Embed Size (px)
Citation preview

IgM Nephropathy11/29/2011
Jun‐Ki Park

•
First described by Cohen, Border et al. in 1978, in a series of 12
cases whose initial native renal biopsy specimens displayed:
‐
mild glomerular mesangial hypercellularity on light microscopy
‐
Diffuse granular mesangial IgM and C3 deposition on IF
‐
EM showed generalized foot‐process effacement; mesangial
electron‐
dense deposits were seen in ~50% of the patients.
•
Excluded those that showed focal sclerosis, those with systemic
disease such as lupus or vasculitis.
•
Critical distinction between IgM mesangial nephropathy and MCD is
poor response rate to steroid therapy.

Light microscopy usually indicates diffuse
proliferation of mesangial cells and
accumulation of extracellular mesangial matrix
Diffuse, granular, mesangial deposition of IgM,
often is associated with complement,
especially C3
EM shows generalized foot‐process
effacement and mesangial electron‐dense
deposits

•
Failure to identify IgM nephropathy as a distinct clinicopathological entity thus far may have resulted
from failure to adhere to strict pathological criteria.
•
Other series of patients with ‘IgM nephropathy’ have included patients with FSGS (O’Donoghue et al. QJM
1991)
and normal glomeruli by light microscopy (Myllymaeki et al. AJKD 2003) on initial biopsy.
•
Its extreme forms resemble MCD and FSGS

Is IgM Nephropathy a distinct disease entity?Pro…
Border et al. KI 1988

Is IgM Nephropathy a distinct disease entity?Pro…
Border et al. KI 1988

Is IgM Nephropathy a distinct disease entity?Pro…•
Recurrent IgM nephropathy in renal allograft.
‐
Solomon et al. 1981: recurrence in 3 weeks after Tx
‐
Myllymaeki et al. 2003: included normal glomeruli by light microscopy
‐
Salmon et al. NDT 2004: Recurrent diffuse, granular mesangial deposition, with increased mesangial matrix and cellularity in the allograft, 4 yrs after Tx.

Is IgM Nephropathy a distinct disease entity?Contra…•
Many investigators report its presence in the context of MCD, MH
and FSGS, rather than as a distinct pathological entity(Vilches et al Lab Invest 1982; Ji‐Yun et al. KI 1984; Pardo et al. AJKD 1984; Lool et al. Pathology 1985..)
•
Other cases show IgM on IF (often segmental rather than diffuse)
but no mesangial deposits on electron microscopy.
•
IgM deposition without accompanying glomerular abnormalities by
light microscopy is reported to occur in up to 60% or normal kidneys
donated for Tx. (Bloom et al. KI 1978)
•
The International Study of Kidney Disease in Children (ISKDC) did not
differentiate MCD with IgM+ IF from MCD when it characterized
childhood nephrotic syndrome.

Is IgM Nephropathy a distinct disease entity?Contra…
•
Relationship of the IgM in areas of sclerosis to that in the
mesangium of non‐sclerotic glomeruli is unknown, sclerotic
lesions of many diseases demonstrate the presence of IgM
and C3.
(Velosa etal. Mayo Clin Proc 1975)
•
In this setting, the IgM may be nonspecifically deposited onto
an abnormally permeable glomerular basement membrane or
trapped in an area of glomerulosclerosis.

Is IgM Nephropathy a distinct disease entity?Contra…
•
Experimental studies have demonstrated an increase in
uptake of macromolecules by the mesangium in
experimentally induced nephrotic syndrome whether induced
by aminonucleoside of puromycin or anti‐GBM antibody.
•
The mechanism of increased uptake is not clear but may
reflect increased mesangial perfusion in nephrotic states. It is
possible that the deposition of IgM in the mesangium in INS
reflects a similar mechanism
Michael et al. KI 1980

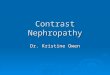
Morphologic transition observed
The morphologic group and outcome
in patients with idiopathic nephrotic
syndrome who had more than one
biopsy; the presence (+) or absence
(—) of IgM in the glomerulus is
indicated.
Ji‐Yun et al. KI 1984

IgMN: clinical picture and long‐term prognosis
•
Of 2217 biopsy specimens between 1977 –
1998, 110
specimen met criteria for IgM nephropathy. (included normal
glomeruli on LM)
•
Excluded patients with systemic disease (SLE, RA, DM,
paraproteinemia)
•
63 M/47F
•
Mean age was 29yrs (range 1‐75yrs); 36 were younger than
16yrs
Myllymaeki et al. AJKD Feb 2003

IgMN: clinical picture and long‐term prognosis
Myllymaeki et al. AJKD Feb 2003

Myllymaeki et al. AJKD Feb 2003

Myllymaeki et al. AJKD Feb 2003

Myllymaeki et al. AJKD Feb 2003

Fig 2. Renal insufficiency and ESRD in patients with IgM
nephropathy at time of biopsy and in postbiopsyfollow‐up.
Myllymaeki et al. AJKD Feb 2003

Myllymaeki et al. AJKD Feb 2003

•
The histologic and clinical criteria for diagnosing IgMN,
the effect of mesangial IgM on prognosis and response
to therapy, and the relation of IgMN to MCD are
questions that cannot be fully resolved until the genesis
of the IgM deposits is understood.

