Embed Size (px)
Citation preview

HEALTH PROMOTIONin
Health Disaster Management
Presented by: Yayi Suryo PrabandariDepartment of Health Behavior, Social Medicine &
Environment Health Graduate Program of Public Health @2017
Faculty of Medicine - Universitas of Gadjah MadaBased on chapter book “Health Promotion in Emergency Situation”
written by M. Agus P., & Yayi SP, Guest lecture at University of Groningen presented by Yayi

Topik hari ini
• Indonesia sebagai negara dengan toko serba ada bencana
• Promosi kesehatan – pengingatan kembali
• Konsekuensi kesehatan masyarakat dalam bencana
• Respon kesehatan masyarakat dalam bencana
• Peran promosi kesehatan dan profesi promosi kesehatan dalam penatalaksanaan bencana
• Contoh program promosi kesehatan untuk bencana di Indonesia

Indonesia tercinta : negara penuh
dengan Hazard bencana

Indonesian Archipelago
Indonesia terdiri : 33 propinsi, 349 kab and 91 kotamadya
Ring of fire sebaran gunung berapi di Indonesia
Kecuali Kalimantan, semua pulau berisiko terkena
gempa

Indonesia :
Ring of Fire

Indonesia: earthquake islands

Indonesia – toko serba ada bencana
Bencana yang mungkin terjadi di Indonesia
Natural disaster Man made disaster Lainnya
Gempa bumi Konflik KLB
Erupsi gunung berapi Terorism Kekeringan
Banjir Polusi lingkungan
Longsor Kecelakaan industri
Badai Kecelakaan transportasi
Angin topan dan putingbeliung
Tsunami

Promosi Kesehatan
Pengingatan

The Fundamental Conditions and
Resources for Health
Peace, shelter, education, food, income, a stable eco-system, sustainable resources, social justice and equity.
(prerequisite of health):
Improvement in health requires a secure foundation in these basic prerequisites

Promosi Kesehatan
• WHO menyebutkan bahwa promosi kesehatan merupakan proses untuk mendorong orang meningkatkan kontrol dan mengembangkan kesehatannya.

Promosi Kesehatan =Pendidikan kesehatan +
kebijakan
Promosi kesehatan adalah proses advokasi kesehatan yang dilaksanakan untuk meningkatkan kemungkinan:
– personal (individu, keluarga & masyarakat),
– swasta (profesional dan bisnis) serta
– pemerintah (nasional, propinsi, lokal)
untuk mendukung praktek kesehatan positif menjadi norma sosial.
Sehat, kualitas hidup, sejahtera
secara menyeluruh
TUJUAN
PROMOSI
KESEHATAN

Promosi Kesehatan
Sebelum 2016
• A = advokasi
• B = bina suasana
• G = gerakan pemberdayaan masyarakat
Pasca Shanghai
Declaration (2016) & SDG
3 Pilar Promosi Kesehatan
• Health literacy
• Good governance
• Healthy in all setting

Promosi kesehatanPerubahan yg direncanakan untuk
kesehatan yang berhubungan dengan
gaya hidup dan kondisi fisik melalui
perubahan individu dan lingkunganTingkat
populasi
Kondisi
kehidupan
Lingkungan fisik
dan psikososial
Aksi politik
Organiasi
masyarakat
Pengem-
bangan
masyarakatPeningkatan kesehatan individ dan
kesejahteraan:
Menjadi individu, keluarga,
sekolah, tempat kerja, pelayanan
kesehatan & masyarakat
Tingkat
Individual
Perilaku
Pilihan
Gaya hidup
Pendidikan
kesehatan
Pemasaran sosial
Komunikasi
INTERAKSI
PROMOSI
KESEHATAN*
*Adapted from O’Neill & Stirling, 2007, cit. Fertman & Aleensworth, 2010

Health Promotion Cycle
Community Analysis
Targeted assessment
Evaluation Program Plan Development
Implementation

Perjalanan Promosi kesehatan
Ottawa Chatter for HP (WHO, 1986)
• Develop healthy public policy
• Develop personal skills
• Strengthen community action
• Create supportive environments
• Reorient health service
Jakarta Declaration on leading HP (WHO,
1997)
• Promote social responsibility of health
• Increase investment for health developments in all sectors
• Consolidate and expand partnerships for health
• Increase community capacity and empower individuals
• Secure an infrastructure for health promotion
Bangkok Declaration 2005
• Promote social responsibility for health
• Increase investment for health development
• Consolidate and expand partnerships for health
• Increase community capacity and empower the individual health promotion I carried out by and with people
• Secure an infrastructure for health to secure an infrastructure for health promotion, new mechanisms of funding it locally, nationally and globally must be found

