Embed Size (px)
Citation preview
18. Brunot B, Petras 5, Germain P. Vinee P. Constantinesco A. Biopsy and quantitativehepatobiliary scintigraphy in evaluation of liver transplantation. J NucI Med 1994;35:1321—1327.
19. Daniel GB, Bright RM, Monnet E, Ollis P. Comparison of per-rectal portal scintigraphy using @“technetiumpertechnetate to mesenteric injection of radioactive microspheres for quantification of portosystemic shunts in an experimental dog model. VetRadiol Ultrasound I990;3 1:I75—181.
20. Susumu 5, Kuroki T, Kurai 0, et al. Portal circulation by technetium-99m pertechnetate per-rectal portal scintigraphy. J NucI Med 1988;29:460—465.
21. Daniel GB, Bright RM, Ollis P. Shull R. Per rectal portal scintigraphy using @“Tcpertechnetate to diagnosis portosystemic shunts in dogs and cats. J Vet Intern Med1991;5:23—27.
22. Fritzberg AR. Advances in the development ofhepatobiliary radiopharmaceuticals. In:Fritzberg AR, ed. Radiopharmaceuticals: progress and clinical perspectives. BocaRaton, FL: CRC Press; 1986:90—I16.
23. Loberg MD, Cooper M, Harvey E. Development ofnew radiopharmaceutical based onN-substitution of iminodiacetic acid. J Nuci Med l976;17:633—638.
24. Loberg MD, Fields AT. Chemical structures of@―Tc-labeled N-(2,6-dimethylphenylcarbamoylmethyl) iminodiacetic acid (Tc-HIDA). mt J AppI Radiat iso 1978;29: I67—173.
25. O'Connor KW, Snodgrass PJ, Swonder JE, et al. A blinded prospective studycomparing four current noninvasive approaches in the differential diagnosis of medicalversus surgical jaundice. Gastroenterology I983;84: 1498—1504.
26. Center SA. Pathophysiology. laboratory diagnosis and diseases ofthe liver. In: EttingerSi, Feldman EC, eds. Textbook ofveterinary internal medicine, disease ofihe dog andcat. Philadelphia: WB Saunders; l995;1261—l3l2.
27. Feldman BF. Clinical pathology of the liver. In: Kirk RW, ed. Current veterinarytherapy VI!!. Philadelphia: WB Saunders; 1980:875—885.
28. Klingensmith wC, Fritzberg AR, Spitzer VM, Kuni CC, Williamson MR. Gerhold JP.Work in progress: clinical evaluation of c9mTc1@[email protected] 9'@―Tcdiisopropyl-IDA for hepatobiliary imaging. Radiology 1997; 146:181—184.
29. Nunn AD, Loberg MD, Conley RA. A structure-distribution relationship approachleading to the development of @‘@‘Tc-mebrofenin:an improved cholescintigraphicagent. J NucI Med l983;24:423—430.
30. Winograd H, Lorgue G, Keister DM. Thiacetarsamide toxicity in the normal dog. In:Soil MD, Coleman MW, Courtney CH, Jackson RF, Keough Ri, Knight DH, eds.Proceeding of the heartworm sYmposium 92. Batavia, IL: American HeartwormSociety; 1992:215—222.
3 1. Zimmerman HJ. Hepatotoxicity. New York: Appleton-Century-Crofts; 1978:47—90.
phaticopelvic fistulization, skipping of lymphatic chain, patency of thoracic duct and abnormal leg lymphatics (1—3).However, it requires tedious cannulation of lymphatics, isinvasive and is not readily reproducible. It also can result inlocal tissue necrosis, fat embolism to the lungs, hypersensitivityreaction and exacerbation of lymphedema by the contrastmaterial (4). Lymphoscintigraphy using 99mTc@sulfurmicrocolbid, antimony sulfide colloid, stannous phytate, rhenium sulfurcolloid, human serum albumin or dextran delineates the patternof lymphatic drainage, is fast and nontraumatic and has noknown side effects (5—6). Use of lymphoscintigraphy in investigating chyluna, chyloperitoneum and chylothorax has beenlimited to a few case reports (7—13). We retrospectivelyanalyzed lymphoscintigraphic studies to determine their efficacy in the investigation of chyluria, chyloperitoneum andchylothorax.
