Embed Size (px)
Citation preview
PENATALAKSANAAN
ABORTUS INKOMPLIT
• Prinsip : Pembersihan sisa konsepsi.
• Caranya tergantung :
– Usia kehamilan, besar uterus dan hasil – Usia kehamilan, besar uterus dan hasil penghitungan HPHT
– Ketersediaan peralatan, pasokan dan tenaga kesehatan yg terampil
→ tidak ada : RUJUK !

Table 1. Impact of Unsafe Abortion by Region
Region
Number
of unsafe
abortions
(1000s)††
Unsafe
abortions
per 1000
women 15-
49
Number of
deaths from
unsafe
abortion††
Mortality from
unsafe
abortion per
100,000 live
births
Case fatality
per 100
unsafe
abortions
Risk of
death
More developed 2340 8 600 4 0.03 1 in 3700More developed
countries
2340 8 600 4 0.03 1 in 3700
Less developed
countries†17620 17 69000 55 0.4 1 in 250
Africa 3740 26 23000 83 0.6 1 in 150
Asia† 9240 12 40000 47 0.4 1 in 250
Europe 260 2 100 2 0.04 1 in 2600
Latin America 4620 41 6000 48 0.1 1 in 800
USSR (former) 2080 30 500 10 0.03 1 in 3900

Table 2. Provision of Postabortion Care by Level of Healthcare Facility and Staff
LevelStaff May Include Emergency Postabortion Care Provided
Postabortion Family
Planning
Community Community residents with
basic health training
Traditional birth attendants
Traditional healers
•Recognition of signs and symptoms of abortion and serious post
abortion complications
•Referral to facilities where treatment is available
Provision of pills,
condoms, diaphragms and
spermicides
Referral and follow up for
these and other methods
Primary
(Primary health
clinics, Family
planning clinics
or Polyclinics)
Health workers
Nurses
Trained midwives
General practitioners
All primary care facilities. Above activities, plus:
•Diagnosis based on medical history and physical and pelvic
examination
•Resuscitation/preparation for treatment or transfer
•Haematocrit/hemoglobin testing
•Referral, if needed
Provision of above
methods plus IUDs,
injectables and Norplant®
implants
Referral for voluntary
sterilization
If trained staff and appropriate equipment are available.
Above activities, plus:
•Initiation of emergency treatments
•antibiotic therapy
•intravenous fluid replacement •intravenous fluid replacement
•oxytocics
•Uterine evacuation during first trimester for uncomplicated cases
of incomplete abortion
•Pain control
•simple analgesia and sedation
•local anesthesia (paracervical block)
First Referral
Level
(District hospital)
Nurses
Trained midwives
General practitioners
Ob/Gyn specialists
Above activities, plus:
•Emergency uterine evacuation through second trimester
•Treatment of most postabortion complications
•Local and general anesthesia
•Diagnosis and referral for severe complications (septicemia,
peritonitis, renal failure)
•Laparotomy and indicated surgery (including for ectopic
pregnancy)
•Blood crossmatch and transfusion
Provision of above
methods plus voluntary
sterilization
Followup
Secondary and
Tertiary Level
(Regional or
Referral
hospital)
Nurses
Trained midwives
General practitioners
Ob/Gyn specialists
Above activities, plus:
•Uterine evacuation as indicated for all incomplete abortions
•Treatment of severe complications (including bowel injury,
severe sepsis, renal failure)
•Treatment of bleeding/clotting disorders
All above activities
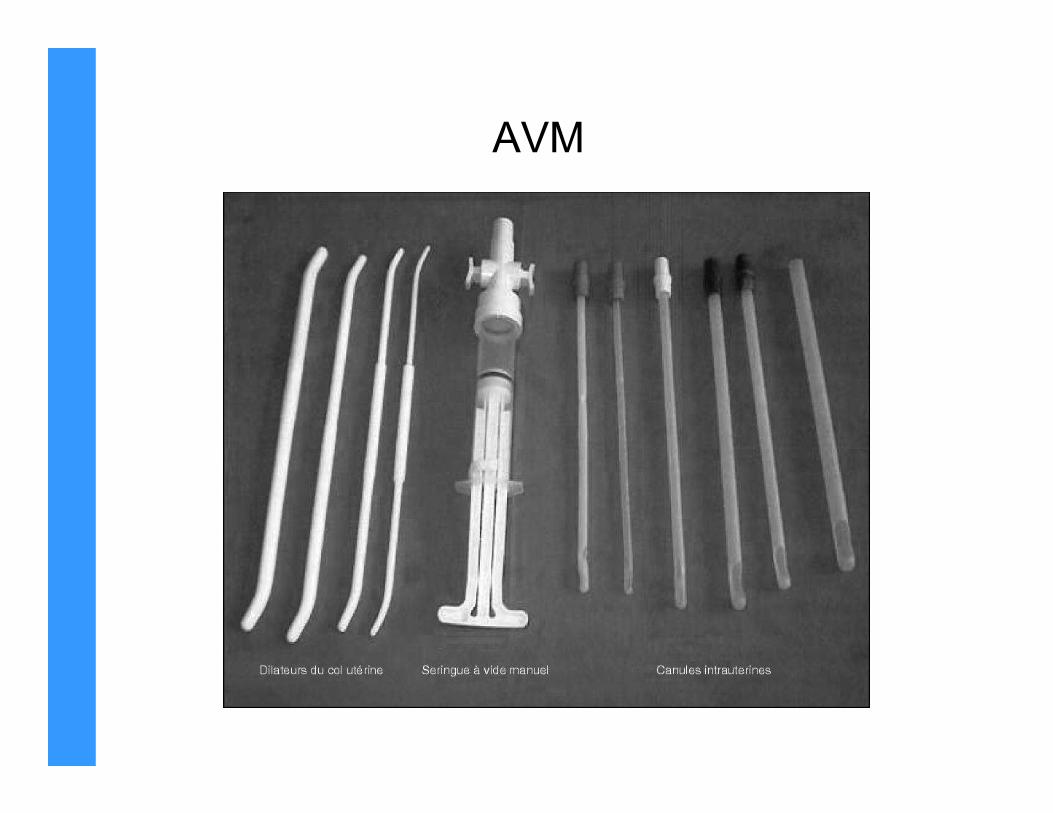
AVM
KEUNGGULAN AVM
– Sampai usia 12-14 mgg
– Risiko lebih rendah drpd kuret
tajamtajam
– Anestesi umum (-)
– Ruang khusus (-)

