Embed Size (px)
Citation preview

9/22/2015
1
Trauma Centers:Challenges for the
Future
Glen A Franklin MD
Professor & Vice Chairman for Education
The Hiram C Polk, Jr MD Department of Surgery
University of Louisville
I Am No JD Richardson
• J David Richardson MD
• President-Elect of American College of Surgeons
• Professor & Vice Chairman Faculty Affairs
• Director Emergency Surgical Services
• Avid Horseman
• My Mentor, Colleague & Friend
J David Richardson

9/22/2015
2
University of Louisville Hospital
Louisville Trauma History
• Louisville “Accident Service” opens 1911 at Louisville City Hospital• Dr William O Roberts assigns 4 UofL Medical
Students to be on hand at all times to provided accidents victims with instant attention
• Credited with performing the first successful operation on a human abdominal stab wound
• Dr R Arnold Griswold (1932)• City’s first blood bank (developed auto transfusion)• Revolutionized fracture care (Griswold machine)• Operative intervention for penetrating cardiac injury• Equipped police cars and fire trucks with medical
supplies• Challenged Ford to design safer cars – collapsible
steering column, and probably the first advocate of seat belts in cars

9/22/2015
3
Access to Trauma Care
13 states lack Level 1 Trauma CenterMap shows those within 1 hr of Level 1 or 2 Centers
Traumamaps.org
US Highway Fatality
Ky State Police Data
9/22/2015
4
KY Trauma System
• House Bill 371• Co-sponsored by Rep. Bob DeWeese (MD) and Rep.
Mary Lou Marzian (RN), both of Louisville, was passed in 2008. It charged the Department for Public Health and the Kentucky Trauma Advisory Committee with developing and implementing a statewide trauma care system, integrated with the public health system for injury prevention.
• No money
• Entirely a grassroots effort!
KY Trauma Centers
II
IIIII
I
III
III
III II
IpIpIV
IVIV
IV
KY Trauma Centers

9/22/2015
5
New TechNew Tech FinancesFinances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges
New Tech FinancesFinances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges
Medical Advances
• We are in the “techno age”
• Tablets, iPhones, Twitter, Instagram, iWatches
• Medical knowledge and technology is advancing more rapidly than ever before
• “He who has the best toys, wins”
• High tech = high costs
• When does a new technology suddenly become the “standard of care”
New Tech

9/22/2015
6
Adopting New Technology
• Real consequences for cost of care (albeit they may be better)
• FAST• Easy to learn, several early adopters, training for both
surgeons and emergency medicine• Noninvasive, advertised as part of the “physical exam”• Ultrasound machine costs ~$20,000• DPL costs ~$150 (kit costs & procedure fee to patient)
• Virtually no major EDs without one in less than a decade
Resuscitation Tech
• Thromboelastography (TEG)
• Rotational thromboelastometry (ROTEM)• Method for testing the efficiency of blood
coagulation• Very little data
• Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA)• AAST Trial – 8 Trauma Centers (DuBose et al)
• Compared open occlusion vs REBOA• No difference in survival
• Angioembo pelvic fracture (Tesoriero et al)• ~5 hours to hemorrhage control• 60% deaths due to uncontrolled hemorrhage• Recommended early packing, REBOA and hybrid angio
suites with surgeon performed embolization
Other New Tech
• da Vinci Robot• ~$2 million• GU, GYN, ColoRectal, Thoracic,
ENT will want it• “Unless we inform the patient population
on this, there will be a drive from the consumer that trumps everything else, because at that point hospitals and physicians are caught in a difficult dilemma,” Michelassi said. “Hospitals and physicians are caught in the dilemma to either continue to deliver optimal care or to respond to market requests.” Fabrizio Michelassi MD

9/22/2015
7
Really Cool Tech
• DARPA (Defense Advanced Research Projects Agency)• Arsenal Foam Technology• “Wound Stasis System”
• Animal models reduced blood loss six fold and 72% survival rate vs 8% in controls
• EMS cannot afford the cost• Will need partners in Trauma
Centers to assist
• Will it matter in civilian penetrating or blunt trauma?
New TechNew Tech FinancesFinances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges
New TechNew Tech Finances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges

