Embed Size (px)
Citation preview
8/3/2019 jurnal diabates retinopati
http://slidepdf.com/reader/full/jurnal-diabates-retinopati 1/6
Diabetic retinopathy is a common
microvascular complication o
diabetes (Donnelly et al, 2000).
It is also the leading cause o blindness in
people o working age in the UK (Kohner
et al, 1996), with an estimated prevalence in
people with diabetes o almost 60% (Watkins,
2003). Through optimising some o the risk
actors o diabetic retinopathy, the progression
o retinopathy can be minimised (Diabetes
Control and Complications Trial Research
Group, 1993; UK Prospective Diabetes Study
Research Group, 1998).
As early as 1997, the worldwide prevalence
o diabetes was predicted to increase two- to
three-old by 2010 (Amos et al, 1997). There
are now approximately 2.5 million people
in the UK with diabetes, and this fgure isexpected to rise to 4 million by 2025 (Diabetes
UK, 2010).
With the expected increase in the prevalence
o diabetes in the coming years, the burden o
diabetic retinopathy workload and the number
o people aected by retinopathy is expected to
rise accordingly.
In recognition o these actors, the Diabetes
Eye Nurse Project – a joint venture between
the ophthalmology and diabetes departments
at the University Hospitals o Leicester NHS
Trust – was undertaken to optimise the care
o people with diabetes and related eye disease.
This article describes the project and the results
o a subsequent audit undertaken to evaluate
its eectiveness. Box 1 outlines the fve stages
o diabetic retinopathy and Figure 1 shows a
schematic diagram o the eye.
Retinal screening in LeicestershireRetinal eye screening is an integral part
o diabetes care, and annual screening is
Diabetic retinopathy:
Role o the diabetesspecialist eye nurse
Author details can be oundat the end o this article.
Traditionally, there is minimal cooperation between ophthalmology and diabetes departments. However, during the implementationphase o the diabetes National Service Framework in Leicestershire,people with diabetes expressed a wish or a “joined-up” diabetesservice, giving rise to the Diabetes Eye Nurse Project – a joint venture between the diabetes and ophthalmology departments.
The project has reduced the mean HbA 1c and serum lipid levels ina cohort o more than 100 people with diabetic eye disease, thereby reducing the risk o progression o the condition and other micro-and macrovascular complications. This article reviews this initiativeand demonstrates the value o a diabetes specialist eye nurse.
Article points
1. The Diabetes EyeNurse Project – a jointventure between theophthalmology anddiabetes departments atthe University Hospitals o Leicester NHS Trust – wasundertaken to optimise thecare o people with diabetesand related eye disease.
2. An audit was undertakento evaluate the eectivenesso the service in reducingHbA
1cand lipid levels over
the frst 12 months.
3. Glycaemic controlimproved in all cohorts,as did serum lipid levels.
4. Diabetes eye care deliveredby a diabetes specialist eye
nurse is a new, innovativeservice and is one o themany good examples o theexcellent multidisciplinary approach to the care o people with diabetes.
Key words
- Diabetes specialisteye nurse
- Eye- Ophthalmology - Retinopathy
Sabera Khan, Sam Wong, Rosi Gorrod,
Ismail Gangat, Stephen Hiles, JamesDeane, Ian Lawrence
292 Journal o Diabetes Nursing Vol 14 No 8 2010

8/3/2019 jurnal diabates retinopati
http://slidepdf.com/reader/full/jurnal-diabates-retinopati 2/6
recommended or all people with diabetes (NICE, 2004; 2008). In
people with type 1 diabetes, retinopathy develops gradually over timeand it is unusual or any changes to be seen within the frst 5 years. In
comparison, one third o people with type 2 diabetes may already have
some orm o retinopathy at diagnosis. It is thereore important that all
people with diabetes have access to retinal screening when diagnosed.
Retinal screening is dierent rom a general eye examination at the
opticians, which ocuses on the general health o the eye and whether
the person can see properly. I spectacles are required, the correct ones
are then prescribed. It is thereore important to highlight to people
with diabetes that they still need to visit the optician in addition to
their annual retinal screening i they wear spectacles.