MATERIALS AND METhODSBetween June 1989 and May 1996, lymphoscintigraphy was
performed on 18 patients with chyluria (9 women, 2 men), chyluriaand chyloperitoneum (2 men), chyloperitoneum and chylothorax (3women, 2 men). Follow-up scans were obtained on 3 patients,giving a total of 21 lymphoscintigraphic studies. The averagepatient age was 38.0 yr (range 25—57yr), and average duration ofsymptoms was 4.7 yr (range 3 mo to 36 yr) for chyluna and 6.0 mo(range 10 days to 18 mo) for chyloperitoneum and chylothorax.Elephantiasis of the lower extremities was the most commonassociated symptom. Other associated symptoms and signs included hematuria, flank pain, dysuria, urinary frequency, oliguria,weight loss, fever, cough, anasarca, chest discomfort, dyspnea andenlarged inguinal lymph nodes. A previous history of filariasis wasknown in 7 of 13 patients with chyluria. Urine, peritoneal, pleuralor pericardial fluid were positive for fat droplets after Sudanstaining and negative for acid-fast bacilli, culture and cytology inall patients. Repeated thick-film night blood smears were alsonegative for microfilaria in all patients. Final diagnoses were made
Lymphoscintigraphy allows functional assessment of lymphatictransport and depiction of regional @,mphnodes, is fast and nontraumatic and has no known side effects. We retrospectively analyzed lymphoscintigraphic studies to determine their efficacy in theinvestigation of chyluria, chyloperitoneum and chylothorax. Methods: Twenty-one whole-body lymphoscintigrams using @rc-antimony sutilde colloki or dextran were acquired in 18 patients withchyluria, chyloperitoneum and/or chylothorax. The images werereviewed to assess the rate of tracer transport and number, size anddistributionof lymph vessels and nodes as well as the presence ofcollateral, fistula or lymph reflux. Results Lymphoscintigraphy wasnormal (5 of 11 patients) or showed lymphatic obstruction (6 of 11patients) in chyluria associated with filariasis. Lymphatic obstructionwas demonstrated in ch@rioperftoneumand/or chylothorax associated with liver cirrhosis (2 patients), postoperative (1 patient) orcongenital (1 patient) lymphatic dysplasia, inferior vena cava obstruction (1 patient) and nephrotic syndrome (1 patient). Enhancedlymph flow was seen in systemic lupus erythematosus (1 patient).Follow-up lymphoscintigrams showed patency of lymphovenousanastomosis (1 patient), improvement (1 patient) or no change (1patient) in lymphatic drainage aftertreatment. Conclusion: Lymphoscintigraphy can demonstrate abnormal lymphatic drainage in chyluria, chyloperitoneum and chybthorax. It is useful for selectingpatients for surgery and assessing the effect of treatment.Key Words chyluria; chyloperitoneum; chylothorax; lymphoscintigraphy
J Nucl Med I998 39.1292-1296
L ymphangiographyhasbeenthemainimagingmodalityininvestigating chyluria, chyloperitoneum and chylothorax. It isuseful for detecting abnormal retroperitoneal lymph nodes,leakage from dilated lymphatics, lymphoperitoneal and lym
ReceivedJun. 23, 1997;accepted Sep. 3, 1997.For correspondence or reprints contact: Margaret H. Pul, MD, Department of
RadlObgy, Ago Khan Un@ersftyMedical center, Stadium Rd., P0 Box 3500, Karachi74800, Pakistan.
