misplacing things. 8. Changes in mood or behavior. 9. Changes in personality. 10.Loss of initiative.

33
5M 5
35
MM 5
1
MS 1
213
SE 3
11
E126

Wahlund et al, 1999 Psych Res 90(3): 193‐199

Smith et al, Neurology. 2007 Apr 17;68(16):1268‐73.

Shoghi‐Jadid K, et al. Localization of neurofibrillary tangles and beta‐amyloid plaques in the brains of living patients with Alzheimer disease

Rowe CC et al., Imaging beta‐amyloid burden in aging and dementia. Neurology. 2007 May 15;68(20):1718‐25.

POPULATION AD
E2 8%
E3 77%
E2 4%
E3 58%E3 77%
E4 15%
E3 58%
E4 38%4 5 4 3
Petersen et al., JAMA 1995;273:1274‐1278

No proven serum biomarkers
CSF amyloid and tau are commercially available
Not proven yet
Not covered by most insurance

BiomarkerBiomarker SensitivitySensitivity SpecificitySpecificity Sample (n)Sample (n)
CSF total tauCSF total tau 81.481.4 91.591.5 30273027
CSF CSF phosphophospho--tautau 81.381.3 91.291.2 15881588phosphophospho tautau
CSF AB42CSF AB42 85.985.9 88.588.5 12011201
CSF AB+tauCSF AB+tau 89.389.3 90.290.2 11951195
Blennow K, NeuroRx. 2004 Apr;1(2):213‐25. Review


SecondarySecondaryPreventionPrevention TreatmentTreatmentPrimaryPrimary
PreventionPreventionIntervention:Intervention:
NormalNormal ADADPrePre--
symptomatic symptomatic ADAD
Mild Mild Cognitive Cognitive
ImpairmentImpairment
Clinical Clinical StateState
No DiseaseNo DiseaseNo SymptomsNo Symptoms
Early BrainEarly BrainChangesChanges
No S mptomsNo S mptoms
AD Brain AD Brain ChangesChanges
Mild S mptomsMild S mptoms
Moderate toModerate toSevere Severe
ImpairmentImpairment
BrainBrainPathologic Pathologic StateState
Disease ProgressionDisease Progression
No SymptomsNo Symptoms No SymptomsNo Symptoms Mild SymptomsMild Symptoms ImpairmentImpairmentStateState
Disease ProgressionDisease Progression
National Institute on Aging, USANational Institute on Aging, USA..

AD Research: the Search for Causes
Scientists examine characteristics, lifestyles, and disease rates f f l t th l b t ibl f AD
Epidemiologic Studies
of groups of people to gather clues about possible causes of AD. The NIA is currently funding epidemiologic studies in a variety of different groups. Two of the studies focus on religious communities Researchers conduct yearly exams of physical and communities. Researchers conduct yearly exams of physical and mental status, and studies of donated brains at autopsy. Some early results indicate:
• Mentally stimulating activity protects the brain in some ways.
• In early life, higher skills in grammar and density of ideas are associated with protection against AD in late life.

Green R & DeKosky S, Neurology. 2006 Nov 14;67(9 Suppl 3):S2‐5.

g AD
f dev
elop
inRisk of
Zandi PP et al, JAMA. 2002 Nov 6;288(17):2123‐9.

Schumaker et al, JAMA. 2004 Jun 23;291(24):2947‐58.