The English National Screening Committee Programme or
Diabetic Retinopathy (ENSPDR, 2006) requires all retinal screenersto have either a NVQ or a Diploma in retinal screening. Locally, the
diabetes specialist eye nurse (DSEN) is responsible or the training,
assessment and mentoring o the retinal screeners. In addition, the
DSEN ensures that the screeners are able to understand the principles
and practice o testing the individual’s visual acuities and instilling
the correct eye drops. Once the competencies are met, the screeners
are then registered to undertake the City & Guilds Level 3 Certifcate
in Diabetic Retinopathy Screening.
In Leicestershire, there are approximately 47000 people with
diabetes. To cater or this population there is a systematic diabetic
eye screening service delivered in primary care. The University o Leicester NHS Trust employs 22 retinal screeners who are
placed in GP surgeries to carry out digital retinal imaging, as
recommended by the ENSPDR (2006).
Following assessment and documentation o visual acuity, the
individual’s pupils are then dilated. Images captured are initially
graded by the screeners and then by the ophthalmologist. People with
294 Journal o Diabetes Nursing Vol 14 No 8 2010
Diabetic retinopathy: Role o the diabetes specialist eye nurseACTOS ® pioglitazone
Prescribing Information
(Refer to Summary of Product Characteristics before prescribing) Actos ® tablets
(pioglitazone) Presentations: Actos 15mg tablets containing 15mg pioglitazone as
hydrochloride - blister packs of 28 EU/1/00/150/001 £25.83. Actos 30mg tablets containing
30mg pioglitazone as hydrochloride - blister packs of 28 EU/1/00/150/004 £35.89. Actos45mg tablets containing 45mg pioglitazone as hydrochloride - blister packs of 28
EU/1/00/150/012 £39.55. Indications:Monotherapy treatment of Type 2 diabetes mellitus inpatients inadequately controlled by diet and exercise for whom metformin is inappropriate
because of contraindications or intolerance. As dual oral therapy in patients with insufficientglycaemic control despite maximal tolerated dose of oral monotherapy, in combination with
either metformin (particularly in overweight patients) or a sulphonylurea (in patients for whommetformin is not tolerated or contraindicated). As triple oral therapy with metformin and a
sulphonylurea in patients (particularly overweight patients) with insufficient glycaemic control
despite dual oral therapy. In combination with insulin in patients with insufficient glycaemiccontrol on insulin for whom metformin is not tolerated or contraindicated. Dosage: 15mg or
30mg once daily with or without food. Dose may be increased in increments up to 45mg oncedaily. In combination therapy with insulin the current insulin dose can be continued. If patients
report hypoglycaemia, the dose of insulin should be decreased. Elderly & renal impairment(Cl creatinine > 4 ml/min): No dosage adjustment required . No information is available from
dialysed patients therefore pioglitazone should not be used. Children and adolescents(under 18 years): Not recommended. Contraindications: Hepatic impairment.
Hypersensitivity. Cardiac failure or history of cardiac failure (NYHA stages I to IV). Diabeticketoacidosis.Warnings and precautions:Can cause fluid retention, which may exacerbate
or precipitate heart failure. Observe patients for signs and symptoms of heart failure, weight
gain or oedema particularly those with reduced cardiac reserve or on insulin. Discontinuepioglitazone if deterioration in cardiac status occurs. For patients with at least one risk factor
for congestive heart failure, start therapy with the lowest dose of pioglitazone and increasegradually. Concomitant insulin administration may increase the risk of oedema. Check liver
enzymes before starting treatment. Following initiation it is recommended that liver enzymesbe monitored periodically based on clinical judgement. Do not start treatment in patients with
increased baseline liver enzyme levels (ALT > 2.5 x upper limit of normal [ULN]). If ALT levelsincrease to 3 x ULN, reassess as soon as possible. If ALT levels remain > 3 x ULN or jaundice
is observed, discontinue therapy. If symptoms suggest hepatic dysfunction, check liverenzymes. Advise patients to adhere strictly to a calorie-controlled diet and monitor weight. In
some cases, an increase in weight may be a symptom of card iac failure. Small reductions inhaemoglobin and haematocrit, consistent with haemodilution have been noted. Treatment inpatients with polycystic ovarian syndrome may result in ovulation. If a patient wishes to
become pregnant or if pregnancy occurs, discontinue treatment. An increased incidence inbone fractures in women has been observed in a pooled analysis of safety data involving
pioglitazone treatment. The risk of fractures should be considered in the long term care ofwomen treated with pioglitazone. Interactions: Use with caution during concomitant
administration of cytochrome P450 2C8 inhibitors (e.g. gemfibrozil) or inducers (e.g.rifampicin). Monitor glycaemic control. Pregnancy and lactation: Do not use. Potential risk
unknown. Undesirable effects: Suspected adverse reactions reported as more than an
isolated case in double-blind studies listed below. Very common: >10%, common: 1-10%,
uncommon: 0.1-1%, rare: 0.01-0.1% and very rare: < 0.01%. In monotherapy: Common:visual disturbance, upper respiratory tract infection, weight increased, hypoaesthesia.
