Embed Size (px)
Citation preview

Workshop DIN 2017 Peritoneaal dialyse
Landelijke trend Stellingen PROMS Casus
(potentiële) Belangenverstrengeling Geen
Voor bijeenkomst mogelijk relevante relaties met bedrijven -
• Sponsoring of onderzoeksgeld • Honorarium of andere (financiële)
vergoeding • Aandeelhouder • Andere relatie, namelijk
• Geen • Sprekersvergoeding
• Nvt • Nvt
Dialysis Initiatives Nefrologen 2017
Disclosure belangen C.W.H. de Fijter

Landelijke PD-ontwikkeling

Stelling 1
• De afname van PD in Nederland kent verschillende redenen, die vooral toe te schrijven zijn aan:
• Patiënt • Nefroloog • Infrastructuur • Uitkomst/complicaties
Stelling 2
• Minimaal 3-6 maanden is nodig om een patiënt goed voor te lichten over nierfunctievervangende therapie.

Stelling 3
• De startende nefroloog is beperkt geschoold in PD

NIO enquête parttime PD stage OLVG 6 maanden 1 dag per week
• 1. Eén dag per week PD stage elders vond ik zinvol, vanwege extra patiëntencontacten, en stimulerend door nieuwe gezichtspunten therapie/werkwijze/organisatie.
• 2. Expositie aan PD patiënten en problemen was ruim voldoende aanwezig en aanvulling op ervaring in eigen opleidingscentrum.
• 3. Follow-up van (poli)klinische patiënten en problemen: goed mogelijk ondanks parttime aanwezigheid op locatie.
• 4. Voor- en nadelen van PD alsmede complicaties zijn voldoende aan bod gekomen. Zeker. Bijdrage thuisbehandeling aan flexibiliteit / mogelijkheid te werken.
• 5. Ik voel mij in staat zelf PD kandidaten te werven, met PD te starten en de behandeling te monitoren. Meer capabel en zelfstandig.
• 6. Evaluatie stage in 1 woord of zin. Zeer nuttig, leerzaam en leuk. “geleerd hoe elegant PD behandeling is”; “gevoel gekregen voor waar grenzen liggen”; “stimulans om eigen standpunt te bepalen”

Samenvatting NIO-dag PD april 2017
N = 37
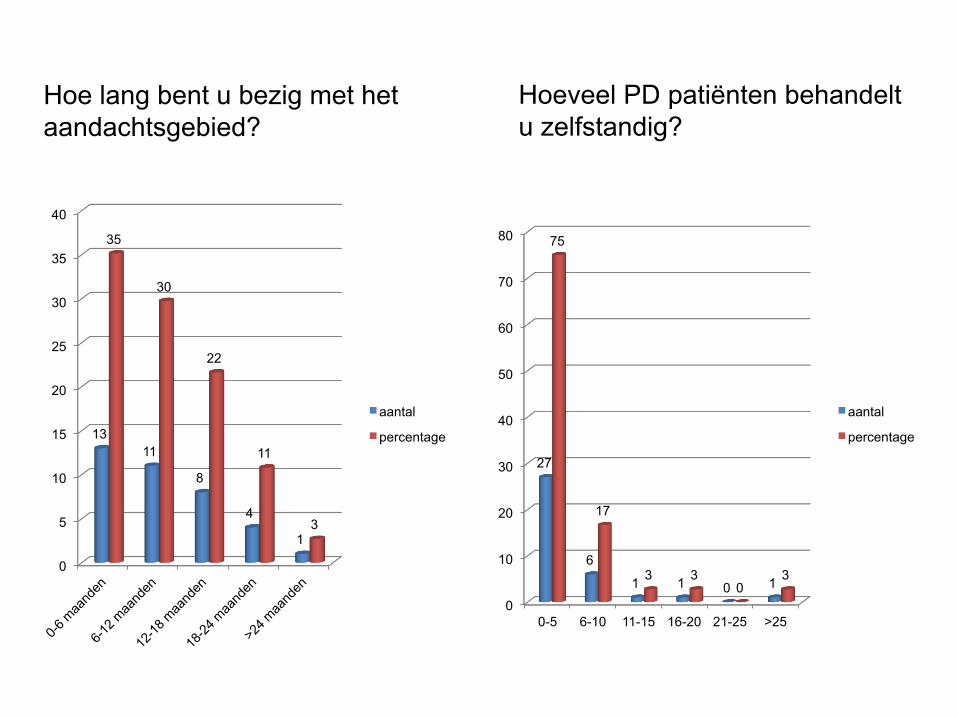
Hoe lang bent u bezig met het aandachtsgebied?
0
5
10
15
20
25
30
35
40
13 11
8
4
1
35
30
22
11
3
aantal
percentage
Hoeveel PD patiënten behandelt u zelfstandig?
0
10
20
30
40
50
60
70
80
0-5 6-10 11-15 16-20 21-25 >25
27
6
1 1 0 1
75
17
3 3 0
3
aantal
percentage