McGeer & McGeer, Neurobiol Aging. 2007 May;28(5):639‐47.
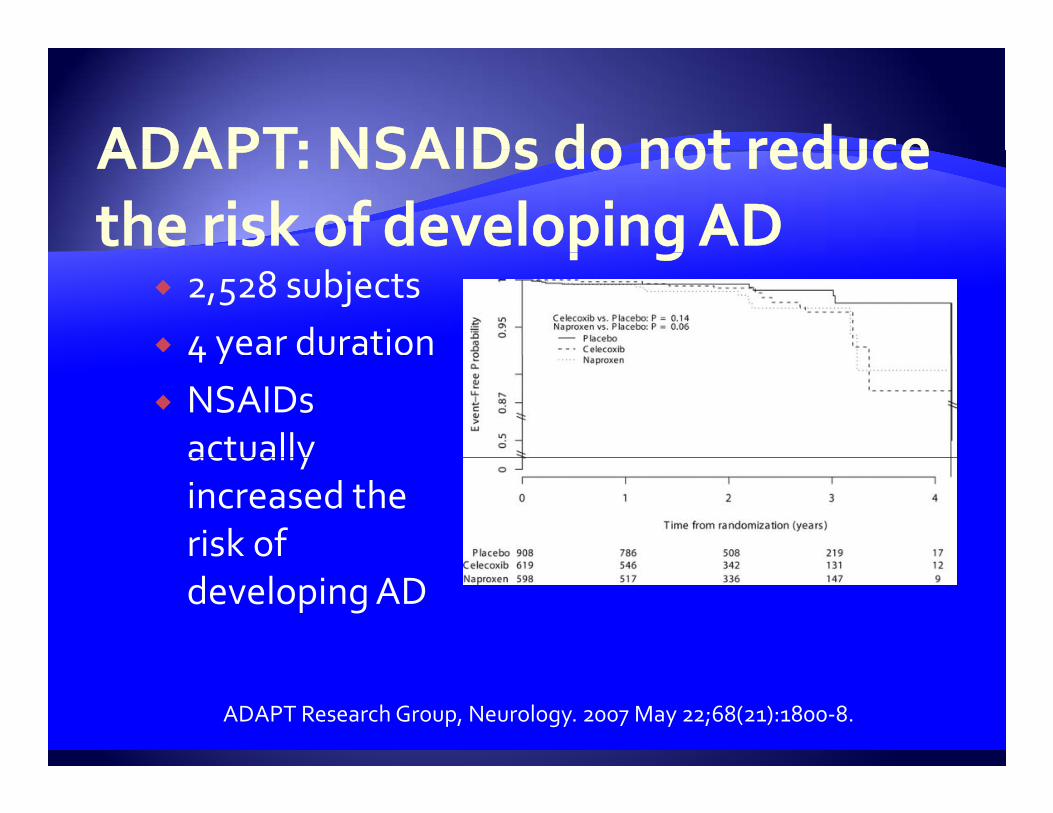
2,528 subjects 4 year duration4 y NSAIDs actually actually increased the risk of developing AD
ADAPT Research Group, Neurology. 2007 May 22;68(21):1800‐8.
AD Research: the Search for TreatmentsDrugs used to treat mild to moderate AD symptoms include:
• Aricept (donepezil)
• Exelon (rivastigmine)Exelon (rivastigmine)
• Razadyne (galantamine)
• Namenda (memantine)
• These drugs can help improve some patients’ abilities to carry out activities up to a year or so, but they do not stop or reverse AD.
Scientists are also studying agents that someday may be useful in preventing AD. For example, they have experimented with a vaccine against AD. Although the first clinical trial was stopped due to side effects in some participants, valuable information was gathered.

e of
AD
e
of A
D
00
55
88
66
Prev
alen
cPr
eval
enc
ons)
ons)
.5.5
11
22
66
44
U.S
. PU
.S. P
(mill
io(m
illio
DelayDelay
5522
Delay Delay (years)(years)
20072007 20172017 20272027 20372037 20472047
YY
00
19971997 20072007 20172017 YearYear
Brookheimer et al. Brookheimer et al. Am J Pub HealthAm J Pub Health. 1998;88:1337. 1998;88:1337--1342.1342.


‐6Improve
0
6
Decline in ADAS‐Cog scorebased on the natural history of
12
18
based on the natural history ofuntreated patients with moderateAlzheimer’s disease* Decline
0 6 12
Cumulative Weeks From Baseline of the Double‐blind Study
9862 74 8526 38 5014
Rogers SL, Friedhoff, LT. Eur Neuropsychopharmacol. 1998;8:67‐75.*Stern RG, et al. Am J Psychiatry. 1994;151:390‐396.