Uncommon: sinusitis, insomnia. With metformin: Common: anaemia, weight increased,
headache, visual disturbance, arthralgia, haematuria, erectile dysfunction. Uncommon:
flatulence.With sulphonylurea: Common: weight increased, dizziness, flatulence. Uncommon:glycosuria, hypoglycaemia, increased lactic dehydrogenase, appetite increased, headache,
vertigo, visual disturbance, sweating, proteinuria, fatigue. With metformin and sulphonylurea:
Very common: hypoglycaemia. Common: weight increased, blood creatinine phosphokinase
increased, arthralgia. With insulin: Very common: oedema. Common: hypoglycaemia,bronchitis, weight increase, back pain, arthralgia, dyspnoea, hear t failure. Oedema reported
in 6-9% of patients on pioglitazone over one year, compared to 2-5% in the comparatorgroups (metformin and sulphonylurea). Oedema was generally mild-moderate and usually
did not require discontinuation of treatment. In most clinical trials, reduced total plasmatriglycerides and free fatty acids, and increased HDL-cholesterol levels were seen, with small,
but not clinically significant, increases in LDLcholesterol levels. In clinical trials the incidence
of elevations of ALT > 3 x ULN was equal to placebo. In an outcome study of patients withprior major macrovascular disease, the incidence of heart failure was 1.6% higher with
pioglitazone than with placebo, when added to therapy that included insulin. However, this didnot lead to an increase in mortality. Rare cases of elevated liver enzymes and hepatocellular
dysfunction have occurred in postmarketing experience, although causal relationship has notbeen established. There have been a small number of post marketing reports of macular
oedema. Be alert for disturbances in visual acuity. An increased incidence in bone fracturesin women has been observed in a pooled analysis of safety data involving
pioglitazone treatment.
Please refer to the summary of product characteristics for details on the full side-
effect profile of Actos. Adverse events should be reported. Reporting forms and
Information can be found at www.yellowcard.gov.uk . Adverse events should alsobe reported to Takeda UK Ltd.
PI Date Code: Jan 2010 Legal category: POM. MARKETING AUTHORISATION HOLDER:
Takeda Global R & D Centre (Europe) Ltd. Takeda UK Ltd. is responsible for the sale andsupply of ACTOS in the UK. Actos is a registered trademark owned by Takeda
Pharmaceutical Company Ltd. For further information contact: Takeda UK Ltd. Takeda House,Mercury Park, Wycombe Lane, Wooburn Green, High Wycombe, Bucks HP10 0HH.
Tel: 01628-537900, Fax: 01628-526617. AC091241
Please find more information at www.T2Dresource.co.uk
1. Campbell IW. Br J Diabetes Vasc Dis 2009; 9: 53-63.
2. Tan et al. Diabetes Care 2005; 28: 544–550
3. Belcher et al. Diabetes Res Clin Pract 2005; 70: 53 – 62
4. National Institute for Health and Clinical Excellence Type 2 diabetes—themanagement of type 2 diabetes. Clinical Guideline 87. London: NICE, 2009
5. Haffner, et al. Diabetes Care 1999; 22: 562-568
6. Lincoff et al. JAMA 2007; 298: 1180-11887. Takeda Uk Ltd. Actos Summary of Product Characteristics.
accessed at www.emc.medicines.org.uk. accessed date June 2010
8. Data on File at Takeda UK Ltd. AC200901
9. IMS Health, BPI, December 2007 - January 2010
References:
Code: AB100728jDate of Preparation: September 2010
Figure 1. Schematic diagram o the human eye.
