Embed Size (px)
Citation preview
Jaundice. Mr Daffodil - 57
Collapsed in the kitchen whilst doing the dishes
HPC
Neurological Causes:
- No headaches
- No Confusion
- No incontinence
- No Loss of Consciousness
- No vision or hearing changes
Chest/heart-No chest
pain- No
breathlessness
Metabolic: -Not a diabetic -Struggling to eat -Very obviously jaundiced
-Further three collapses of similar nature over the last week
-Felt slightly dizzy- legs felt shaky - Felt very tired following the episodes
HPC Contd. Severe loss of appetite
over a 4/5 week period Lost 1-2 stone over a 2
month period Itchy No nausea or vomiting No change in bowel
habits
Jaundice started 2/52 ago Before this – generally fit and well
Similar episode to this happened 7/8 years ago – collapsed several times but without jaundice. No cause found
Chesty cough for 3 weeks and chest infection
DDxJaundice Chronic alcoholic liver disease Gall Stones Pancreatic cancer, pancreatitis Hepatitis Hepatocellular carcinoma Cholangiocarcinoma, cholangitis
Collapse
Alcohol related collapse – alcohol withdrawal
Heart problem
Epilepsy
Management of chronic alcoholic
hepatitis Advise to stop drinking – look at AA forums
etc Provide withdrawal support –antabuse,
acamprosate Manage complications of portal
hypertension High nutrition diet – high fibre, high protein,
low fa Severe alcoholic hepatitis – corticosteroids
- reduce liver inflammation Transplant
Jaundice Derives from french word for yellow – jaune HYPERBILIRUBINAEMIA Total Bilirubin plasma concentrations rise in
all forms of jaundice and can collect in the extracellular fluid, causing skin and sclera to turn yellow
What happens normally?
How is bilirubin made? Bilirubin is a breakdown product of heme. Heme is
broken down into biliverdin by heme oxygenase, which is catalysed to bilirubin by biliverdin reductase. This bilirubin is UNCONJUGATED
Bilirubin is bound to albumin and travels to the liver
Once in the liver, bilirubin is CONJUGATED with gluronic acid by the enzyme glucuronyltransferase. This makes it water soluble

The Entero-hepatic circulation
The conjugated water soluble bilirubin is mainly excreted in bile with the bile salts.
It goes through the small intestine… until it reaches the terminal ileum
Most of the bile is reabsorbed at the terminal ileum (95%) What happens to the bilirubin left in the intestine?
Some conjugated bilirubin in the small intestine is catalysed back to unconjugated bilirubin, which is then further converted to urobilinogen. Any urobilinogen remaining in the small intestine is then converted to stercoblinogen. Stercobilinogen is oxidised to stercobilin.
Some urobilinogen is also reabsorbed. This enters the blood stream and is filtered by the kidneys. It is oxidised to urobilin, giving urine its yellow colour
What happens to the bilirubin that is absorbed? The cycle is repeated and generally it is resecreted in the bile


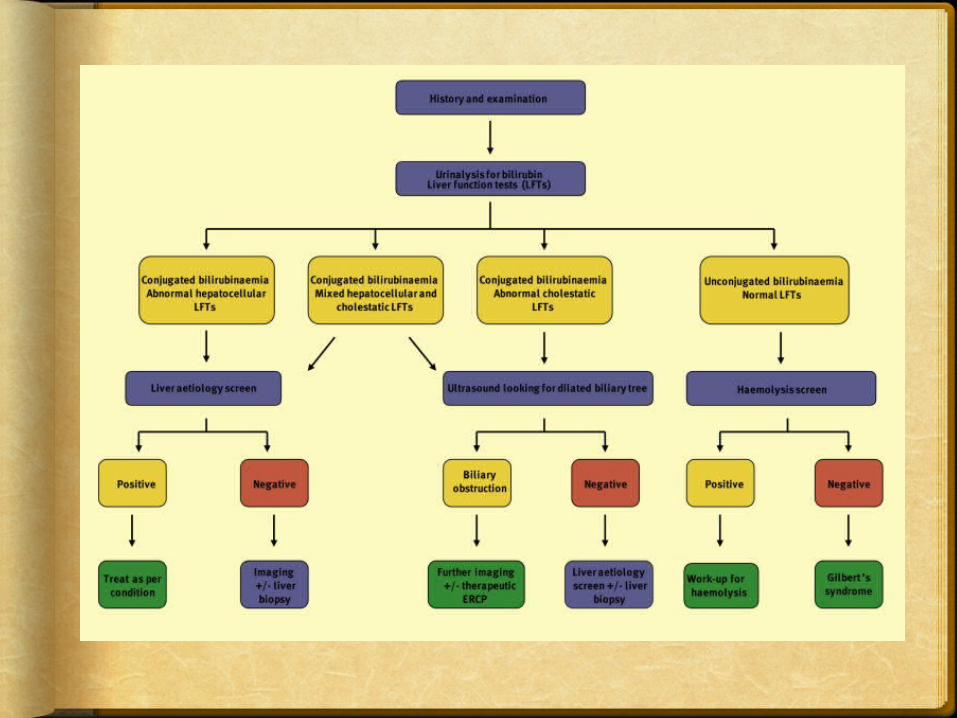
Pre-hepatic Jaundice
Haemolytic Cause: Genetic Causes
Sickle cell anaemia Spherocytosis Thalassemia Glucose 6-phosphate dehydrogenase
deficiency Kidney
Haemolytic uremic syndrome Defects in bilirubin metabolism
Gilbert’s Syndrome Rotor Syndrome Dubin Johnson Crigler-Najjar Syndrome
Infectious causes: Malaria
Where is the problem?-Spleen/blood/periphery
What is the problem?-Increased production of bilirubin
Is this going to result in increased Conjugated or unconjugated bilirubin or both?-Unconjugated
What symptoms will this produce?-Increased Urobilinogen-Normal Stools -Normal colour urine -Splenomegaly-Normal LFTs

Hepatic Jaundice Hepatocellular Causes:
Acute or Chronic Hepatitis Hepatotoxicity Cirrhosis Drug induced hepatitis Alcohol induced liver disease
Where is the problem?-Hepatocytes
What is the problem?-Swelling, oedema, fibrosis-Leading to a problem in transporting bilirubin from the blood to the biliaryCanaliculi.-Also can lead to problems with bilirubinConjugation
Is this going to result in increased Conjugated or unconjugated bilirubin or both?Both
What symptoms will this produce?-Increased urobilinogen, Increased urobilin (dark urine), Normal/pale stools, splenomegaly, deranged LFTs
Post Hepatic Jaundice
Obstructive Gall stones Pancreatitic cancer Liver flukes Biliary atresia Cholangiocarcinoma Pancreatitis Pancreatitc pseudocysts Mirizzi’s syndrome
Where is the problem?In the biliary tract
What is the problem?Generally obstruction Conjugated bilirubin cannot make it toThe small intestine
Is this going to result in increased Conjugated or unconjugated bilirubin or both?conjugated
What symptoms will this produce?Normal urobilinogen, dark urine (increased urobilin)Pale Stools No splenomegaly Normal LFTs
References Oxford Handbook of Clinical Medicine 2008
edition Kumar and Clark 2005 edition. Vander’s Physiology Marsano et al., 2003; Diagnosis and
Treatment of Alcoholic Chronic Disease and its complications; Alcohol Research and Health; 27; 3
http://www.gpnotebook.co.uk/simplepage.cfm?ID=161087510