*** p < 0.0001** p < 0.005
Holmes: Neurology, Volume 63(2).July 27, 2004.214‐219

Normal functionNormal functionNormal functionNormal function
Alzheimer’s Alzheimer’s diseasedisease
Treated with Treated with M tiM tiMemantineMemantine
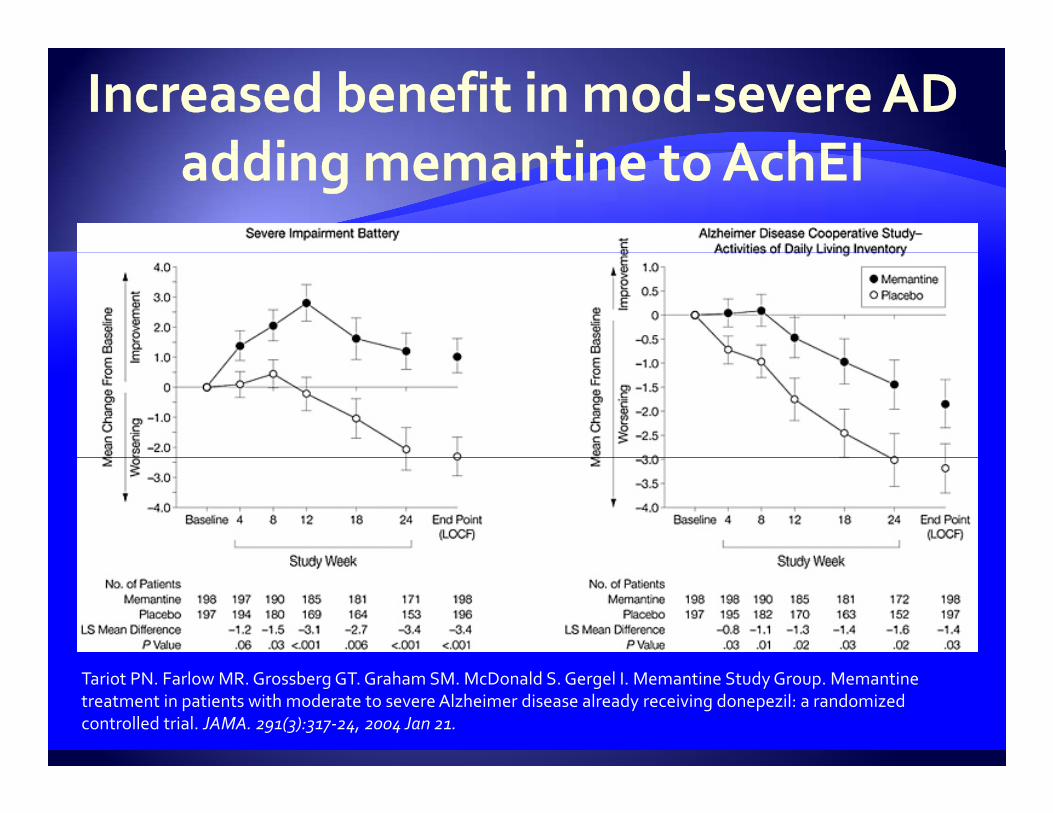
Tariot PN. Farlow MR. Grossberg GT. Graham SM. McDonald S. Gergel I. Memantine Study Group. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA. 291(3):317‐24, 2004 Jan 21.

100%
Level of detection
ction
of F
unc
Leve
l
TIME

100%Mi i l i t
Level of detection
Minimal improvement seen in most cases
ction Or here?
of F
unc
Leve
l
In several years do you want to be here?
TIME
you want to be here?

100%
Level of detection
ction
Or here?
Or here?
of F
unc Or here?
Or here?
Leve
l
In several years do you want to be here? O h ?
TIME
you want to be here? Or here?