Cornea
Anterior chamber(aqueous humour)
IrisPupilCiliary muscles
Suspensory ligamentLens
Vitreous humour
Retina
Choroid
Sclera
Optic disc
Fovea
Retinal blood vessels
Optic nerve

8/3/2019 jurnal diabates retinopati
http://slidepdf.com/reader/full/jurnal-diabates-retinopati 3/6
ungradeable images, or images that highlightsome indication o retinopathy, are invited to
a retinal screening clinic in secondary care or
urther examination.
Retinopathy is diagnosed through undus
examination (examining the back o the eyes)
by instilling dilating drops (tropicamide 1%
and phenylepherine 2.5%). The various stages
o retinopathy progression (Box 1) are then
diagnosed and recorded in the individual’s case
notes. Annual retinal screening is important as
this is how retinal changes are picked up.
Laser therapy
It is important to inorm people with diabetes
that laser treatment is not a cure and cannot
restore damaged vision, but can help prevent or
delay urther damage to the retina in over 90%o cases (Diabetic Retinopathy Study Research
Group, 1981). In most cases it is possible to
preserve the reading and driving vision.
There are three types o laser therapy: pan-
retinal photocoagulation, grid photocoagulation
and macula ocal photocoagulation.
Panretinal photocoagulation
Panretinal photocoagulation is usually used or
the treatment o prolierative retinopathy. Ater
instilling dilating drops and using a contact
lens that enlarges the view o the retina, theophthalmologist points a tiny laser beam into
the abnormal part o the retina. Small bursts o
laser dots are applied all over the retina (except
or between the optic disc and ovea) to stop the
296 Journal o Diabetes Nursing Vol 14 No 8 2010
1. Background retinopathy
This occurs in most people with diabetes approximately 20 years ater the onset o the condition and can thereore aect all age groups rom
late teens onwards. Usually, no symptoms present until there is macular involvement resulting in impairment o central vision to the eye
(Figures 2a and b ). To ensure that the eye in those diagnosed with early changes does not deteriorate urther, the person is discharged back to
the retinal call and recall services. Such individuals are advised to have annual check-ups to assess the degree o retinopathy (unduscopy − dots,blots and hard, waxy exudates), to control their cholesterol levels, and also given dietary advice and treatment rom the diabetes clinic.
2. Preprolierative retinopathy
This may develop in the eyes with background retinopathy only (Figure 3 ). The eye requires close observation but is not usually treated
unless regular ollow-up is not possible or vision in the ellow eye has been lost to prolierative disease (Scott, 2008).
3. Prolierative retinopathy
This is the main cause o visual impairment in people with type 1 diabetes. It occurs sooner ollowing the diagnosis o type 2 diabetes, possibly
because the diabetes has gone on or longer undetected. In this orm o retinopathy, the blood vessels grow into the vitreous humour and
bleed, causing a vitreous haemorrhage (Figures 4a and b ). Laser therapy, i required, can be used to treat prolierative retinopathy and aims to
prevent neovascularisation occurring. A laser beam is applied to the retina, as a dead retina will not encourage new vessel growth – scotomas
(areas o lost or depressed vision) present cause little visual impairment (Early Treatment Diabetic Retinopathy Study Research Group, 1985).
Vitrectomy (surgical intervention) can be used in severe cases to remove the haemorrhage and provide a scaold into which the new vessels can
grow. I perormed early in the development o retinopathy, laser therapy can help to improve visual recovery.
4. Advanced retinopathy
This is the end result o uncontrolled prolierative retinopathy (Figure 5 ). The eye can develop retinal tears or a detached retina, which
can lead to blindness. Early vitrectomy and also treating neovascular glaucoma (involvement o the iris with major risk o acute glaucoma)
improves visual recovery in people with prolierative retinopathy and severe vitreous haemorrhage (Mohamed et al, 2007). The individual
also requires management o visual impairment (support rom eye clinic liaison ofcers).
5. Maculopathy
This is the main cause o visual impairment in people with type 2 diabetes (Figure 6 ), and is classifed into our types:
lFocal/exudative.
lCystoid/diuse.
lIschaemic.
lMixed.
Only the ocal/exudative and mixed type o maculopathy can be treated by laser. Cystoid/diuse maculopathy is difcult to treat by
laser and ischaemic maculopathy cannot be treated.
Box 1. The fve stages o diabetic retinopathy.