1292 THEJOURNALOFNUCLEARMEDICINE•Vol. 39 . No. 7 •July 1998
Lympho scintigraphy in Chyluria, Chyloperitoneumand ChylothoraxMargaret H. Pui and Tian-Chao YuehDepartment ofNuclear Medicine, First Affiliated Hospital ofSun Yat-Sen University ofMedical Sciences, Guangzhou,People ‘sRepublic of China
by on April 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from
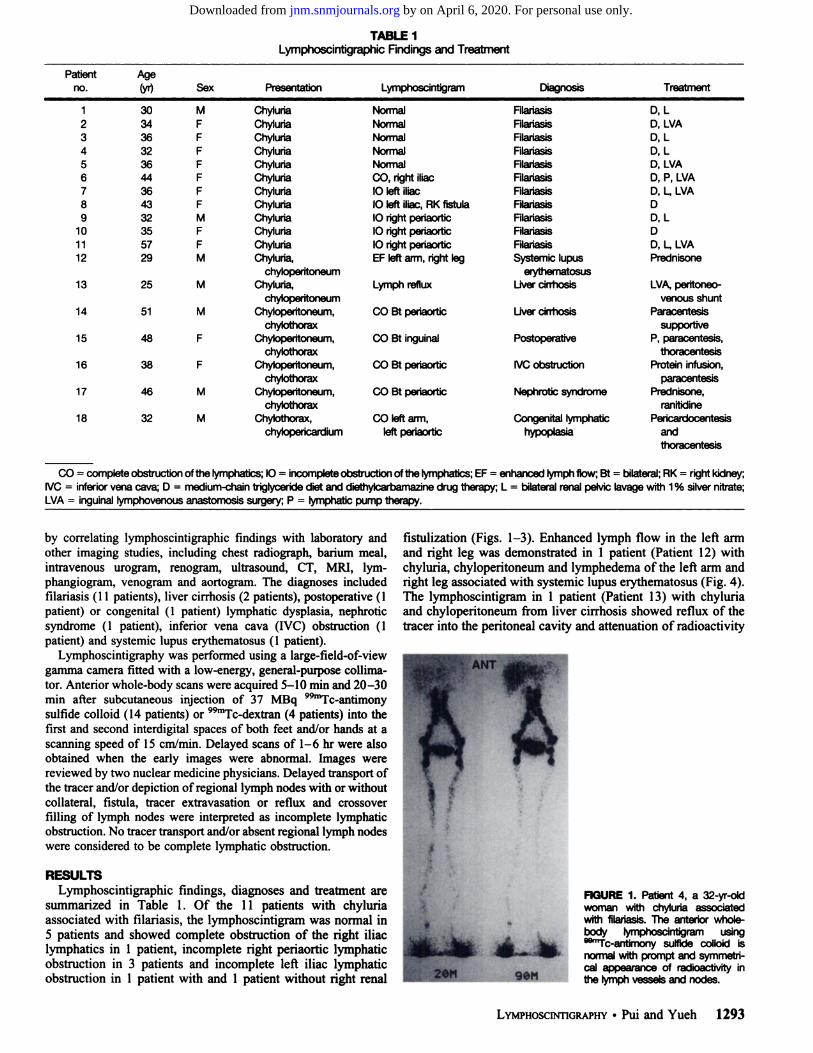
PatientAgeno.(yr)Sex Presentation Lymphoscintigram Diagnosis Treatment
CO = completeobstruclion ofthe lyrnphatics; 10 = incompleteobstruction ofthe lymphatics; EF = enhanced lyrnphflow, Bt = bilateral; AK= nght kidney;IVC= inferiorvena cava 0 = medium-chalntriglyceridediet and diethylcarbamazinedrug therapy L = bilateralrenalpeMc lavagewith1% silvernftrate;LVA= inguinaltymphovenousanastomosis surgery P = lymphaticpump therapy.
TABLE ILymphoscintigraphic Findings and Treatment
1 30 M Ch@,1uria2 34 F Chyluna3 36 F Chyluria4 32 F Chyluria5 36 F Chyluria6 44 F Chyluna7 36 F Chyluria8 43 F Chyluria9 32 M Chyluria
10 35 F Chyluria11 57 F Chyluria12 29 M Chyluna,
chybperftoneum13 25 M Chyluria,
chyicperftoneum14 51 M Chyloperftoneum,
chylothorax15 48 F Chyloperitoneum,
ChylOthOraX16 38 F Chyloperitoneum,
chylothorax17 46 M Chylopeiltoneum,
chylothorax18 32 M Chylothorax,
chylopericardium
NormalNormalNormalNormalNormalGo,nghtillac10 leftillac10 leftlIlac,AKfistula10 nght periaortic
10nghtperiaorticl0 nghtperi@rt@cEF left arm, nght leg
Lymphreflux
COBt periaor@c
CO Bt inguinal
COBtperiaortic
COBtperiaortic
CO left arm,left@
FdariasisFilañasisFilariasisFilariasisFilariasisAlariasisFilariasisFilaiiasisFilariasisAlailasisFilaiiasisSystemic lupus
e@osusLivercirrhosis
Uver @nhosis
Postoperative
wC obstruction
Nephrotic @me
Congenital lymphatichypu@
0, LD, LVA
D, L
D,LD, LVA
0, P. LVA
0, L LVA0
0, L00, L LVAPrednisone
LVA, peritoneo
venous shuntParacentesis
supportiveP. paracentesis,
thoracentesisProtsin infusion,
paracentesisPrednisone,
ranitidinePericardocentesis
andthoracentes@
by correlating lymphoscintigraphic fmdings with laboratory andother imaging studies, including chest radiograph, barium meal,intravenous urogram, renogram, ultrasound, CT, Mill, lymphangiogram, venogram and aortogram. The diagnoses includedfilariasis (1 1 patients), liver cirrhosis (2 patients), postoperative (1patient) or congenital (1 patient) lymphatic dysplasia, nephroticsyndrome (1 patient), inferior vena cava (NC) obstruction (1patient) and systemic lupus erythematosus (1 patient).
