Embed Size (px)
Citation preview
- 1 -
Protocol
Healthcare-associated infection surveillance
on intensive care units
© National Reference Center For Nosocomial Infection Surveillance
at the Institute for Hygiene and Environmental Medicine
Charité – University Medicine Berlin
www.nrz-hygiene.de
December 2012

- 2 -
Contact information: Nationales Referenzzentrum (NRZ) für Surveillance von nosokomialen Infektionen am Institut für Hygiene und Umweltmedizin (Institute director: Prof. Petra Gastmeier, MD) Charité - Universitätsmedizin Berlin gemeinsame Einrichtung von Freier Universität Berlin und Humboldt-Universität Berlin Hindenburgdamm 27 12203 Berlin, Germany Tel.: 049 30/ 8445 3680 Fax: 049 30/ 8445 3682 E-mail: [email protected] Homepage: www.nrz-hygiene.de

- 3 -
Table of Contents 1. Introduction ........................................................................................... 4 2. Goals of the surveillance protocol ........................................................ 5 3. Requirements for participation in ITS-KISS and the duties of KISS institutions ................................................................................................ 6 4. Methods of HAI surveillance ................................................................. 7
4.1 Methods for ICUs .......................................................................................................... 7 4.2 Surveillance process .................................................................................................... 7 4.3 Infection rate comparison .......................................................................................... 15
5. Documentation specifications ............................................................. 16
5.1. Electronic surveillance data entry ........................................................................... 16 5.2 Surveillance plan: Object and components of surveillance .................................. 16 5.3 Data collection on ICUs ............................................................................................. 17 5.3 Monthly forms for ICUs .............................................................................................. 22 5.5 Pathogen codes .......................................................................................................... 24
6. References ......................................................................................... 26 7. Appendix ............................................................................................ 27
7.1 Monthly data chart for KISS ICUs ............................................................................ 27 7.2 Example monthly data form for ICUs ....................................................................... 28 7.3. Infection data collection form for ICUs ................................................................... 29
8. Legal Notice ....................................................................................... 30

- 4 -
1. Introduction The KISS module ITS-KISS enables intensive care units in Germany to perform surveillance of patients with multidrug-resistant drug organisms (MDRO) or Clostridium difficile-associated diarrhea (CDAD), and/or surveillance of patients with healthcare-associated infections (HAI). This protocol includes all specifications for surveillance of HAI on ICUs participating in ITS-KISS. The specifications for surveillances of MDRO and CDAD are in the protocol “Surveillance of patients with multidrug-resistant organisms and/or Clostridium difficile-associated diarrhea”, which can be found on the NRZ web site. ITS-KISS module: Patients in intensive care units (ICUs) have an increased risk of acquiring healthcare-associated infections because they are subject to invasive procedures more frequently than other patients and often already have severe illnesses. Since 1997, healthcare-associated infections have been recorded by an increasing number of ICUs in all of Germany through voluntary participation in KISS (KISS=Krankenhaus-Infektions-Surveillance-System), a hospital infection surveillance system run out of the National Reference Center for the Surveillance of Nosocomial Infections (Nationale Referenzzentrum= NRZ). Because of their frequency and severity, KISS surveillance on ICUs concentrates on lower respiratory infections (pneumonia and bronchitis), bloodstream infections (BSI), and urinary tract infections (UTI). When especially relevant for an ICU, ITS-KISS (Intensivstation = ITS= (eng.) ICU) can also be used for surveillance of external ventricular drainage-associated meningitis/ventriculitis. The use of devices (e.g., urinary tract catheters, central vascular catheters, invasive or non-invasive mechanical ventilation, or external ventricular drainage) is also taken into account during analysis as a risk factor for the development of healthcare-associated infections. Participating ICUs transfer their data to the NRZ, making an evaluation of device utilization rates and device-associated infection rates possible for each ICU. Moreover, the data of all ICUs for the last five-year period is summarized and made available as reference data for comparison. In addition, a stratification of rates according to the kind of ICU is undertaken in order to include the different kinds of underlying patient illness on different kinds of ICUs. In this way, important predisposing factors and risks related to exposure are taken into account. Differences between hospitals or over time can be important signs of problems that should be investigated more closely. When needed, surveillance of other healthcare-associated infections can be undertaken on the ICU.

