Embed Size (px)
Citation preview

In the name of godIn the name of god
04/18/2304/18/23 11ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

Congenital Congenital muscular torticollismuscular torticollis
Mohammad reza etemadifar MDMohammad reza etemadifar MD
St Zahra hospitalSt Zahra hospital
Isfahan university of medical Isfahan university of medical sciencessciences
04/18/2304/18/23 22ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

terminologyterminology
• The term torticolis is derived form The term torticolis is derived form two Latin words, tortus, meaning two Latin words, tortus, meaning “twisted,” and collum, meaning “twisted,” and collum, meaning “neck,.”“neck,.”
• Wryneck is a lay term is used to Wryneck is a lay term is used to describe torticollis arising from any describe torticollis arising from any cause.cause.
04/18/2304/18/23 33ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

definitiondefinition• Congenital muscular Congenital muscular
torticollis is an torticollis is an asymmetrical deformity asymmetrical deformity of the head and neck of the head and neck – the head is tilted toward the head is tilted toward
the side with the the side with the shortened muscleshortened muscle
– the chin rotated towards the chin rotated towards the opposite side. the opposite side.
• This is caused by This is caused by unilateral contracture of unilateral contracture of the sternocleidomastoid the sternocleidomastoid muscle. muscle.
04/18/2304/18/23 44ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
etiologyetiology
• The exact cause of fibrosis of the The exact cause of fibrosis of the sternocleidomastoid muscle in congenital sternocleidomastoid muscle in congenital muscular torticollis is not known.muscular torticollis is not known.
• Intrauterine malposition is commonly Intrauterine malposition is commonly associated with the deformity and associated with the deformity and possibly it is due to a local ischemic possibly it is due to a local ischemic process resulting from intrauterine process resulting from intrauterine malposition. malposition.
04/18/2304/18/23 55ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

etiologyetiology
• The immediate cause of the The immediate cause of the deformity is fibrosis within the deformity is fibrosis within the sternocleidomastoid muscle, which sternocleidomastoid muscle, which subsequently contracts and shortens. subsequently contracts and shortens.
• The exact pathogenesis of the The exact pathogenesis of the fibrosis is unknown. Edema, fibrosis is unknown. Edema, degeneration of muscle fibers and degeneration of muscle fibers and acute inflammation lead to fibrosis. acute inflammation lead to fibrosis.
04/18/2304/18/23 66ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

PathologyPathology
• On section, the “tumor” appears white and On section, the “tumor” appears white and glistening, in gross appearance resembling glistening, in gross appearance resembling a soft fibroma.a soft fibroma.
• Microscopic study shows that it consist of Microscopic study shows that it consist of dense fibrous tissue. dense fibrous tissue.
• In an older child, after the disappearance In an older child, after the disappearance of the tumor, tissue excised from of the tumor, tissue excised from sternocleidomastoid muscle shows that the sternocleidomastoid muscle shows that the muscle has been replaced fibrous tissuemuscle has been replaced fibrous tissue
04/18/2304/18/23 77ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
• If the deformity is not corrected the soft If the deformity is not corrected the soft tissues of the affected side undergo tissues of the affected side undergo adaptive shortening as growth proceeds. adaptive shortening as growth proceeds.
• The deep cervical fascia becomes The deep cervical fascia becomes thickened and contracted. thickened and contracted.
• The scalenus The scalenus anterior and medius muscles and medius muscles become shortened. become shortened.
• Later, the carotid sheath and the enclosed Later, the carotid sheath and the enclosed vessels contract. vessels contract.
PathologyPathology
04/18/2304/18/23 88ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

clinical Findingsclinical Findings
• The deformity may be present at birth or it The deformity may be present at birth or it may become evident about the second or may become evident about the second or third weeks.third weeks.
• The condition is more common in girls The condition is more common in girls than in boys.than in boys.
• The head is tilted towards side of the The head is tilted towards side of the affected muscle, and the chin is rotated to affected muscle, and the chin is rotated to the opposite side.the opposite side.
• Rotation of the neck to the side of the Rotation of the neck to the side of the deformity and lateral motion to the deformity and lateral motion to the opposite side are limitedopposite side are limited
04/18/2304/18/23 99ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

