-
Artikel Penelitian
J Indon Med Assoc, Volum: 61, Nomor: 11, November 2011 429
Glycemic Control inSwitching Insulin-based Regimen Among
Type 2 Diabetic Patients
Pradana Soewondo, Imam Subektion behalf of INTERBASE Study
Group
Department of Internal Medicine, Faculty of Medicine Universitas
Indonesia/Dr. Cipto Mangunkusumo Hospital, Jakarta
Abstract: Appropriate diet and physical activity, maintaining a
healthy body weight and propercontrol of diabetes using oral anti
diabetic (OAD) in people with diabetes type 2 will helpreduce its
complications. However, some advance diabetic cases need
insulin-based regimen toaggressively lower blood glucose level.
Local data was insufficient to determine whether type 2diabetes
patients on insulin were indeed attaining glycemia goals. The aim
of this study was toassess the clinical response of type 2 diabetic
patients who were switched to another insulinregimen to achieve
glycemic control. The study was performed as a non-interventional
prospec-tive disease registry that mirror real life management of
these subjects after a 3 month follow up.To assess the clinical
response, we performed measurement of fasting blood glucose level,
HbA1c,waist circumference and body weight. One hundred and fifteen
type 2 diabetes patients whowere already on insulin therapy with
unsatisfactory control of glycaemia parameters wereadmitted in this
study of an actual clinical setting. Only 93 cases have been
examined in a 3month follow up. Premix, Short-acting and
Intermediate-acting insulin were the most popularinsulin-based
regimens that previously been prescribed, while basal analogue
insulin is themost common regimen for switching therapy. The newly
prescribed insulin-based regimen showedsignificant reduction of
important glycaemia parameters such as fasting blood glucose level
andHbA1c. Serum blood glucose was decreased 61.76 mg/dL (p
-
J Indon Med Assoc, Volum: 61, Nomor: 11, November 2011430
Kontrol Glikemik pada Penderita DM Tipe 2dengan Perubahan
Rejimen Insulin
Pradana Soewondo, Imam Subekti,atas nama INTERBASE Study
Group
Departemen Ilmu Penyakit Dalam, Fakultas Kedokteran Universitas
Indonesia/Rumah Sakit Umum Pusat Dr. Cipto Mangunkusumo,
Jakarta
Abstrak: Kontrol diabetes secara rutin dengan mengatur diet dan
aktivitas fisik, menjaga beratbadan ideal dan konsumsi obat
hipoglikemia oral (OHO) diharapkan dapat menurunkankomplikasi
kronik Diabetes Melitus tipe 2. Meskipun demikian, sejumlah kasus
diabetes yanglanjut memerlukan terapi insulin untuk menurunkan
kadar glukosa darah secara agresif. Datapenelitian yang ada di
Indonesia masih kurang mencukupi untuk menggambarkan
pencapaiantarget glikemik pada pasien DM tipe 2 yang menggunakan
insulin. Tujuan penelitian ini adalahmenilai respons klinis pasien
DM tipe 2 dengan perubahan rejimen insulin untuk pencapaiantarget
glikemik. Penelitian ini menggunakan desain studi registri
non-interventional, prospektif,mencerminkan penanganan DM tipe 2
sehari-hari setelah terapi selama 3 bulan. Untuk menilairespons
klinis, dilakukan pemeriksaan kadar glukosa darah puasa, HbA1c,
lingkar pinggangdan berat badan. Seratus lima belas pasien DM tipe
2 yang telah menggunakan insulin namunbelum mencapai kontrol
glikemik kemudian diubah jenis terapi insulinnya selama 3 bulan
dalamkondisi klinis sehari-hari. Hanya 93 kasus yang dapat dinilai
selama 3 bulan terapi. Insulinpremix, kerja pendek dan kerja
menengah merupakan jenis insulin yang terbanyak
digunakansebelumnya, sedangkan insulin basal analog adalah insulin
terbanyak yang digunakan dalamperubahan terapi. Perubahan jenis
insulin yang baru menunjukkan penurunan parameter glikemikyang
bermakna, yakni kadar glukosa darah puasa dan HbA1c. Penurunan
glukosa darah mencapai61,76 mg/dL (p
-
Glycemic Control in Switching Insulin-based Regimen Among Type 2
Diabetic Patients
J Indon Med Assoc, Volum: 61, Nomor: 11, November 2011 431
MethodsThis study was performed as a non-interventional pro-
spective disease registry that mirror real life management
ofthese subjects (purely for observational study). Nineteenstudy
centers from four provinces in Indonesia (Jakarta,West Java, East
Java and Bali) have reported 115 type 2diabetic patients who were
currently receiving insulin treat-ment but still had uncontrolled
glycemia parameter (HbA1c> 8%, data from the DiabCare Asia 2008
study demonstratesthe mean of HbA1c achieved was 8.1%), whose
physicianshad decided to change the current insulin regimen to a
newinsulin regimen due to any reason, and were willing to signa
informed consent form.
