-
ICU monitoring; Critically ill trauma patient
ICU trauma
-
Tri Modal Distribution of Trauma Death
-
First peak
Tri Modal Distribution of Trauma Death
-
Second peak Golden hours
30% (hemorrhage)
(Central nervous systems)
Tri Modal Distribution of Trauma Death
-
Third peak 24 10-20%
pulmonary embolism multi-organ failure
Tri Modal Distribution of Trauma Death
-
Patho: Critically ill Trauma Patients
(Gebhard & Huber-Lang, 2008)
-
Critically ill Trauma Patients
(Gebhard & Huber-Lang, 2008)
-
Hypoperfusion
TBI IICP
Blunt abd. FIND
Chest inj. ICD
Shock SI
TM monitoring RASS,PAIN
-
Traumatic brain injury
ICP ICP
CPP CPP
CBF CBF
Ischemia
Ischemia
Edema
Edema
Tissue pressure
Tissue pressure
Secondary Brain injury
Primary Brain injury
Goal is to stop
2nd injury
CPP=MAP-ICP
CPP=Cerebral Perfusion Pressure CBF = cerebral blood flow
Factor:2nd TBI Hypotension hypoxia
Factor:2nd TBI Hypotension hypoxia
-
Traumatic brain injury
Goal of treatments
(American college of surgeons,2015)
-
Traumatic brain injury
How to stop 2nd brain injury
Step 1. Management of intracranial pressure
Head of bed 30 degrees
Sedation and analgesia (recommend
propofol,midazolam,fentanyl)
Continuous ventricular drainage
If ICP >20-25 mmHg. Next steps?
(American college of surgeons,2015)
-
Traumatic brain injury
Step 2. hyperosmolar therapy (mannital,3%NSS)
Keep CPP > 50 mmHg. ICP
Neuromuscular blocking
Suction clear airway (15sec,80 mmHg., SjvO2>50%
If ICP >20-25 mmHg. Next step?
(American college of surgeons,2015)
-
Traumatic brain injury
Step 3. decompresive hemi-craniectomy adequate sedation : goal
paralysis propofol hypotension
SBP>100 mmHg. #### Propofol
phebitis### Hypothermia ( 4mm.
90%
(American college of surgeons,2015)
-
Blunt Abdominal injury
F Fast track (trauma)
I Intra abdominal pressure
Keep
-
F: Fast track (Trauma)
Indication : Vascular injury, penetrating injury, Hypovolemic
shock, cardiac arrest
Management:
1.notify staff trauma
2.Door to OR 30 (team : Ward + Blood Bank+lab+Anesth.)
3.Post-OP care in ICU
-
I:intra-abdominal pressure
-
Infuse 50-100 mL saline into an empty bladder, measureing at the
level of the symphysis pubis
-
I:intra-abdominal pressure
-
D: drainage
Suction abdominal drainage < 40 mmHg.
Record content drainage per hour. Keep
-
ICU TM KKH.
-
trauma triad of death
-
HEMORRHAGE TRUAMA Classification of shock
-
Resuscitate goal
SvO2 >70%
-
SI
-
Goals of damage control in the severely Injured Patient
1. Stable airway and oxygenation
2. Effective analgesia and sedation (MO,fentanyl,midazolam)
3. Hemostasis-control of life-threatening hemorraghe (EL,
Thoracotomy,ligation, Temporary closure etc.)
4. Appropriated blood compossition (RBC,Plt.,Clotting
factors,Ca+,glucose,K,CL)
-
Predicting Fluid Responsiveness
SVV keep 9-13%
Leg raising test
CVP keep 8-15 mmHg.
-
Hemodynamic monitoring
-
SVV
-
Leg raising
: A-line , flow-track, VIGILIO
-
CVP:Central venous pressure
the Frank-Starling curves
-
46
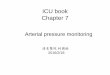
Fluid Challenge Test
Initial CVP 15 cm H2O
PAOP 16 mm Hg
Volume & Rate 200 mL/10 min 100 mL/10 min 50 mL/10 min
During infusion, CVP rises >5 cm H2O
or PAOP rises >7 mm Hg
Yes No
Stop challenge Complete the volume
Wait 10 min Wait 10 min
CVP change >5 3-5
-
Secondary care: set zero Complication
TM Pt
IHT
Delirium
CAUTI
VAP
CLABSI
malnutrition
-
IHT:Intrahospital Transfer
Cardiac arrest
Respiratory problem
SBP 20%
cardiac arrest Management
Respiratory problem
Management
shock Management
Agitation Agitation Management
1. 2. 3.