clinical Findingsclinical Findings
• Palpation reveals a hard, nontender, Palpation reveals a hard, nontender, fusiform swelling, or tumor, in the fusiform swelling, or tumor, in the sternocleidomastoid muscle. Usually both sternocleidomastoid muscle. Usually both the sternal and clavicular heads are the sternal and clavicular heads are involved.involved.
• Occasionally only the sternal head is Occasionally only the sternal head is affected.affected.
• The superior portion of the muscle close The superior portion of the muscle close to its mastoid attachment is rarely, if ever, to its mastoid attachment is rarely, if ever, involved.involved.
04/18/2304/18/23 1010ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
clinical Findingsclinical Findings
• If the contracture is not treated If the contracture is not treated secondary deformities of the face secondary deformities of the face and head develop. The face on the and head develop. The face on the side of the contracted muscle side of the contracted muscle becomes flattened because of becomes flattened because of external pressure. The infant usually external pressure. The infant usually sleeps in prone posture.sleeps in prone posture.
04/18/2304/18/23 1111ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

clinical Findingsclinical Findings
• Spontaneously, as it is more comfortable, Spontaneously, as it is more comfortable, the neck is rotated so that the affected the neck is rotated so that the affected side is down. side is down.
• Ipsilaterally, the face is flattened by Ipsilaterally, the face is flattened by remodeling to conform to the bed. remodeling to conform to the bed.
• A word of caution is appropriate A word of caution is appropriate plagiocephaly can be congenital owing to plagiocephaly can be congenital owing to synostosis of the coronal fissures; this is synostosis of the coronal fissures; this is ruled out by radiograms of the skull.ruled out by radiograms of the skull.
04/18/2304/18/23 1212ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

clinical Findingsclinical Findings
• With skeletal growth, asymmetry of the face With skeletal growth, asymmetry of the face increase. increase.
• The levels of the eyes and ears change, The levels of the eyes and ears change, defects that are less noticeable when the head defects that are less noticeable when the head is tilted to one side and more obvious when is tilted to one side and more obvious when the head and neck are straight in the midline. the head and neck are straight in the midline.
• Eye strain may result from ocular imbalance.Eye strain may result from ocular imbalance.
• A lower cervical-upper dorsal scoliosis with A lower cervical-upper dorsal scoliosis with concavity towards the affected side may concavity towards the affected side may develop.develop.
04/18/2304/18/23 1313ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
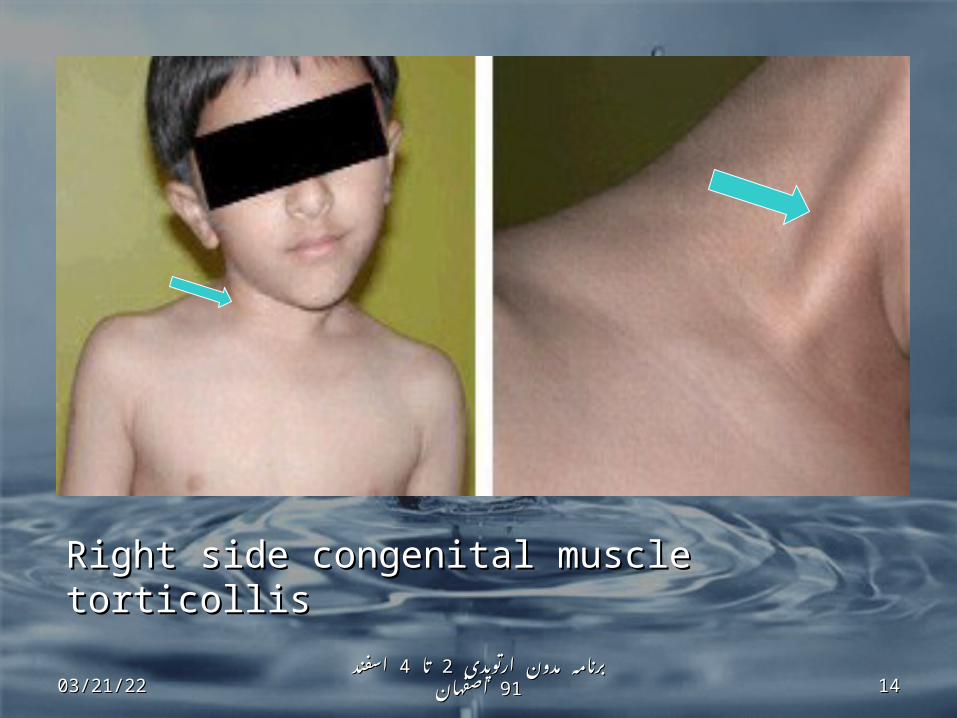
Right side congenital muscle torticollisRight side congenital muscle torticollis
04/18/2304/18/23 1414ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

