Embed Size (px)
Citation preview

La Ricerca GerontologicoLa Ricerca Gerontologico--Geriatrica Geriatrica in Italia:in Italia: NNuoveuove LLinee inee SStrategichetrategiche
Firenze, 29 novembre 2008Firenze, 29 novembre 2008
5353°° Congresso NazionaleCongresso Nazionale
Fabrizia LattanzioFabrizia Lattanzio


0100002000030000400005000060000700008000090000
1970-79 1980-89 1990-99 2000-08
Numero Totale di Pubblicazioni
Rapp. Pubblicazioni di Istituti Geriatr./Non Geriatr.
0
10
20
30
40
50
1970-79 1980-89 1990-99 2000-08
%0
5001000150020002500300035004000
1970-79 1980-89 1990-99 2000-08
Numero di Pubblicazioni Italiane
Totali
Limits: Humans; Keywords: Elderly OR Ageing OR Aging; ItalyAffiliation Geriatr* OR Gerontol*
Analisi della letteratura gerontologica/geriatrica in italia e nAnalisi della letteratura gerontologica/geriatrica in italia e nel mondoel mondo
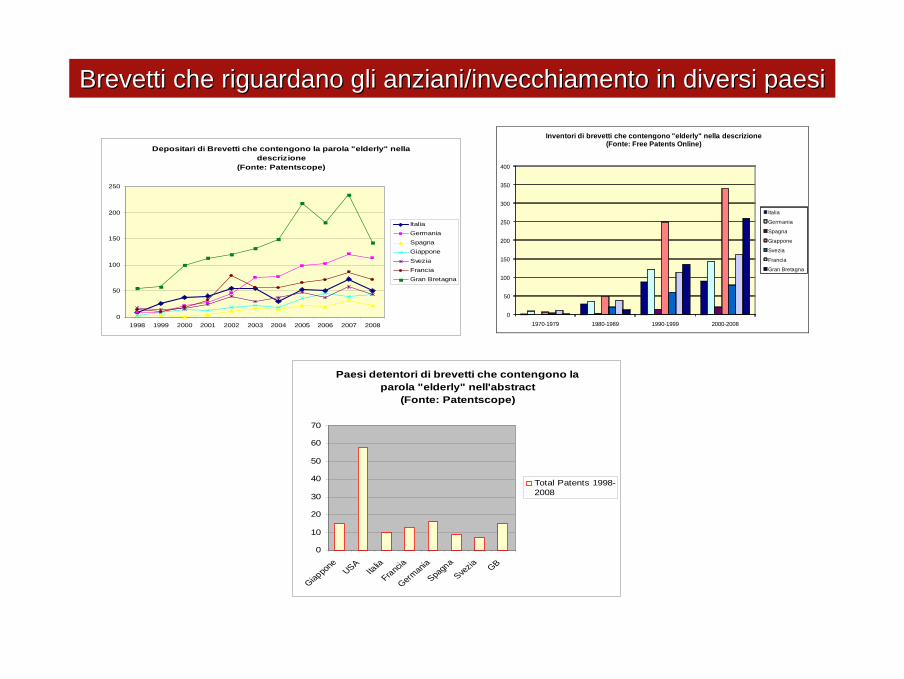
Depositari di Brevetti che contengono la parola "elderly" nella descrizione
(Fonte: Patentscope)
0
50
100
150
200
250
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
ItaliaGermaniaSpagnaGiapponeSveziaFranciaGran Bretagna
0
50
100
150
200
250
300
350
400
1970-1979 1980-1989 1990-1999 2000-2008
Inventori di brevetti che contengono "elderly" nella descrizione(Fonte: Free Patents Online)
Italia
Germania
Spagna
Giappone
Svezia
Francia
Gran Bretagna
Paesi detentori di brevetti che contengono la parola "elderly" nell'abstract
(Fonte: Patentscope)
0
10
20
30
40
50
60
70
Giappo
neUSA
Italia
Francia
German
iaSpa
gna
Svezia GB
Total Patents 1998-2008
Brevetti che riguardano gli anziani/invecchiamento in diversi paBrevetti che riguardano gli anziani/invecchiamento in diversi paesiesi