5C 5
5
Case 1: 1995
3
5
72 yo ♂
Forgetful
No functional impairment 5
3
No functional impairment
Tests normal
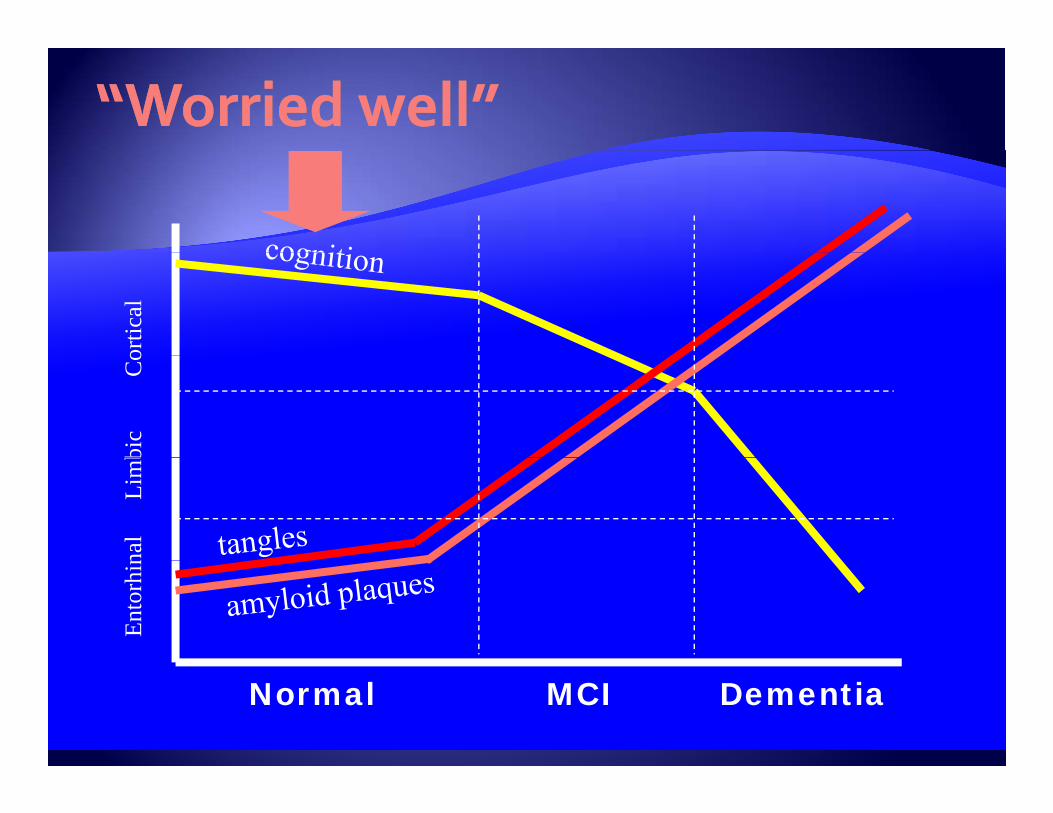
Dx: “worried well”2
1
33
1
11
30
ortic
albi
c
C
ona
l
Lim
bEn
torh
in
Normal MCI Dementia

Increeasing seeverity oAmyloid plaques
of diseasNFTs
Amyloid plaquesse



4C 6 4
5
Case 1: 1996
3
5
73 yo ♂
More forgetful
No functional impairment 5
1
No functional impairment
Memory tests abnormal
Dx: MCI2
1
33
1
11
28

ortic
albi
c
C
ona
l
Lim
bEn
torh
in
Normal MCI Dementia

Increeasing seeverity o
MCI
of diseaseAmyloid plaques
eNFTs
Amyloid plaques

Cognitive ContinuumCognitive Continuum
NormalNormal
Mild CognitiveMild CognitiveImpairmentImpairmentpp
D tiD tiDementiaDementia

30 16
20
25
MiniMini 10
12
14
LogicalLogical
10
15
MiniMini--mental mental state state examexam 6
8
10LogicalLogicalmemorymemoryIIII
0
5
10
0
2
4
0NormalNormal MCIMCI ADAD
General cognitionGeneral cognition
0NormalNormal MCIMCI ADAD
MemoryMemory
Petersen RC et al: Arch Neurol 56:303‐308, 1999

MCI MCI AD 12%/yrAD 12%/yr Control Control AD 1AD 1--2%/yr2%/yr100100
80
90
80
90
60
70
60
70
5050Initial 12 24 36 48exam Months
Initial 12 24 36 48exam Months
Petersen RC et al: Arch Neurol 56:303Petersen RC et al: Arch Neurol 56:303--308, 1999308, 1999