ASPIRASI VAKUM MANUAL
→→→→ Dgn tek. negatif
• Masukkan kanula, hubungkan dg tabung
pengisap melalui adaptorpengisap melalui adaptor
• Buka katup pengatur sampai tek. negatif
• Kanula digerakkan maju-mundur sambil
rotasi ke kanan-kiri

PERLENGKAPAN ALAT AVM
• Tabung vol.60 ml, dengan :
– 1 atau 2 katup pengatur
– Toraks & tangkai
penarik/pendorongpenarik/pendorong
– Penahan toraks
– Silikon pelumas cincin karet
• Kanula steril

PEMILIHAN ALAT AVM
UKURAN
KANULKATUP USIA KEHAMILAN
5 – 6 mm 1 atau 2 0-8 minggu
6-10 mm
12 mm2 katup
Trimester I - II awal
(< 14 mgg)

KEWASPADAAN SEBELUM
TINDAKAN AVM
Yg menjadi perhatian, bila :
• Besar uterus tdk sesuai dgn usia • Besar uterus tdk sesuai dgn usia
kehamilan (HPHT)
• Usia kehamilan > trimester pertama

PERSIAPAN PROSEDUR AVM
1. Mengurangi Risiko Infeksi
– Cuci tangan dg sabun & air mengalir
– Peralatan yg steril atau DTT
– Bersihkan vagina & serviks dg lar. antiseptik
– Teknik tanpa sentuh

2. Menyiapkan Instrumen AVM
– Periksa fungsi isap tabung AVM
– Kesiapan tindakan gawat darurat
– Buat tekanan negatif dengan :
• Kunci katup pengatur• Kunci katup pengatur
• Tarik tangkai toraks
3. Pemeriksaan Panggul
– Besar & arah uterus (bimanual)
– Kondisi vagina & serviks

