Embed Size (px)
Citation preview
Integrating Prevention & Treatment of Substance Use Disorders with Primary Care
Webinar – June 19, 2013
Patrick GauthierAHP Healthcare Solutions
1
PROBLEM Fragmentation Marginalization Discrimination High Costs Poor Quality and Outcomes High Morbidity and Mortality High Societal Costs Multiple Chronic Conditions
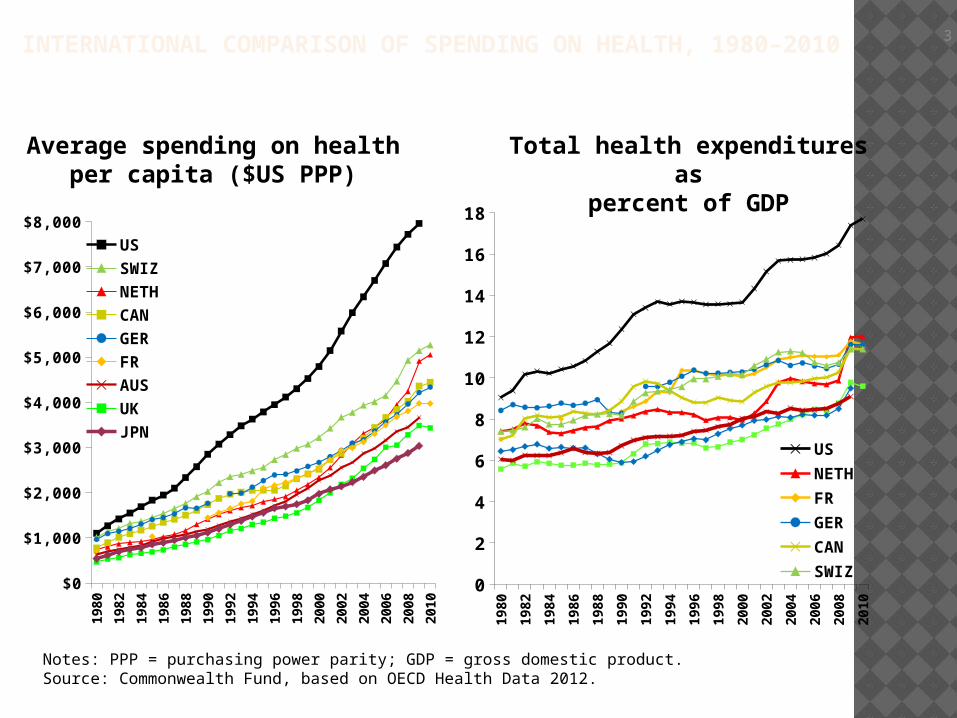
INTERNATIONAL COMPARISON OF SPENDING ON HEALTH, 1980–2010
19
80
19
82
19
84
19
86
19
88
19
90
19
92
19
94
19
96
19
98
20
00
20
02
20
04
20
06
20
08
20
10
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
USSWIZNETHCANGERFRAUSUKJPN
3
Average spending on healthper capita ($US PPP)
19
80
19
82
19
84
19
86
19
88
19
90
19
92
19
94
19
96
19
98
20
00
20
02
20
04
20
06
20
08
20
10
0
2
4
6
8
10
12
14
16
18
USNETHFRGERCANSWIZUK
Total health expenditures aspercent of GDP
Notes: PPP = purchasing power parity; GDP = gross domestic product.Source: Commonwealth Fund, based on OECD Health Data 2012.
