Embed Size (px)
Citation preview
Högt Hb hos vuxna och barn – utredning och klinik
Jan Samuelsson Vetenskaplig sekreterare
Conflict of interest statement • ”I have a bagful of interesting conflicts,
and I would prefer to keep them to myself” (R Horton, chief editor Lancet 2003)
• Konsultuppdrag åt Swedish Orphan och Roche
• Advisory board Shire Pharmaceuticals
Polyglobulier hos barn/ungdomar
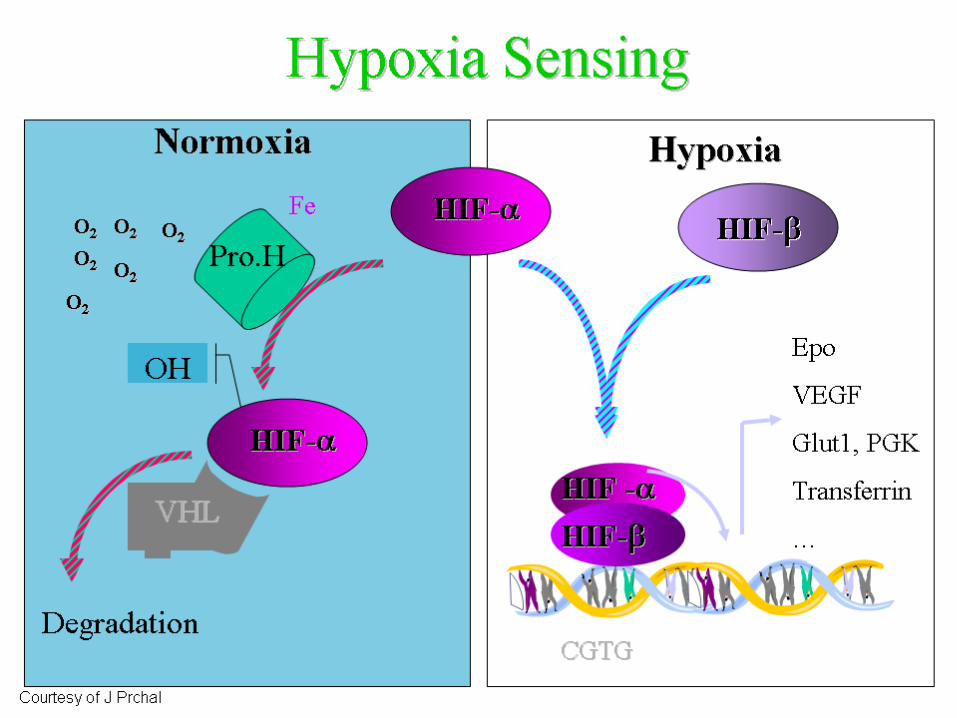
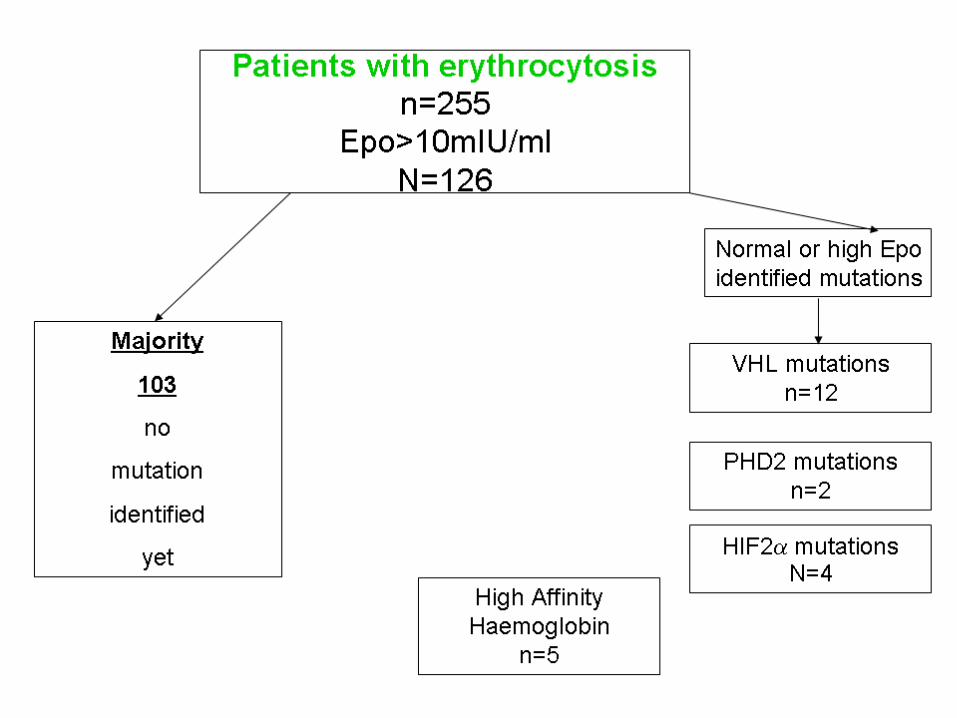