Lymphoscintigraphy was performed using a large-field-of-viewgamma camera fitted with a low-energy, general-purpose collimator. Anterior whole-body scans were acquired 5—10mm and 20—30mm after subcutaneous injection of 37 MBq 9@―Tc-antimonysulfide colloid (14 patients) or 9@Tc-dextran (4 patients) into thefirst and second interdigital spaces of both feet and/or hands at ascanning speed of 15 cm/mm. Delayed scans of 1—6hr were alsoobtained when the early images were abnormal. Images werereviewed by two nuclear medicine physicians. Delayed transport ofthe tracerand/or depiction ofregional lymph nodes with or withoutcollateral, fistula, tracer extravasation or reflux and crossoverfilling of lymph nodes were interpreted as incomplete lymphaticobstruction. No tracer transport and/or absent regional lymph nodeswere considered to be complete lymphatic obstruction.
RESULTSLymphoscintigraphic findings, diagnoses and treatment are
summarized in Table 1. Of the 11 patients with chyluriaassociated with filariasis, the lymphoscintigram was normal in5 patients and showed complete obstruction of the right iliaclymphatics in 1 patient, incomplete right periaortic lymphaticobstruction in 3 patients and incomplete left iliac lymphaticobstruction in 1 patient with and 1 patient without right renal
fistulization (Figs. 1—3).Enhanced lymph flow in the left armand right leg was demonstrated in 1 patient (Patient 12) withchyluria, chyloperitoneum and lymphedema of the left arm andright leg associated with systemic lupus erythematosus (Fig. 4).The lymphoscintigram in 1 patient (Patient 13) with chyluriaand chyloperitoneum from liver cirrhosis showed reflux of thetracer into the peritoneal cavity and attenuation of radioactivity
4
.@ S.
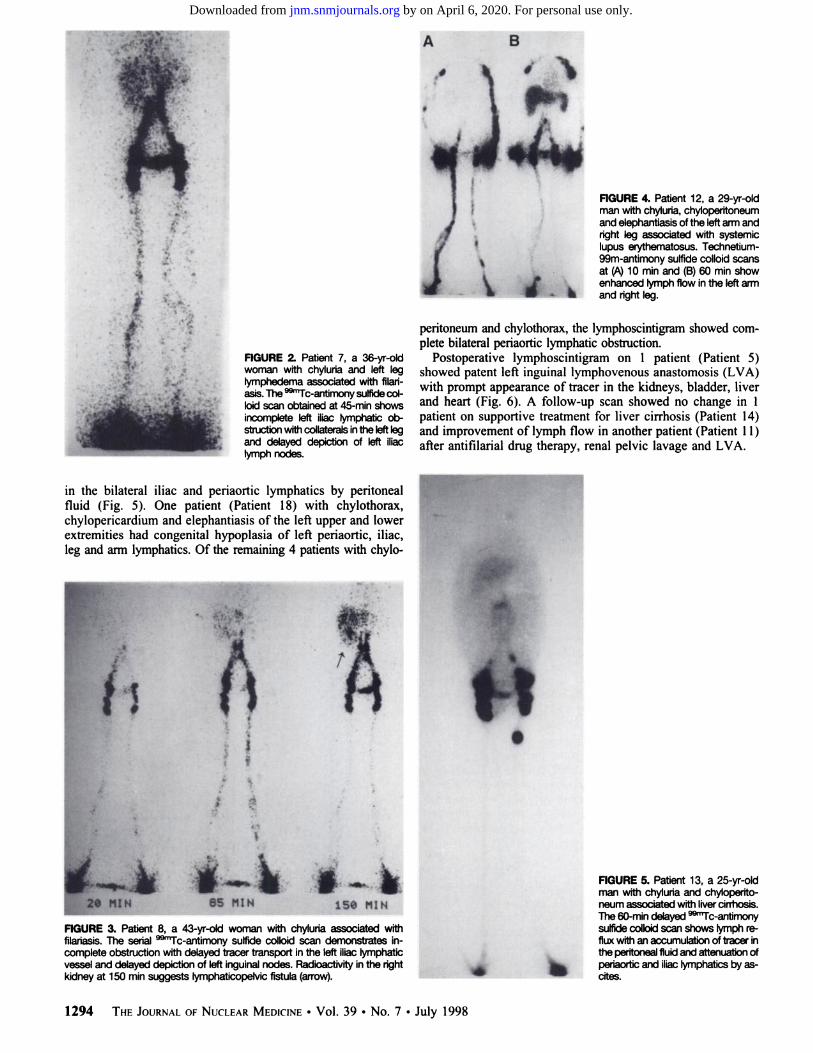
FIGURE1. Patient 4, a 32-yr-oldwoman with chylUna associatedwith filariasis.The anterior wholebody lymphosolntigram usingssmTc@antimony sulfide colloid isnormal with prompt and symmetrical appearance of radioactivity inthe lymph vesseLs and nodes.
LYMPHOSCINTIGRAPHY •Pui and Yueh 1293
by on April 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from
A B
IV.