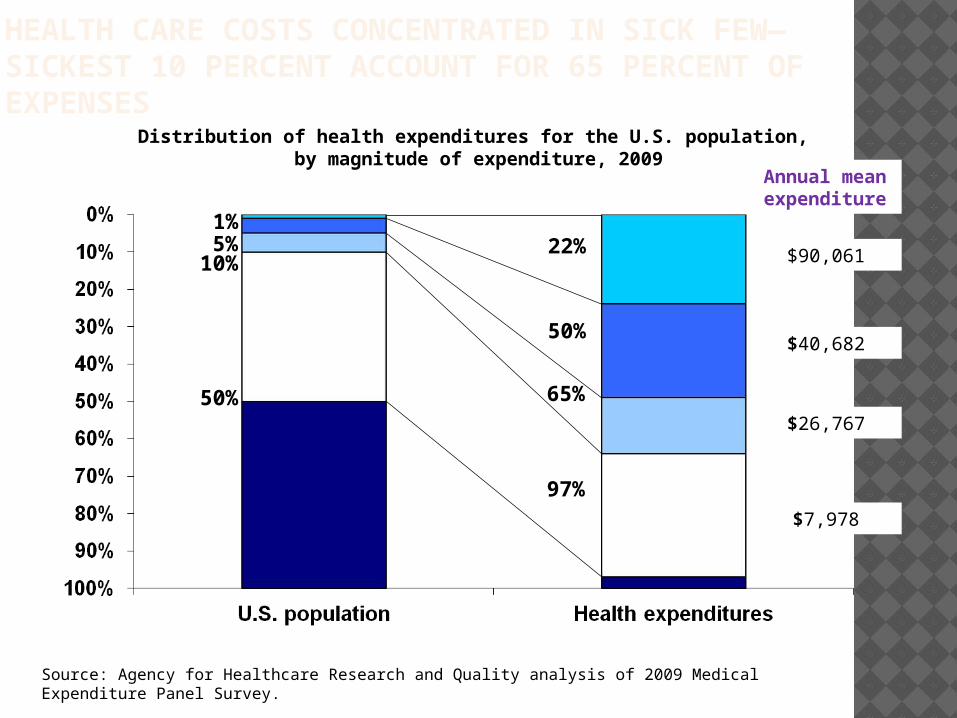
HEALTH CARE COSTS CONCENTRATED IN SICK FEW—SICKEST 10 PERCENT ACCOUNT FOR 65 PERCENT OF EXPENSES
Source: Agency for Healthcare Research and Quality analysis of 2009 Medical Expenditure Panel Survey.
Distribution of health expenditures for the U.S. population, by magnitude of expenditure, 2009
1%5%
10%
50%
65%
22%
50%
97%
$90,061
$40,682
$26,767
$7,978
Annual mean expenditure
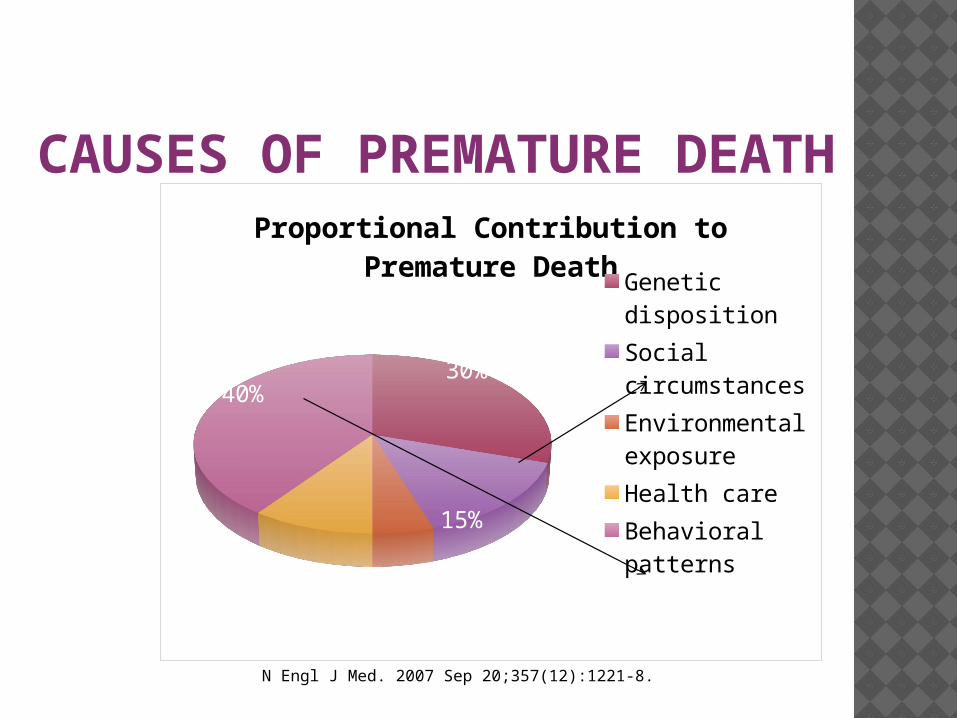
CAUSES OF PREMATURE DEATH
N Engl J Med. 2007 Sep 20;357(12):1221-8.