9/22/2015
8
Finances
• Money seems to be the primary driver
• As hospitals align in ACOs, where will trauma fit?
• UofL single most profitable activity is:• Basketball - $39 million
• Football - $24 million
• Trauma - $40 million
• More beds – NO
• New ED – NO
• Expanding Papa John’s Cardinal Stadium - YES
Finances
Who is Making the Money?
• Examined hospital and physician financial charges, cost and reimbursement
• Direct cost attributed on the basis of cost accounting system that attached resources used by the patient to the trauma hospital product line
• Commercial (55%), Govt(21%) & Indigent (24%)
Rodriguez, J Trauma, 2005
Trauma Center & Surgeon DichotomyInsured All Patients
• Trauma Center margin was 182-fold greater than the surgeons
• For every cost dollar generated by the surgeon, it recouped its cost plus 2 cents
• For every cost dollar generated by the hospital, it recouped its cost plus 47 cents
• Trauma Center margin was 31-fold greater than the surgeons
• For every cost dollar generated by the surgeon, it recouped its cost plus 35 cents
• For every cost dollar generated by the hospital, it recouped its cost plus 71 cents

9/22/2015
9
Trauma Centers Bleeding
• Texas: -$20 million
• California: -$400 million
• Georgia: -$70 million
Med Care, 2009
J Trauma, 2005
Impact of ACA
• Joseph et al, AAST 2015, July 2012 – Sept 2014
• 15% decrease in uninsured, 14% increase in reimbursement
• Decrease in commercially insured patients
New TechNew Tech FinancesFinances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges

9/22/2015
10
New TechNew Tech FinancesFinances Private vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges
Private vs Academic
• Rural trauma centers are primarily private facilities
• Private health care systems are rapidly developing trauma systems and centers• HCA & CHI
• They are frequently located in suburban areas which may offer better payer mixes than urban
• ACS only verifies, states designate
• Should there be documented “need” prior to trauma center development
Private vsAcademic
Florida’s Trauma Centers
9/22/2015
11
There’s a lot to read about
Best to let Dr John Armstrong tell the story
New TechNew Tech FinancesFinances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges

9/22/2015
12
New TechNew Tech FinancesFinances Private vsAcademicPrivate vsAcademic
Education Surgeon InterestSurgeon Interest
Trauma Center Challenges
Education
• ATLS, RTTDC, ASSET, ATOM, DMEP
• Surgical Education• Trauma vs Critical Care vs Acute Care Surgery
• ? Burn Surgery, Endovascular, Thoracic
• Maintaining surgical skills in the era of non-operative management of so many injuries
• Can others be trained to care for many non-operative patients freeing up more time for elective cases?
Education
Acute Care Surgery
• Trauma Surgeons believe the specialty must change
• Broader practice, emergency and elective surgery
• ACS is attractive to Trauma Surgeons
• Many lack some of the operative skills or an elective surgery practice
J Trauma, 2008
J Trauma, 2006
9/22/2015
13
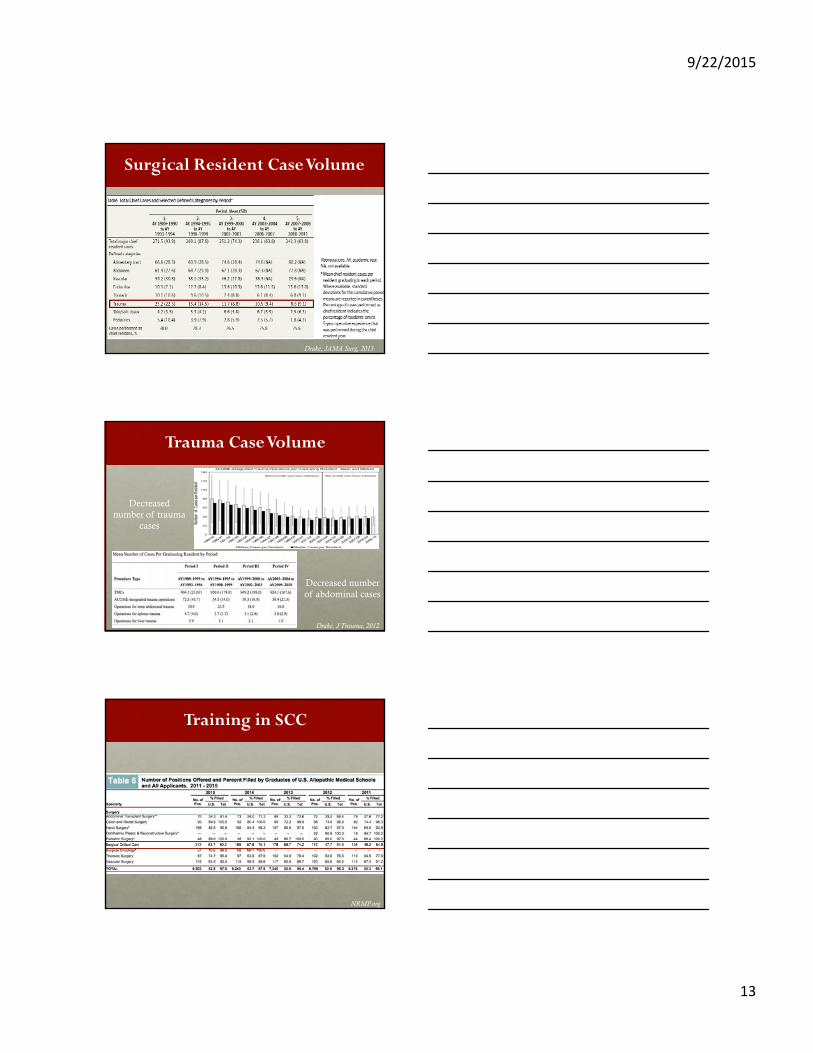
Surgical Resident Case Volume
Drake, JAMA Surg, 2013
Trauma Case Volume
Drake, J Trauma, 2012
Decreased number of trauma
cases
Decreased number of abdominal cases
Training in SCC
NRMP.org