FIGURE4. Patient12,a 29-yr-oldman withchyluria,chyloperitoneumand elephantiasisofthe leftarmandnght leg associated with systemiclupus erythematosus. Technetium99m-antimonysulfidecolloidscansat (A)10 mm and (B)60 mm showenhanced lymphflowinthe leftarmand rightleg.
peritoneum and chylothorax, the lymphoscintigram showed complete bilateral periaortic lymphatic obstruction.
Postoperative lymphoscintigram on 1 patient (Patient 5)showed patent left inguinal lymphovenous anastomosis (LVA)with prompt appearance of tracer in the kidneys, bladder, liverand heart (Fig. 6). A follow-up scan showed no change in 1patient on supportive treatment for liver cirrhosis (Patient 14)and improvement of lymph flow in another patient (Patient 11)after antifilarial drug therapy, renal pelvic lavage and LVA.
FIGURE5. Patient 13, a 25-yr-oldman with chyluna and chyloperitoneumassociated withlivercirrhosis.The 60-mm delayed @‘Tc-antimonysulfide coflokiscan shows lymph refluxwithan accumulationoftracer in
. the peritoneal fluid and attenuation of
@ perisortic and iliaclymphatics by ascites.
I
C
FIGURE2. Patient7, a 36-yr-oldwoman with chyluna and left leglymphedemaassociated withfilalasia. The @“Tc-antimonysulfidecolk@dscan obtained at 45-mm showsincomplete left iliac lymphaticobstruction withcollaterals inthe leftlegand delayed depiction of left iliac
@mphnodes.
in the bilateral iliac and periaortic lymphatics by peritonealfluid (Fig. 5). One patient (Patient 18) with chylothorax,chylopericardium and elephantiasis of the left upper and lowerextremities had congenital hypoplasia of left periaortic, iliac,leg and arm lymphatics. Of the remaining 4 patients with chylo
“I
,4@.@
@ NIH •5MIN 15SPuNFIGUREa Patient8, a 43-yr-oldwomanwithchyluriaassociatedwithfilariasis.The serial @rc-antimonysulfideCOIIOidscan demonstrates incomplete obstructionwithdelayed tracer transport inthe leftiliaclymphaticvessel and delayed depiction of left inguinal nodes. Radioactivity in the nghtkidneyat 150 mmsuggests IymphaticopeMcfistula(arrow).
ff1O
1294 THEJOURNALOFNUCLEARMEDICINE•Vol. 39 •No. 7 . July 1998
-@ .i@
by on April 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from

dextran. Although the thoracic duct was not demonstrated, theleft supraclavicular node was usually seen.