30%
15%
5%10%
40%
Proportional Contribution to Premature Death
Genetic disposi-tionSocial cir-cumstancesEnvironmental exposureHealth careBehavioral pat-terns
SOLUTION
Applying the Chronic Care Model in Integrated Practice Developing an Informed, Activated
Patient Using Information Technology Developing a Prepared, Proactive Practice
Teams Re-Organizing Healthcare System to
Include SUD Treatment, Prevention, Health and Wellness
INTEGRATING SUD WITH MH AND PRIMARY CARE Pre-Reform = special pilot programs and
grant-funded initiatives Post-Reform = Chronic Care Model,
Triple Aim, Accountable Care Organizations, Patient-Centered Medical Homes, and Health Homes Integration via ConsolidationDe-Institutionalization and focus on
community-based carePrimary Care locus and “medicalization”Reimbursement reforms and shared risk
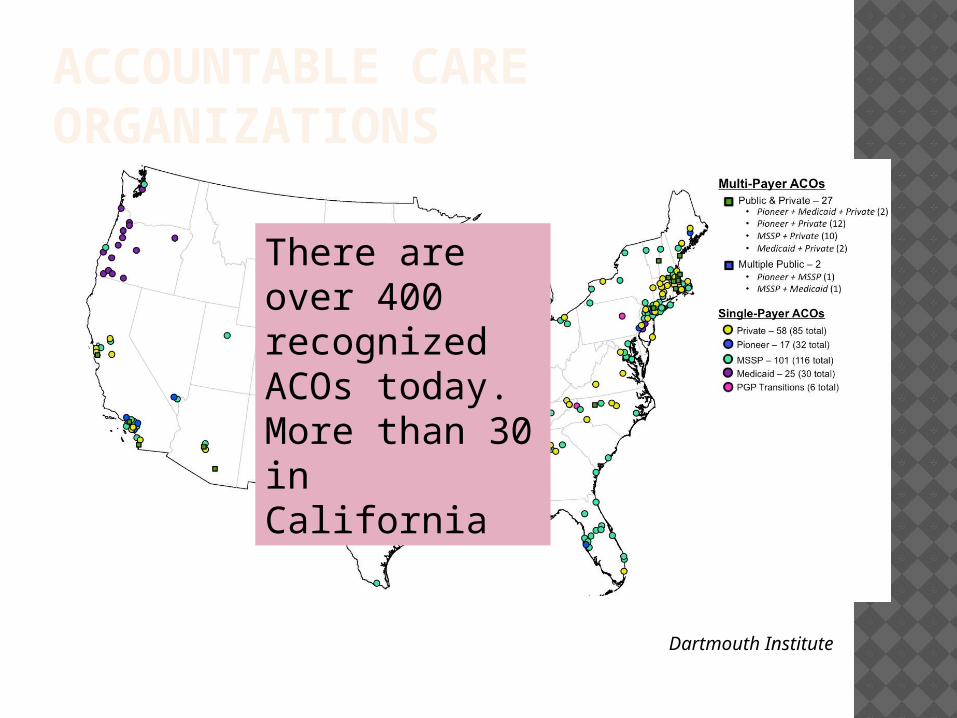
ACCOUNTABLE CARE ORGANIZATIONS
Dartmouth Institute
There are over 400 recognized ACOs today. More than 30 in California
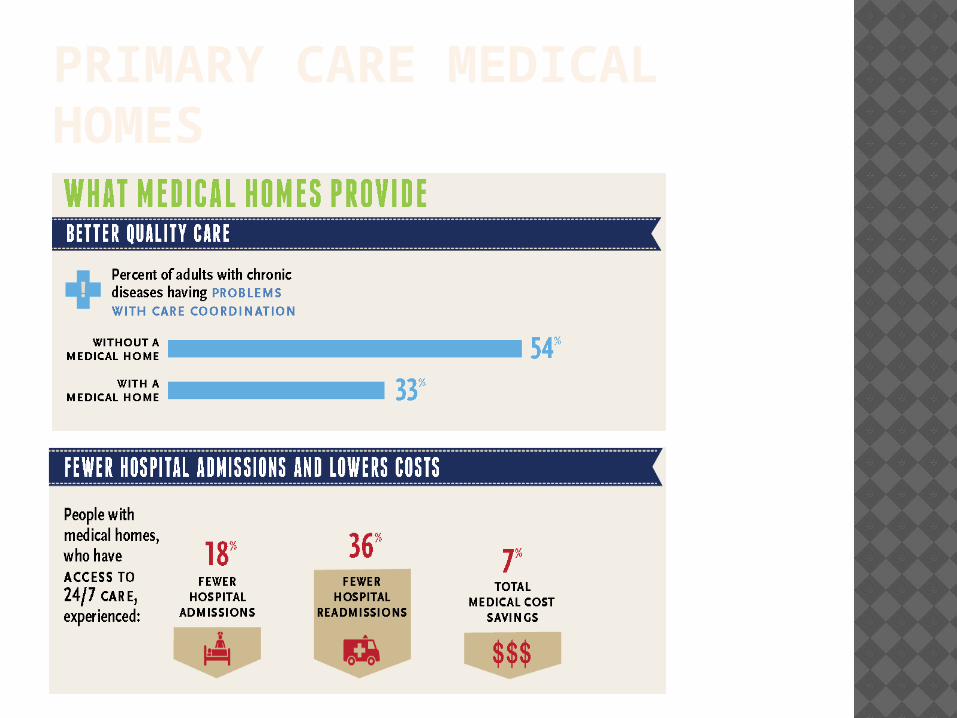
PRIMARY CARE MEDICAL HOMES
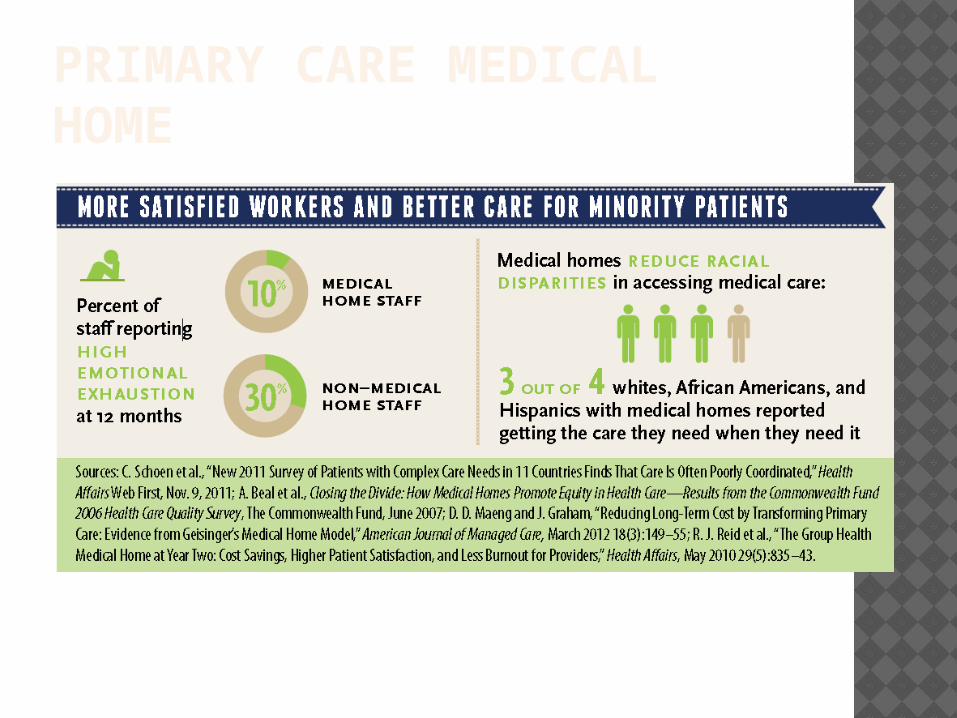
PRIMARY CARE MEDICAL HOME
INTEGRATION: BEHAVIORAL MEDICINE“the field concerned with the development of behavioral science knowledge and techniques relevant to the understanding of physical health and illness and the application of this knowledge and techniques to prevention, diagnosis, treatment, and rehabilitation”
Yale Conference on Behavioral Medicine
SUPPORT FOR INTEGRATED MODELS One study showed that medical costs of patients with
chronic diseases reduced by 20% if these patients received behavioral health interventions, but increased by 17% to 27% if they were treated in traditional office settings
Another study of non-diabetic patients showed that lifestyle (behavioral) changes reduced the incidence of diabetes by 58% compared to patients who received the placebo therapy
One analysis of 91 studies showed that medical utilization decreased by an average of 15.7% over baseline following behavioral intervention, compared with an increase of 12.3% without behavioral intervention, and thus yielded an overall 28% cost return

BEHAVIORAL MEDICINE TARGETS
Adolescent HealthAgingArthritisAsthmaCancerCardiovascular
Disease (heart disease, hypertension, stroke),
Children's HealthChronic PainCystic Fibrosis
DepressionDiabetesEating Disorders HIV/AIDS Obesity Pulmonary Disease Substance Use
Disorders including Smoking Cessation
Women's Health
KEY STRATEGIESLifestyle Changes Improve nutrition, increase physical activity, stop smoking, use medications appropriately, practice safer sex, prevent and reduce alcohol and drug abuse.