Diabetic retinopathy: Role o the diabetes specialist eye nurse
Page points1. Retinopathy is diagnosed
through undusexamination (examiningthe back o the eyes) by instilling dilating drops(tropicamide 1% andphenylepherine 2.5%).
2. It is important to inormpeople with diabetes thatlaser treatment is not acure and cannot restoredamaged vision, but can
help prevent or delay urther damage to theretina in over 90% o cases.

8/3/2019 jurnal diabates retinopati
http://slidepdf.com/reader/full/jurnal-diabates-retinopati 4/6
growth o new blood vessels (Figure 7 ). This isusually carried out over several appointments
within an outpatient eye clinic. Fluorescein
angiography is perormed in-between sessions to
pinpoint remaining aected areas or to establish
the need or urther laser treatment.
I the vision is stabilised ater a ew sessions
o laser treatment, the possibility o urther
new vessel ormation is relatively unlikely.
However, the need or annual screening is still
recommended to monitor urther changes.
Grid photocoagulationGrid photocoagulation is used or treating
exudative maculopathy. Laser spots are applied
in a grid pattern lateral to the ovea. In cases
o retinal haemorrhage that do not clear using
grid photocoagulation, surgical intervention
(vitrectomy) may be perormed under a general
anaesthetic to remove abnormal tissue. Vision
can improve signifcantly but it is a major
operation and can be avoided i eective
screening and laser treatment is maintained.
Macular ocal photocoagulation
Focal photocoagulation o clinically signifcant
macular oedema substantially reduces the risk
o visual loss. Focal treatment also increases
the chance o visual improvement, decreases
the requency o persistent macular oedema
and causes only minor visual feld loss (Early
Treatment Diabetic Retinopathy Study Research
Group, 1985). Clinically signifcant macular
oedema is defned as retinal thickening that
involves or threatens the centre o the macula
(even i visual acuity is not yet reduced) and is
assessed by stereo contact lens biomicroscopy or
stereo photography.
Role o the DSEN:The Diabetes Eye Nurse Project
Traditionally, there is little or no major
cooperation between ophthalmology
and diabetes departments. During the
implementation phase o the diabetes National
Service Framework (NSF; Department o
Health [DH], 2001) in Leicestershire, people with diabetes expressed a wish or a “ joined-up”
diabetes service. They highlighted a need or
diabetes expertise in the ophthalmology clinics,
where many people were attending with diabeticeye disease, including diabetic retinopathy.
Pump-priming unding through a
pharmaceutical company led to the appointment
o a DSEN working in both the diabetes and
ophthalmology clinics in 2004. This new
routine service is in line with Standards 10, 11
and 12 o the diabetes NSF (DH, 2001):
lStandard 10: all young people and adults with
diabetes will receive regular surveillance or
the long-term complications o diabetes.
l Standard 11: the NHS will develop,implement and monitor agreed protocols and
systems o care to ensure that all people who
develop long-term complications o diabetes
receive timely, appropriate and eective
investigation and treatment to reduce their
risk o disability and premature death.
lStandard 12: all people with diabetes requiring
multi-agency support will receive integrated
health and social care.
Most people are reerred rom the district
retinal screening service; some rom other diabetes
retinal clinics. The other ophthalmologists were
introduced to the diabetes eye service and the
reerral protocol via a presentation delivered by
the DSEN (Box 2 ). This collaboration has helped
raise the profle o the diabetes eye service as the
eye department now consists o 14 consultant
ophthalmologists, maintaining varied specialist
eye clinics, and who have been able to access
diabetes expertise as needed.
Following initial assessment o the person by
the DSEN, other elements are then reviewed:
l Baseline biomedical parameters (HbA 1c level,renal unction, lipid profle and urine albumin
excretion).
298 Journal o Diabetes Nursing Vol 14 No 8 2010
Diabetic retinopathy: Role o the diabetes specialist eye nurse
Figure 2. Normal retina with no diabetic retinopathy (a); background diabetic retinopathy with microaneurysms,haemorrhages and exudates (b). Copyright 1st Retinal Screening Ltd.
a
b
Figure 3. Preprolierative diabetic retinopathy with cotton wool spots, intraretinal microaneurysm
and multiple blot haemorrhages. Copyright 1st Retinal Screening Ltd.