• Medfödda – EPO receptormutation – VHL, Chuvash – HIF-2α mutation – Högaffinitetshemoglobin – Gravt hjärtfel
• Förvärvade – Polycytemia vera
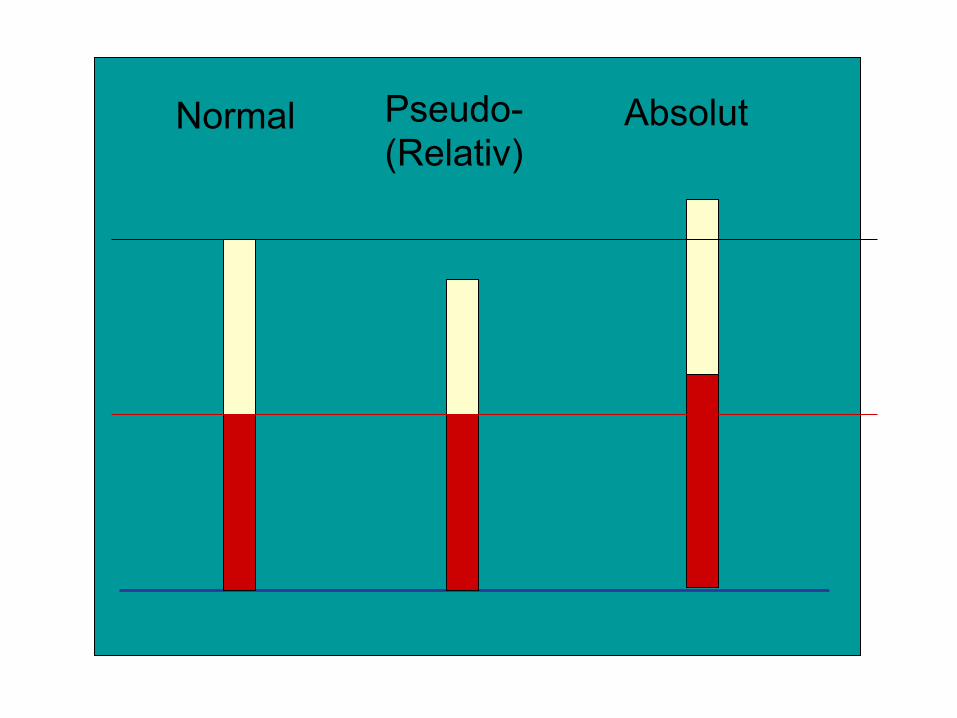
Normal Pseudo- (Relativ)
Absolut
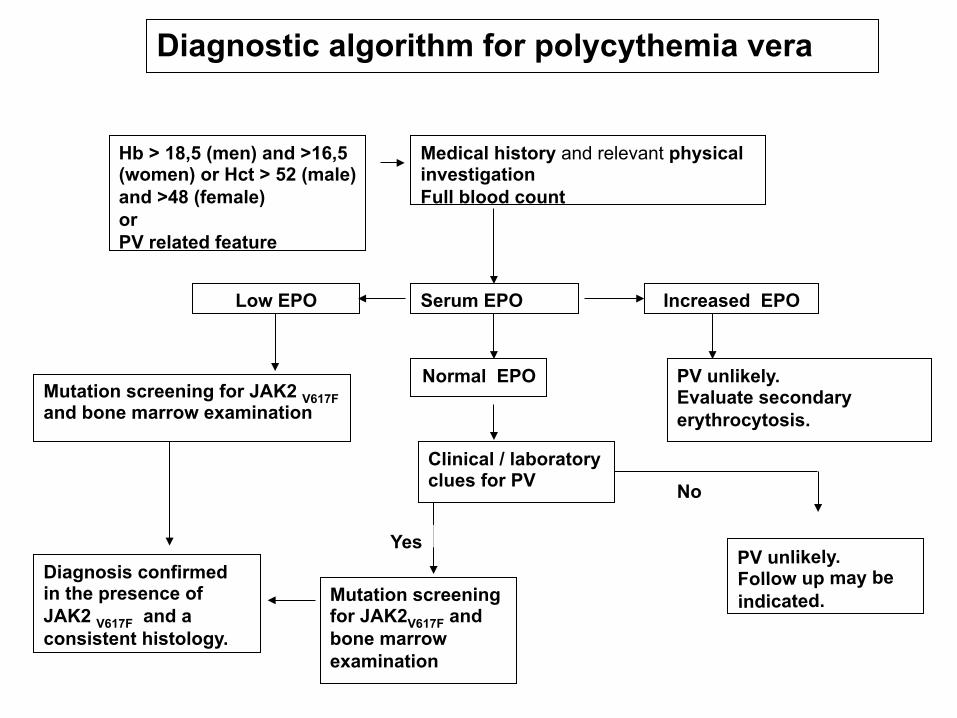
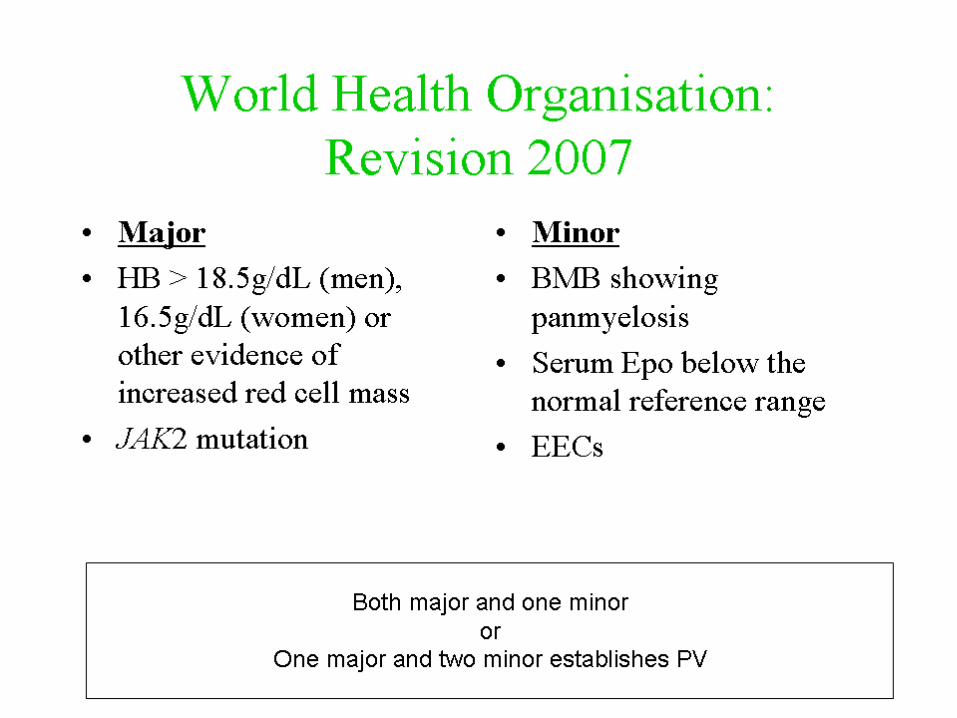
Diagnostic algorithm for polycythemia vera
Hb > 18,5 (men) and >16,5 (women) or Hct > 52 (male) and >48 (female) or PV related feature
Medical history and relevant physical investigation Full blood count