- 5 -
2. Goals of the surveillance protocol This surveillance1 protocol should primarily provide participating hospitals with necessary definitions and specifications. These definitions are used for data collection and data analysis. Secondarily, it allows other, interested but non-participating hospitals to collect data with these definitions and specifications and then evaluate their data analogically. In this manner, hospitals can orient themselves by the reference data provided by the hospitals participating in the project. Definitions by the National Healthcare Safety Network (NHSN) system of the Centers for Disease Control and Prevention (CDC) in the USA were used as a basis for this protocol. This surveillance protocol is directed at interested hospital hygienists, infection control nurses, and physicians who want to take part in the surveillance project. All requests for further specifications and explanations are welcome.
1 Continuous, systematic collection, analysis and interpretation of health-related data necessary for planning, introducing and evaluating medical procedures, as well as the regular transfer of these data on those who need them.
- 6 -
3. Requirements for participation in ITS-KISS and the duties of KISS institutions Participating ICUs must fulfill the following requirements: • ICU heads must agree to the unit’s participation in the project • Infection control personnel must be involved (ICP are the most important contact
partners for KISS and are responsible for organizing surveillance on location. The involvement of a hospital hygienist is desired but not necessary.)
• Completion of an introductory course from the NRZ • Agreement to use CDC definitions for healthcare-associated infection diagnosis.
Treating physicians must be made aware of these definitions.
• Strict utilization of the obligatory specifications found in the surveillance protocol (Hospitals may, of course, record data that may be useful for quality management in addition to the data recommended by the NRZ)
• Surveillance of all three indicator infections (lower respiratory infections, BSI, UTI)
must be carried out, independent of device association (e.g., newly acquired pneumonia without associated mechanical ventilation must be recorded)
• Data collection and transfer via webKess • Preparedness to share descriptive parameters (structural and procedural
parameters of the ICU and the hospital, e.g. size of hospital) • Preparedness to complete internal quality assurance measures upon relevant
surveillance results • Participation in regular NRZ events for experience exchange • Preparedness to participate in validity procedures The institutions supporting KISS promise the participating hospitals: • To provide advice and expert support during surveillance • To handle data strictly confidentially • To enable participating hospitals to prepare data analyses • To advise them on the implementation of surveillance results for quality
management

- 7 -
4. Methods of HAI surveillance
The methods proposed by KISS have the primary goal of supporting internal quality assurance measures. Continuous, intensive contact between surveillance personnel and the doctors and nursing staff on the unit in question is very important. Equally crucial for the identification of patients with healthcare-associated infections is the regular examination of laboratory findings and patient charts on each unit. The less often laboratory testing is performed in a hospital, the more closely patient clinical symptoms must be paid attention to. Regular visitations and close contact to unit personnel are appropriate methods. CDC definitions for healthcare-associated infections are used for determining the presence of a healthcare-associated infection on an ICU (see www.nrz-hygiene.de).
4.1 Methods for ICUs
Surveillance in ITS-KISS always includes the following indicator infections: urinary tract infection (UTI), infections of the lower respiratory system (pneumonia and bronchitis) and laboratory-confirmed bloodstream infections (BSI) (clinical sepsis is included for children <1 year). These infections must always be documented when acquired on an ICU (i.e., the first symptoms appeared after admission) participating in KISS, whether or not devices were in use. Upon diagnosis of an indicator infection, device association in terms of time should be recorded. Upon the diagnosis of a urinary tract infection, indwelling catheter association should be investigated; mechanical ventilation should be checked for in the case of a lower respiratory infection; and central vascular catheter association should be checked for in the case of BSI. ICUs participating in ITS-KISS can optionally expand their surveillance of respiratory infections by including non-invasive ventilation with the surveillance module “non-invasive ventilation.” Similarly, external ventricular drainage (EVD)-associated meningitis/ventriculitis can be included as a further kind of infection with the surveillance module “EVD-associated meningitis.” Furthermore, surveillance for other healthcare-associated infections (e.g., infected decubital ulcers, etc.) can be carried out for internal quality management. The frequency of these other infections for each station is calculated as incidence density. Because of the lack of an appropriate standardization procedure, KISS does not prepare reference data for comparison with other ICUs for these other infections or for indicator infections not associated with devices.
4.2 Surveillance process
Surveillance takes place monthly. The following data are recorded daily and put onto the monthly data form for ICUs (see Appendix 8.1, 8.2). (We recommend using “midnight statistics” in order to avoid including patients who are only on the ICU for observation for a few hours):
The following data must be recorded:

- 8 -
1. Number of all newly admitted patients. (All patients admitted to the unit in the last 24h are counted for this figure, including those who are no longer present at the time of counting and may have only been on-unit for a few hours.)
2. Number of all patients on one day (at a certain time, e.g. midnight)
3. Number of patents with a transurethral urinary catheter (UC) at midnight 4. Number of patients with central vascular catheters (CVC) (only one CVC is
counted in patients with more than one CVC) at midnight
5. Number of patients with invasive mechanical ventilation via intubation or tracheostoma (INV) at midnight
When the optional surveillance modules “non-invasive ventilation” and/or “EVD-associated meningitis” have been chosen, the following data are included in KISS:
6. Number of patients with mechanical, non-invasive ventilation (NIV) for at least 6h in the last 24h. In the event that patients meet the definitions for non-invasive ventilation as well as invasive ventilation, then only the invasive ventilation is counted.
7. Number of patients with external ventricular drainage (EVD)
Example A unit has eight beds. On June 10, seven patients were on the ICU at midnight. On June 11, five of these patients are transferred and four more are newly admitted. One of the new patients has a CVC and a UC and is ventilated for two hours. This patient is transferred during the night to a non-intensive care unit after eight hours. At midnight the data for June 11 for the monthly data list are recorded as follows:
• Total newly admitted patients: 4 • Total patients at midnight: 5 • Total patients with UC (=of the five patients present at midnight, all five have a UC; the UC of
the patient already transferred is not included): 5 • Total patients with CVC (=of the five patients present at midnight, four have a CVC; the CVC
of the patient already transferred is not included) :4 • Patients with ventilation (=of the five patients present at midnight, two are still being ventilated
at midnight, the ventilation of the patient already transferred is not included): 2 At the end of the month, all five (or six, or seven) data sets are summed up individually to provide a monthly total of newly admitted patients, monthly total patient days, all UC, CVC, and INV days, and all NIV or EVD days, if these devices are under surveillance. • All patients who were on the ICU on the first day of the month and those who
came during the month should be observed for healthcare-associated infection. • If a patient develops a healthcare-associated infection on the ICU, or is infected
with or colonized by a multidrug-resistant pathogen while on the unit, further data must be collected. (See infection data collection form for ICUs 8.3, and the multidrug resistant pathogen case form, 8.4).

