Embed Size (px)
Citation preview

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 1/48
Amala
Nisanthi
Kavitha
Afiqah
Shuhaila

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 2/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 3/48
Is a disorder in which the red blood cells aredestroyed faster than the bone marrow can producethem
The term for destruction of red blood cells is hemolysis Iron and other by ²products remain in plasma.Lysis
within circulatory system or due to phargocytosis bycells of retiloendothetial system
Hematopoietic activities of bone marrow increase
8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 4/48
There are 2 types of hemolytic anemiaincluding the following:
*Intrinsic-the destruction of the RBC due toa defect within the RBC themselves
Intrinsic hemolytic anemia's are ofteninherited, such as sickle cell anemia and
thalassemia
These conditions produce RBC that do notlive as long as normal RBC

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 5/48
Extrintic- RBC are produced healthy but
are later destroyed by becoming
trapped in the spleen,destroyed byinfection

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 6/48
Abnormal paleness or lack of color of thespleen
Jaundice Dark color of urine Fever Weakness Dizziness Confusion Enlargement of the spleen and liver tachycardia

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 7/48
Blood test
Medical history
Physical e xamination

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 8/48
o Change in diet
o Medication
o Splenectomy-surgery to remove thespleen
8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 9/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 10/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 11/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 12/48
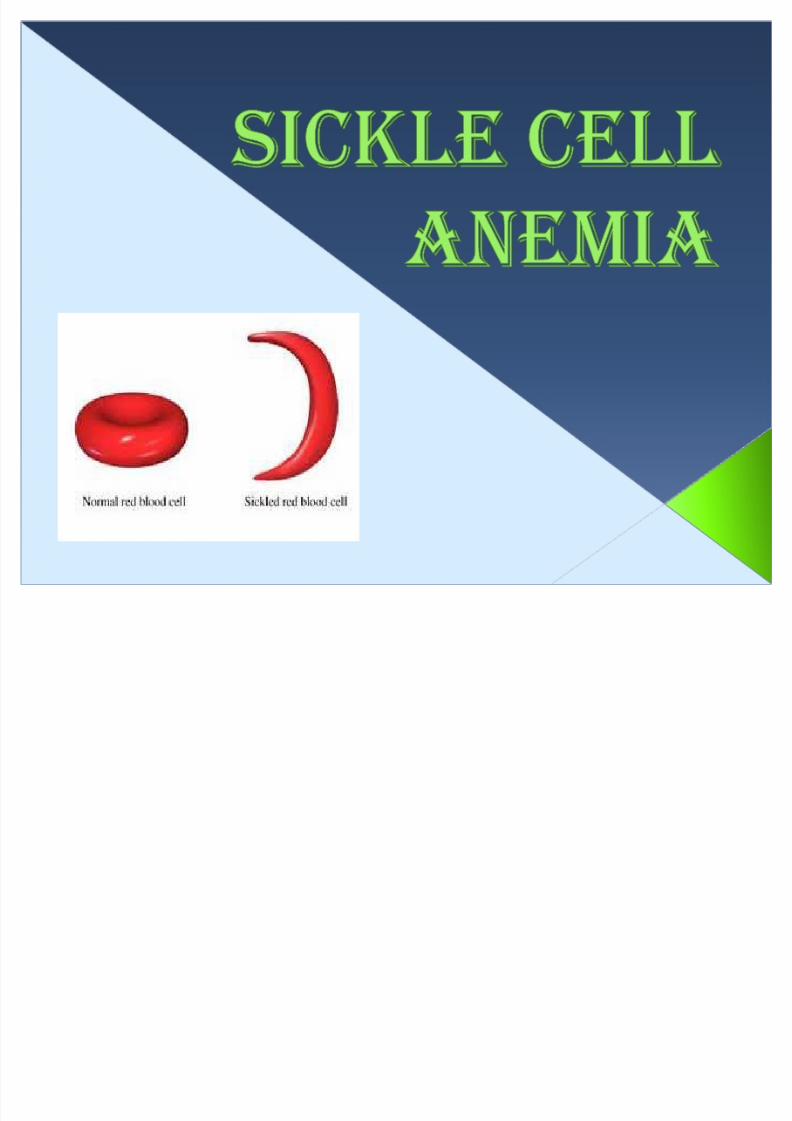
Hemoglobin is a protein inside red blood cellthat carries o xygen
Abnormal hemoglobin call hemoglobin S
Distorts the shape of red blood cells especiallywhen e xposed to low o xygen levels
Sickle cell deliver less o xygen to the body tissue
Clog more easily in small blood vessel, break into pieces that disrupt healthy blood flow
Inherited from both parents