Nairobi Declaration 2009
• S t r e n g t h e n l e a d e r s h i p a n d
w o r k f o r c e s
• M a i n s t r e a m h e a l t h p r o m o t i o n
• E m p o w e r c o m m u n i t i e s a n d
i n d i v i d u a l s
• E n h a n c e p a r t i c i p a t o r y p r o c e s s e s
• B u i l d a n d a p p l y k n o w l e d g e

Helsinki Statement - 2013We, the participants of this conference
• Prioritize health and equity as a core responsibility of governments to its peoples.
• Affirm the compelling and urgent need for effective policy coherence for health and well-being.
• Recognize that this will require political will, courage and strategic foresight.

Helsinki Statement - 2013
We call on governments
to fulfil their obligations to their peoples’ health and well-being by taking the following actions:
• Commit to health and health equity as a political priority by adopting the principles of Health in All Policies and taking action on the social determinants of health.
• Ensure effective structures, processes and resources that enable implementation of the Health in All Policies approach across governments at all levels and between governments.
• Strengthen the capacity of Ministries of Health to engage other sectors of government through leadership, partnership, advocacy and mediation to achieve improved health outcomes.
• Build institutional capacity and skills that enable the implementation of Health in All Policies and provide evidence on the determinants of health and inequity and on effective responses.
• Adopt transparent audit and accountability mechanisms for health and equity impacts that build trust across government and between governments and their people.
• Establish conflict of interest measures that include effective safeguards to protect policies from distortion by commercial and vested interests and influence.
• Include communities, social movements and civil society in the development, implementation and monitoring of Health in All Policies, building health literacy in the population.

Shanghai Declaration 2016
• We recognize that health and wellbeing are essential to achieving sustainable development
• We will promote health through action on all the SDGs
• We will make bold political choices for health
• Good governance is crucial for health
• Cities and communities are critical settings for health
• Health literacy empowers and drives equity
•

Kerangka untuk PromosiKesehatan (Keleher, MacDougall & Murphy, 2007)
Prevensi
penyakit
Strategi
Komunikasi
Edukasi
kesehatan dan
pemberdayaan
Pengembangan
kesehatan dan
komunitas
Perubahan
infrastruktur
dan sistem
Primer
Sekunder
Tersier
Informasi
kesehatan
Kampanye
perubahan
perilaku
Pengetahuan
Pemahaman
Pengembangan
keterampilan
Keterlibatan
Pengembangan
komunitas
Kebijakan
Legislasi
Perubahan
organisasi
Lini bawah Lini atas
INTERVENSI
Pelayanan
primerPendekatan gaya hidup dan
perilaku
Pendekatan ekologis

Konsekuensi kesehatanmasyarakat
dalam bencana

Apa yang terjadi dalam bencana?
• 1. Kehilangan nyawa, luka-luka
• 2. Kerusakan berat pada infrastruktur
• 3. Adanya penyintas dan cerai berainya keluarga
• 4. Kesulitan ekonomi
• 5. Masa berkabung dan kemarahan yang intens

Kehilangan nyawa dan luka-luka• Kebutuhan kesehatan dan sosial yang segera
• Trauma psikologis
• Luka atau cidera yang tidak mendapatkan pengobatan yang adekuat
• Nutrisi yang tidak optimal dan seimbang mengandalkan pada bantuan
• Kehilangan nyawa akibat cidera
• Kecacatan permanen

Kerusakan infrastruktur
• Tidak hanya fasilitas kesehatan yang rusak, namun infrastruktur yang lain (sanitasi, air minum dsb)
• Pelayanan untuk keluarga juga terkena jasa penitipan anak dsb
• Risiko adanya epidemik
• Akses terbatas pada populasi yang terkena bencana (rusaknya jalan – keamanan)

Penyintas• Habitat baru
• Ketegangan atau hambatan untuk mendapatkan hak sipil ataupun fasilitas yang diperlukan sebagai anggota masyarakat
• Pasien penyakit kronis akan rentan
• Orang tua dan anak-anak (terutama balita) kurang mendapatkan nutrisi yang tepat dan seimbang
• Perasaan tidak aman
• Kehilangan harga diri
• Pengungsian

Masa yang berat utk Ekonomi
• Kehilangan kesempatan untuk berwirausaha
• Pelepasan terhadap bantuan
• Peningkatan ketergantungan
• Rentan terhadap penyakit dan sakit
• Dapat tergiring ke arah perlaku anti sosial dan kejadian

Masa berkabung dan kemarahan
• Rentan secara psikologis dan emosional
• Dapat menghasilkan perilaku aneh
• Muncul ketidakpuasan/ketidak senangan dengan pemerintah atau organisasi pemberi bantuan lainnya
• Sebagian mendapatkan informasi yang tidak benar dari media massa

Peran promosi kesehatan dan profesional promkes dalam
bencana

What happened in this situation?