- 9 -
• A healthcare-associated infection has to have been acquired on the unit in order to be counted as an infection for that unit. In other words, the infection was not present or incubating at admission.
• Colonization or infection by multidrug-resistant pathogens should be included in
surveillance of those pathogens, even if they were present before admission.
The following rates are calculated for data evaluation: • Device utilization rates The device utilization rate describes the percentage of patient-days on which a certain device was present, and is calculated as the quotient of the total of device days and the total number of a unit’s patient days multiplied by 100. The following rates are always calculated: Total UC days UC utilization rate = ───────── x 100 Total patient days Total CVC days CVC utilization rate = ───────── x 100 Total patient days INV utilization rate Total number of ventilation days by intubation or tracheostoma for ventilation by = ─────────────────────────────────────X 100 intubation or Total patient days tracheostoma When chosen as surveillance modules within ITS-KISS by surveillance personnel, the following rates are also calculated: Total NIV days NIV utilization rate = ───────── x 100 Total patient days Total EVD days EVD utilization rate = ────────── x 100 Total patient days
- 10 -
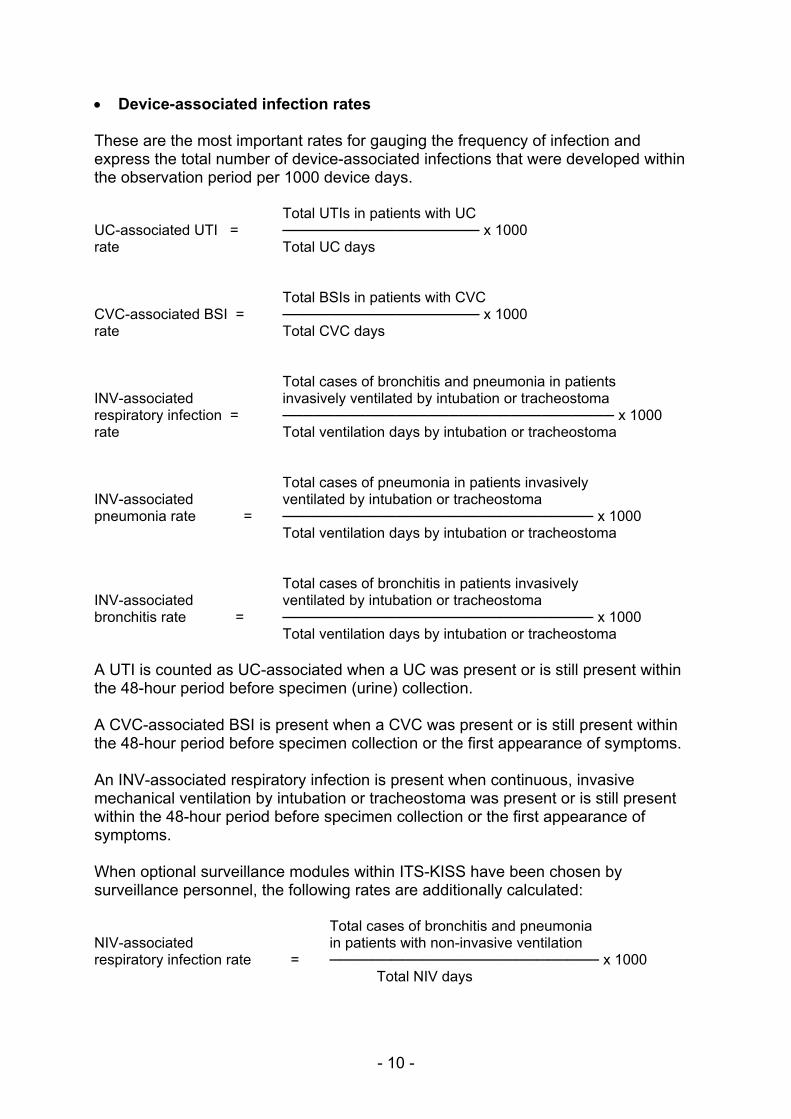
• Device-associated infection rates These are the most important rates for gauging the frequency of infection and express the total number of device-associated infections that were developed within the observation period per 1000 device days. Total UTIs in patients with UC UC-associated UTI = ─────────────────── x 1000 rate Total UC days Total BSIs in patients with CVC CVC-associated BSI = ─────────────────── x 1000 rate Total CVC days Total cases of bronchitis and pneumonia in patients INV-associated invasively ventilated by intubation or tracheostoma respiratory infection = ──────────────────────────────── x 1000 rate Total ventilation days by intubation or tracheostoma Total cases of pneumonia in patients invasively INV-associated ventilated by intubation or tracheostoma pneumonia rate = ────────────────────────────── x 1000 Total ventilation days by intubation or tracheostoma Total cases of bronchitis in patients invasively INV-associated ventilated by intubation or tracheostoma bronchitis rate = ────────────────────────────── x 1000 Total ventilation days by intubation or tracheostoma A UTI is counted as UC-associated when a UC was present or is still present within the 48-hour period before specimen (urine) collection. A CVC-associated BSI is present when a CVC was present or is still present within the 48-hour period before specimen collection or the first appearance of symptoms. An INV-associated respiratory infection is present when continuous, invasive mechanical ventilation by intubation or tracheostoma was present or is still present within the 48-hour period before specimen collection or the first appearance of symptoms. When optional surveillance modules within ITS-KISS have been chosen by surveillance personnel, the following rates are additionally calculated: Total cases of bronchitis and pneumonia NIV-associated in patients with non-invasive ventilation respiratory infection rate = ────────────────────────── x 1000 Total NIV days