1. 2. 3.
-
Delilium
Risk factors for delirium ( daily alcohol,
smoke,intubation,Isolation, no visible daylight)
the Confusion Assessment Method for the ICU (CAM-ICU) the
Intensive Care Delirium Screening Checklist (ICDSC)
Sedate critical care clients carefuly; monitor sedation,
analgesia, and delirium scores
Holiday sedate sedate 1-2
-
The bloomsbury sedation scale Sedation Score
3 Agitation and restless
2 Awake and comfortable
1 Aware but calm
0 Roused by voice
-1 Roused by touch
-2 Roused by painful stimuli
-3 Unrousable
A Natural sleep
P Paralysed
-
Richmond Agitation-Sedation Scale
-
CAUTI:catheter associated urinary tract infection
1.
2. 2
3.
4.
-
VAP:Ventilator associated pneumonia
CPIS score
30
mouth care q 2 hr. (chlorhexidine, special mouth wash)
Suction prn. 1-2
Check cuff pressure keep 20-30 cmH2O
-
Prevention central line-associated bloodsteam
infection(CLABSI)
C-line
2 tegaderm
triple lumen/duble lumen 7
septicemia Hemo culture
Change heparin every day
-
Malnutrition
The subjective global assessment (SGA),IJEE
Early feeding 24-48 hr.
Continous feeding
20 cc/hr. Check content 4 hr. keep
-
Biffl et al,2002)
-
Biffl, W. L., Moore, E. E., & Haenel, J. B. (2002).
Nutrition support of the trauma patient. Nutrition, 18(11),
960-965.
Ely, E. W., Truman, B., Shintani, A., Thomason, J. W., Wheeler,
A. P., Gordon, S., ... & Sessler, C. N. (2003). Monitoring
sedation status over time in ICU patients: reliability and validity
of the Richmond Agitation-Sedation Scale (RASS). Jama, 289(22),
2983-2991.
Curtis N. Sessler, Mark S. Gosnell, Mary Jo Grap, Gretchen M.
Brophy, Pam V. O'Neal, Kimberly A. Keane, Eljim P. Tesoro, and R.
K. Elswick "The Richmond AgitationSedation Scale", American Journal
of Respiratory and Critical Care Medicine, Vol. 166, No. 10 (2002),
pp. 1338-1344.
-
http://www.edwards.com/eu/products/pages/cceducationmap.aspx
Truman, B., Stephens, R., & Ely, E. W. (2003). Critical care
nurses'
perspectives on delirium in the ICU.(Poster Abstracts). American
Journal of Critical Care, 12(3), 284-285.
Ghajar, J. (2000). Traumatic brain injury. The Lancet,
356(9233), 923-929. Spahn, D. R., Bouillon, B., Cerny, V., Coats,
T. J., Duranteau, J., Fernndez-
Mondjar, E., ... & Neugebauer, E. (2013). Management of
bleeding and coagulopathy following major trauma: an updated
European guideline. Crit Care, 17(2), R76.
Rowe, K., & Fletcher, S. (2008). Sedation in the intensive
care unit. Continuing Education in Anaesthesia, Critical Care &
Pain, 8(2), 50-55.
Kusek, L. (2012). Preventing central line-associated bloodstream
infections. Journal of nursing care quality, 27(4), 283-287.
-
Thank you
-
Keep warm
How to Keeping Pt. warm
Warm blood products/IV
Blanket warmer
Warm operating room
-
Clinical differences between TIC and DIC
TIC DIC
Early bleeding Late bleeding
Hypothermia Normo-/hyperthermia
Hypovolemia Euvolemia
Systemic anticoagulation Systemic hypercoagulation
Hyperfibrinolysis Hypofibrinolysis(occasionally: hyper)
Microthrombi rare Microthrombi
TIC Trauma-induced intravascular coagulopathy, DIC disseminated
intravascular coagulopathy