4. Persiapan Pasien
– Kosongkan kandung kemih
– Bersihkan perut bawah, lipat paha, genitalia
eksterna dengan sabun & air.eksterna dengan sabun & air.
– Siapkan vagina & serviks dgn antiseptik 2-3 kali
(bila dengan iodofor tunggu 2’)

LANGKAH-LANGKAH PROSEDUR AVMLANGKAH-LANGKAH PROSEDUR AVM

Langkah 1
• Masukkan spekulum
• Keluarkan jaringan atau bekuan darah
• Cabut AKDR bila ada.
Langkah 2
• Bersihkan servik & vagina dgn larutan
antiseptik

Langkah 3
• Blok paraservikal (bila perlu)
Langkah 4
• Pegang bibir atas serviks dengan
tenakulum/klem ovum (jam 1 dan jam 11)
• Ukur bukaan ostium dengan kanul
Anestesi verbal G

Langkah 5
• Masukkan kanula
dengan adaptordengan adaptor
• Dorongan ringan dan
putar kiri-kanan

Langkah 6
• Perhatikan ukuran bila
kanula telah mencapai
fundusfundus
• Titik terdekat 6 sm
• Tarik sedikit ujung
kanula dari fundus

Langkah 7
• Hubungkan pangkal
kanula dengan
tabung AVMtabung AVM

Langkah 8
• Buka katup pengatur
• Bila bekerja : cairan • Bila bekerja : cairan
darah & busa

Langkah 9
• Gerakkan kanula maju-mundur + rotasi jam 10-2
• Jangan sampai tertarik keluar
• Bila tek. negatif hilang • Bila tek. negatif hilang � tutup pengatur + lepaskan kanula
• Siapkan tek. negatif kembali & pasang kembali
• Jangan pegang pada tangkai pendorong !

Langkah 10
• Periksa kebersihan kavum uteri
• Tanda :
– Busa-busa merah
– Jaringan tak terlihat
– Terasa kasar
– Uterus kontraksi
– Kanul seperti terjepit
Langkah 11• Keluarkan kanula
• Lepaskan sambungan
• Masukkan ke wadah dekontaminasi
– Kanul seperti terjepit

Langkah 12
Periksa jaringan :
• Jumlah & massa kehamilan• Jumlah & massa kehamilan
• Pastikan kebersihan evakuasi
• Adanya kelainan seperti mola

Cara Pemeriksaan
• Isi mangkok + air bersih + kassa saringan
• Hasil evakuasi + mangkok �angkat
• Jaringan :
– Vili korialis :– Vili korialis :
• Putih keabuan, memanjang, mengambang
– Endometrium :
• Massa lunak, licin, butiran putih tanpa juluran halus, tenggelam

Bila Tak Tampak Jaringan Kehamilan
Kemungkinan :
• Abortus komplit
• Kurang terampil � tidak terambil
• Bukan abortus inkomplit
• Uterus abnormal
Bila Tak Tampak Jaringan Kehamilan + Tanda
Kehamilan � KEHAMILAN EKTOPIK !!!

Langkah 13-16
• Lepaskan tenakulum & spekulum
• Dekontaminasi alat : klorin 0,5% 10’ :
– 2 tempat : logam + non logam
– Alat tidak terkunci
• Bersihkan sarung tangan � balikkan
• Cuci tangan dgn sabun & air mengalir