Hoeveel PD patiënten worden er in uw centrum behandeld?
Is er voldoende PD expertise in uw centrum?
0
10
20
30
40
50
60
70
80
90
ja nee anders
32
2 3
86
5 8
aantal
percentage
0
5
10
15
20
25
30
0-5 6-10 11-15 16-20 21-25 >25 ?
5
3 2
9
5
10
3
14
8
5
24
14
27
8
aantal
percentage

Is er een aparte PD stage?
0
5
10
15
20
25
30
35
40
13 11
8
4
1
35
30
22
11
3
aantal
percentage
Wordt er voldoende aandacht besteed aan PD tijdens uw opleiding?
0
5
10
15
20
25
30
35
40
45
50
ja nee anders
18
13
6
49
35
16
aantal
percentage
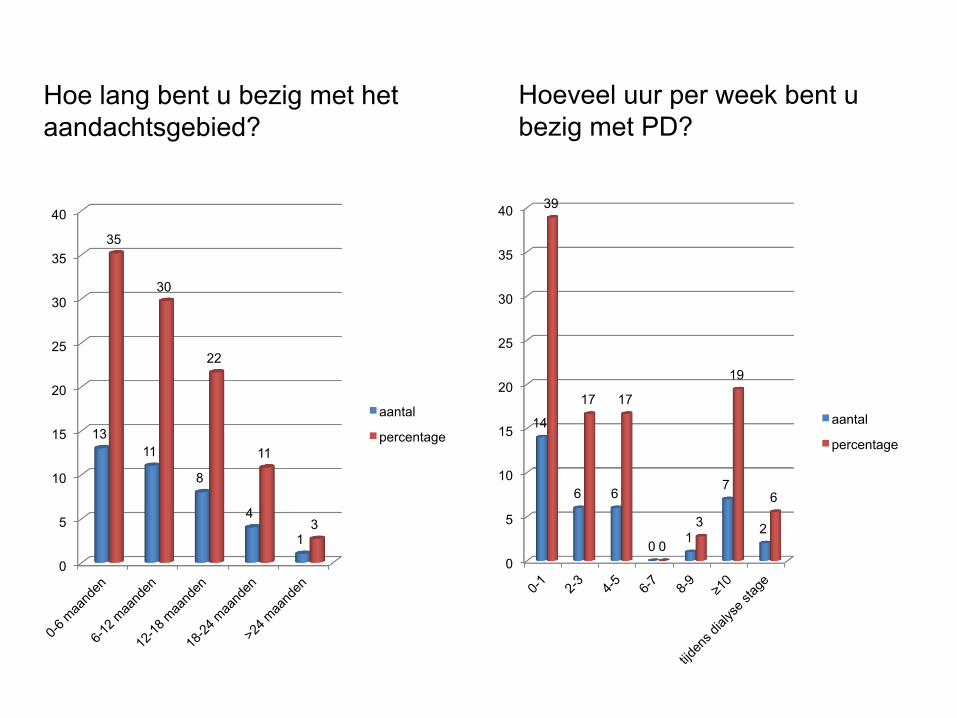
Hoe lang bent u bezig met het aandachtsgebied?
0
5
10
15
20
25
30
35
40
13 11
8
4
1
35
30
22
11
3
aantal
percentage
Hoeveel uur per week bent u bezig met PD?
0
5
10
15
20
25
30
35
40
14
6 6
0 1
7
2
39
17 17
0
3
19
6
aantal
percentage