Rehabilitation
Preparednessss Response
Event
Impact &
Damage
Mitigation
LESSON
LEARNED
Health
Promotion?
Where?

Phase of Emergency Situation (Oxfam, 2005)
• High risk situation
• Medium risk
• Health maintenance

Nine Contextual Determinant of Health Population in Emergency Situation
• Geography
• Political structure and governance
• Community socioeconomic status
• Distribution relative of income and wealth
• Culture
• Health and social infrastructure
• Physical environment
• Social environment
• Civil Society

Where is the place of health promotion in emergency situation?

IDP (internally displacement
person/penyintas) health issues
Surveillance
Mental Health
Hospital, Medical
Services, Rehabilitation
Child, Maternal,
Reproductive
Immunization
Information and Supply Management
Health
Promotion
Water Sanitation
Food & Nutrition
Communicable Disease

Stages after events up to
disaster
Hazard
Risk
Impact
Damage
Disaster
Event
PreventionModification
Absorb
capacity
Buffering
capacity
Vulnerability
Response
ResilianceBuffering
capacity

Health Promotion
Cycle
Community Analysis
Targeted assessment
Evaluation Program Plan Development
Implementation
Disaster Phases:
•Preparedness
•Response
•Mitigation
•Recovery
• Rehabilitation

Health promotion cycle and
disaster phases
Risk & Emergency
Preparedness
Event
Assessment
& Analysis
Planning &
Objective SetImplementationMonitoring
Evaluation
&
Impact
measuremen
t

Sayangnya terkadang bencana tidak mengikuti alur linier
• Rehabilitation
• Recovery
• Adaptation
• Acute phase
• Emergency / disaster

Pentingnya Promkes dlm Bencana• Menekankan dampak kesehatan masyarakat
• Dalam konteks pengelolaan kedaruratan atau bencana, Promkes melibatkan diri melalui bekerja dengan masyarakat untuk mencegah, mempersiapkan dan respon terhadap bencana untuk mengurangi risiko, meningkatkan resiliens dan mitigasi dampak bencana terhadap kesehatan
• Pemberdayaan masyarakat merupakan dasar dalam situasi tersebut

Pentingnya Partisipasi Masyarakat dalam bencana
Persiapan kedaruratan:
• Partisipasi dalam mengukur risikodan kerentanan
• Meningkatkan kesadaran akan tandalingkungan (hazard) dan keamanan
• Memperkuat organisasi danpenerimaan masyarakat
• Peningkatan kesadaran danpelatihan adalah hal yang utama
Respon dan pemulihanterhadap kedaruratan
• Partisipasi dalam faserespon
• Menekankan padajaminan peningkatan dankeberlangsungankesehatan lingkunan

Persiapan(Preparedness)
Respon (Response) Pemulihan (Recovery)
Mengorganisasikanmasyarakat agar merekasadar sehat dan keamanan
Memberikan informasi “how to” (bagaimana caranya) danmempromosikan kesadaran
Secara bertahapmengintegrasikan aksi untukkondisi yang stabil
Mendefinisikan populasiberisiko dan tingkatrisikonya
Menekankan pada konsekuensikondisi dan memberikanrekomendasi tindakan
Melakukan assessment padapopulasi yang membutuhkanpelayanan jangka panjang
Merancang informasi risikodidasarkan karakteristikindividu
Menyesuaikan aktivitas promosikesehatan sesuai dengankeadaan dan kelangkaan
Menekankan bahwamembangun kembali proses adalah “fokus sehat’
Membantu masyarakatuntuk mengembangkanpersepsi risiko
Kebutuhan untuk menyelesaikanmasalah psikososial dalamsituasi tersebut
Menggunakan pesandidasarkan masalah ataupraktek dalam masapemulihan
Adaptasi metode untukkebutuhan yang aktual danpotensial
Identifikasi pesan dan metodekomunikasi yang spesifik padasituasi tersebut
Dukungan rehabilitasipsikologis jangka panjang
Mempromosikan praktekhidup sehat dalampengembangan komunitas
Memberikan panduan danpelatihan dalam aksi
Fokus pada persiapan danpencegahan bencana

Pertanyaan pada mitigasi• Manakah praktek atau tindakan yang menempatkan risiko
untuk kesehatan?
• Manakah kelompok masyarakat yang paling rentan?
• Apa yang harus dilakukan agar masyarakat mengadopsi praktek/tindakan yang aman?
• Siapa yang akan menjadi sasaran program?
• Bagaimana caranya berkomunikasi dengan mereka?