- 11 -
Total cases of pneumonia NIV-associated in patients with non-invasive ventilation pneumonia rate = ────────────────────────── x 1000 Total NIV days Total cases of bronchitis NIV-associated in patients with non-invasive ventilation bronchitis rate = ────────────────────────── x 1000 Total NIV days Total cases of meningitis/ventriculitis EVD-associated in patients with EVD meningitis rate = ────────────────────────── x 1000 Total EVD days Bronchitis or pneumonia is NIV-associated when the patient was non-invasively mechanically ventilated within the 48-hour period before the first symptoms or signs or specimen collection. If the patient was mechanically ventilated non-invasively and invasively within the 48-hour period before the first signs and symptoms, then the bronchitis/pneumonia should be counted as INV-associated. EVD-associated meningitis/ventriculitis was or is still present when EVD was present within the 48-hour period before the first appearance of symptoms or specimen collection. • Incidence density of healthcare-associated indicator infections (total
device-associated and not device-associated infections) and other healthcare-associated infections
Incidence density represents the frequency of healthcare-associated infections per 1000 patient days. It is an estimation of the probability that a patient will acquire a healthcare-associated infection while being treated in-patient. The most important risk factor, device use, is not taken into account in incidence density. For this reason, incidence densities are not appropriate for comparison between ICUs, and are better suited for showing trends over time on a single unit. Moreover, it provides a figure for healthcare-associated infection frequency per 1000 patient days on a single unit. “Other” infections Total non-indicator healthcare-associated infections incidence density = ───────────────────────── x 1000 Total patient days Total (device and not device associated) UTI UTI incidence density = ───────────────────────── x 1000 Total patient days Total (device and not-device associated) BSI BSI incidence density = ───────────────────────── x 1000 Total patient days

- 12 -
Total (device-associated and not-device Respiratory infection associated) respiratory infections incidence density = ───────────────────────── x 1000 Total patient days Total (device-associated and not-device associated) cases of meningitis Meningitis incidence density = ───────────────────────── x 1000 Total patient days

- 13 -
Example calculation: In this example calculation, the optional modules “NIV-associated respiratory infections” and “EVD-associated meningitis” have been selected in addition to the three indicator infections. Other healthcare-associated infections were also recorded. Known: Total UTI 3 Of those UC-assoc. UTI 2 Total BSI 1 Of those CVC-assoc. BSI 1 Total pneumonia 1 Of those INV-assoc. pneumonia 1 Of those NIV-assoc. pneumonia 0 Total bronchitis 2 Of those INV-assoc. bronchitis 1 Of those NIV-assoc. bronchitis 1 Total meningitis 1 Of those EVD-assoc. meningitis 1 Total other infections 1 (arterial or venous infection F1) As well as the data from the example monthly data form (see 7.2) Unknown: all descriptive rates
Calculation:
• Device utilization rates Interpretation
UC utilization rate =(216/240) x 100 = 90 90 UC days per 100 patient days CVC utilization rate =(200/240) x 100 = 83 83 CVC days per 100 patient
days INV utilization rate =(80/240) x 100 = 33 33 INV days per 100 patient
days Rates for optional surveillance modules “non-invasive ventilation” and/or “EVD-associated meningitis”
NIV utilization rate =(40/240) x 100 = 17 17 NIV days per 100 patient
days EVD utilization rate =(30/240) x 100 = 12.5 12.5 EVD days per 100 patient
days • Device-assoc. infection rates
UC-assoc. UTI rate =(2/216) x 1000 = 9.2 9.2 UC-assoc. UTI per 1000
UC days

- 14 -
CVC-assoc. BSI rate =(1/ 200) x 1000 = 5.0 5 CVC-assoc. BSI per 1000 CVC days
INV-assoc. respiratory infection rate
=(2/80) x 1000 = 25 25 INV-assoc. respiratory infections per 1000 INV days
INV-assoc. pneumonia rate =(1/80) x 1000 = 12.5 12.5 INV-assoc. pneumonia
per 1000 INV days INV-assoc. bronchitis rate =(1/80) x 1000 = 12.5 12.5 INV-assoc. bronchitis
per 1000 INV days Rates for optional surveillance module “non-invasive ventilation”
NIV-assoc. respiratory infections rate
=(1/40) x 1000 = 25 25 NIV-assoc. respiratory infections per 1000 NIV days
NIV-assoc. pneumonia rate =(0/40) x 1000 = 0 Zero NIV-assoc. pneumonia
per 1000 NIV days NIV-assoc. bronchitis rate =(1/40) x 1000 = 25 25 NIV-assoc. bronchitis
per 1000 NIV days Rates for optional surveillance module “EVD-assoc. meningitis”
EVD-assoc. meningitis =(1/30) x 1000 = 33.3 33.3 EVD-assoc. meningitis
per 1000 EVD days • Incidence density
Incidence density for other infections
=(1/240’) x 1000 = 4.2 4.2 other infections per 1000 patient days
Incidence density for respiratory infections
=(3/240) x 1000 = 12.5 12.5 respiratory infections per 1000 patient days
Incidence density for UCI = (3/240) x 1000 = 12.5 12.5 UCI per 1000 patient
days Incidence density for meningitis
=(1/240) x 1000 = 4.2 4.2 meningitis cases per 1000 patient days
Incidence density for BSI =(1/240) x 1000 = 4.2 4.2 BSI per 1000 patient
days