Figure 4. Prolierative retinopathy with new vessels at the optic disc (a); prolierative retinopathy with preretinal and vitreous haemorrhages. Copyright 1st Retinal Screening Ltd.
a b

8/3/2019 jurnal diabates retinopati
http://slidepdf.com/reader/full/jurnal-diabates-retinopati 5/6
l
Blood pressure.lLiestyle (including smoking cessation, basic
dietary review, physical activities and alcohol
consumption).
l Current medications.
l Provision o individual diabetes education,
including sel-monitoring o blood glucose.
Intervention is provided or any identifed
diabetes-related problems to delay urther
progression o eye disease and other diabetes-
related complications. Follow-up care or
titration o medication is maintained through
telephone contact. The frst telephone callis usually within 1−2 weeks o the initial
contact and a urther DSEN advisory clinic
appointment is within 1 month or earlier,
depending on the individual’s needs. Those
with more complex issues are seen in the clinic
o the supervising diabetes physician, alongside
the DSEN and diabetes dietitian.
Audit
Aim and methods
An audit was undertaken to evaluate theeectiveness o the service in reducing
HbA 1c
levels over the frst 12 months ater
implementation. The case notes o 181 people
seen at least once in the ophthalmology
clinic were reviewed. Biomedical parameters,
including HbA 1c
levels and total cholesterol,
were measured at baseline and then monitored
every 6 months. The data presented in here are
or 6- and 12-month ollow-up.
Results and discussion
Baseline data separated into three cohorts: white
European origin (53.6%; n =97); south Asian
origin (41.5%, n =75); other (4.9%, n =9). At12 months, ollow-up data were only available
or 100 people.
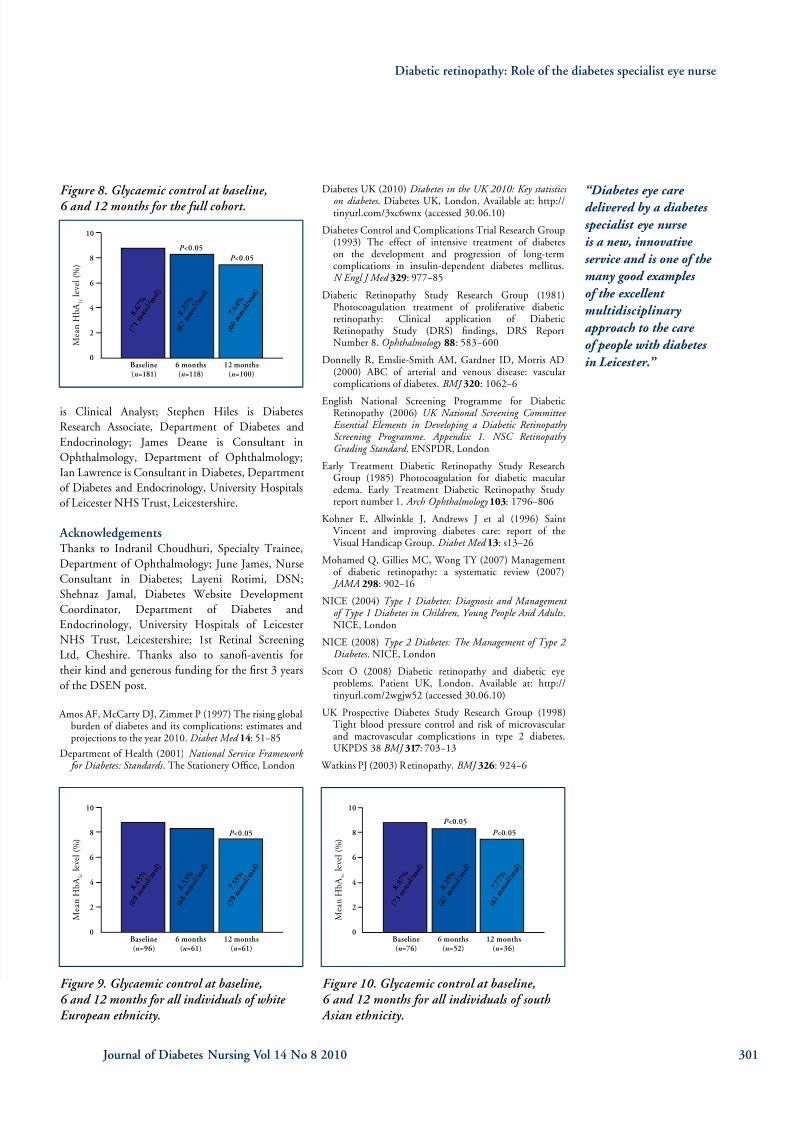
Glycaemic control improved in all cohorts
(Figures 8–10 ). Mean HbA 1c
levels or the ull
cohort reduced rom 8.67% (71 mmol/mol) at
baseline to 8.27% (67 mmol/mol) at 6 months,
and at 12 months this had urther reduced
to 7.64% (60 mmol/mol; P <0.001). Prior to
the intervention over 30% o individuals had
a baseline HbA 1c
o >9% (>75 mmol/mol);
ollowing the intervention this number had
reduced to 10%. By study end over 50% o individuals had achieved an HbA
1clevel o
<7.5% (<58 mmoL/mol).