LE: life expentancy yearsHLE: health life expentancy years
-
-
-
-
-
LU
IT
- - - - -
DK
MT
GRUK NL
IE
SE
FR
ESBESI
PL
CZ
AT
FICY
PT
DESKLV
LT
EEHU
28 30 32 34 36
8
12
16
20
24
HLE
/yrs
LE/yrs
♀-
-
-
-
-
LVLT
HU
EE
SK
CZ
PL
SI
R
DE
ATPT
CY
LUBE
FR
ESIEGR
NLUK
MT
DK
ITSE
- - - -- - - -
24
20
16
12
8
20 22 24 26 28 30 32
HLE
/yrs
LE/yrs
♂
Aspettativa di vita in buona salute a 50 anni nei 25 della CEAspettativa di vita in buona salute a 50 anni nei 25 della CE
LANCET 2008

Percentages of the individuals born in 1905 classified as independent at four assessments in the period 1998–2005. Dotted lines show the ‘‘history’’of individuals completing at least 2, 3, and 4 waves, respectively.For example, the graphs show that among the 156 persons (30 men and 126 women) who participated in all four assessments, 33% were independent at the last assessment at age 99–100 years, but 70% were independent at the intake assessment at age 92–93 years. The graph thus shows that, although the level of independence in the overall 1905 cohort remained nearly stable from age 92–93 years through age 99–100 years, most of the individuals experienced a loss of abilities after age 92–93 years. The explanation for this apparent paradox is a very high mortality among the dependent participants.
Christensen K. PNAS 2008

GERONTOLOGY
Kirkwood T. Nature 2008

Farrelly C. BMJ 2008
Has the time to get more serious the effort to slow human aging?
This ultimate goal can be achieved by curing disease but it can also be achieved increasing the duration of disease-free life. There is no reason why we cannot pursue both strategies – aggressively tackling individual disease and aging
Un sistema complesso è un sistema in cui gli elementi subiscono continue modifiche singolarmente prevedibili, ma di cui non èpossibile, o è molto difficile, prevedere uno stato futuro.
Un sistema complesso è un sistema in cui gli elementi subiscono continue modifiche singolarmente prevedibili, ma di cui non èpossibile, o è molto difficile, prevedere uno stato futuro.
Maggiore è la quantità e la varietà delle relazioni fra gli elementi di un sistema e maggiore è la sua complessità
Maggiore è la quantità e la varietà delle relazioni fra gli elementi di un sistema e maggiore è la sua complessità
Paziente anziano
Comorbilità
Trattamento farmacologico
Outcomes geriatrici

0
10000
20000
30000
40000
50000
1970‐1979 1980‐1989 1990‐2000 2000‐2008
N° di pubblicazioni mondiali su "Medication and Elderly"
Tot n° papers
0%
20%
40%
60%
80%
100%
1970‐1979 1980‐1989 1990‐2000 2000‐2008
Pubblicazioni su "Medication and Elderly"
Italy
Germany
France
UK
Japan
USA
0%
20%
40%
60%
80%
100%
1970‐1979 1980‐1989 1990‐2000 2000‐2008
Pubblicazioni su "Medication and Elderly" (Clinical trials I or II)
Italy
Germany
France
UK
Japan
USA
0%20%40%60%80%
100%
1970‐1979 1980‐1989 1990‐2000 2000‐2008
Pubblicazioni su "Medication and Elderly" (Clinical trials III)
Italy
Germany
France
UK
Japan
USA
0%20%40%60%80%
100%
1970‐1979 1980‐1989 1990‐2000 2000‐2008
Pubblicazioni su "Medication and Elderly" (Clinical trials IV)
Italy
Germany
France
UK
Japan
USA
Pubblicazioni relative a farmaci e trials clinici negli anziani Pubblicazioni relative a farmaci e trials clinici negli anziani