9/22/2015
14
Programs & Positions Filled
Research & Scholarship
• Valsangkar, et al, AAST 2015
• Most crazy, extensive, complete, database search ever
• Scholarly metrics for 3,850 faculty at top 50 NIH-funded and 5 hospital-based surgery departments
① Junior TS had fewer papers than junior GS and Subspecialties
② Decreased NIH funding
③ Senior TS equally as productive
④ Are we just freeing up time for our colleagues to be more productive?
New TechNew Tech FinancesFinances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon InterestSurgeon Interest
Trauma Center Challenges
9/22/2015
15
New TechNew Tech FinancesFinances Private vsAcademicPrivate vsAcademic
EducationEducation Surgeon Interest
Trauma Center Challenges
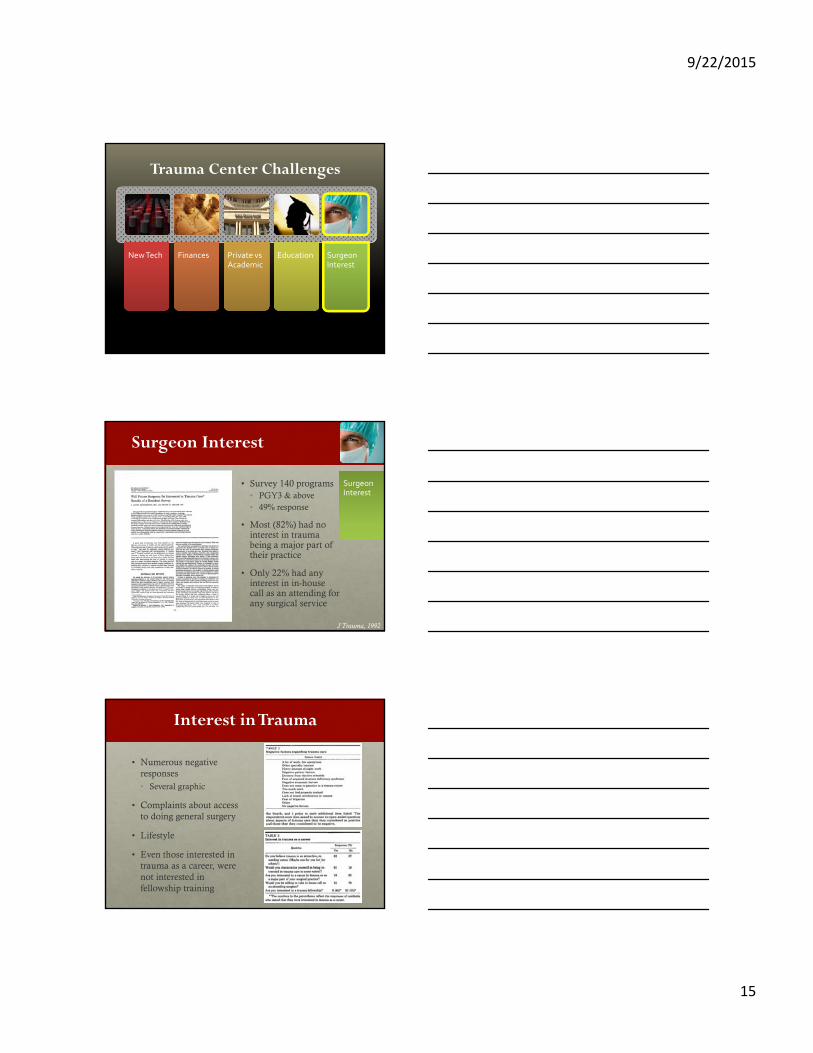
Surgeon Interest
• Survey 140 programs• PGY3 & above• 49% response
• Most (82%) had no interest in trauma being a major part of their practice
• Only 22% had any interest in in-house call as an attending for any surgical service
Surgeon Interest
J Trauma, 1992
Interest in Trauma
• Numerous negative responses• Several graphic
• Complaints about access to doing general surgery
• Lifestyle
• Even those interested in trauma as a career, were not interested in fellowship training