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 13/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 14/48
Bone pain
Breathlessness
Fatigue Rapid heart rate
Ulcer on the lower leg(adult)
Yellowing of the eyes and skin(jaundice) Excessive thirst
Poor eye sight/blindness
Stroke

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 15/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 16/48
� Infection and gangrene
� Hypovolemic shock and death due tomassive entrapment of cells
� Necrosis
� Cerebral vessel occlusion due to organinfraction

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 17/48
CBC ²Complete Blood Count
Sickle Cell Test

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 18/48
Folic acid (essential for producing RBC),RBCare turned over so quickly
Narcotic ² To treat the pain(but some
people will large doses of narcotics) Kidney transplant for kidney
disease(Dialysis) Antibiotic and vaccine-prevent bacterial
infection(children with sickle cell) Large amount of [email protected]. fluids to correct
hypovolemia and prevent dehydrationvessel occlusion

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 19/48
� Acute pain related occlusion of small
vessel by sickle cells

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 20/48
� Assess pain types, location and intensity
R:Other vessel to the brain ,heart , lungs, spleen and penis becomeoccluded , causing pain
� Support joints and lower e xtremities withpillows
R:Relieve the joints pain
� Administer analgesic as ordered by doctor R: Relief from pain
� Document patient progress in nursing report R: Document pain levels

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 21/48
� Ineffectiveness Tissue Perfusion related to
a decreased number of RBCs
8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 22/48
� Monitor vital sign and mental alertness R:As a baseline and monitor abnormality
� Encourage to drink 8 to 10 glasses of water daily
R: Dehydration causes RBCs to sickle cells
� Monitor for symptom of obstructed vesselssuch as leg ulcerations, and dyspnea
R: RBCs are sickling, vessels supplying blood to other organ canbecome obstucted
� Document patient progress in nursing report R: Document the abnormal of condition such as breathing pattern

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 23/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 24/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 25/48
� the molecular abnormalities that led to
the thalassemic syndromes, it still is not
known how accumulation of e xcessunmatched alpha-globin in beta
thalassemia.
� O xidant injury may cause hemolysis, butthere is no evidence that it causes
ineffective erythropoiesis

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 26/48
� Hemoglobin E/beta thalassemia is now aworldwide clinical problem. The reasons
underlying the heterogeneity andoccasional severity of the syndromeremain obscure.
� Ineffective erythropoiesis now appears
to be caused by accelerated apoptosis,in turn caused primarily by deposition ofalpha-globin chains in erythroidprecursors.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 27/48
�
Heredity disorders ofhemoglobin-chain
synthesis.
8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 28/48
1. ALPHA THALASSEMIA2. BETA THALASSEMIA

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 29/48
1. ALPHA THALASSEMIA� occurs when a gene or genes related to the
alpha globin protein are missing or changed(mutated).
� occur most commonly in persons fromsoutheast Asia, the Middle East, China, and inthose of African descent.
2. BETA THALASSEMIA� occurs when similar gene defects affect
production of the beta globin protein.
� occur in persons of Mediterranean origin, andto a lesser extent, Chinese, other Asians, andAfrican Americans.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 30/48
� There are many forms of thalassemia.
Each type has many different subtypes.Both alpha and beta thalassemia
include the following two forms:
1. THALASSEMIA MINOR
2. THALASSEMIA MAJOR