Risk Reduction (%)
Trial N Age Stroke CAD CHF AllCVD
Australian 582 60-69 33% 18% NA 31%EWPHE 840 > 60 36% 20% 22% 29%Coope 884 60-79 42% 3% 32% 24%STOP-HTN 1627 70-84 47% 13% 51% 40%MRC 4396 65-74 25% 19% NA 17%HDFP 2374 60-69 44% 15% NA 16%SHEP 4736 > 60 33% 27% 55% 32%Syst-Eur 4695 > 60 42% 26% 36% 31%STONE 1632 60-79 57% 6% 68% 60%Syst-China 2394 > 60 38% 33% 38% 37%
Trials of Antihypertensive Treatment in the Trials of Antihypertensive Treatment in the ““ElderlyElderly

MortalitMortalitàà generalegenerale
MortalitMortalitàà CVCV
Eventi coron.Eventi coron.
Insuff. card.Insuff. card.
Eventi CVEventi CVEWPHEEWPHESHEPSHEP--PPSHEPSHEPSTOPSTOPSystSyst--EurEur
1.00.80.2 0.4 0.6 1.2 1.4 1.6 1.8RR (95% CI)RR (95% CI)
Trattamento antiipertensivo vs. PlaceboTrattamento antiipertensivo vs. Placebo
EtEtàà>>80 aa80 aaN=1566N=1566
IctusIctus
Prevenzione del rischio CV nel Prevenzione del rischio CV nel ““grande vecchiogrande vecchio”” iperteso: iperteso: metanalisi di trial in doppio ciecometanalisi di trial in doppio cieco
Gueyffier F et al., Lancet 1999; 353:793

Placebo
Placebo
+ Placebo+ Placebo
Indapamide SR 1.5 mg
+ Perindopril 2 mg
+ Perindopril 4 mg
M-2 M-1 M0 M3 M6 M9 M12 M18 M24 M60
The Trial:International, multi-centre, randomised double-blind placebo controlled
Inclusion Criteria: Exclusion Criteria:Aged 80 or more, Standing SBP < 140mmHgSystolic BP; 160 -199mmHg Stroke in last 6 months+ diastolic BP; <110 mmHg, DementiaInformed consent Need daily nursing care
Primary Endpoint:All strokes (fatal and non-fatal)
Target blood pressure150/80 mmHg

- Campione direttamente derivato da una popolazione ‘reale’ non selezionata di anziani fragili
- Outcome geriatrici
- Monitoraggio dei pazienti Costante
- Evidenze direttamente applicabili alla pratica clinica.
Quale metodologia per il paziente complesso?Quale metodologia per il paziente complesso?

Soggetto anzianoCaratteristiche biologiche



0
50
100
150
200
250
2000 2001 2002 2003 2004 2005 2006 2007 2008
Pubblicazioni su "OMICS" and Elderly
Geriatrics and genetics Geriatrics and Molecular Biology Elderly and genomics
Elderly and proteomics Elderly and Metabolomic
Nuove tecnologie: Nuove tecnologie: ““OMICHEOMICHE”” e invecchiamentoe invecchiamento


Stover P.J. JADA 2008
Nutrient-genome interactions.Nutritional genomics encompasses both nutrigenetics, the influence of genetic variation on nutrient utilization/metabolism, food tolerances, and nutrient requirements; and nutrigenomics, the modulatory role of nutrients on genome evolution, mutation rate, in-utero viability, programming, and expression. In turn, several of the nutrigenomic outcomes (ie, genome evolution) contribute to the genetic variation observed within genetically diverse human populations.