All Data Collection Forms (DCFs) were verified for ex-istence
and eligibility of patients, and for the presence ofinformed
consent. A Source Data Verification was performedin 63% of the
sites.
The quantitative variables were compared by an analy-sis of the
variance and Students paired t-test (for param-eters measured
before and after the treatment period). Allstatistical tests have
been performed using 2-tailed tests at5% level of significance or
with adjustment if needed.Results
The diabetic cases were equally distributed among maleand female
patients with an average age of 54 years (SD =8.8 years). The
majority of cases belonged to 50 60 yearsage group. The average
body mass index was 24.1 kg/mand the waist circumference was 88.3
cm. The HbA1c andfasting blood glucose level at baseline were
particularly high(Table 1).
As all of the cases are in unsatisfactory state of glycae-mia
control, most of them suffered from diabetic complica-tions.
Neuropathy is the most common complication with67.8% of subject
show neurological signs. The second most
Table 1. Characteristic of Subjects
Variable N (%) Mean or Median
Gender (n=115)Male 56 (48.7)Female 59 (51.3)
Age (n=114) 54.0 +/- 8.861 + yrs 18 (15.8)50 - 60 yrs 59
(51.8)< 50 yrs 37 (32.5)
Education (n=112)Low 28 (25.0)Middle 56 (50.0)High 28 (25.0)
Previous insulin(s) (n=115)Rapid-acting 10 (8.7)Short-acting 40
(34.8)Intermediate-acting 32 (27.8)Basal analogue 9 (7.8)Premix 31
(27.0)
Previous OAD(s) (n=115)Glimepiride 21 (18.3)Acarbose 22
(19.1)Metformin 63 (54.8)Gliquidone 7 (6.1)Glibenclamide 14
(12.2)Gliclazide 30 (26.1)Glibenclamide/Metformin 5 (4.3)Other 3
(2.6)
Type 2 diabetes history (yrs, n=93) 6.1 +/- 4.9Body Mass Index
(kg/m, n=115) 24.1 +/- 4.4Waist circumference (cm, n=106) 88.3 +/-
12.3Systolic blood pressure (mmHg, n=115) 132.5 +/- 18.0Diastolic
blood pressure (mmHg, n=115) 81.9 +/- 8.8HbA1c (%, n=115) 10.0 +/-
1.8Fasting blood glucose (mg/dl, n=108) 223 (43-501)
0 10 20 30 40 50 60 70 80
P e r c e nt
Dyslipidemia
Hypert ension
Vascular
Nephropat hy
Neuropat hy
Ret inopat hy
common complication is retinopathy with 30.7%, followedby
vascular diseases and nephropathy with 26.1% and 23.5%respectively.