Koordinasi: sulitkah?• Duplikasi atau menyia-siakan sumber yang langka
• Terkadang masyarakat tidak diassess : kebutuhannya berdasarkan kebutuhan mereka sendiri, dan bukan kebutuhan yang nyata
• Tidak ada informasi yang non sintesis
• Agenda instansi donor?
• Bagaimana dengan partai politik yg memanfaatkan kejadian bencana?
• Pemerintah menggantungkan pada organisasi yang membantu dalam bencana

Peran profesi promkes• Mengelola data dan informasi untuk keefektifan
program promkes
• Hygiene dan sanitasi (air, perumahan dan sanitasi)
• Promosi kesehatan mental
• Imunisasi (KIA)
• Prevensi epidemik
• Merawat pasien penyakit kronis
• Menghitung kecenderungan

LAMPIRAN:
Contoh Promkes dalam Bencana

Health Promotion Program at
Nias Island – 6 months after
Earthquake
NiasCoordinates: 1°6′N 97°32′E1.1°N 97.533°E
Area: 4,771 km2 (1,842 sq mi)
Highest point: unnamed (800 m (2,600 ft))
Province: North Sumatra
Regencies: Nias, South Nias
Population: 639,675
Density: 134.08 /km2 (347.3 /sq mi)
Ethnic groups: Malay, Batak, and Chinese

People in Nias
• The theory of cultural dissemination states Nias's ancestors came from Yunan, in the south of China, about 3.500 years ago.
• Material culture -- such as sword hilts and coffins -- and their traditional architecture, which is dominated by dragon-head motifs.
• Nias Island represents the glory of the megalithic age from Indonesia's perspective. • Areas in Nias Island are dominated by large stones portraying their cultural
civilization which take the form of menhirs, dolmens, stone coffins, monuments, statues from the megalithic age and house ladders.
• Rituals and traditions involving stones have been passed down from generation to generation as well as working in a group
• Stone is symbolizes the religious, social, eternal, devotional and conceptual values within the Nias people.

Nias Island after Earthquake
· A great earthquake was noted at 23:09:36 hrs, local time at epicenter, on Monday, March 28, 2005.The magnitude was 8.7 on the Richter scale and located in NORTHERN SUMATRA, INDONESIA.The epicenter was located 90 km south of Sinabang with 30 Km Depth 2.065 N 97.010 E

After earthquake
Government officials update figures:
• Deaths tolls at 532, with 422 in the Nias District, and 113 from South Nias.
• 1125 seriously injured persons and 928 minor injury cases.
• The number of temporary displaced has been put at 19,016 while the number of permanently displaced has been put at 35,235 (houses destroyed)

Community Analysis*
Targeted assessment
Evaluation Program Plan Development
Implementation
50
*conducted by UGM and Nias district health office officers
** based on the conceptual framework by Dignan & Carr

Need Assessment Result• Several diseases were found at Gunung Sitoli
community:– ARI (Acute Respiratory Infection)
– Skin diseases
– Musculoskeletal diseases
– Dyspepsia
– Hypertention
– Malaria
– Diarrhoea.
The children had higher risk for the diseases.
The people’ hygiene practice was poor.
They never washed their hand after defecating.

Need Assessment Result
• Several health promotion programs have been done by UNICEF and Indonesian Health Office since the disaster. An (NGO) has made printed media health messages i.e. poster and banner.
• The basic problem was water supply.
• Vector borne diseases were a serious problem
after the earthquake

Aim
• To facilitate sufficient and feasible health information and education for people in the disaster area
• To overcome the health problem, particularly hygiene and sanitation, mother and child health, and infectious disease prevention.

Activities
• Capacity building for sustaining the health promotion delivery (through training for trainers)
• Advocacy to the local authority (to assess the continuity of the program)
• Developing health education media
• Distribution and delivering mass media (printed and electronic media)
• Traditional performance art (for implementing mass health promotion)

Expected outcome
• The increasing knowledge and attitude toward healthy environment, including hygiene and sanitation, infectious disease prevention, as well as mother and child health care after the health promotion activities
• The change of health behavior practice of Nias people after disaster.