Compared with baseline, mean total cholesterol
levels had reduced at 12 months (4.80 mmol/L
vs 4.50 mmol/L, respectively; P =0.001), as had
mean LDL-cholesterol levels at both 6 months
(3.04 mmol/L vs 2.73 mmol/L, respectively;
P <0.05) and at 12 months (3.04 mmol/L vs
2.57 mmol/L, respectively; P =0.001). The
improvement in lipid parameters was seen both
in the white European and south Asian groups,and the south Asian group also had reduced
triglycerides over the 12-month study period
(−0.34 mmol/L, P <0.05).
Conclusion
To date, 350 people have been seen as part o
the Diabetes Eye Nurse Project, and initial
4-year ollow-up data were presented as an
abstract at the Diabetes UK Annual Proessional
Conerence in 2010. These data are to be
written up or publication later this year.
The Diabetes Eye Nurse Project has helped
to identifed high-risk individuals with diabetes
oten with untreated risk actors. Diabetes eye
care delivered by a DSEN is a new, innovative
service and is one o the many good examples o
the excellent multidisciplinary approach to the
care o people with diabetes in Leicester. n
AuthorsSabera Khan is Diabetes and Ophthalmic Specialist
Nurse, Department o Diabetes and Endocrinology;
Sam Wong is Associate Specialist in Ophthalmology,Department o Ophthalmology; Rosi Gorrod is
Senior Diabetes Nurse Specialist; Ismail Gangat
300 Journal o Diabetes Nursing Vol 14 No 8 2010
lPeople with at least background (or more serious) diabetic retinopathy.
lPeople with HbA 1c
levels o ≥7.5% (≥58 mmol/mol; changed to ≥9.1%[≥76 mmol/mol] ater the service was established).
lPoorly controlled hypertension.
lRaised lipid parameters.
lMicroalbuminuria, smoking or obesity.
lOther major concerns regarding the individual’s diabetes care that may adversely aect vision.
Box 2. Reerral protocol.
Figure 7. Laser treatment – laser dots around the retina.Copyright 1st Retinal Screening Ltd.
Diabetic retinopathy: Role o the diabetes specialist eye nurse
Figure 5. Advanced retinopathy – fbrous prolieration. Copyright 1st Retinal Screening Ltd.
Figure 6. Diabetic
maculopathy with haemorrhages and circinate exudates and multiple blot haemorrhages. Copyright 1st Retinal Screening Ltd.
8/3/2019 jurnal diabates retinopati
http://slidepdf.com/reader/full/jurnal-diabates-retinopati 6/6
is Clinical Analyst; Stephen Hiles is Diabetes
Research Associate, Department o Diabetes and
Endocrinology; James Deane is Consultant in
Ophthalmology, Department o Ophthalmology;
Ian Lawrence is Consultant in Diabetes, Department
o Diabetes and Endocrinology, University Hospitals
o Leicester NHS Trust, Leicestershire.
AcknowledgementsThanks to Indranil Choudhuri, Specialty Trainee,
Department o Ophthalmology; June James, Nurse
Consultant in Diabetes; Layeni Rotimi, DSN;
Shehnaz Jamal, Diabetes Website Development
Coordinator, Department o Diabetes and
Endocrinology, University Hospitals o Leicester
NHS Trust, Leicestershire; 1st Retinal Screening
Ltd, Cheshire. Thanks also to sanof-aventis or
their kind and generous unding or the frst 3 years
o the DSEN post.