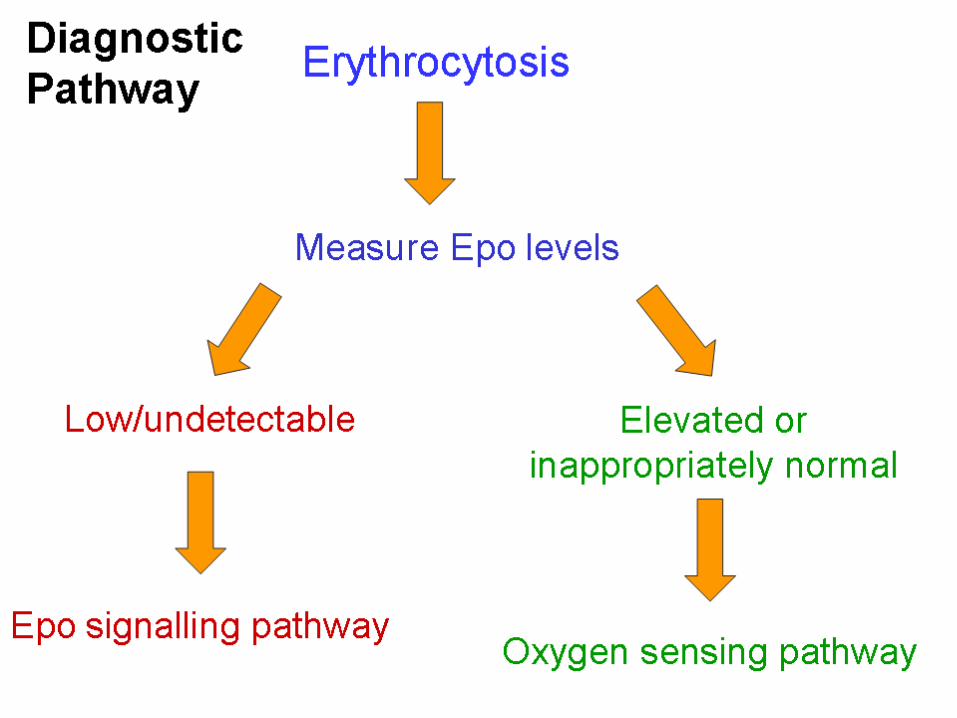
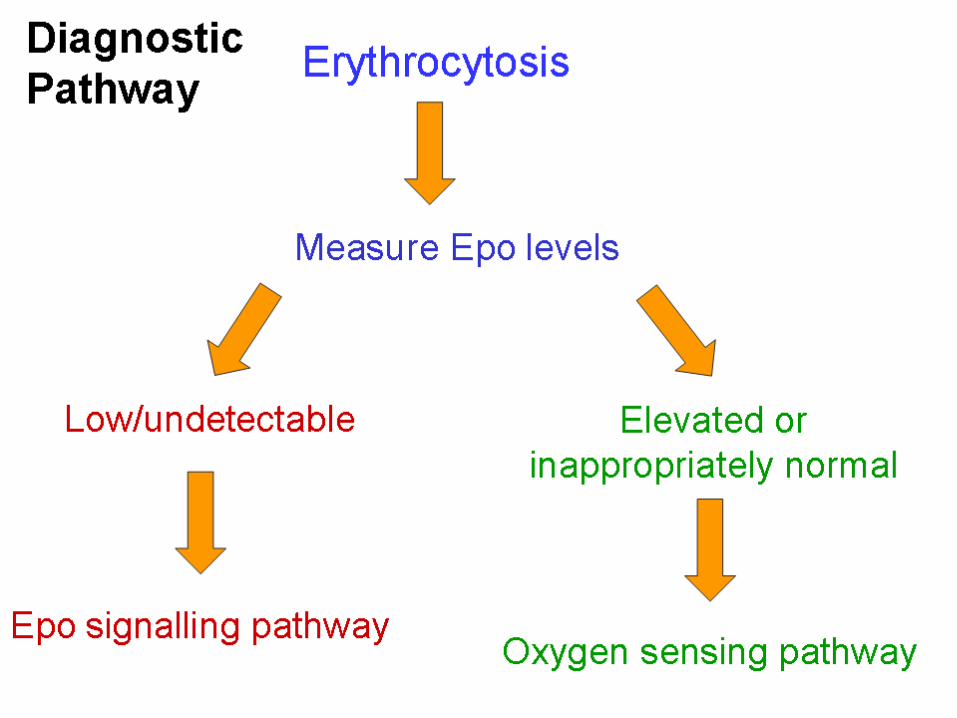
Serum EPO Increased EPO
Low EPO
Normal EPO Mutation screening for JAK2 V617F and bone marrow examination
Mutation screening for JAK2V617F and bone marrow examination
Diagnosis confirmed in the presence of JAK2 V617F and a consistent histology.
Clinical / laboratory clues for PV
PV unlikely. Evaluate secondary erythrocytosis.
PV unlikely. Follow up may be indicated.