Dislipidemia and hypertension are the two con-comitant conditions
of diabetes. More than 71% of cases
Figure 1. Clinical Signs of Diabetics Complication
-
Glycemic Control in Switching Insulin-based Regimen Among Type 2
Diabetic Patients
J Indon Med Assoc, Volum: 61, Nomor: 11, November 2011432
Table 2. Means and Standard Devisition of Daily Does of the
Previous and Current Insulin Regimen
Type of Insulin Previous Insulin Current InsulinNumber Mean S D
Min Max Number Mean S D Min Max
Long-acting insulin 6 22.7 12.8 8 42 80 18.1 9.5 8
40Intermediate insulin 26 16.2 7.8 8 40 NilShort acting insulin 33
30.2 16.1 6 75 2 60 0 60 80Rapid acting insulin 9 30.7 12.2 18 60
12 21.8 13 6 48Premix insulin 25 22.5 10.4 8 50 12 22.8 5.2 14
34
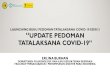
0 10 20 30 40 50 60 70 80 90
Percent
Rapid-act ing
Basal analogue
Intermediate-act ing
Short-act ing
Premix
Pre New
Figure 2. Previous and Newly Prescribed Insulin-based
Regimens
also suffered from dislipidemia and almost 48% have highblood
pressure (figure 1).
The most common prescribed insulin-based regimensare
short-acting (34%), followed by intermediate-acting(27.8%) and
premix (27%). Basal analogue (7.8%) and rapid-acting (8.7%) were
rarely prescribed as first line insulin-basedregimens. The daily
dose administration of short- and rapid-acting insulin was higher
than other regimens (table 2). Know-ing that these previously
prescribed insulin regimens showedunsatisfactory response of
glycemia control, the doctorsagreed to switch to new insulin
regimen.
The newly prescribed regimens are dominated withbasal analogue
(85.2%) and only few patients were givenpremix (13%) or
rapid-acting Insulin (9.6%) (figure 2). Thedaily dose
administration of short-acting insulin was thehighest among insulin
regimens (Table 2). After therapy waschanged, patients received
either insulin alone or combina-tion with OAD, depending on the new
treatment. Approxi-mately 20% of patients with basal analogue
insulin receivedonly basal insulin during the study, while others
receivedcombination therapy with OAD(s) (table 3). These
patientswere followed up after a therapeutic period of 3
months.
Only 93 patients returned to the study centers and could
beexamined.
After a 3 month period using newly prescribed insulin-based
regimen, there are significant improvements of some
Table 3. Distribution of Subjects According to Current Insu-lin
Regimen and Concomitant Oral Therapy (n=93)
Concomitant Current insulin regimen TotalOral Therapy Glargine
Glul is ine Premix
Glimepiride 11 0 0 11Arcabose 10 0 0 10Metformin 19 1 6
26Gliquidone 8 1 0 9Glibenclamide 3 0 2 5Pioglitazone 1 0 0
1Glibenclamide/ 5 1 0 6
MetforminGliclazide 4 0 3 7Glipizide 1 0 0 1No concomitant 16 0
1 17oral therapy
Total 78 3 12 93
-
J Indon Med Assoc, Volum: 61, Nomor: 11, November 2011
Glycemic Control in Switching Insulin-based Regimen Among Type 2
Diabetic Patients
433
important glycemia parameters. Level of HbA1c decreasedfrom
9.83+1.71% to 8.44+1.85% (p
-
Glycemic Control in Switching Insulin-based Regimen Among Type 2
Diabetic Patients
J Indon Med Assoc, Volum: 61, Nomor: 11, November 2011434
nificantly with an average of 0.70 cm. There is an
interestingphenomenon that almost 43% of subject showed good
re-sponse in reducing body weight, but in overall there was
anaverage of 0.26 kg weight gain experienced by type 2 diabe-tes
patients at the 3 month follow up visit, though it was
notstatistically significant. The good response of important
gly-caemia parameters to the changing of insulin-based regimenmight
reflects the probability of treatment saturation for spe-cific
regimen due to complex biological processes. The satu-rated regimen
needs to be replaced with other regimen toenable better response in
type 2 diabetes patient.
ConclusionIt was concluded that despite the prescription of
insu-
lin-based regimens combined with OAD for type 2
diabetespatients, there were still cases of unsatisfactory
glycemiccontrol that need medification of insulin regimen.
Medificationof insulin-based regimen gave better result for the
type 2diabetes patients.