Left sided congenital muscle torticollisLeft sided congenital muscle torticollis
04/18/2304/18/23 1515ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
diagnosisdiagnosis
• Recognition of congenital muscular torticollis is Recognition of congenital muscular torticollis is not usually difficult because of the characteristic not usually difficult because of the characteristic cordlike contracture of the cordlike contracture of the sternocleidomastoid musclesternocleidomastoid muscle. . The early The early fusiform tumor may escape notice. Postural fusiform tumor may escape notice. Postural torticollis should be distinguished from torticollis should be distinguished from congenital muscular torticollis.congenital muscular torticollis.
• The The postural deformationpostural deformation is caused by is caused by intrauterine malposture, and the deformity is intrauterine malposture, and the deformity is less severe. Although the sternocleidomastoid less severe. Although the sternocleidomastoid muscle is shortened, there is no true fibrotic muscle is shortened, there is no true fibrotic replacement of the muscle. Often there are replacement of the muscle. Often there are other findings associated with intrauterine other findings associated with intrauterine malposture such as pelvic obliquity with malposture such as pelvic obliquity with abduction-adduction contracture of the hips, or abduction-adduction contracture of the hips, or postural metatarsus varus or valgus.postural metatarsus varus or valgus.04/18/2304/18/23 1616
ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامهاصفهاناصفهان

Differential Diagnosis of Congenital Differential Diagnosis of Congenital Muscular TorticollisMuscular Torticollis
Congenital AnomaliesCongenital Anomalies• Postural torticollis Postural torticollis • Hemivertebra, cervical-superior dorsal spine Hemivertebra, cervical-superior dorsal spine • Unilateral atlanto-occipital fusion Unilateral atlanto-occipital fusion • Klippel-Feil syndrome Klippel-Feil syndrome • Unilateral congenital absence of sternocleidomastoid muscle Unilateral congenital absence of sternocleidomastoid muscle • Pterygium colli Pterygium colli Trauma-particularly C1, C2Trauma-particularly C1, C2• Rotatory subluxation Rotatory subluxation • Fracture Fracture Inflammatory conditions unilateralInflammatory conditions unilateral• Cervical lymphadenitis Cervical lymphadenitis • Spontaneous hyperemic subluxation of the atlas Spontaneous hyperemic subluxation of the atlas • Rheumatoid arthritis Rheumatoid arthritis Neurologic DisordersNeurologic Disorders• Visual disturbances Visual disturbances • Syringomyelia Syringomyelia • Cervical spinal cord tumor Cervical spinal cord tumor • Brain tumor, Brain tumor, posterior fossa fossa 04/18/2304/18/23 1717
ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامهاصفهاناصفهان

Evaluation of torticollisEvaluation of torticollis
• Diagnostic algorithm Diagnostic algorithm
04/18/2304/18/23 1818ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

Imaging Algorithm for Acute TorticollisImaging Algorithm for Acute Torticollis
Patient withtorticollis
Newborn infantOlder child or
adult
Trauma No traumaUltrasound
CT neck and/orcervical spine
Negative Positive
StopCT or MRI of
neck
CT neck and/or cervical spine
Negative Positive NegativePositive
StopMRI C-Spine
MRA neckMRI C-spine
MRI brainStop
04/18/2304/18/23 1919ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

Type 1 Atlanto-axial Rotatory Type 1 Atlanto-axial Rotatory FixationFixation
Axial CT image with head rotated to left shows Axial CT image with head rotated to left shows widened space between dens and right C1 lateral widened space between dens and right C1 lateral mass which persists with rotation of head to right mass which persists with rotation of head to right (arrowheads) compatible with AARF. The atlanto-(arrowheads) compatible with AARF. The atlanto-
dental interval is normal making this a type 1 AARF.dental interval is normal making this a type 1 AARF.04/18/2304/18/23 2020
ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامهاصفهاناصفهان

TreatmentTreatment
• Treatment should be begun as soon Treatment should be begun as soon as the diagnosis is made.as the diagnosis is made.
• Manipulations consisting of passive Manipulations consisting of passive stretching of the contracted stretching of the contracted sternocleidomastoid muscle should sternocleidomastoid muscle should be performed by the parents after be performed by the parents after adequate instruction.adequate instruction.
04/18/2304/18/23 2121ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