- 15 -
4.3 Infection rate comparison • Evaluations for device utilization rates, device-associated infection rates,
incidence densities and multidrug-resistant pathogen rates can be prepared for participating ICUs.
• In addition, the rates of all ICUs (not including incidence density) are summarized over the entire period and made available as reference data. The mean as well as the 25% quartile, median and 75% quartile are given in these figures. (The 25% quartile is the value for utilization and infection rates under which 25% of ICUs lie. The median and 75% quartile are those values under which 50% or 75% of ICUs lie, respectively.) In addition to being standardized, the rates are stratified by type of ICU in order to take the patients’ underlying illnesses into account. When significant predisposing and treatment-related risk factors are taken into account, differences between hospitals or over time can become clear that should be investigated more closely.

- 16 -
5. Documentation specifications 5.1. Electronic surveillance data entry The NRZ has made an electronic system for data entry available for KISS participants. webKess can be accessed under www.webkess.de. webKess makes the collection of surveillance data possible and can be used by any participant to evaluate their data at any time. In order to guarantee that the calculation of reference data includes the most current data, KISS participants are required to complete their surveillance data entry within the four weeks after the end of each calendar year data collection period. In the event that webKess is unavailable because of technical difficulties, the data collection forms included in this protocol should be used for the period in question. The data must be entered into webKess as soon as it is running again.
5.2 Surveillance plan: Object and components of surveillance
Surveillance takes place monthly in ITS-KISS and it is possible to not perform surveillance some months out of the year and still participate in ITS-KISS. The specification of surveillance months and surveillance components is referred to as the “surveillance plan” in ITS-KISS. At the beginning of a new calendar year, ITS participants specify in which months surveillance will take place. In webKess, participants select for each month at the beginning of each year:
• Object of surveillance: HAI and/or MDRO • If HAI surveillance: which optional components, if any • Surveillance for the entire year or with interruptions
The surveillance plan has an effect on the evaluation and accuracy of an individual unit’s data, the selection of data for the creation of reference data, and also whether a unit will achieve a certificate or not. More details on the required length of surveillance to receive a certificate for ITS participation are on the NRZ website.

- 17 -
5.3 Data collection on ICUs If a patient acquires a healthcare-associated infection as defined by the CDC while being treated on an ICU, then certain data must be collected about the infection. An infection control professional or other person trained in the use of CDC definitions should be responsible for infection data collection. (Example infection data collection forms are attached). KISS participants enter the data into a system provided by the NRZ (webKess). The following information must be provided.
Master data
Hospital An abbreviation will be provided by the NRZ.
ICU An abbreviation will be provided by the NRZ.
Type of ICU Select the appropriate type of ICU. ICUs are not classified by the department heading the ICU, but rather by the treatment of the majority of patients. If patients are mostly treated surgically, choose “surgical” (even when the surgeries come from different departments, e.g. gynecology, general medicine or ENT). If most patients are treated medically (i.e., non-surgically), then chose “medical.” If equal numbers of patients are treated medically and surgically, choose “interdisciplinary.” Choose “neurosurgical,” “pediatric” or another option as appropriate. A recent addition is “burn trauma.” For those ICUs or burn trauma centers with a majority of burn patients, select “burn trauma.” If another type of ICU has a number of beds reserved only for burn victims, it is possible to complete surveillance separately for the two types of ICU, as if there were two separate ICUs. This separation must be permanent; a transfer from a burn-bed to a non-burn bed counts as a transfer from one unit to another. ICUs that do not fit in a given scheme should choose “other.”
Infection data
Date of admission Day, month and year of patient admission to unit.
Sex Male or female.