Stellingen over PD vs HD
0 10 20 30 40 50 60 70 80 90
100
eens oneens geen mening
0
37
0 0
100
0 0
10 20 30 40 50 60 70 80
eens oneens ligt aan type patient
28
8 1
76
22
3
0
10
20
30
40
50
60
eens oneens anders
12 20
5
32
54
14
PD is een inferieure behandeling tov centrum HD
PD is een gelijkwaardige behandeling t.o.v. centrum HD
PD is een betere behandeling t.o.v. centrum HD

Wat mist u tijdens uw opleiding m.b.t. PD?
Transitie predialyse -> PD PD overbrugging naar Tx Stage Praktijkervaring Betrokkenheid plaatsing katheter Structureel onderwijs Theoretische achtergrond
Hands-on ervaring Betrokkenheid meerdere nefrologen Patiënten Onderwijs PD poli mag vaker Structurele begeleiding
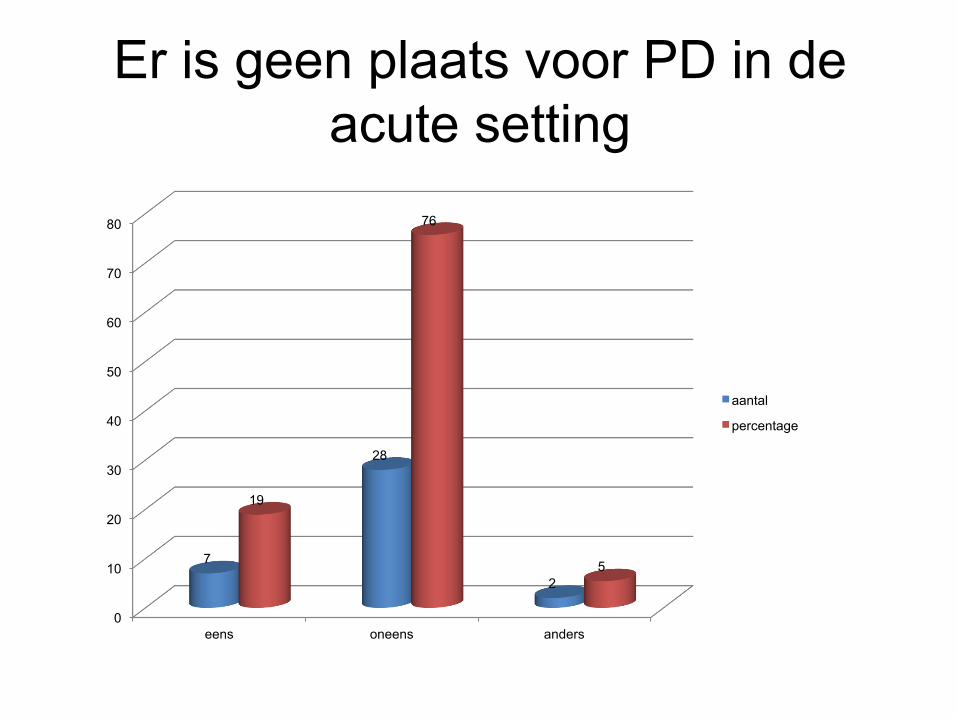
Er is geen plaats voor PD in de acute setting
0
10
20
30
40
50
60
70
80
eens oneens anders
7
28
2
19
76
5
aantal
percentage

Welcoming patients to the floor: PROMs HD vs PD in OLVG Oost
• About 40% of patients is durably treated with peritoneal dialysis in our teaching hospital.
• Patient’s perspectives were studied by patient reported outcome measurements (PROMs) to find out why the generally reported decline in the use of PD hardly occurred in our facility.