Manipulation techniqueManipulation technique• First the head is bent First the head is bent
laterally so that the ear laterally so that the ear on the side opposite on the side opposite the shortened muscle the shortened muscle approaches the approaches the shoulder, then the shoulder, then the head is rotated so that head is rotated so that the chin approaches the chin approaches the shoulder of the the shoulder of the affected side. affected side.
04/18/2304/18/23 2222ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
• An additional method of stretching the An additional method of stretching the sternocleidomastoid muscle is to make use of sternocleidomastoid muscle is to make use of gravity by placing the infant supine on the gravity by placing the infant supine on the mother’s lap with the head hanging into mother’s lap with the head hanging into hyperextension. One hand stabilizes the hyperextension. One hand stabilizes the shoulders and chest, and the other hand tilts shoulders and chest, and the other hand tilts the head laterally away from the contracted the head laterally away from the contracted muscle so that the contra lateral ear touches muscle so that the contra lateral ear touches the opposite shoulder. The chin is then the opposite shoulder. The chin is then rotated toward the contracted muscle. rotated toward the contracted muscle.
04/18/2304/18/23 2323ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

• Prone posture during sleep should be Prone posture during sleep should be avoided, as it will aggravate the facial avoided, as it will aggravate the facial deformities and the contracture. deformities and the contracture.
• Ordinarily, if the stretching exercises are Ordinarily, if the stretching exercises are begun at a very early age and begun at a very early age and performed faithfully and correctly every performed faithfully and correctly every day, the contracture of the day, the contracture of the sternocleidomastoid muscle will sternocleidomastoid muscle will corrected and surgery will not be corrected and surgery will not be necessary. necessary.
04/18/2304/18/23 2424ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
• It is unlikely that the fibrous cord that It is unlikely that the fibrous cord that replaces the sternocleidomastoid replaces the sternocleidomastoid muscle can be stretched by muscle can be stretched by manipulation after the age of manipulation after the age of one yearone year. .
• This is especially true if restriction of This is especially true if restriction of rotation of the neck is greater than 30 rotation of the neck is greater than 30 degrees and there is an established degrees and there is an established facial asymmetry. facial asymmetry.
04/18/2304/18/23 2525ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

SurgerySurgery
• In 10% of children, surgery may be In 10% of children, surgery may be needed to correct the torticollis. This needed to correct the torticollis. This is an outpatient surgery to lengthen is an outpatient surgery to lengthen the short muscle. the short muscle.
04/18/2304/18/23 2626ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

Surgery Surgery is indicated is indicated
• when the torticollis does not respond when the torticollis does not respond to conservative measures up to one to conservative measures up to one year of ageyear of age
• in cases in which the condition is in cases in which the condition is
neglected until the child is a year old neglected until the child is a year old or when the parents have not or when the parents have not complied in performing an effective complied in performing an effective exercise regimenexercise regimen
04/18/2304/18/23 2727ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
Age considerationsAge considerations
• Only conservative treatment is indicated Only conservative treatment is indicated during infancy (scar is a problem) during infancy (scar is a problem)
• the operation should be delayed until the the operation should be delayed until the child is between the ages of 1 and 4 years.child is between the ages of 1 and 4 years.
• Some recommend surgery after 3 years Some recommend surgery after 3 years • bipolar release should be considered as bipolar release should be considered as
the treatment of choice in patients older the treatment of choice in patients older than 6 years of age than 6 years of age
• Surgery performed Surgery performed before the age of 6 before the age of 6 to 8to 8 years may allow remodeling of any years may allow remodeling of any facial asymmetry and plagiocephalyfacial asymmetry and plagiocephaly
• In older ages also it is better to operate In older ages also it is better to operate 04/18/2304/18/23 2828
ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامهاصفهاناصفهان

• Satisfactory results are usually Satisfactory results are usually obtained by division or partial obtained by division or partial excision of the muscle, provided the excision of the muscle, provided the head is kept in the corrected position head is kept in the corrected position for a sufficient length of time after for a sufficient length of time after the operation, and active and passive the operation, and active and passive exercises are carried out to prevent exercises are carried out to prevent any recurrence of the deformity. any recurrence of the deformity.
04/18/2304/18/23 2929ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

Surgical techniquesSurgical techniques
• Unipolar releaseUnipolar release of the of the muscle distally is muscle distally is appropriate for mild appropriate for mild deformity.deformity.
• Bipolar releaseBipolar release proximally and distally proximally and distally may be indicated for may be indicated for moderate and severe moderate and severe torticollis or recurrent torticollis or recurrent cases cases
• LENGTHENING?LENGTHENING?
• Endoscopic release ??Endoscopic release ??
04/18/2304/18/23 3030ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