Training Coping, relaxation, self-monitoring, stress management, time management, pain management, problem-solving, communication skills, time management, priority-setting.
Social Support Group education, caretaker support and training, health counseling, community-based sports events
KEY STRATEGIES Integrating behavioral medicine
strategies into primary care and managed care;
Increasing public awareness of behavioral interventions;
Including effective behavioral interventions in development of clinical practice guidelines;
Increasing use of information technology for behavioral interventions;
Improving integration of research and practice
WHY IS THIS IMPORTANT? Approximately one in four Americans has
MCC, including one in 15 children. Among Americans aged 65 years and older,
as many as three out of four persons have MCC. In addition, approximately two out of three Medicare beneficiaries have MCC.
People with MCC are also at increased risk for mortality and poorer day-to-day functioning.
MCC are associated with substantial health care costs in the United States. Approximately 66 percent of the total health care spending is associated with care for the over one in four Americans with MCC.
OBJECTIVESIdentify evidence‐supported models for persons with multiple chronic conditions to improve care coordination
Define appropriate health care outcomes for individuals with multiple chronic conditions
Develop payment reform and incentives
Implement and effectively use health information technology
Promote efforts to prevent the occurrence of new chronic conditions and to mitigate the consequences of existing conditions
Perform purposeful evaluation of models of care, incentives, and other health system interventions

OBJECTIVES
Facilitate self-care management
Facilitate home and community‐based services
Provide tools for medication management
Identify best practices and tools
Enhance health professionals’ training
Address multiple chronic conditions in guidelines
ELEMENTS OF INTEGRATED CARE
Integrated Services Integrated Teams Cross-functional Screenings/Assessments Integrated Treatment Planning Tools Cross-trained Practitioners Stage-wise Treatment Motivational Interventions Cognitive-Behavioral Treatment Integrated Medication Management Integrated Billing Integrated Outcomes and Quality
OTHER SETTINGS Community Mental Health Centers Federally-Qualified Health Centers Emergency Departments Critical Access Hospitals (25 and fewer
beds) Rural Health Centers Primary Care Clinics/Community Health
Centers Public Health Correctional Facilities
SETTINGDistance
• Consult• Referral• Case
Management
Onsite
• Screening • Treatment• Case Mgmt.• Specialized
Services
Integrated
• Shared Care Plans• Coordinated Care/Case Mgmt.• Shared Infrastructure and Business
Model/Financials• Integrated satisfaction, quality and
outcomes measures
IMPLEMENTATION CONSIDERATIONS Networking and Affiliation Business Model and Marketing Material Agreements Revenue Share/financial model Reimbursement reforms Billing for Case Management/Care
Coordination
IMPLEMENTATION CONSIDERATIONS Knowledge barriers Stigma and cultural differences Privacy laws Willingness to collaborate and partner Access to capital Structure and governance Health IT infrastructure compatibility
EVIDENCE-BASED PRACTICES Integrate EBP into policies and
procedures Assess training needs Share tools and expertise across
boundaries Monitor and evaluate regularly Ensure services are culturally competent

THE SYSTEM OF CARE: GOALS & OBJECTIVESGOAL 1:Improve the Coordination of Behavioral Health Services with Primary Care and Supportive Services and Maximize the Use of Available Resources to Effectively Address Behavioral Healthcare Needs by Reducing Fragmentation and Ensuring a Full Spectrum of Care
Source: Taking Integration to the Next Level: The Role of New Service Delivery Models in Behavioral Health. 2012 - Cornerstones for Behavioral Healthcare Resource Series. Joel E. Miller, Senior Director of Policy and Healthcare Reform National Association of State Mental Health Program Directors (NASMHPD)
OBJECTIVES Accelerate the necessary linkages between
physical health care and behavioral health services to promote and achieve recovery for people with mental illnesses and/or substance abuse who also have chronic physical diseases.
Provide content expertise in the development and implementation of behavioral health aspects of service delivery system reforms such as medical homes, health homes and accountable care organizations, and related payment initiatives such as bundling and capitation.
OBJECTIVES Accelerate the necessary linkages between
behavioral healthcare services and the array of supportive services (supported housing, employment, transportation, education and training, etc.)
Develop and implement effective behavioral health promotion, wellness and prevention activities.