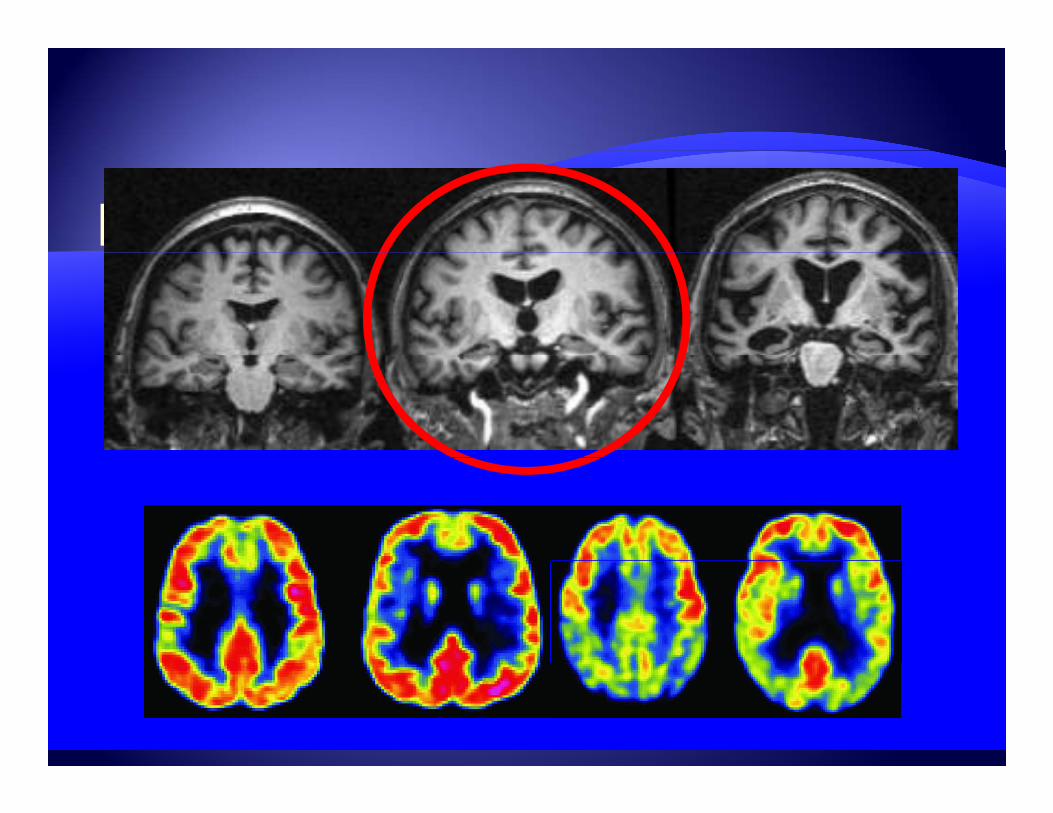
Neuro‐imaging with MRINeuro imaging with MRI
Jack CR. In Mild Cognitive Impairment. Ed. RC Petersen, Oxford University Press 2003
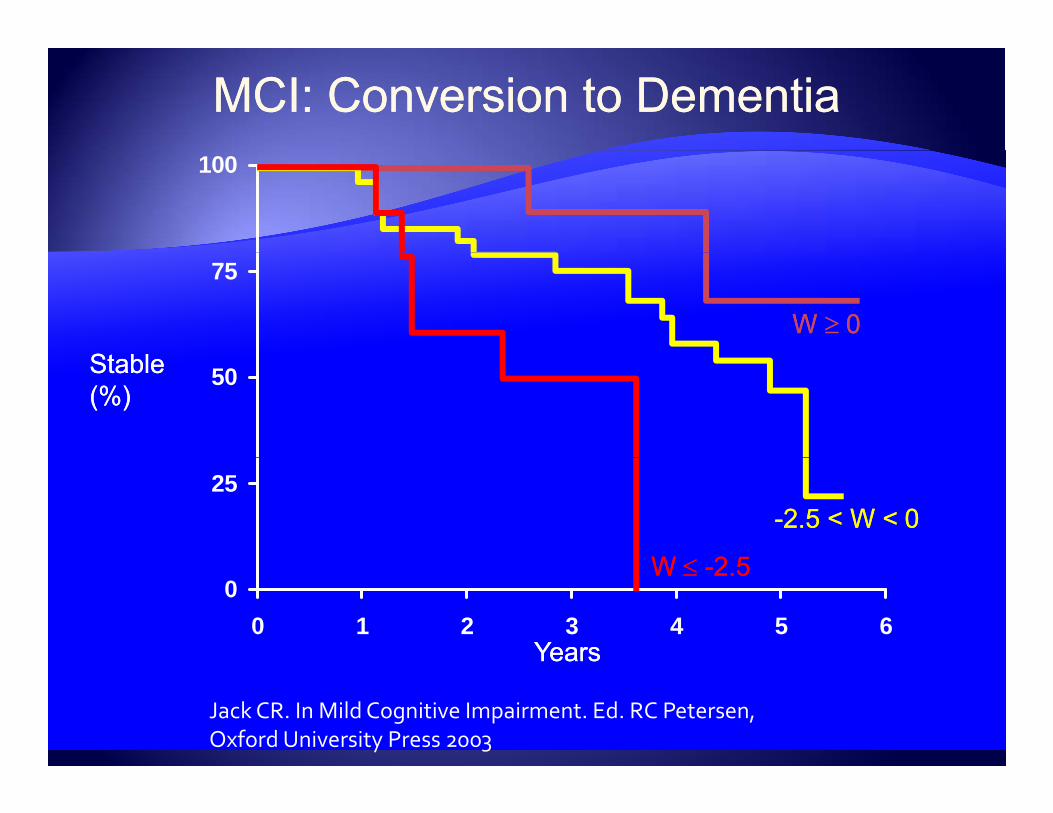
MCI: Conversion to DementiaMCI: Conversion to Dementia100
75
St blSt blW W 00
50StableStable(%)(%)
25--2.5 < W <2.5 < W < 00
WW 2 52 50
0 1 2 3 4 5 6YearsYears
W W --2.52.5
Jack CR. In Mild Cognitive Impairment. Ed. RC Petersen, Oxford University Press 2003