PROMs - Methods
• All 75 prevalent adult dialysis patients (HD duration 27, PD 16 months) were included. All had received predialysis care and education for > 6 months.
• Cross-sectional sociodemographic and clinical data*,
SF-36, KDQOL-SF, frailty and predialysis anxiety/depression scores were collected in February 2016.
• Differences in PROMs between PD and HD patients were analyzed.
• *including age, sex, ethnicity, primary kidney disease, comorbidity, residual renal function [rGFR, urine production], body mass index (BMI), dialysis modality, time on dialysis, erythropoietin use, and subjective global assessment (SGA).

Herkomst patiënten
Nederland 46%
Suriname 20%
Antillen 3%
Marokko 3%
Turkije 6%
China 3%
Filippijnen 3%
Pakistan 3%
Egypte 3%
Chili 3%
Italie 3%
Luxemburg 3%
Oekraine 3%
Nederland 21%
Suriname 36%
Antillen 4%
Marokko 11%
Turkije 15%
Filippijnen 2%
Egypte 2%
Eritrea 2%
Armenie 2%
Senegal 2%
Sierra Leone 2%
PD
HD

PD (n=33)
HD (n=42)
p-value
Age 66 ± 14 66 ± 11 0.89 Aged > 80 years (n(%)) 7(21) 4(10) 0.16 Male (n(%)) 9(27) 27(64) 0.44 Ethnicity (n(%)) Caucasian Afro-American Asian
21(64) 9(27) 3(9)
17(40) 23(55)
2(5)
0.06
Born in the Netherlands (n(%))
16(48) 11(24) 0.08
Primary kidney disease (n(%)) Diabetic nephropathy Glomerulonephritis Renal vascular disease ADPKD Others
13(40) 4(12) 11(33) 2(6) 3(9)
16(38) 1(2)
15(36) 2(5)
8(19)
0.41
Diabetes Mellitus (n(%)) 14(42) 19(45) 0.81 Davies comorbidity score None Intermediate High
3(9)
13(39) 17(52)
13(31) 17(40) 12(29)
0.04
BMI (kg/m2) 29.9 ± 7.2
27.6 ± 6.2
0.15
Patient characteristics. Mean values +/- SD or median values (interquartile range), depending on the distribution.

PD (n=33)
HD (n=42)
p-value
nPNA (g/kg/day) 1.1 ± 0.1 1.1 ± 0.2 0.26 Erythropoietin use (n(%)) 18(55) 42(100) 0.00 Anuric patients (n(%)) 6(18) 22(52) <0.001 Urine production in non anuric patients ml/24u
919 ± 573
1121 ± 556
0.23
rGFR in non-anuric patients (ml/min)
5.0 ± 2.2 4.1 ± 2.6 0.21
Hemoglobin (g/dl) 11.4 ± 0.7
10.9 ± 0.8 0.09
Parathyroid hormone (pmol/l)
27.5 ± 16.7
30.1 ± 17.3
0.53
Serum albumin (g/l) 37.5 ± 4.5
39.6 ± 4.2 0.05
Dialysis Kt/Vurea* 2.0 ± 0.4 1.4 ± 0.3 Months on dialysis
16 (10-34)
27 (12-57)
0.06
HADS score (n of returned forms) Anxiety Depression HADS score > 12 (n(%))
28 5.5 ± 3.9 6.6 ± 4.4 12.0 ±
7.7 12(43)
29 8.4 ± 3.8 7.7 ± 4.9
16.1 ± 8.1 20(69)
0.01 0.36 0.06 0.03
CSHA frailty score Living alone (n(%))
3.9 + 1.1 9(27)
3.7 + 1.0 16(38)
0.13 0.37