Provide content expertise on the development of and inclusion of behavioral health quality measures in specifications for electronic health records, in the development of health information exchanges, and in public and private sector initiatives to improve the quality of behavioral healthcare.
OBJECTIVES Provide leadership to health providers, federal and
state policymakers and officials, national medical societies, including primary care organizations, to ensure the adequacy of providers in the behavioral health workforce to deliver quality behavioral health care services.
Empower consumers to maximize control of their recovery through new and emerging ways to design, apply and organize existing treatments and by finding new platforms and avenues to deliver new treatments.
Provide content expertise on benefits and scope and requirements for behavioral health services – in partnership with state insurance authorities – that are offered in public and private health insurance plans operating in the state.
OBJECTIVES Actively ensure the outreach and
enrollment of individuals with mental and substance use disorders so they may receive and maintain health coverage based on their eligibility and are able to easily access care.
CONDUCTING YOUR ENVIRONMENTAL
SCAN
Source: Mady Chalk, TRI
ACCOUNTABILITY Environment:
Major focus on medical home in primary care setting
Pressure to implement EHRsField still struggling with hand-offs and
transitions between levels of care/agencies
Co-morbidity (MH/SA and MED/SA) issues are still befuddling payers and providers
PATIENT/FAMILY ROLE
Environment:Focus on patient centered care Increase pressure on offering choice of
providerNew eligibles—different age/socio-
economic group—maybe more vocal about their treatment and treatment options
PERFORMANCE EXPECTATIONS
EnvironmentImplementing National Quality Forum
(NQF) Standards of CareDecreasing drop-outs/increasing
engagement, retention, and continuing care
Increasing use of medications as part of comprehensive treatment
Continuous monitoring during treatment and use of data to adapt treatment services during treatment
SUD ROLE IN HEALTH CARE Environment:
Increase access to treatment through FQHCs
SBIRT is both an NQF Standard and consider important to provide in healthcare settings
Medi-Cal authorities’ decision-making process about changes in benefits, providers, services and reimbursement
Pressures by health plans to have credentialed practitioners deliver services
Linking health and specialty care is considered critical
ACCESS Environment:
Access is still a premium to payersStill defined in fairly traditional termsMedi-Cal, payers, managed care
organizations and the Department of Insurance will be tracking access for newly eligible patients more closely
Assumes new coverage = new or different utilization patterns and services
VALUE/COST
Environment: Identification of services/practices that add
valueProof or evidence to support purchasing
decisionsPayers more likely to define value in terms of
savings or offsets—not necessarily on improved health outcomes
Will have to show value to the customer who will have some “skin” in the game (deductibles, co-pays)
INTEGRATION
Environment:Developing standards for integrated careProviders are further along than payersAssumption that carve-ins will get you
closer to integrationReimbursement rules don’t necessarily
encourage integration at the practice level
Still focusing on differences versus similarities
Public payer silos continue to thwart integration
WORKFORCE
Environment:Payers equate a credentialed workforce with
quality although a significant portion of workforce is not credentialed
All over the map regarding a definition of competency (versus credentialed)
Good supervision is diverted by productivity expectations and reimbursement
Recovery support providers have momentum and creating formal networks to compete for dollars
ROLE OF TECHNOLOGY IN DELIVERY
Environment:Technology is moving faster than practiceThere are simple uses of technology to
enhance access (texting reminders)Investment in technology in the provider
community is spotty
TREATMENT INTERVENTIONS
Environment:Interventions should produce value and
we have evidence of what worksPressures exist to keep buying the “same
old”Payers don’t yet fully embrace newer
interventions – this is an “educated sale”We aren’t good at the “elevator speech”
in describing interventions
REIMBURSEMENT
Environment:Continued focus by payers on purchasing
units of services, some initial discussion re: purchasing episodes of care versus widgets
Providing integrated treatment made difficult by outdated reimbursement rules that preclude billing two services on same day from same address
Pay for performance strategies not widely used yet in SUD
Different payers/different rates/same services
NEXT STEPS Conduct Local Market Research Conduct Your Own Environmental Scan Develop Business Model/Integration
Model Begin Networking with Primary
Care/Settings Prepare Internally:
Board on boardStaff trained and ready to meet
requirements Infrastructure assessed and deployed
(staffing, EBPs, Tools, IT, etc.)Ready for new reimbursement, quality and
outcomes models, methods and measures
THANK YOU – QUESTIONS?Contact:Patrick GauthierDirectorAHP Healthcare [email protected]