‐6Improve
0
6
Decline in ADAS‐Cog scorebased on the natural history of
12
18
based on the natural history ofuntreated patients with moderateAlzheimer’s disease* Decline
0 6 12
Cumulative Weeks From Baseline of the Double‐blind Study
9862 74 8526 38 5014
Rogers SL, Friedhoff, LT. Eur Neuropsychopharmacol. 1998;8:67‐75.*Stern RG, et al. Am J Psychiatry. 1994;151:390‐396.


1C 4
Case 1: 2000
3
5
77 yo ♂
Starting to have trouble with ADLs
Multiple cognitive domains abnormal 5
0
Multiple cognitive domains abnormal
Dx: Early AD
2
1
33
1
11
22

ortic
albi
c
C
ona
l
Lim
bEn
torh
in
Normal MCI Dementia

Increeasing seeverity oof diseaseAmyloid plaques
eNFTs
Amyloid plaques





*** p < 0.0001** p < 0.005
Holmes: Neurology, Volume 63(2).July 27, 2004.214‐219

0C 0
Case 1: 200481 yo ♂
Even basic ADLs affected
1
0
Even basic ADLs affected
Severely fragmented cognitive function
Prominent behavioral changes 0
0
Dx: Late stage AD
1
1
1
0
00
4

ortic
albi
c
C
ona
l
Lim
bEn
torh
in
Normal MCI Dementia

Increeasing seeverity oof diseaseAmyloid plaques
eNFTs
Amyloid plaques




Tariot PN. Farlow MR. Grossberg GT. Graham SM. McDonald S. Gergel I. Memantine Study Group. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA. 291(3):317‐24, 2004 Jan 21.

22
23
atio
n
260
265
atio
n Heart disease
18
19
20
21
22
per 1
00K
pop
ula
245
250
255
260
per 1
00K
pop
ula
AD
15
16
17
18
1999 2000 2001 2002 2003
Dea
th ra
tes
230
235
240
1999 2000 2001 2002 2003
Dea
th ra
tes
1999 2000 2001 2002 2003 1999 2000 2001 2002 2003
196
197
198
pula
tion
59
60
pula
tion
193
194
195
196
es p
er 1
00K
pop
55
56
57
58es
per
100
K p
op
Neoplasm CVD
190
191
192
1999 2000 2001 2002 2003
Dea
th ra
t
53
54
55
1999 2000 2001 2002 2003
Dea
th ra
tNeoplasm CVD

22
23
atio
n
260
265
atio
n Heart disease
18
19
20
21
22
per 1
00K
pop
ula
245
250
255
260
per 1
00K
pop
ula
AD
15
16
17
18
1999 2000 2001 2002 2003
Dea
th ra
tes
230
235
240
1999 2000 2001 2002 2003
Dea
th ra
tes
1999 2000 2001 2002 2003 1999 2000 2001 2002 2003
196
197
198
pula
tion
59
60
pula
tion
193
194
195
196
es p
er 1
00K
pop
55
56
57
58es
per
100
K p
op
Neoplasm CVD
190
191
192
1999 2000 2001 2002 2003
Dea
th ra
t
53
54
55
1999 2000 2001 2002 2003
Dea
th ra
tNeoplasm CVD

You can You can help us help us help us help us promote promote
l l normal, normal, healthy, healthy, brain brain
aging for aging for g gg gall!all!





