Langkah-langkah kuret dengan
kuret tajamkuret tajam

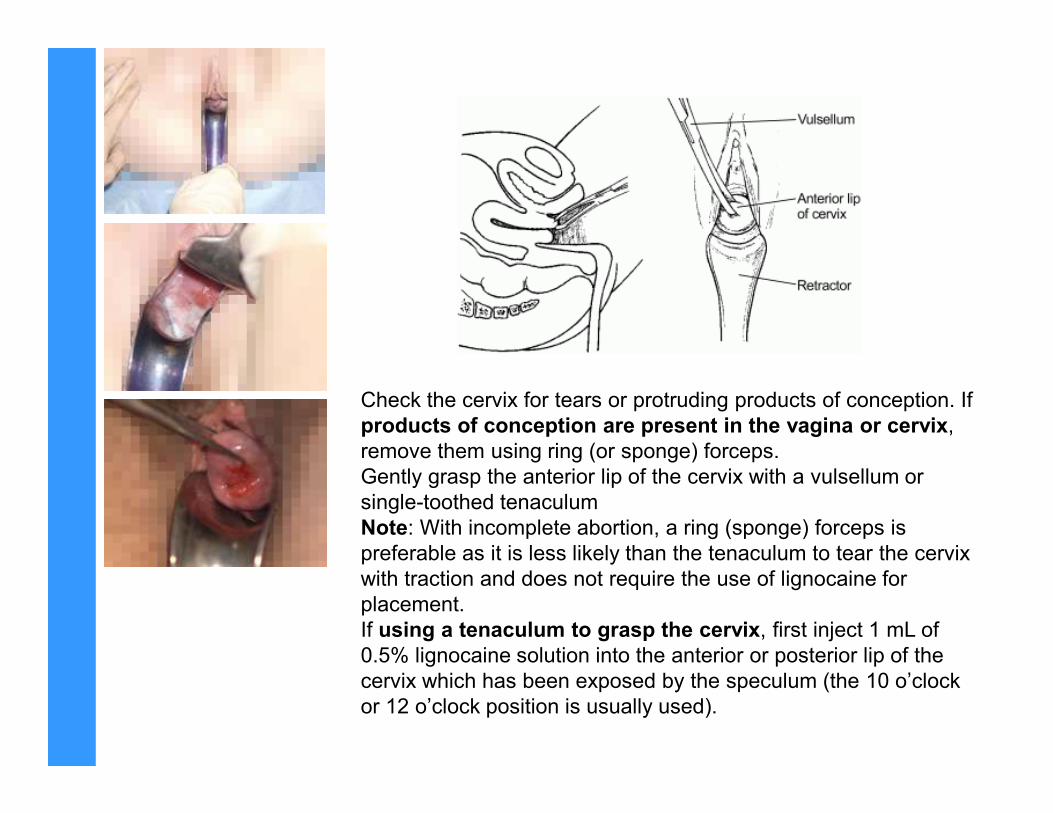
Check the cervix for tears or protruding products of conception. If Check the cervix for tears or protruding products of conception. If
products of conception are present in the vagina or cervix,
remove them using ring (or sponge) forceps.
Gently grasp the anterior lip of the cervix with a vulsellum or
single-toothed tenaculum
Note: With incomplete abortion, a ring (sponge) forceps is
preferable as it is less likely than the tenaculum to tear the cervix
with traction and does not require the use of lignocaine for
placement.
If using a tenaculum to grasp the cervix, first inject 1 mL of
0.5% lignocaine solution into the anterior or posterior lip of the
cervix which has been exposed by the speculum (the 10 o’clock
or 12 o’clock position is usually used).

Dilatation is needed only in cases of missed abortion or when some
retained products of conception have remained in the uterus for several
days:
- Gently introduce the widest gauge cannula or curette;
- Use graduated dilators only if the cannula or curette will not pass.
Begin with the smallest dilator and end with the largest dilator that
ensures adequate dilatation (usually 10–12 mm) (Fig P-33);
- Take care not to tear the cervix or to create a false opening.

Gently pass a uterine sound through the cervix to assess the length and
direction of the uterus.
The uterus is very soft in pregnancy and can be easily injured during
this procedure.
Evacuate the contents of the uterus with ring forceps or a large curette
Gently curette the walls of the uterus until a grating sensation is felt.


Give paracetamol 500 mg by mouth as needed.
Encourage the woman to eat, drink and walk about as she wishes.
Offer other health services, if possible, including tetanus prophylaxis,
counselling or a family planning method.
Discharge uncomplicated cases in 1–2 hours.
Advise the woman to watch for symptoms and signs requiring Advise the woman to watch for symptoms and signs requiring
immediate attention:
- prolonged cramping (more than a few days);
- prolonged bleeding (more than 2 weeks);
- bleeding more than normal menstrual bleeding;
- severe or increased pain;
- fever, chills or malaise;
- fainting.

KURET HISAP






