Yes
No
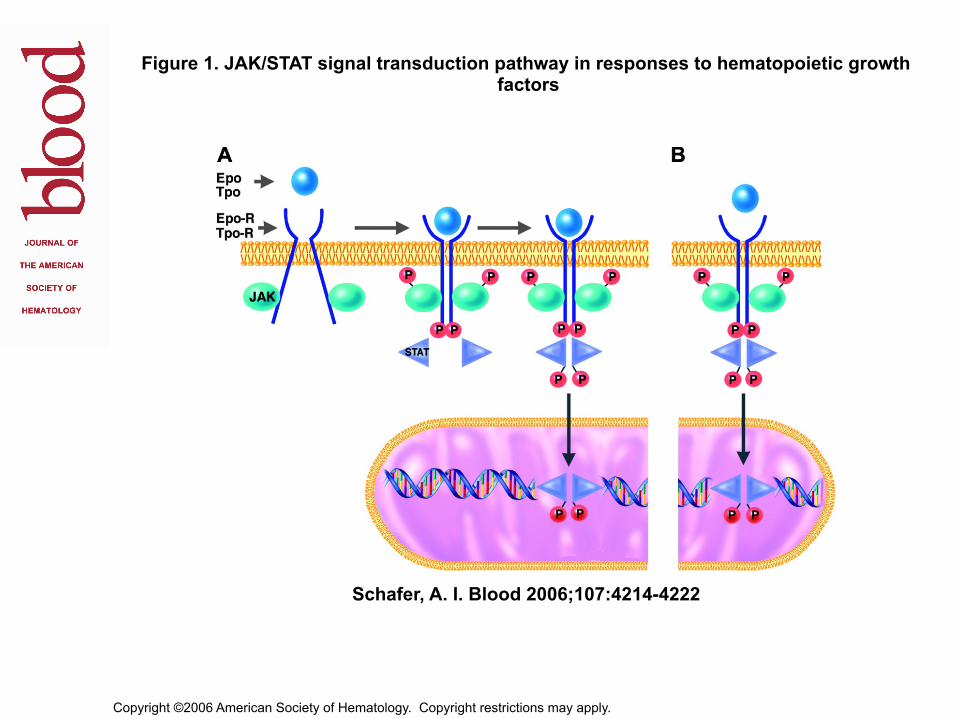
Copyright ©2006 American Society of Hematology. Copyright restrictions may apply.
Schafer, A. I. Blood 2006;107:4214-4222
Figure 1. JAK/STAT signal transduction pathway in responses to hematopoietic growth factors
Hur vanligt är PCV?
• Incidens ~ 200 pat/år i Sverige • Uppskattad prevalens ~ 2500 pat
• 5 % < 40 år vid diagnos • 1 % < 25 år • 0,1 % < 20 år
Polycytemia vera – naturalförloppet Chiewitz & Thiede Acta Med Scand 1962
• 250 pat • Obehandlad PCV 18 mån
medianöverlevnad • 70 % av dödsfallen i
trombos, fr a stroke
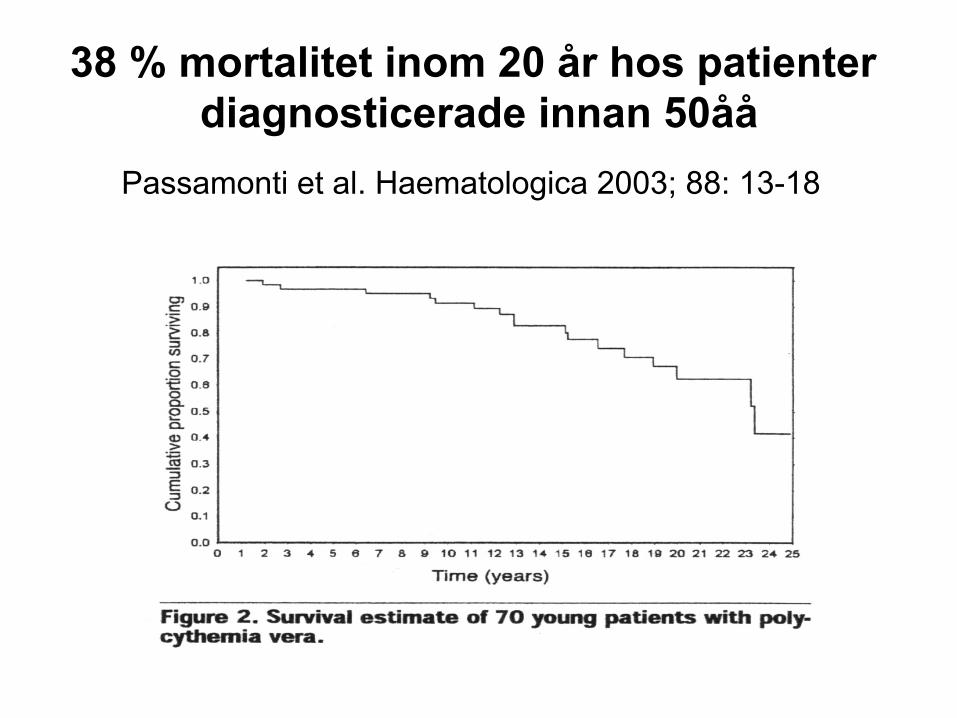