9/22/2015
16
What’s Up With Trauma?
• Cryer HM. The future of trauma care: At the crossroads. J Trauma. 2005;58:425-436.
• Esposito TJ, Rotondo M, Barie PS, et al. Making the case for a paradigm shift in trauma surgery. J Am CollSurg. 2006;202:655- 667.
• Moore EE, Maier RV, Hoyt DB, et al. Acute care surgery: Eraritjaritjaka. J Am Coll Surg. 2006;202:698-701.
• Moore EE. Trauma surgery: is it time for a facelift? Ann Surg. 2004;240:563-564.
• Esposito TJ, Leon L, Jurkovich GJ. The shape of things to come: results from a national survey of trauma surgeons on issues concerning their future. J Trauma. 2006;60:8-16.
• Ciesla DJ, Moore EE, Moore JB, et al. The academic trauma center is a model for the future trauma and acute care surgeon. J Trauma. 2005;58:657-662.
• Rodriguez JL, Christmas AB, Franklin GA, et al. Trauma/critical care surgeon: a specialist gasping for air. J Trauma. 2005;59:1-7.
• Roettger RH, Taylor SM, Youkey JR, et al. The general surgery model: a more appealing and sustainable alternative for the care of trauma patients. Am Surg. 2005;71:633-638.
• Richardson JD. Is there an ideal model for training the trauma surgeons of the future? J Trauma. 2003;54:795-797.
• Ciesla DJ, Moore EE, Cothren CC, et al. Has the trauma surgeon become house staff for the surgical subspecialist? Am J Surg. 2006;192:732-737.
The Painful Truth:The Documentation Burden of a Trauma Surgeon
• Golob et al, AAST 2015
• EHR to examine documentation by 8 trauma attendings
• 3,111 admissions (2014) with 26,455 entries (74% were daily progress notes, 5% op notes
A Discipline in Crisis?
• Steven Green MD• Loma Linda University
• Trauma Surgery: a discipline in crisis
• Golden Age of Trauma Surgery was ¼ century ago
• Shift to non-operative care
• Non-surgeon management in Europe & Canada
• Decline of Trauma Surgery within General Surgery
• Lack of ABS approved subspecialty
• Shortage of Trauma Surgeons
• Attempt to “reinvigorate” our field by redefining it as Acute Care Surgery
Green, Annals of Em Med,

9/22/2015
17
Will General Surgeons Do the Work?
• Expresses concern over the availability of trauma care outside of the Trauma Center model
• Concerns raised over the lack of general surgery for those who choose trauma as a career
• General surgeons can and should provide trauma care in areas where it is needed
Presidential Address AAST 1999, J Trauma, 2000
What About Trauma Surgeons Doing General Surgery?
• Total Trauma Service admissions averaged 3,003 patients per year (34% nontrauma)
• Minor procedures decreased as DPL gave way to FAST and CT
• 33% of operations were on nontrauma, particularly as non-operative management increased
J Trauma, 2000
What Can We Do?
• Don’t give up hope
• Trauma Centers are as necessary as air and water
• Continue to partner with Local, State and Federal Government (they need to know, they need us)
• Work with other specialties, we are all part of the “team”• Advocacy work with OTA, NNA, STN, ATS, SCCM, COT,
AANS, ACEP, AAST, EAST
• Define who we are (General Surgeons who practice urgent care)
• Strengthen our practice with evidence based care

9/22/2015
18
Trauma Center Challenges
• We will face many challenges in the future• Costs, external forces, reimbursement models,
recruitment and retention
• We are sometimes a specialty looking for it’s true identity• General surgery, trauma surgery, critical care, emergency
surgery, acute care surgery
• We are no longer the “only ones” interested in trauma
• But, we will evolve to meet the challenge
• The future is bright and just around the corner
Questions
Thanks to the Trauma Center Association of America

![Universitatea Tehnica de Constructii Bucuresti · 2020. 7. 30. · DIASPORA Rom,/ Rep Moldova Albania Rep Moldova Rep. Moldova Rep. Moldova Rep Moldova DIASPORA Rom] lordania Rep](https://img.pdfslide.tips/doc/110x75/60ac185ef0835e610377952c/universitatea-tehnica-de-constructii-bucuresti-2020-7-30-diaspora-rom-rep.jpg)



