SF-36 en KDQoL: gemiddelde + SD score op fysiek, mentaal en sociaal gebied van de HD- en PD-patiënten uit het OLVG
Bodily pain 58 ± 25 45 ± 29 0.05
PD HD p-value Short Form 36
KDQOL
Symptoms/problems 71 ± 16 64 ± 15 0.05
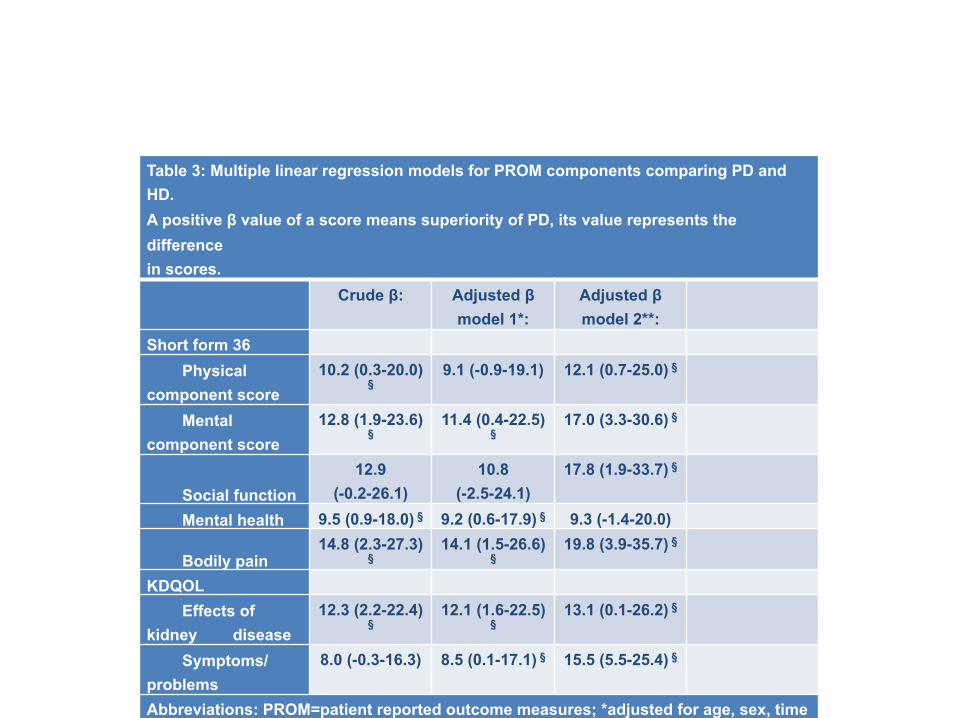
Table 3: Multiple linear regression models for PROM components comparing PD and HD. A positive β value of a score means superiority of PD, its value represents the difference in scores. Crude β: Adjusted β
model 1*: Adjusted β model 2**:
Short form 36 Physical component score
10.2 (0.3-20.0) §
9.1 (-0.9-19.1) 12.1 (0.7-25.0) §
Mental component score
12.8 (1.9-23.6) §
11.4 (0.4-22.5) §
17.0 (3.3-30.6) §
Social function 12.9
(-0.2-26.1) 10.8
(-2.5-24.1) 17.8 (1.9-33.7) §
Mental health 9.5 (0.9-18.0) § 9.2 (0.6-17.9) § 9.3 (-1.4-20.0)
Bodily pain 14.8 (2.3-27.3)
§ 14.1 (1.5-26.6)
§ 19.8 (3.9-35.7) §
KDQOL Effects of kidney disease
12.3 (2.2-22.4) §
12.1 (1.6-22.5) §
13.1 (0.1-26.2) §
Symptoms/problems
8.0 (-0.3-16.3) 8.5 (0.1-17.1) § 15.5 (5.5-25.4) §
Abbreviations: PROM=patient reported outcome measures; *adjusted for age, sex, time on dialysis; **+ born in the Netherlands, Davies comorbidity score, anuria, diabetes mellitus;§p<0.05.

PROMs – Results - summary
• Despite more comorbidity in the PD population, generally used dialysis parameters were adequate and similar between HD (n=42) and PD (n=33) patients as was annual mortality (13 vs 11%).
• Many factors associated with a predialysis modality choice for PD were absent.
• A higher anxiety/depression score was found in pre-HD compared to pre-PD patients.
• PROMs were returned by 97%. • PD patients performed better on a number of PROMS
than their HD mates.