38 % mortalitet inom 20 år hos patienter
diagnosticerade innan 50åå Passamonti et al. Haematologica 2003; 88: 13-18
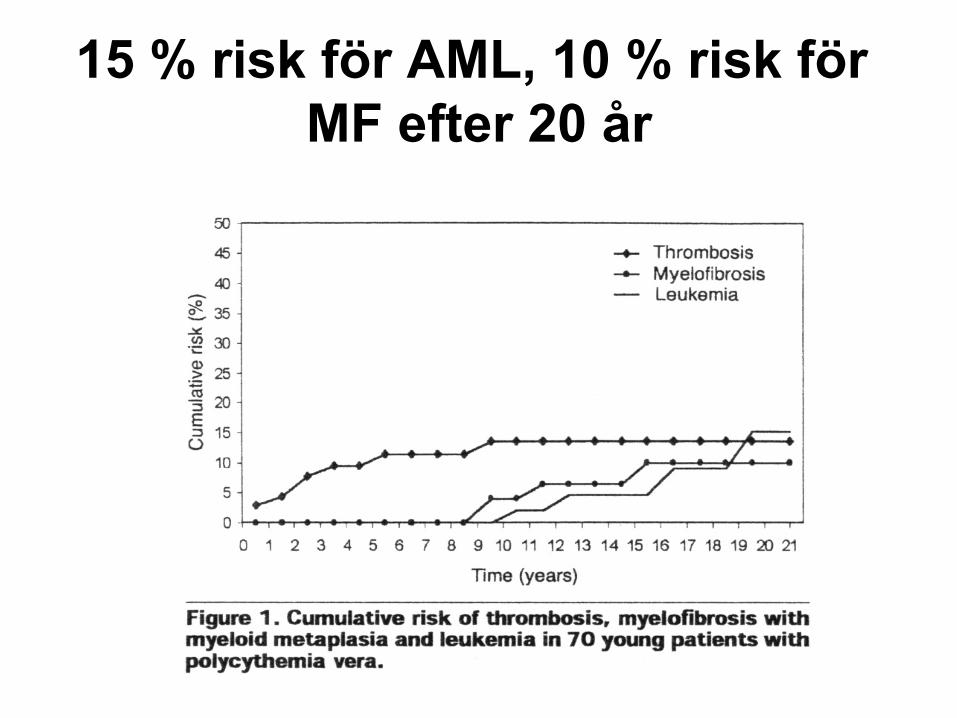
15 % risk för AML, 10 % risk för MF efter 20 år
Föreslagna rekommendationer för behandling PV
• Flebotomi för att hålla EVF < 0.45 (grad B rekommendation). Inget stöd för olika nivåer kvinna/man
• Acetylsalicylsyra 75 mg/dag om ej kontraindicerat (grad A rekommendation)
• Stöd rökstopp (grad C)
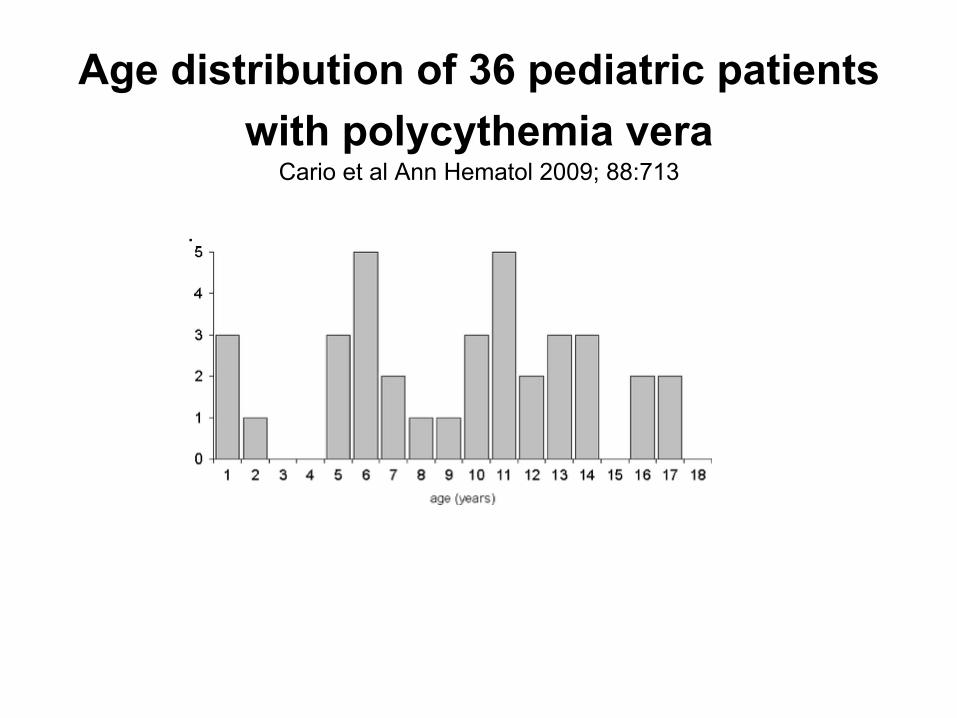
Age distribution of 36 pediatric patients
with polycythemia vera Cario et al Ann Hematol 2009; 88:713
.