- 18 -
Year of birth Patient birth year.
Date of infection Day, month and year on which the first clinical evidence of infection was present, or the date on which the sample was taken that lead to diagnosis, whichever was earlier.
Urinary tract infection (UTI)
Select D1a-c= symptomatic UTI; D2= asymptomatic bacteriruia with secondary BSI; D3= other infections of the urinary tract (see CDC definitions)
Urinary catheter (UC) (=UC-associated)
Select only for patients with UC. Select if a UC (transurethral indwelling catheter) was present within the 48h period before specimen collection. There is no minimum amount of time for which the UC had to be present. Intermittent catheterization is not included in device-association.
Respiratory infections Pneumonia (C1a, C1b, C1c, C1d), bronchitis/tracheobronchitis, tracheitis (J1), other infection of the lower respiratory tract (J2). Choose infection based on CDC definitions.
Mechanical ventilation Select only for patients with a respiratory infection.
Invasive ventilation by intubation or tracheostoma (=INV-associated)
Select if a patient was continuously ventilated by endotracheal intubation or tracheostoma in the 48h period before specimen collection or the first appearance of symptoms. There is no minimum duration for which the patient had to be invasively ventilated. Invasive ventilation is defined as mechanical, positive-pressure ventilation of a patient (controlled, assisted or in pressure support mode) at various levels of pressures in inspiration and expiration by endotracheal intubation or tracheostoma. Note to CPAP: The sole utilization of continuous positive airway pressure (CPAP) is NOT mechanical ventilation and should not be recorded as ventilation. If the time interval between removal of the device and infection acquisition is more than 48h, then compelling reasons must be present to consider the infection device-associated.
Optional fields for surveillance module “non-invasive ventilation”
Non-invasive ventilation-association (=NIV-associated)
Pneumonia is NIV-associated when the patient was continuously or discontinuously non-invasively ventilated for at least 6h within the 48h period before the first
- 19 -
symptoms or specimen collection. Non-invasive ventilation is defined as mechanical, positive-pressure (controlled, assisted or in pressure support mode) ventilation at various levels of pressure in inspiration and expiration over a mask system (mouth piece or nasal, face or helmet mask) without the simultaneous presence of endotracheal intubation. A note on CPAP: The sole use of continuous positive airway pressure (CPAP) is NOT considered mechanical ventilation and should not be recorded as ventilation. If a patient was ventilated noninvasively and invasively by intubation or tracheostoma (INV) within the 48h period before then first signs and symptoms, then the respiratory infection should be considered INV-associated. If the time interval between removal of the device and infection acquisition is more than 48h, or the patient was noninvasively ventilated for less than 6h, then compelling reasons must be present to consider the infection device-associated.
No ventilation Select if the patient was not mechanically ventilated by the invasive or non-invasive methods defined above during the 48h period before the first signs or symptoms, or if non-invasive ventilation was present but is not being included in surveillance.
Bloodstream infection (BSI)
Select either laboratory-confirmed bloodstream infection (B1) or clinically defined sepsis in children <12 months (B2). CDC definitions are to be used.
Central vascular catheter (CVC) and CVC association (=CVC-associated)
Select only for patients with BSI. Select if patients had a CVC for at least 12h during the 48h period before the start of infection. A CVC terminates at or close to the heart or in one of the great vessels. There is no minimum duration for which the CVC had to be present. If the period between device removal and infection appearance is greater than 48h, then the infection is only to be considered CVC-associated for compelling reasons. If the patient with BSI had both a CVC and a peripheral vascular catheter (PVC) and the infection is definitely related to the PVC, then select “no.”
Total parenteral nutrition
Select only for patients with BSI. Select “yes” if a patient received total parenteral nutrition in the 48h period before specimen collection or the appearance of the first symptoms.

- 20 -
Optional fields for the optional surveillance module “EVD-associated meningitis”
Meningitis/ ventriculitis
G2 (meningitis or ventriculitis) as per CDC definition
Ventricular drainage (=EVD-associated)
Select if external ventricular drainage was in use within the 48h period before specimen collection or the first appearance of symptoms. There is no minimum duration for which EVD had to be in use. External ventricular drainage consists of an external ventriculostomy for draining cerebrospinal fluid (CSF) or for intraventricular measurement via pressure probe in the ventricular system and measurement of intracranial pressure. Contact to CSF and CSF extraction is possible via intraventricular measurement. If the period between device removal and infection appearance is greater than 48h, then the infection is to be considered EVD-associated only for compelling reasons.
Other infections If other infections should be included in surveillance for internal quality management, use the CDC for those infections (for example, gastroenteritis, I1).
Other:
Secondary BSI Select when a secondary BSI appears as a complication to a documented healthcare-associated infection. A laboratory-confirmed (blood culture) BSI related to a healthcare-associated infection at another body site is to be recorded as a secondary BSI. For a secondary BSI, the proven pathogen and its antibiogram must coincide with the primary source of infection. For example, if a patient with a healthcare-associated UTI has a positive blood culture, and the pathogens and antibiogram are identical, then the infection should be recorded as UTI with secondary BSI. Secondary BSIs are not recorded alone.
Death of patient Select if the patient died during surveillance, independent of the cause of death.
Comments Information should be documented here that could be useful for internal quality management (e.g., special patient risk factors or outside environmental factors)

- 21 -
Laboratory
Proof of pathogen Select yes or no if an etiologically relevant pathogen has been proved present.
Pathogen 1/2/3/4 Give up to four etiologically relevant pathogens from the drop-down list.
Material Entry required only for respiratory infections. Give method by and the substance in which the pathogen was detected (sputum, bronchoalveolar lavage (BAL)/ protected specimen brush (PSB), blood, other)

- 22 -
5.3 Monthly forms for ICUs
Monthly data collection forms for ICUs are filled out ideally by ICU personnel. Six figures are recorded for every day at a set time (e. g., in the context of statistical measurements at midnight). These daily figures are summed together at the end of the month and at the end of the form as monthly totals for each column. (An example form is in the appendix). The following information is required, and documentation should always be filled out at the same time of day. Month/Year The month and year of the data
Total new admitted patients
Total patients admitted onto the ICU in the last 24h, including patients only admitted briefly that may not be present at the time of documentation
Total patients Total patients at the time of documentation, including patients that were admitted immediately before the time of documentation. Documentation should always be completed at the same time of day.
Total patients with: UC Total patients with indwelling urinary catheter
(transurethral only; suprapubic urinary diversions are not included) at time of documentation
CVC Total patients with central vascular catheter at the time of documentation (patients with two or more CVC are counted only once)
INV Total patients with invasive ventilation (INV) at the time of documentation INV=mechanical positive pressure ventilation (controlled, assisted or pressure support mode) at various levels of pressures for inspiration and expiration by endotracheal intubation or tracheostoma. Note to CPAP: The sole use of continuous, positive airway pressure (CPAP) is NOT considered mechanical ventilation and should NOT be recorded as ventilation.
Fields for optional surveillance modules
NIV Total patients with non-invasive ventilation (NIV) at the time of documentation. NIV= mechanical, positive pressure ventilation