Pathogenesis•
The pathogenesis of IgM nephropathy remains
unclear, although abnormal T‐cell function or a disturbance in immunoaggregate clearance by
mesangial cells have been suggested.
•
Many studies have reported increased serum IgM or IgM immunocomplex concentration in patients with IgM nephropathy.

In vitro B‐lymphocyte switch disturbance from IgM into IgG in IgMN
Lin et al. Pediatr Nephrol 1989

In vitro B‐lymphocyte switch disturbance from IgM into IgG in IgMN
Lin et al. Pediatr Nephrol 1989

Fig. 1. Serum IgM levels in patients
with IgM mesangial nephropathy (●),
minimal change nephrotic syndrome
(MCNS) with hypercellularity (◌) and
MCNS with normal cellularity (□)
during the acute nephrotic phase.
The solid lines indicate values (mean
+ 2SD) from normal controls
Lin et al. Pediatr Nephrol 1989

Fig. 2. Relationship between serum IgM level and in vitro IgM production
during acute nephrotic phase in patients with IgMN (●), MCNS with
hypercellularity (◌) and normal cellularity (□)
Lin et al. Pediatr Nephrol 1989

Lin et al. Pediatr Nephrol 1989
suppressor T‐cells
activated suppressor T‐cells
suppressor T‐cell inducers

In vitro B‐lymphocyte switch disturbance from IgM into IgG in IgMNAuthors conclude:
•Previous B‐lymphocyte development study demonstrated T‐cell involvement in the
constant region of heavy chain (CH) isotype "switching".
•The abnormality of T‐cells may influence the isotype expression and even the Ig
production.
•Hyperfunction of the suppressor T‐cells in the IgMN and MCNS patients with
hypercellularity may play a role as a direct or indirect "switch
blocker" and cause a
high level of IgM production, a low level of IgG production, in these patients during
the acute nephrotic phase.
•The OKT8 cell levels were correlated both with in vitro IgM production and with in
vitro IL‐2 production. These results indicate that high Tac expressed, activated
suppressor T‐cells either directly cause hyperfunction of suppressor T‐cells or
secrete some factor(s) which block(s) the switch of immunoglobulin synthesis from
IgM to IgG, leading to high serum IgM and low serum IgG levels.

Circulating heavy IgM in IgMN
DiSciullo et al. Clin. Exp. Immunol 1988

Presence of heavy IgM
DiSciullo et al. Clin. Exp. Immunol 1988

DiSciullo et al. Clin. Exp. Immunol 1988
Circulating heavy IgM in IgMN

Presence of IgM‐C3 complex
•
Fractions were collected and assayed for the presence of IgM
and IgM‐C3 complexes using enzyme immunoessays.
•
Dissociation of this heavy IgM by KSCN and glycine HCL is
compatible with the hypothesis that the IgM is in the form of
circulating immune complexes. This is further supported by
the observation of acid dissociable C3‐IgM complexes.

Presence of IgM‐C3 complex
•
May indicate abnormality in B cell differentiation d/t defect in
regulatory T cell function.
•
May be secondary reduce clearance of circulating antigen IgM
antibody complexes. (e.g in liver dysfunction)
•
Circulating IgM complexes have been detected in SLE, viral
hepatitis A and , IgAN, HSP, membranous GN and lupus
nephritis.
•
Increased IgM immuncomplexes may be compatible with
IgMN but not proof that IgMN is separate disease entity.


Swartz et al. Pediatr Nephrol 2009

Swartz et al. Pediatr Nephrol 2009

Swartz et al. Pediatr Nephrol 2009

Swartz et al. Pediatr Nephrol 2009

Swartz et al. Pediatr
Nephrol
2009

In conclusion:
‐IgM
pos IF identified to be a marker of disease severity in children with
MCD, MH and FSGS
‐Children with steroid‐dependent or steroid‐resistant nephrotic
syndrome and MCD with IgM
pos IF have a relatively poor prognosis
and poor response to adjuvant therapy
‐Children with MCD with IgM
pos IF have a tendency to respond better
to cyclosporine therapy as initial adjuvant therapy when compared with
cyclophosphamide.
‐A prospective study is needed to verify the findings

Summary•
It remains controversial, if IgMN
is a separate disease
•
Strict pathological criteria to define IgMN
needed
•
Studies required to elucidate pathogenetic
role of IgM
deposits on
molecular level
•
Presence of IgM
deposits in MCD signifies poorer prognosis, with
fewer than 50% steroid sensitivity
•
Prospective studies required to identify favorable adjuvant therapy

Thank You!