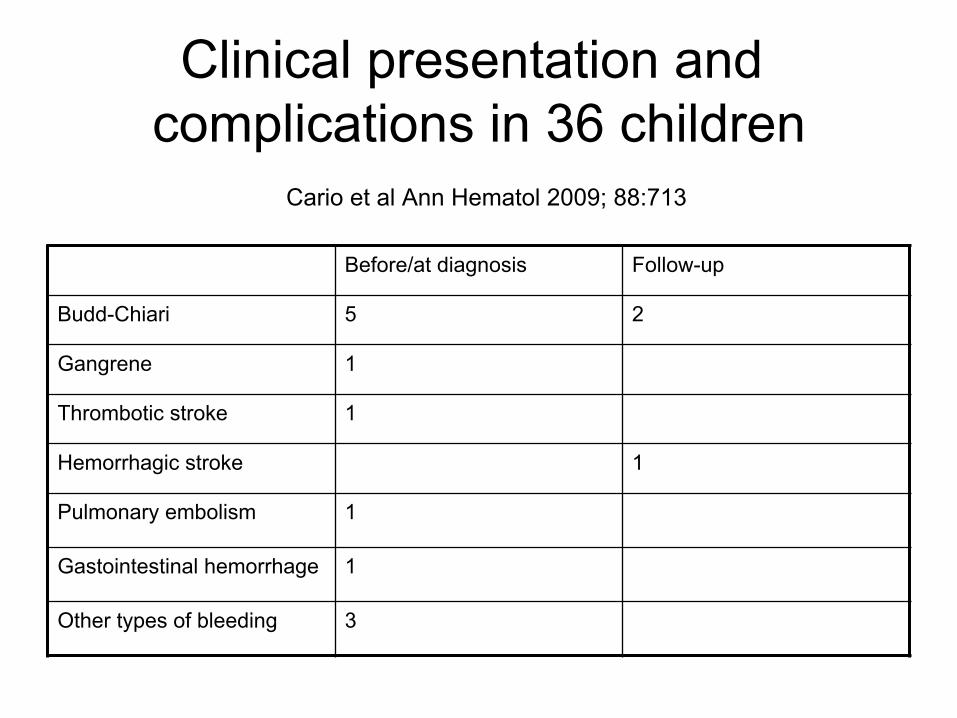
Clinical presentation and
complications in 36 children Cario et al Ann Hematol 2009; 88:713
Before/at diagnosis Follow-up
Budd-Chiari 5 2
Gangrene 1
Thrombotic stroke 1
Hemorrhagic stroke 1
Pulmonary embolism 1
Gastointestinal hemorrhage 1
Other types of bleeding 3
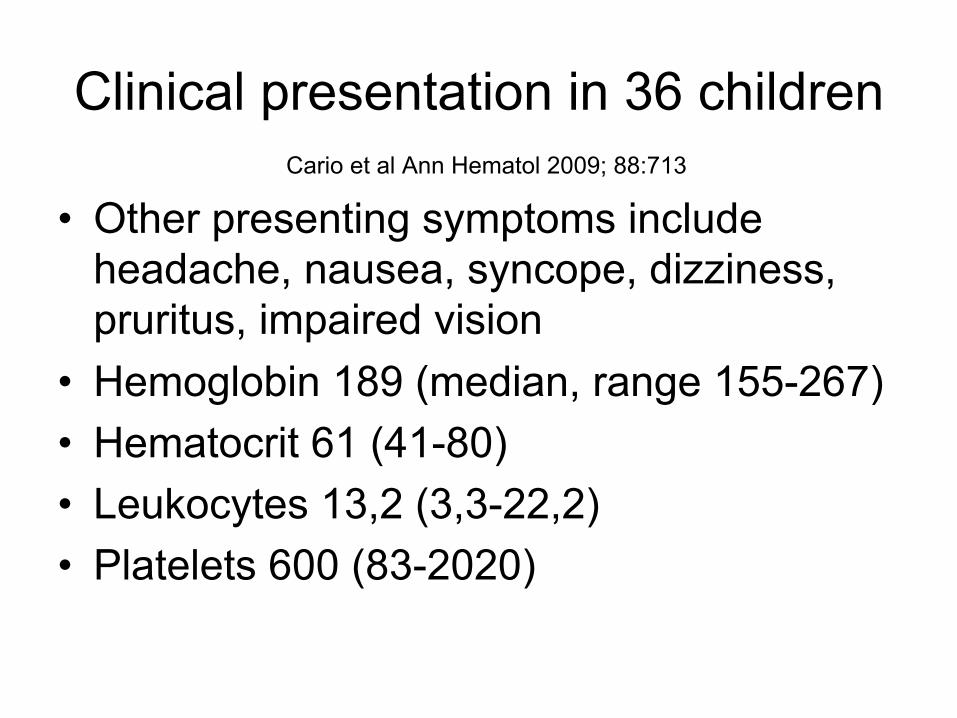
Clinical presentation in 36 children
Cario et al Ann Hematol 2009; 88:713
• Other presenting symptoms include headache, nausea, syncope, dizziness, pruritus, impaired vision
• Hemoglobin 189 (median, range 155-267) • Hematocrit 61 (41-80) • Leukocytes 13,2 (3,3-22,2) • Platelets 600 (83-2020)

Clinical presentation in 36 children
Cario et al Ann Hematol 2009; 88:713
• 17/19 patients subnormal S-EPO
• JAK2 V617F mutation 9/16, exon 12 mutation 2/16 → 10/16 (62 %) mutationsfrekvens
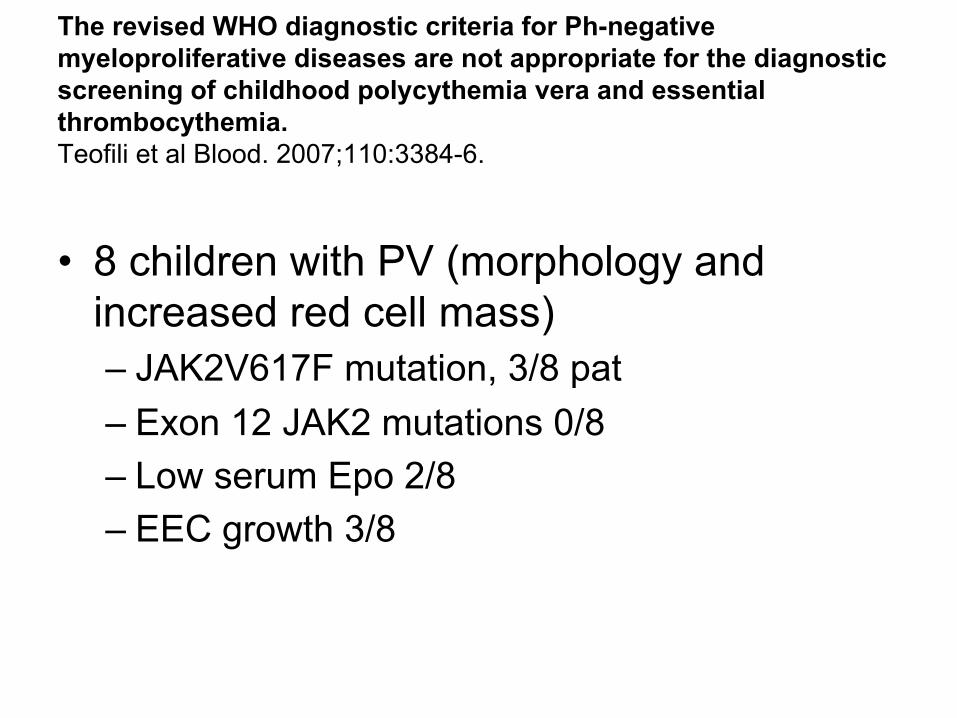
The revised WHO diagnostic criteria for Ph-negative myeloproliferative diseases are not appropriate for the diagnostic screening of childhood polycythemia vera and essential thrombocythemia. Teofili et al Blood. 2007;110:3384-6.