Age (months) of mice
Young-adult age Ageing Very old age0 2 15 24
Accelerated switching on =death of aged
Delayed switching on =increased longevity IL-6
zinc availability
Genetic background
StressMTmRNA
gp130MTmRNA
(lamp)SUCCESSFUL AGING
IL-6(hand to press switch)
gp 130 (switch) Immune plasticity
(spring)= normal immune response
Absence of immune plasticity = immune decrement
Maintenance of immune plasticity =satisfactory immune plasticity
Zinc ion avalability
Immune plasticity, zinc ion availabiity and inflammation in ageiImmune plasticity, zinc ion availabiity and inflammation in ageing/succesful ageingng/succesful ageing
Mocchegiani et al. Exp. Gerontol. 2004

HEALTH YOUNG-ADULT
(Men) Age-range (30-40 yrs, n=30)
OLD (Men) Age-range (65-85 yrs, n=30)
NONAGENARIANS(Men) Age-range (90-97 yrs, n=20)
OLD INFECTED PATIENTS(Men) Age-range (65-83 yrs, n=20)
C+ (n=16) C- (n=14) C+(n=14) C-(n=16) C+(n=12) C-(n=8) C+(n=13) C-(n=7)
IL-6 (pg/ml) 0.7±0.03 1.00±0.2* 0.88±0.3 1.21±0.4* 0.77±0.5 1.43±0.7* 3.50±0.7 5.72±0.9*
NK cell activity
(L.U. 20/107) 78.1±8.7 68.7±7.3* 62.3±6.7 50.2±5.5* 73.4±5.7 58.1±6.5* 46.3±7.3 15.2±5.4*
IL-10 (pg/ml) 1.55±0.37 0.93±0.23* 1.50±0.25 0.61±1.84* 1.70±0.23 1.30±0.15* 1.60±0.26 1.40±0.12*
TNF-alpha (pg/ml) 0.65±0.14 0.95±0.21* 0.96±0.18 1.44±0.11* 0.58±0.15 1.32±0.14 2.50±0.12 3.67±0.16*
MTmRNA
MT-IIA/βactin 0.85±0.05 1.23±0.07* 2.12±0.7 3.13±0.8* 1.00±0.03 3.70±0.5* 3.37±0.08 4.23±0.03*
Zinc (µg/dl) 135±27 128.3±28.1* 82.2±7.7 77.5±6.4 80.4±8.7 72.2±7.4* 70.2±6.7 69.4±8.2*
Zinc ion
bioavailability
(ratio Total thymulin/
active thymulin)
1.00±0.02
2.00±0.03*
2.33±0.02
3.53±0.05*
1.33±0.02
2.03±0.05*
3.33±0.02
4.03±0.05*
p<0.01 as compared to C+ (paired Student’s t-test)
“C- carriers” were associated to increased IL-6 and decreased IL-10 production and to impaired peripheral immune efficiency, as well as, to altered zinc status
Immune and nutritional parameters in CImmune and nutritional parameters in C-- and C+ (ILand C+ (IL--6 gene promoter 6 gene promoter --174 G/C 174 G/C polymorphism) infected patients, in old and nonagenarian subjectpolymorphism) infected patients, in old and nonagenarian subjectss
Giacconi et al. Exp. Gerontol. 2004

C- C+ (BS) (PS) (BS) (PS)
Mean SD Mean SD Mean SD Mean SD Age (y) 74 7 - - 71 7 - -
Dietary intake of zinc (mg/day) 7.74 3.68 - - 8.56 2.51 - -
Plasma Zn (µM) 9.0 1.4 10.2* 1.8 8.7 1.5 10.5* 1.9 Zn/Alb .34 .06 .38* .07 .32 .05 .39* .06
RBC Zn (µM) 104 45 98 42 114 39 113 34 MT (MFI) 80.1 28.2 112.6* 53.7 78.3 22.8 105.1* 33.5
iZnL 1.25 .10 1.31* .11 1.27 .07 1.34* .13 iZnR .18 .08 .23* .10 .18 .05 .22* .09
MT/iZnR 583 361 398* 159 541 221 485 303 NK activity 17.7 6.5 24.9* 4.5 9.8 7.9 15.0* 8.8
GDS 2.8 2.8 2.5 2.5 3.7 3.2 2.7 2.3 PSS 17.5 7.5 14.8 7.8 14.1 6.1 13.0 6.7
MMSE 25.4 2.4 26.4 2.3 23.8 4.6 24.8 3.7 BS= before supplementation; PS= after supplementation; Zinc dose=10 mg/day for 48 days
Effect of zinc supplementation on zinc status, immune and psychoEffect of zinc supplementation on zinc status, immune and psychological parameters in logical parameters in old subjects with plasma zinc old subjects with plasma zinc ≤≤ 10.5 mM in dependence of IL10.5 mM in dependence of IL--6 6 --174 polymorphism174 polymorphism

Butler B. BMJ 2008
The most efficient approach to combating disease and disability is to pursue the means to modify the key risk factor that underlies them all – aging itself.