Chyluria may present as chylous clot, chylous clot retention,hematuria, flank pain, dysuria, weakness, fever and weight loss.There is a high content of fat, albumin and fibrin and a varyingamount of erythrocytes in the urine. The total fat content isrelated to diet, phase of digestion, posture and exercise. Hypolipidemia, hypoproteinemia, iron deficiency anemia, malnutrition and abnormalities of the immune system can occur as aresult of the disrupted fat, protein and blood metabolism.Elephantiasis may also be associated. Chyluria is a late manifestation of filariasis, a parasitic infestation endemic in southeast Asia. Other associated conditions include repeated retropentoneal infection, especially tuberculosis, trauma, genitourinaiyor gastrointestinal tumors, malignancy of the thoracic duct andthyroid, ureteric stone, hydrocele, inguinal hernia and pregnancy. Filanasis is caused by Wuchereria bancrofli and Brugiamalayi parasites. The adult worm lives and reproduces inperipheral lymphatics, intermittently showering the bloodstream with microfilarial offspring. Extensive local damage tolymphatic truncal walls and regional lymph nodes is producedby the adult worm. Patients present with recurrent fever,axillary or inguinal lymphadenitis, acute or chronic lymphedema, hydrocele, chyluria and cyloperitoneum. Similar to otherinvestigators, we found lymphoscintigraphy to be useful forassessing the degree of lymphatic damage by showing delayedor absent lymph transport, dilatation of draining lymphaticswith dermal collateralization, tortuous bizarre deep lymphatics,intralymphatic valvular incompetence, lymph reflux and faintor absent lymph nodes (15). While abnormal lymphaticourmnarycommunication at the level of the kidney, ureter or bladder iswell shown on lymphangiogr@phy, it is more difficult to detecton scintigraphy because of dilution of the tracer in the bloodstream, uptake of the radioisotope in the liver, spleen andkidneys and poor camera resolution. Radioactivity in thekidneys and bladder from free pertechnetate and normal retention may be difficult to distinguish from lymph reflux (16). Weobserved right renal lymph reflux in only one patient withchyluria. The initial diagnosis offilariasis is based on laboratorycriteria using filaria-specific IgG and thick-film blood smear ofnight blood specimens for microfilariae. It has been shown thatasymptomatic infected persons invariably have circulating microfilariae, whereas patients who have clinical manifestationsand active filarial infection frequently have no detectablemicrofilaremia (1 7). None of the patients with chyluria associated with filariasis in our study had microfilaremia. The diagnosisof filariasis in these patients was based on a history of previousexposure, exclusion of other causes of chyluria and response toantifilarial therapy.
Chyloperitoneum and chylothorax result from interference oflymph flow at the base of the mesentery, cisterna chyli orthoracic duct caused by primary lymphatic dysplasia; infection,especially filariasis and tuberculosis; peritoneal dialysis; orlymphatic damage from neoplasm, surgery or radiation. Increased hydrodynamic pressure in the lymphatics causes backpressure with dilatation of lymph vessels, retrograde flow,collateralization and diffusion of vessel contents through wallsinto serous spaces or lumina, parenchyma or surfaces of organs.If the backpressure is severe enough or if there is structuraldisease of the lymphatics, vessel rupture occurs with freeleakage. In our study, abnormal lymphatic drainage in the formof enhanced lymph flow or lymphatic obstruction was detectedby lymphoscintigraphy in all patients with chylopentoneum andchylothorax. Chylopentoneum and chylothorax were present inone patient with IVC obstruction and two patients with liver
LYMPHOSCINTIGRAPHY •Pui and Yueh 1295
M
FIGURE6. Patient 5, a 36-yr-oldwoman with chyluria associated
@thfliariasis.Post@ lymphoscintigraphy using @Tc-antimonysulfidecolloiddemonstrates patentinguinallymphovenous anastomosis with rapid appearance of radioactivity in kidneys, bladder, liverandhea@
Of the 11 patients with chyluria associated with filariasis, 2responded to medium-chain triglyceride diet and drug treatmentwith diethylcarbamazine; 4 required additional bilateral renalpelvic lavage with 1% silver nitrate; inguinal LVA was performed in 5. One patient (Patient 13) with chyluria and massivelymph reflux into the peritoneal cavity on the lymphoscintigramdid not respond to peritoneovenous shunt and LVA. Specifictreatment of the primary disorder and/or supportive therapywith repeated therapeutic paracentesis and thoracentesis weregiven to the remaining 6 patients with chyloperitoneum andchylothorax.