PROMs - Conclusion
• Single center cross-section with a low number of patients but an almost 100% patient response shows that having a high% of patients on PD is possible with excellent results in terms of patient reported outcomes.
• A structured patient education with attention for personal needs of patients, an adequate infrastructure for PD and a dedicated team with ongoing patient support are key factors.
• Sharing best practices may help to slow down or even reverse the decline of PD which is a pity both for patients and society.

Casus gecompliceerde SLE
• Mw M 52 jaar • 2003 NS t.g.v. SLE nefritis V, complicatie: v. porta
trombose - P/aza: goede respons; leverbx: verstoorde microcirkulatie
• 2013 Recidiverend hematemesis en ascites - TIPS/chirurgie onmogelijk: frequent RBL varices, diuretica,
ascitesdrainage, albumine iv - Opname 16x, a 2 wk, nierfunctie stapsgewijs naar 12%,
Karnofsky score drastisch omlaag naar 20-30

Casus SLE
• Physical examination: - RR 130/80 mmHg, tense ascites with collateral circulation reflected in abdominal
wall veins.
• Lab: - normal liver function and enzymes, creatinine 5.7 mg/dl, urea 70 mg/dl. ECC 12 ml/
min, proteinuria of 0.5 g/24 h. - Serum albumin was 37 g/l, ascites albumin 9 g/l, SAAG 28 g/l. Ascites white blood
count 0.1 x 10e9/l.
• Abdominal echography: - portal vein thrombosis with collateral vasculature, a hepatopetal flow and ascites.
• Endoscopy: - bleeding varices, treated by multiple banding sessions.
• Echocardiography: - no cardiac failure or cardiac inflow obstruction.

…refractory ascites, the need for frequent large volume paracenteses, deteriorating renal function with uremia, trombocytosis & activated clotting cascade, low quality of life and frequent hospitalisation due to relapsing overt hematemesis with hypotension….
• Nephrological management challenge - CVVH w regional citrate: not (cost-effective) for the long run. - HDF w/wo anticoagulant? Frequent hypotension - PD?
. No evidence based solution!

PD as last resort?
• After drainage of ascites a Swan-neck Tenckhoff catheter was laparoscopically placed without complications.
• Initially, drainage of the ascites was started and gradually PD fluid was introduced to achieve a negative fluid balance.
• No episodes of hypotension or peritoneal fluid leakage were observed.
• CAPD: 4 x 1,5L 1,36% glucose
The following years…
• no peritonitis or other PD-related complications. • no episodes of oedema, and she presented less frequently
with bleeding episodes.
• Endoscopic studies showed diminishing gastric and oesophageal varices.
• Liver function tests remained normal. Salbumin 37 g/l. • At present, a residual diuresis of 1100 ml, a renal creatinine
clearance of 7 ml/min, Kt/V of 2.2.

The following years…
• Hospitalisation rate decreased tremendously (from 55 days/ year in the year prior to PD to 14 and 0 days/year in the two consecutive years with CAPD, respectively).
• Her clinical condition as well as her quality of life increased favourably (Karnofsky score improved from 20-30 to 70). At present she feels well.
• PD appears cost-effective with respect to hospitalisation rate, morbidity and quality of life.

Casus PD as last resort?
• Hr D 61yr, ESRD due to DM2 • 2002 IHD 3x/week • 2006 collaps, hypoxemia: CT no pulmonary embolism but
pericardial & pleural effusion; ascites, hypalbuminemia, hypotension.
• Kt/V 1,3; daily haemodialysis and isolated ultrafiltration were necessary because of overhydration.
• Echocardiography revealed a good left and right ventricular function, no valve abnormalities, and pericardial effusion of 1 cm all around without inflow obstruction.

• The ascites was a straw-coloured exudate, had a white blood cell count of 0.1 x 109/l and a SAAG of 1 g/l.
• Ascites culture and cytology were negative, including a polymerase chain reaction for typical and atypical mycobacteria.
• Liver function tests, iron studies, thyroid-stimulating hormone, and parathyroid hormone were normal.
• No evidence was found of portal hypertension, cardiac or pericardial disease, peritoneal infection or malignancy.






