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 31/48
1. THALASSEMIA MINOR� Less severe
� Receive the defective gene from only oneparent.
�
Blood smear are small(microcytic),pale(hypochromic), variouslyshape(poikilocytosis) RBC.
� Carry less o xygen.
�
Persons with this form of the disorder arecarriers of the disease and usually do nothave symptoms.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 32/48
1. THALASSEMIA MAJOR
� Severe
� Inherit the defective gene from both
parents� O xygen depletion in the body becomes
apparent within the first 6 months of life.
� Left untreated, death usually results when a
few years.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 33/48
� Still birth(death of the unborn baby duringbirth or the late stages of pregnancy).
� Children born with thalassemia major
(Cooley's anemia) are normal at birth, butdevelop severe anemia during the first yearof life.
� Bone deformities in the face�
Fatigue� Growth failure� Shortness of breath� Yellow skin (jaundice)

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 34/48
� CBC
� Iron level and total iron-binding capacity
� Serum ferritin
� Sickle cell test
� Bone marrow e xamination
� Quantitive essay of g6pd
8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 35/48
� Assess the patient at risk for falls using a
fall risk assessment tool
� Assist the patient to change positions� Assist the patient with ambulation
� Always raise the cord side bed to
preventpatient falling down.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 36/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 37/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 38/48
� Glucose-6-phosphate dehydrogenase
deficiency is an X-linked recessive
hereditary disease characterised byabnormally low levels of glucose-6-
phosphate dehydrogenase.
� Glucose-6-phosphate dehydrogenase
deficiency is a genetic disorder thatoccurs most often in males.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 39/48
� G6PD deficiency reduces energy
available to maintain the integrity of the
red cell membrane, which shortens RBCsurvival.
� Hemolysis selectively affects older RBCs
among affected blacks and amongmost affected whites.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 40/48
� Hemolysis occurs commonly after fever,
acute viral and bacterial infections, and
diabetic acidosis. Less commonly,hemolysis occurs after e xposure to drugs
or to other substances that produce
pero xide and cause o xidation of Hb and
RBC membranes.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 41/48
�
Inherited disorders, sex-linked, RBC metabolic
disorder

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 42/48
� Father is UNAFFECTED, mother is UNAFFECTED.ALL of their children will be UNAFFECTED.
� Father is G6PD DEFICIENT, mother is UNAFFECTED.
All sons will be UNAFFECTED.All daughters will be PARTIALLY DEFICIENT.
� Father is G6PD DEFICIENT, mother is PARTIALLYDEFICIENT.Out of two sons, one will be G6PD DEFICIENT and the
other will be UNA
FFE
CTE
D.Out of two daughters, one will be PARTIALLYDEFICIENT and the other will be G6PD DEFICIENT.

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 43/48

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 44/48
� Paleness (in darker-skinned childrenpaleness is sometimes best seen in themouth, especially on the lips or tongue)
� Extreme tiredness
� Rapid heartbeat
� Rapid breathing or shortness breath
� Jaundice or yellowing of the skin and eyesparticularly in newborns and enlargedspleen
� Dark, tea-colored urine

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 45/48
� CBC
� Iron level and total iron-binding capacity
� Quantitive essay of G6PD

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 46/48
� Rest in bed
� Assess the patients general condition
� Adminiser o xygen as prescribed
� Refer abnormal investigation results
� Give medication as ordered by doctor

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 47/48
� Consult a dietition
� Administer supplements as ordered
� Administer liquid supplements with a drinkingstraw to avoid staining the teeth
� Administer intramuscular iron injection by theZ-track method to avoid staining the injectionsite

8/6/2019 Hemolytic Anemia(Presentation 1) (2)
http://slidepdf.com/reader/full/hemolytic-anemiapresentation-1-2 48/48