Training
• Development training module
• Training for trainer
• Training for health promotion officer

Media Development
The health promotion poster : before (left) and after pre
testing (right)
Poster
Flip Chart
Pre test of media

Advocacy
Head of Nias Health Office
Head of Nias Development planning board (Bappeda)
Head of communicable disease division (Seksi P2M)
Head of Gunung Sitoli Sub Distric
Head of Ilir Village
Head of Pasar Gunung Sitoli Village

Traditional Performance Art
Maena Dance Competition

Banner
Distribution of Message

Health education delivery• Place:
– Integrated health post (Posyandu)– Community houses– Religious places– Village meeting halls
• Topics:– Environmental health– Maternal and child health
• Sources– Community leader– Spiritual leader
• Media: – Radio– Poster

The result after the implementation
(evaluation phase)• An increasing practicing in using toilet among women, other than man
(other places to defecate sea shore, pig pen), as well as using water for cleaning (other than leaves & coconut peels)
• Women give more attention on healthy behavior practices of their children other than men
• Women showed an increasing knowledge toward healthy behavior after the program, but men demonstrated an increasing attitude toward healthy behavior

Lesson learnt• Involving local people (DHO and health cadres/lay person) on
health program plays as an important factor in facilitating health program in Nias
• The use of traditional culture (Maena dance) as a health promotion media can be seen as an alternative to deliver health message
• Involving men in family health is challenging need to explore in where and when men can be involved in the family health responsibility (without breaking the culture and norm)
• Nias District Health Office should conduct follow up of the existing program by guiding cadres and midwifes and always empower community and spiritual leaders to elevate the community health status (particularly there were few NGOs still working in the areas and BRR/Rehabilitation & Reconstruction Body of Aceh and Nias is the coordinator)

Promoting Community Health
through Capacity BuildingRehabilitation and Health System Improvement in
Eastern and Central District of Nanggroe Aceh
Darussalam Province
ACEH:
Area : 57,365.57 km2 (22,149 sq mi)
Population : 3,930,000 (2000)
Density : 68.5 /km2 (177 /sq mi)
Ethnic groups : Acehnese (50%), Javanese (16%), Gayo Lut (7%), Gayo Luwes (5%), Alas (4%), Singkil (3%), Simeulu (2%)
Religion: Islam (98.6%), Christianity (0.7%), Hinduism (0.08%), Buddhism (0.55%)
Languages: Indonesian (official), Acehnese

Maternal and infant mortalityMalnutrition
Transmitted disease malaria, DHF, ARI
Chronic diseases cardiovascular, stroke Community
Behavior Smoking habitNon compliance of using helmet
Health promotion program NOT OPTIMAL
CAPACITY BUILDING OF HEALTH PROMOTER
IMPLEMENTATION OF DESA SIAGA/Alert village

•Building capacity of health promoter and community regarding health promotion strategy and technqiue through training from the level of
– District
– Primary Health Care,
– Village (Poskesdes)
in 10 districts in NAD.

•Training for health promotion officers in district health office and Primary Health Care
•Training of health promotion for Midwifes and cadres
•Supervising the implementation of health promotion in village level
•Evaluating the health promotion implementation

PROGRAM EXECUTION
Internal – External Environmental
Assessment(Underpining & Understanding Environment)
HP training for DHO
and Puskesmas officer
Implementation Health Promotion at
Village and sub village level
PROGRAM PLANNING
(Goal, Criteria, Activities)
Advocacy to policy
maker at district level
Formative
Evaluation
Summative Evaluation
N
e
x
t
S
t
a
g
e
HP training for Midwife
and cadre
Support
and
Supervise
Reinforcement
Problem Based
Discussion
Reinforcement
Community
Action plan
Conceptual Framework*
*Based on the
IDM concept

• Finalizing the plan and need assessment (Health Promotion need assessment and training need assessment-collaboration between UGM and PHO & DHO).
• Program implementation that consist of first stage training (district health officer and Primary health care officer) and second stage (midwife and cadre).
• An independent activity by cadre, midwife, Primary Health Care oficer and district health officer with supervision from UGM
• Evaluation