Amos AF, McCarty DJ, Zimmet P (1997) The rising globalburden o diabetes and its complications: estimates andprojections to the year 2010. Diabet Med 14: 51−85
Department o Health (2001) National Service Framework for Diabetes: Standards . The Stationery Ofce, London
Diabetes UK (2010) Diabetes in the UK 2010: Key statistics on diabetes . Diabetes UK, London. Available at: http://tinyurl.com/3xc6wnx (accessed 30.06.10)
Diabetes Control and Complications Trial Research Group(1993) The eect o intensive treatment o diabeteson the development and progression o long-termcomplications in insulin-dependent diabetes mellitus.N Engl J Med 329: 977−85
Diabetic Retinopathy Study Research Group (1981)Photocoagulation treatment o prolierative diabeticretinopathy: Clinical application o DiabeticRetinopathy Study (DRS) fndings, DRS ReportNumber 8. Ophthalmology 88: 583−600
Donnelly R, Emslie-Smith AM, Gardner ID, Morris AD(2000) ABC o arterial and venous disease: vascularcomplications o diabetes. BMJ 320: 1062−6
English National Screening Programme or DiabeticRetinopathy (2006) UK National Screening Committee Essential Elements in Developing a Diabetic Retinopathy Screening Programme. Appendix 1. NSC Retinopathy Grading Standard . ENSPDR, London
Early Treatment Diabetic Retinopathy Study ResearchGroup (1985) Photocoagulation or diabetic macularedema. Early Treatment Diabetic Retinopathy Study report number 1. Arch Ophthalmology 103: 1796−806
Kohner E, Allwinkle J, Andrews J et al (1996) SaintVincent and improving diabetes care: report o theVisual Handicap Group. Diabet Med 13: s13–26
Mohamed Q, Gillies MC, Wong TY (2007) Managemento diabetic retinopathy: a systematic review (2007)
JAMA 298
: 902−16NICE (2004) Type 1 Diabetes: Diagnosis and Management
of Type 1 Diabetes in Children, Young People And Adults .NICE, London
NICE (2008) Type 2 Diabetes: The Management of Type 2 Diabetes . NICE, London
Scott O (2008) Diabetic retinopathy and diabetic eyeproblems. Patient UK, London. Available at: http://tinyurl.com/2wgjw52 (accessed 30.06.10)
UK Prospective Diabetes Study Research Group (1998)Tight blood pressure control and risk o microvascularand macrovascular complications in type 2 diabetes.UKPDS 38 BMJ 317: 703−13
Watkins PJ (2003) Retinopathy. BMJ 326: 924−6
Diabetic retinopathy: Role o the diabetes specialist eye nurse
Figure 8. Glycaemic control at baseline,6 and 12 months or the ull cohort.
Figure 9. Glycaemic control at baseline,6 and 12 months or all individuals o white European ethnicity.
Figure 10. Glycaemic control at baseline,6 and 12 months or all individuals o south Asian ethnicity.
Journal o Diabetes Nursing Vol 14 No 8 2010 301
“Diabetes eye care delivered by a diabetes
specialist eye nurse
is a new, innovative
service and is one of the
many good examples
of the excellent
multidisciplinary
approach to the care
of people with diabetes
in Leicester.”
M e a n H b A
1 c
l e v e l ( % )
10
8
6
4
2
0Baseline(n =181)
6 months(n =118)
12 months(n =100)
8 . 6 7
%
( 7 1 m m o l / m
o l )
8 . 2 7
%
( 6 7 m m o l / m
o l )
7 . 6 4
%
( 6 0 m m o l / m
o l )
P <0.05
P <0.05
M e a n H b A
1 c
l e v e l ( % )
10
8
6
4
2
0Baseline(n =76)
6 months(n =52)
12 months(n =36)
8 . 8 7
%
( 7 3 m m o l / m
o l )
8 . 2 5
%
( 6 7 m m o l / m
o l )
7 . 7 7
%
( 6 1 m m o l / m
o l )
P <0.05
P <0.05
M e a n H b A
1 c
l e v e l ( % )
10
8
6
4
2
0Baseline(n =96)
6 months(n =61)
12 months(n =61)
8 . 4 5
%
( 6 9 m m o l / m
o l )
8 . 3 3
%
( 6 8 m m o l / m
o l )
7 . 5 5
%
( 5 9 m m o l / m
o l )
P <0.05