• 8 children with PV (morphology and increased red cell mass) – JAK2V617F mutation, 3/8 pat – Exon 12 JAK2 mutations 0/8 – Low serum Epo 2/8 – EEC growth 3/8
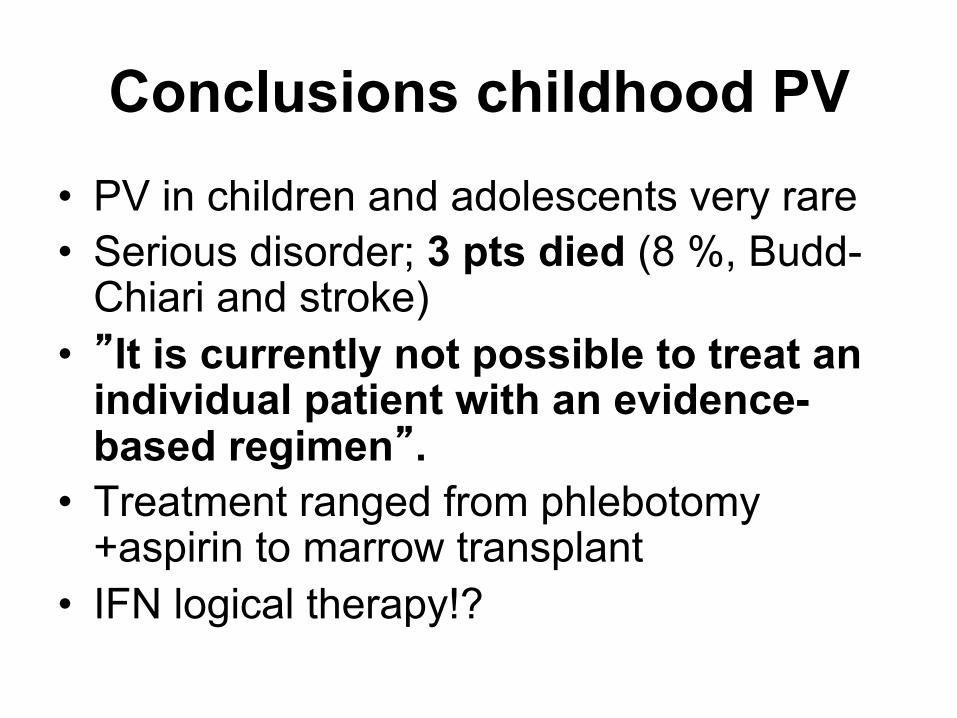
Conclusions childhood PV • PV in children and adolescents very rare • Serious disorder; 3 pts died (8 %, Budd-
Chiari and stroke) • ”It is currently not possible to treat an
individual patient with an evidence-based regimen”.
• Treatment ranged from phlebotomy +aspirin to marrow transplant
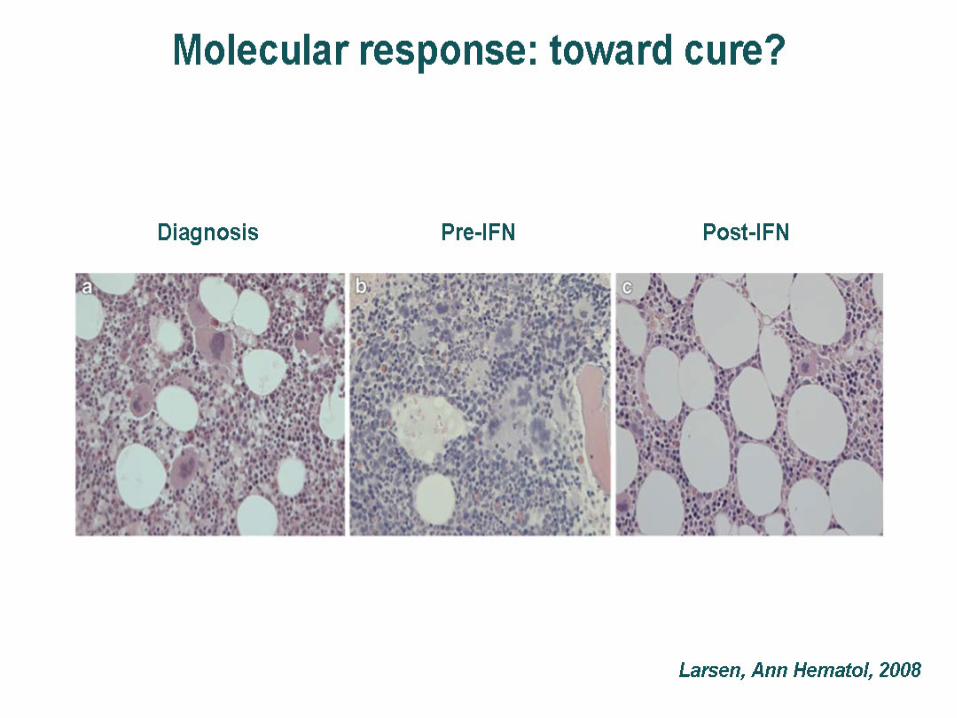
• IFN logical therapy!?