DISCUSSION
Lymphoscintigraphy was first introduced in 1953 using‘98Au-colloid.Because of its high absorbed radiation at theinjection site, ‘98Auhas been replaced by @°Tc-colloid,humanserum albumin and dextran. Lymphoscintigraphy allows functional assessment of lymphatic transport and depiction ofregional lymph nodes. After the interstitially administeredtracer is taken up into the lymphatics, clearance and trapping ofcolloid in lymph nodes are dependent on particle size andfunctional status of the reticuloendothelial system. Less than35% of colloidal particles are absorbed in 24 hr and a delay ofseveral hours may be required to image draining nodes. Transport of dextran depends on diffusion, less on actual lymph flowand is accelerated by skeletal muscle and lymphatic contractions. Thus, total-body uptake of dextran is faster and greaterthan that of antimony sulfide colloid. In spite of rapid lymphnode uptake rates, total popliteal lymph node sequestration ofdextran has been shown to be significantly lower because of itsnoncolloidal nature and its instability. Dextran also can bypassreticuloendothelial activity of ilioinguinal nodes and enter fromthe lymphatic to venous system and increase backgroundradioactivity. Retropentoneal lymphatic trunks are sometimeswell depicted. Dilution of tracer and background activity in theheart, lungs and liver after tracer appears in blood precludesatisfactory intrathoracic definition (14). In our study, theperipheral, iliac and retropentoneal lymphatic vessels andnodes were well shown with both antimony sulfide colloid and
itit
by on April 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from

cirrhosis. A lymphoscintigram of one of the patients with chyloperitoneum from liver cirrhosis showed lymph reflux into theperitoneal cavity. IVC obstruction and postsinusoidal portalhypertension result in increased lymph flow through the thoracic duct from viscera due to venous stasis. Leakage of chylefrom the disrupted lymph vessels and fistulas causes chyloperitoneum and chylothorax. Lymphatic drainage and transdiaphragmatic movement of chylous peritoneal fluid through thepleuroperitoneal canal have been proposed as mechanisms inthe formation of chylothorax. Radioisotope migration speedmay be a clue for differentiating these two mechanisms, whichis more rapid in the presence ofa diaphragmatic defect (18,19).Chyloperitoneum occurs in 52% of nephrotic syndrome patients, possibly because ofbowel ischemia with resultant lactealleakage or malabsorption (20).
Treatment of chyluria, chyloperitoneum and chylothoraxincludes fat restriction or a medium-chain triglyceride dietbecause synthetic triglyceride is transported from the gutdirectly to the liver by the portal system and is not absorbed bythe lymphatics. Thus, formation of intestinal lymph and lymphflow through the thoracic duct are decreased, allowing thefistulas to seal off and the collaterals to open up. In more severecases of chyluria it may be necessary to (a) instill 0.5%—1%silver nitrate into the renal pelvis to induce chemical lymphangitis and fibrosis of the fistulas; (b) surgically disruptlymphaticourinary fistulas; and (c) perform renal decapsulation,LVA, renal autotransplant and nephrectomy (21). Lymphoscintigraphy can identify patent lymph vessels before surgery anddetermine the function of LVA after surgery. It is a suitablemethod of patient selection for surgery and follow-up (22).Paracentesis or peritoneovenous shunting may be effective incontrolling chyloperitoneum (23). Intermittent thoracentesis,closed-chest drainage, pleurodesis and surgical ligation of thethoracic duct below the leakage may also be useful in treatingchylothorax.
CONCLUSIONLymphoscintigraphy can demonstrate abnormal lymphatic
drainage in chyluria, chyloperitoneum and chylothorax. It isuseful for selecting patients for surgery and assessing the effectof treatment.