Contesto sociale
ed
Organizzativo

-
-
-
- - - - - - -0,7
0,8
0,9
1
100 300 500 700
Sopr
avvi
venz
a
Giorni
C. latino atteggiamento + C. latino atteggiamento –C. caucasico atteggiamento + C. caucasico atteggiamento -
Atteggiamento Caregiver e IstituzionalizzazioneAtteggiamento Caregiver e Istituzionalizzazione
JAGS 2004; 52: 1077-84

(% values, by country)
GreeceN=1014
ItalyN=990
UKN=995
SwedenN=921
PolandN=1000
GermanyN=1003
OverallN=5923
Family caregivers
Average age (years) 51,7 53,4 54,5 65,4 51,0 53,8 54,8
% females 80,9 77,1 75,4 72,0 76,0 76,1 76,3
Relationship: - child- spouse/partner
- other
55,417,127,5
60,910,928,2
31,622,845,6
40,548,111,4
51,118,230,7
53,418,428,2
48,922,228,9
Cared for older people
Average age (years) 79,5 82,0 78,0 81,3 78,6 79,7 79,8
% females 64,5 71,2 69,5 57,7 72,8 68,5 67,5
% living in care home 1,2 3,7 4,5 10,0 0,2 9,8 4,8
% severely dependent* 62,8 74,7 59,9 71,4 56,8 71,7 66,1
*: measured by a 6-item IADL-scale from the OARS assessment (Fillenbaum & Smyer, 1981) and dichotomized into two groups (low/moderate vs. severe dependency).
Sample characteristicsSample characteristics
EUROFAMCARE

Domicilio
ANZIANO
OspedaleDim. programmata
M.M.G.
UVG - VMD(Coordinatore del caso)
EleggibilePiano Ind. Ass.(UVG + M.M.G. )
ADI Day Hospital RSA
Bernabei et al, Br Med J 1998; 316:1348-51

DIPARTIMENTO MEDICINA INTERNA E GERIATRIA
U. OPERATIVA MEDICINA INTERNA Postacuzie
RiabilitazioneOrtopediaDay hospital
PRONTO SOCCORSO
No fragilità
A DOMICILIO
ANZIANO FRAGILE
Codice argento U. OPERATIVA GERIATRIA
MMG PUA +COORDINATORE CASO
ELEGGIBILEPIANO INDIVIDUALIZZATO
D’ASSISTENZAMMG + UVG + COORDINATORE CASOADI CENTRO DIURNO RSA
ANZIANO
Percorso assistenziale anziano / anziano fragilePercorso assistenziale anziano / anziano fragile

Paziente anziano
Soggetto anzianoCaratteristiche biologiche
Comorbilità
Trattamento farmacologico
Outcomes geriatrici
Contesto sociale
ed
Organizzativo

JAMA 2008
With the growing importance of health in the global agenda comes the responsibility to develop a scientific foundation of metrics and evaluation.The scope of this emerging field can be viewed in terms of key topics, including health outcomes, other social outcomes related to health systems, health services, resource inputs, evaluations of programmes and systems, and analysis to support policy choice.
Murray CJ, Lancet 2008; 371:1191-99
Health metrics and evaluation: strengthening the scienceHealth metrics and evaluation: strengthening the science


Aging and Technologies
Many enabling technologies could revolutionize the future health and social approach to complexity the
characterize ageing
Clinical epidemiology
Clinical pharmacology
Pharmacogenetics and pharmacogenommics
Clinical Research Organization
Public health
Robotics/Human AssistedRobots Assisting Humans
Other?





