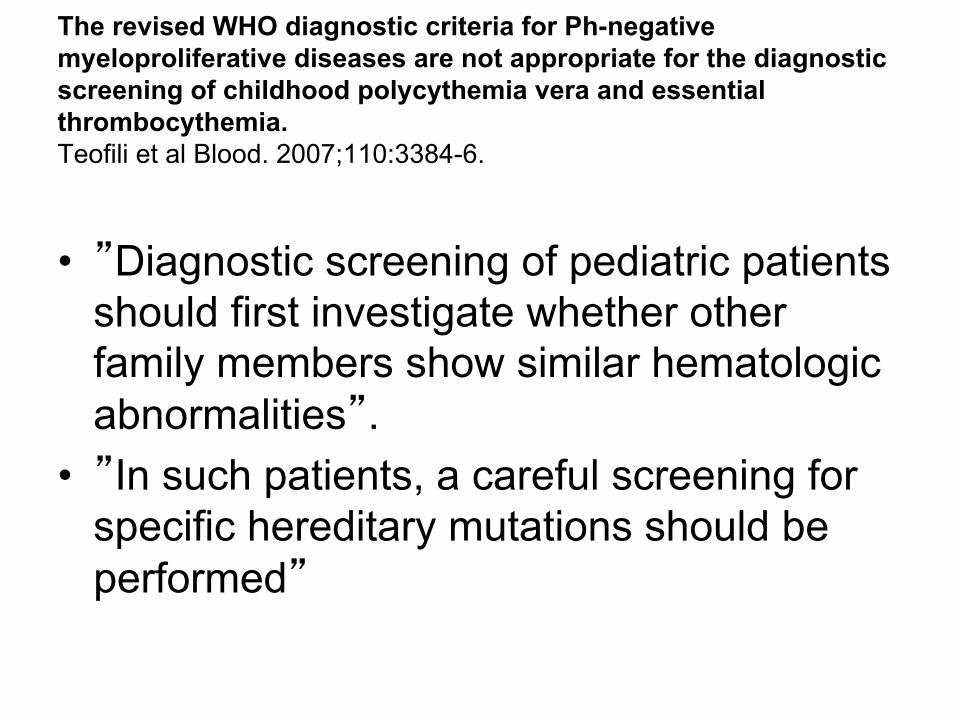
The revised WHO diagnostic criteria for Ph-negative myeloproliferative diseases are not appropriate for the diagnostic screening of childhood polycythemia vera and essential thrombocythemia. Teofili et al Blood. 2007;110:3384-6.
• ”Diagnostic screening of pediatric patients should first investigate whether other family members show similar hematologic abnormalities”.
• ”In such patients, a careful screening for specific hereditary mutations should be performed”


Eero MÄNTYRANTA Naturally Rich Blood
Time for questions!
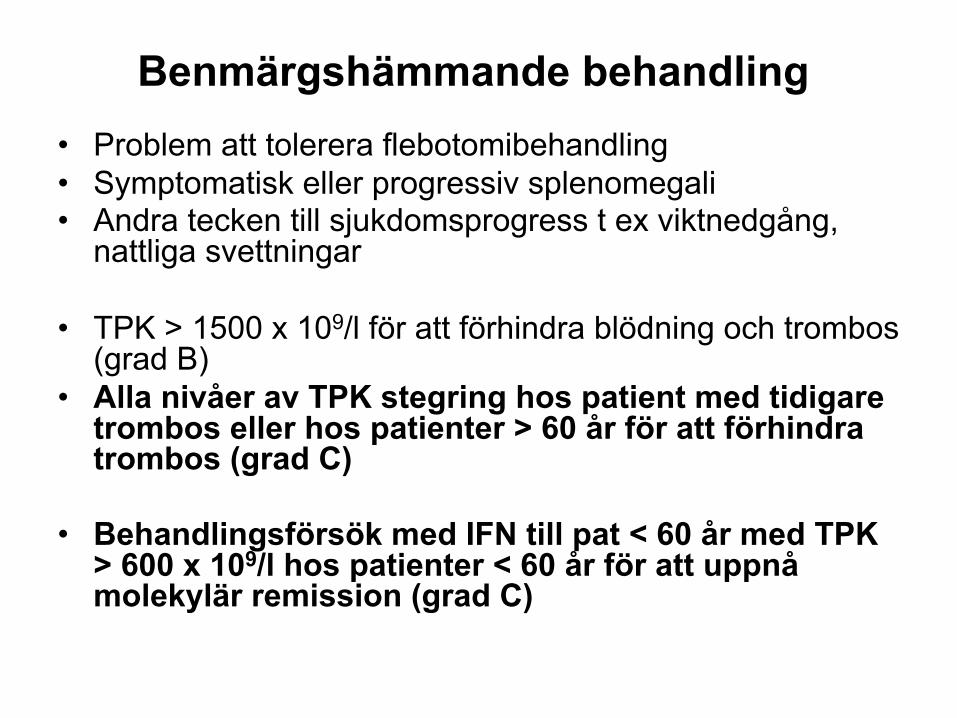
Benmärgshämmande behandling
• Problem att tolerera flebotomibehandling • Symptomatisk eller progressiv splenomegali • Andra tecken till sjukdomsprogress t ex viktnedgång,
nattliga svettningar
• TPK > 1500 x 109/l för att förhindra blödning och trombos (grad B)
• Alla nivåer av TPK stegring hos patient med tidigare trombos eller hos patienter > 60 år för att förhindra trombos (grad C)
• Behandlingsförsök med IFN till pat < 60 år med TPK > 600 x 109/l hos patienter < 60 år för att uppnå molekylär remission (grad C)