- 23 -
(controlled, assisted or pressure support mode) at various levels of pressure for inspiration and expiration via mask systems (mouthpiece, nose, face and helmet mask) without the simultaneous presence of endotracheal intubation. A ventilator day with non-invasive ventilation is present when a patient was ventilated for at least 6h according to the above definition. It is unimportant if the ventilation occurred continuously or discontinuously. Only the total ventilation time via NIV is to be noted. Note to CPAP: The sole use of continuous, positive airway pressure (CPAP) is NOT considered ventilation and should not be recorded as ventilation.
EVD Total patients with external ventricular drainage at the time of documentation. External ventricular drainage consists of an external ventriculostomy for draining cerebrospinal fluid (CSF) or for intraventricular measurement via pressure probe in the ventricular system and measurement of intracranial pressure. Contact to CSF and CSF extraction is possible via intraventricular measurement. Not included are ventriculoperitoneal shunts, subdural or epidural measurements, or intraparenchymal measurements with pressure probes directly in brain tissue without contact to CFS.

- 24 -
5.5 Pathogen codes Up to four pathogens can be documented for a single infection. The following pathogens and pathogen groups are coded as follows. For technical reasons, the abbreviations have not been translated and may therefore seem unusually different from the pathogen name.
Pathogen Abbreviation
S. aureus SAU Coagulase-negative staphylococci KNS Streptococcus pyogenes (A-streptococci) STR_A Streptococcus pneumoniae (pneumococci) STR_P Enterococcus spp. ENT Haemophilus spp. HAE Corynebacterium spp. COR E. coli ECO Klebsiella spp. KLE Enterobacter spp. ENB Citrobacter spp. CIT Proteus spp. PRO Serratia spp. SER Other enterobacteria AEN P. aeruginosa PAE Burkholderia cepacia BCE Stenotrophomonas maltophilia STM Acinetobachter spp. ACI Bacteroides spp. BAC Legionella spp. LEG Clostridium difficile CDI Other Clostridium spp. ACS Other bacteria ANB C. albicans CAN Other Candida spp. ANC Aspergillus spp. ASP Other fungi ANP Viruses VIR Undifferentiated growth WOD
If SAU, ENT, ECO, KLE, ENB, PAE, STM or ACI meets the definitions below for multidrug resistance or special resistance, choose one of the following related abbreviations. Coding MDR pathogens must follow these specifications:
Pathogen Resistant to the
following antibiotic: Abbreviation
S. aureus Methicillin/Oxacillin MRSA E. faecium/E. faecalis Vancomycin VRE

- 25 -
E. coli* See chapter 5.4 for ESBL definition
ESBL_ECO
K. pneumoniae** See chapter 5.4 for ESBL definition
ESBL_KLE
Resistance to > 3 of the following antibiotics
A. baumanii Cotrimoxazol, chinolone, imipenem, amioglycoside
MACI
E. cloacae Broad-spectrum penicillins, imipenem, chinolone, aminglycoside, cotrimoxazol
MENB
E. coli* Third-generation cephalosporine, chinolone, imipenem
MECO
K. pneumoniae** Third-generation cephalosporine, chinolone, imipenem
MKLE
P. aeruginosa Piperacillin, ceftazidim, chinolone, aminoglycoside, imipenem
MPAE
S. maltophilia Cotrimoxazol, chinolone (resistance to two antiobiotics is meaningful in this case)
MSTM
*If E. coli is both ESBL-producing and multidrug-resistant, code it as ESBL_ECO. **If K. pneumoniae is ESBL-producing and multidrug-resistant, code it as ESBL_KLE.

- 26 -
6. References
Emori TG, Culver DH, Horan TC et al. National Healthcare-associated Infections Surveillance (NNIS) System: Description of surveillance methods. Am J Infect Control 1991;19:19-35. The National Health care Safety Network (NHSN) Manual, Patient Safety Module Protocol, http://www.cdc.gov/nhsn/library.html#psc National Healthcare-associated Infections Surveillance System. Healthcare-associated infection rates for interhospital comparison: Limitations and possible solutions. Infect Control Hosp Epidemiol 1991;12:609-21. Horan TC, Emori TG. Definition of key terms used in the NNIS System. Am J Infect Control 1997; 25: 112-116. Geffers C, Koch J, Sohr D et al. Aufbau einer Referenzdatenbank für nosokomiale Infektionen auf Intensivstationen. Anaesthesist 2000; 49:732-737. Handbuch für die Surveillance von nosokomialen Infektionen (Schriftenreihe des Bundesministeriums für Gesundheit, Band 142, ISBN 3-7890-8088-8). A free copy in German can be requested from: Bundesministerium für Gesundheit, Postfach, 53108 Bonn. Definitionen nosokomialer Infektionen (CDC-Definitionen) Available for download in German from the NRZ web site: (www.nrz-hygiene.de). See also for relevant links to CDC/NHSN web sites.