1296 THEJOURNALOFNUCLEARMEDICINE•Vol. 39 •No. 7 •July 1998
REFERENCES
1. Akisada M, Tarn S. Filarial chyluria in Japan. Radiology l968;90:3 11—317.2. Yu HH, Ngan H, Leong CH. Chyluria—a 10-year follow-up. Br] Urol I978;50:126—
133.3. Browse NL, Wilson NM, Russo F, Al-Hassan H, Allen DR. Aetiology and treatment
of chylous ascites. Br J Surg 1992;79:1145—1150.4. Camiel MR, Benninghoff DL, Herman P. Chylous ascites with lymphographic
demonstration oflymph leakage into the peritoneal cavity. Gastroenterology l964;47:188—191.
5. McNeill GC, Wine MH, Wifte CL, Ct al. Whole-body lymphangioscintigraphy:preferred method for initial assessment of the peripheral lymphatic system. Radiology1989;172:495—502.
6. Weissleder R, Thrall JH. The lymphatic system: diagnostic imaging studies. Radiology1989;172:3 15—317.
7. Gates GF, Dove EK, Kawchanapoon V. Thoracic duct leakage in neonatal chylothoraxvisualized by ‘°8Aulymphangiography. Radiology 1972; 105:619—620.
8. Sty JR. Thomas JP, Abrams J. Radionuclide lymphography: a demonstration ofsurgical lymphatic interruption. Clin Nucl Med l978;4:412—413.
9. Heyman S, Wilmott R. Chylothorax on technetium-99m antimony sulfide colloid scan.JNucl Med 1986;27:l783—1784.
10. Lopez OL, Rodriguez-Maisano E, Delevaux JL. Thoracic duct malformations. Lymphoscintigraphic diagnoses. Clin NucI Med I986;11:479—481.
I 1. Gregg DC, Wells RG, Sty JR. Lymphoscintigraphy. Chylous ascites and lymphoceledemonstration. Clin NucI Med 1988;13:300.
12. Lu G, Shih Wi, Chou C. Technetium-99m antimony sulfate lymphoscintigraphy todemonstrate lymphatic communication between the peritoneal cavity and the scrotum.Clin Nucl Med 1995;20:706—708.
13. Biswas G, Samuel AM. Technetium-99m dextran lymphoscintigraphy in an infant withchylous peritoneal effusion. Clin Nucl Med I996;2 1:341—342.
14. Juma N, Audrey 1, Ege GN. Comparison as a lymphoscintigraphic agent between99m1c dextran and 99mTc antimony suiphide colloid. Br J Radiology I985;58:325—330.
15. Witte MH, Jamal 5, Williams WH, et al. Lymphatic abnormalities in human filanasisas depicted by lymphangioscintigraphy. Arch Intern Med l993;153:737—744.
16. Haddad MC, al-Shahed MS. Sharif HS, Miola UJ. Case report: investigation ofchyluria. Clin Radio! 1994;49:137—l39.
17. Freedman DO, de-Almeida-Filho PJ, Besh 5, et al. Lymphoscintigraphic analysis oflymphatic abnormalities in symptomatic and asymptomatic human filariasis. J lnftctDis 1994;I70:927—933.
18. Verreault J, Lepage 5, Bisson G, Plante A. Ascites and right pleural effusion:demonstration ofa peritoneo-pleural communication. JNuclMed l986;27: 1706—1709.
19. Moss R, Hinds 5, Fedullo AJ. Chylothorax: a complication ofthe nephrotic syndrome.Am Rev RespirDis 1989;140:I436—1437.
20. Lindenbaum J, Scheidt 55. Chylous ascites and the nephrotic syndrome. Am J Medl968;44:830—836.
21. Sabnis RB, Punekar SV, Desai RM, Bradoo AM, Bapat SD. Instillation ofsilver nitratein the treatment of chyluria. Br J Urol l992;70:660—662.
22. Gloviczki P, Fisher J, Hoilier LH, et al. Microsurgical lymphovenous anastomosis fortreatment of lymphedema: a critical review. J VascSurg 1988;7:647—652.
23. Ablan Ci, Littooy FN, Freeark Ri. Postoperative chylous ascites: diagnosis andtreatment. Arch Surg l990;l25:270—273.
by on April 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from
1998;39:1292-1296.J Nucl Med. Margaret H. Pui and Tian-Chao Yueh Lymphoscintigraphy in Chyluria, Chyloperitoneum and Chylothorax
http://jnm.snmjournals.org/content/39/7/1292This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1998 SNMMI; all rights reserved.
by on April 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from