1 IntroductionAll about project descriptionThe descriptions of health promotion program situation
2 The roles of health promoter and community empowerment.
3 Need assessment
4 Advocacy : one strategy to influence public policy
5 Presentation technique
6 Basic concept of targeted assessment in health promotion needassessment
7 Health promotion program plan.
8 Health promotion program Implementation
9 Health promotion program evaluation Basic concept of health promotion program evaluation Health promotion program measurement.
10 Follow-up plan
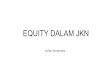
PHO AND DHO TRAINING

1 Introduction
2 Advocating : Strategy
3 Advocating : communication
4 Lobbying and Negotiation
5 Presentation Technique
6 Public Speaking
7 Effective meeting
8 Development of Traditional media to health promotion and creativity
9 Community empowerment
0
2
4
6
8
10
pre test 2.7 2.775 2.35 3.65 3.15 2.95 3.59 4.8
postest 6.185 6.46375 5.5175 6.4825 5.43 5.23 6.73 7.8
Pertemuan
Efektif
Public
SpeakKreativitas Presentasi
Pemberday
aanKomunikasi Lobi Nego
Strat
advokasi

No Village District Health Promotion Programs
1 Rantau Panjang East Aceh Posyandu (integrated health post) Revitalization
2 Oulee Blang East Aceh Elderly integrated health post (posyandu lansia)
3 Bies Penantan Central Aceh Posyandu Lansia dan malnutrition
4 Desa Tebuk Central Aceh Family healthy behavior
5 Marlempang Aceh Tamiang a.Smoking cessationb.Tabulin (Tabungan Ibu Bersalin) (pregnantmother saving)
6 Banai Aceh Tamiang Collective periodically toilet
7 Mupakat Jadi Bener Meriah a.Pregnant mother savingb.Health fundsc.Village ambulance
8 Blanpulo Bener Meriah a.Health fundsb.Village ambulance
9 Salang alas South-East Aceh School health promotion
10 Terutung Pedi South-East Aceh Garbage management
Health Promotion Program Carried out by Midwifes and Health Cadres, supervised by PHO, DHO & UGM

Health promotion delivery
• Place:– Integrated health
post/Posyandu
– Group praying
– Home visit
• Resources:– Midwifes
– Health cadres

The result after the implementation (evaluation phase)
• There was an elevating of knowledge among men and women in the intervention areas
• The practicing of eating healthy food, smoking behavior and helmet wearing were better in the intervention areas compared to the control areas

Lesson learnt
• Districts in Aceh have different characteristics (different DHO & health cadres impact on the results
• Implementing training is challenging due to the several numbers of training carried out by NGOs
• Years in conflict impact on Aceh people to obtain new things
• Community partisipation can be done through intense approach (but still challenging)

Assist Integrated Community Partisipation on Health Program After Earthquake in
Jogjakarta
Area : 185.80 km2 (1,230 sq mi)
Population : 3,121,000 (2003)
Density : 979.7 /km2 (2,537 /sq mi)
Ethnic groups : Javanese (97%), Sundanese (1%)
Religion: Islam (91.8%), Christianity (7.9%), Hinduism (0.2%), Buddhism (0.1%)
Languages: Indonesian (official), Javanese

Assessment (health, etc)
• Carried out by several NGO’s, universities finally coordinate by the PHO of Yogyakarta offices (health) & National Coordination of Emergency
• Cases (health)
– Fracture
– Tetanus (Infection generally occurs through wound contamination and often involves a cut or deep puncture wound)
– ARI

Phase of Emergency Situation (Oxfam, 2005)
• High risk situation – Emergency response
• Medium risk– Assisting existing Primary
health care & temporary clinics
• Health maintenance– Coordinating integrated
health post (local community, NGO, universities & academies)

The different of refugee camps in Aceh & Jogjakarta
• Aceh • Jogjakarta

Lesson learnt- Learning about people in the disaster area plays important role
in the humanitarian action (Aceh = Nias = Jogjakarta)- Aceh disaster after this disaster, Indonesian gov, NGO has
experience on how to coordinate the humanitarian action and its impact to the surrounding community
- Nias disaster has learned from Aceh emergency response- Jogja disaster:
- although the government not “really ready” to that situation, the coordination was better that Aceh case (has had experience)
- The government of Jogjakarta province allow the NGO to work in the disaster area in the maximum of 6 months time

ACKNOWLEDMENT•NOHA• WHO• Gitec
•Health Providers, Cadres, Community and Spiritual leaders in Nias, Aceh &
Jogjakarta Provinces•Nias District Health Office
•North Sumatra, Aceh & Jogja Provincial Health Office
Thanking for your attention