- 27 -
7. Appendix The following forms can be used for internal data collection. Data transfer to the NRZ, however, always takes place electronically. 7.1 Monthly data chart for KISS ICUs Hospital: ________________________________ Month/ Year: _________________ ICU: ______________________________ Kind of ICU: _______________________
Day Total newly
admitted patients
Total patients
Total number of patients with:
UC CVC INV* NIV** EVD***
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 ∑
Total: patients patient days UC days CVC days INV days NIV days EVD days *INV= continuous invasive mechanical ventilation via intubation/tracheostoma **NIV=noninvasive ventilation, ***EVD=external ventricular drainage

- 28 -
7.2 Example monthly data form for ICUs Hospital: ______AAA_______________________ Month/ Year: XX/XXXX ICU: ______XY_____________________ Kind of ICU: ______internal medicine____
Day Total newly
admitted patients
Total patients
Total number of patients with:
UC CVC INV* NIV** EVD***
1 0 6 6 6 3 2 1 2 1 7 6 6 3 1 0 3 1 8 7 7 3 2 0 4 2 8 7 6 2 2 0 5 0 8 7 6 2 2 0 6 3 9 8 7 3 1 0 7 1 10 9 7 3 1 0 8 2 9 8 7 3 1 1 9 0 8 7 7 2 2 1 10 1 8 7 7 2 2 0 11 1 6 6 6 2 2 2 12 2 8 7 6 3 2 2 13 2 10 9 8 3 2 2 14 1 10 9 8 4 2 3 15 0 10 9 8 3 2 3 16 2 9 9 9 3 2 1 17 3 10 9 9 2 1 1 18 1 8 7 7 2 1 1 19 1 7 5 5 2 0 2 20 2 7 6 6 3 0 2 21 0 7 5 5 4 0 0 22 1 6 6 5 4 1 1 23 2 8 7 6 3 1 1 24 0 7 6 6 3 1 0 25 2 7 6 6 2 1 0 26 1 7 6 6 1 1 0 27 1 5 5 4 2 1 0 28 2 6 6 5 2 1 2 29 2 7 7 7 3 1 2 30 2 7 7 6 2 1 0 31 1 7 7 6 1 1 1 ∑ 40 240 216 200 80 40 30
Total: patients patient days UC days CVC days INV days NIV days EVD days *INV= continuous invasive mechanical ventilation via intubation/tracheostoma **NIV=noninvasive ventilation, ***EVD=external ventricular drainage

- 29 -
7.3. Infection data collection form for ICUs —ITS-KISS—
(Complete only for patients with healthcare-associated infections. Only one infection per form.) Hospital: ICU: Patient ID: Type of ICU: Admission date: Sex: f � m� Birth year:
INFECTION DATA Date of infection (Date of first symptoms): Urinary tract infection: SYMP (D1a-c)� ASYMP with sec. BSI (D2) � OTHER (D3)� Urinary catheter (within 48h before specimen collection): yes � no � Laboratory diagnosis (pathogen): Lower respiratory infection: pneumonia (C1a) � (C1b) � (C1c) � (C1d) � bronchitis/tracheobronchitis/tracheitis (J1) � Other respiratory infection (J2) � Mechanical ventilation (within 48h before start of infection): invasive via intubation/tracheostoma (INV) yes � non-invasive (NIV) yes � No ventilation within 48h prior to infection � Material: sputum � BAL/PSB � blood � other � Laboratory diagnosis (pathogen): Primary BSI: Laboratory-confirmed (B1)� clinical sepsis (B2) (only for children ≤12 months) � Central vascular catheter (e.g. CVC) (within 48h before start of infection): yes � no � Total parenteral nutrition (within 48h before start of infection): yes � no � Laboratory diagnosis (blood pathogen): Meningitis/Ventriculitis: (G2) � Laboratory diagnosis (pathogen): External ventricular drainage (EVD) (within 48h before start of infection): yes� no � Other infections: Laboratory diagnosis (pathogen):
COMPLICATIONS Secondary BSI: yes � no � Blood pathogen: Death: yes � no �
Comments

- 30 -
8. Legal Notice Nationales Referenzzentrum (NRZ) für Surveillance von nosokomialen Infektionen am Institut für Hygiene und Umweltmedizin (Director: Petra Gastmeier, MD), Charité-Universitätsmedizin Berlin gemeinsame Einrichtung von Freier Universität Berlin und Humboldt-Universität Berlin Hindenburgdamm 27 12203 Berlin, Germany Tel.: 049 30/8445 3680 Fax: 049 30/8445 3682 Partners: Prof. Markus Dettenkofer, MD am Institut für Umweltmedizin und Krankenhaushygiene (Director: Prof. V. Mersch-Sundermann, MD) Albert Ludwigs-Universität Freiburg Hugstetter Str. 55 79106 Freiburg, Germany Tel.: 049 761/270 8275 Fax: 049 761/270 8253 Robert Koch-Institut (RKI) Abteilung für Infektionskrankheiten, FG 14: Angewandte Infektions- und Krankenhaushygiene (Prof. Martin Mielke, MD) Nordufer 20 13353 Berlin, Germany Tel.: 049 30/4547 2233 Fax: 049 30/4547 2612 To contact NEO-KISS: Contact persons and their addresses are listed on the NRZ homepage (www.nrz-hygiene.de).