AFTERTREATMENTAFTERTREATMENT
• manual stretching ,muscle manual stretching ,muscle
strengthening, and active range-of-strengthening, and active range-of-motion exercises of the neck three motion exercises of the neck three times daily for 3 to 6 monthstimes daily for 3 to 6 months
• The use of plaster casts or braces The use of plaster casts or braces usually is unnecessary usually is unnecessary
• Head-halter traction or a cervical Head-halter traction or a cervical collar?collar?
04/18/2304/18/23 3131ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

prognosisprognosis
• Good or excellent results in 60 to 80 Good or excellent results in 60 to 80 % of surgically treated cases% of surgically treated cases
• The younger the patient the better The younger the patient the better surgical resultssurgical results
04/18/2304/18/23 3232ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان

summarysummary• CMT is a deformity caused by fibrosis of CMT is a deformity caused by fibrosis of
sternomastoid musclesternomastoid muscle• Usually is diagnosed in early infancyUsually is diagnosed in early infancy• More common in girlsMore common in girls• Stretching exercises is recommended in 1Stretching exercises is recommended in 1stst
year of life (about 9o% will improve)year of life (about 9o% will improve)• Surgery is recommended after infancy(2-3 Surgery is recommended after infancy(2-3
years)years)• Unipolar release for mild and bipolar Unipolar release for mild and bipolar
release for severe deformityrelease for severe deformity• Up to 8 years head and facial deformity Up to 8 years head and facial deformity
will improve very well after surgerywill improve very well after surgery• In older ages also it is better to operateIn older ages also it is better to operate• Surgical outcome usually is satisfactorySurgical outcome usually is satisfactory04/18/2304/18/23 3333
ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامهاصفهاناصفهان
• A woman brought her three-month-old infant to the A woman brought her three-month-old infant to the physician for an examination because she was concerned physician for an examination because she was concerned about the position of the infant's head. The pregnancy and about the position of the infant's head. The pregnancy and delivery were unremarkable. Physical examination revealed delivery were unremarkable. Physical examination revealed that the head and body were in an asymmetrical position that the head and body were in an asymmetrical position otherwise, the infant appeared normal. Passive range of otherwise, the infant appeared normal. Passive range of motion in the neck was almost normal with no tightness. motion in the neck was almost normal with no tightness. There was no palpable tumor of the sternocleido-mastoid There was no palpable tumor of the sternocleido-mastoid muscle. Neurologic examination and an ultrasound scan of muscle. Neurologic examination and an ultrasound scan of the neck muscles were normalthe neck muscles were normal
04/18/2304/18/23 3434ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
QuestionQuestion
Based on the patient's history and Based on the patient's history and physical examination, which one of the physical examination, which one of the following is the most likely diagnosis?following is the most likely diagnosis?
• A. Benign, paroxysmal torticollis.A. Benign, paroxysmal torticollis.
• B. Neurogenic torticollis.B. Neurogenic torticollis.
• C. Osseous torticollis.C. Osseous torticollis.
• D. Postural torticollisD. Postural torticollis
04/18/2304/18/23 3535ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان
• Postural torticollis is a painless condition that typically Postural torticollis is a painless condition that typically presents during infancy. The condition usually resolves presents during infancy. The condition usually resolves within a few months without the need for operative within a few months without the need for operative treatment. Potential complications include cervical treatment. Potential complications include cervical scoliosis with compensatory thoracic scoliosis, facial scoliosis with compensatory thoracic scoliosis, facial asymmetry, and plagiocephaly.asymmetry, and plagiocephaly.
• After a child is diagnosed with postural torticollis, the After a child is diagnosed with postural torticollis, the family may be educated about a home stretching family may be educated about a home stretching program and positional cues to encourage functional program and positional cues to encourage functional stretching and use of the muscle. Stretching helps stretching and use of the muscle. Stretching helps resolve torticollis, but follow-up is needed to assess resolve torticollis, but follow-up is needed to assess progressprogress
04/18/2304/18/23ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان 3636

Thank you for your Thank you for your attentionattention
04/18/2304/18/23 3737ارتوپدی مدون ارتوپدی برنامه مدون 9191اسفند اسفند 44تا تا 22برنامه
اصفهاناصفهان