AcknowledgementThe authors are especially grateful to all
investigators
who have participated in INTERBASE study: Dr. SulistiawatyOhnio,
SpPD, Dr. Maxwadi Maas, SpPD, Dr. Eliana Taufik,SpPD, Dr. Asep
Saepul Rohmat, SpPD, Dr. Arief Wibowo,SpPD, Dr. Anton Cahaya, Dr.
Sutji Muljati, Dr. Mery Harita,Dr. Hadi Sunaryo, SpPD, Dr. Maria
Meilitasari Harlim, SpPD,Dr. R. Eka, SpPD, Dr. Nunik K.Kartikawati,
Dr. Ishak S.Dinata,SpPD, Dr. G. Wisito, SpPD, Dr. Agatha Maharani,
SpPD, Dr.Johannes Lusida, SpPD, Dr. Ratna Saraswati, SpPD, Dr. J.
M.Maitriya, SpPD
References1. Dans AL, Morales DD, Abola TB, Roxas J. National
Nutrition
and Health Survey (NNHeS): Atherosclerosis-related diseases
andrisk factors. Phil J Internal Medicine. 2005;43:103-15.
2. Soewondo P, Soegondo S, Suastika K, Pranoto A, SoeatmadjiDW,
Tjokroprawiro A. The DiabCare Asia 2008 study - Out-comes on
control and complications of type 2 diabetic patientsin Indonesia.
Med J Indones. 2010;19:235-44.
3. BPS-Statistics Indonesia Data, 2003. Available from:
http://www.bps.go.id/
4. Lantion-Ag LC. Epidemiology of diabetes mellitus in
WesternPacific region: focus on Indonesia. Diab Res Clin Pract.
2000;50(Supll 2):S29-S34.
5. Turner RC, Cull CA, Frighi V, Holman RR. Glycaemia
controlwith diet, sulfonylurea, metformin, or insulin in patients
withtype 2 diabetes mellitus: progressive requirement for
multipletherapies (UKPDS 49): UK. Prospective Diabetes Study
(UKPDS)Group. JAMA;1999;281:2005-12.
6. UK Prospective Diabetes Study (UKPDS) group. Intensive
bloodglucose control with sulphonylureas or insulin compared
withconventional treatment and risk of complications with
subjectswith type 2 diabetes (UKPDS 33). Lancet.
1998;352:837-53.
7. Palmer AJ, Valentine WJ, Ray JA, Fos V, Lurati F, Smith I, et
al.An economic assessment of analogue basal-bolus insulin
versushuman basal-bolus insulin in subjects with type 1 diabetes in
UK.Curr Med Res Opinion. 2007;23(4):895-901.
8. Hartman I. Insulin analogs: impact on treatment success,
satis-faction, quality of life and adherence. Clin Med Res. 2008;
6(2):54-67.
9. Farmer AJ, Oke J, Stevens R, Holman RR. Differences in
insulintreatment satisfaction following randomized addition of
biphasic,prandial or basal insulin to oral therapy in type 2
diabetes. Diabe-tes Obes Metab. 2011;13(12):1136-41.
10. Janka HU, Plewe G, Riddle MC, Kliebe-Firch C, Schweitzer
MA,Jarvinen HYK. Comparison of basal insulin added to oral
agentsversus twice-daily premixed insulin as initial insulin
therapy fortype 2 diabetes. Diabetes Care. 2005;28:254-9.
11. Riddle M, Umpierrez G, DiGenio A, Zhou R, Rosenstock J.
Con-tributions of basal and postprandial hyperglycemia over a
widerange of A1c levels before and after treatment intensification
intype 2 diabetes. Diabetes Care 2011 Oct 25 [Epub ahead of
print]
12. Davies M, Sinnassamy P, Storms F, Gomis R on behalf of the
ATLANTUS Study Group. Insulin glargine-based therapy
improvesglycemic control in patients with type 2 diabetes
sub-optimallycontrolled on premixed insulin therapies. Diab Res
Clin Pract.2008;79:368-375.
13. Riddle MC. The treat-to-target trial and related studies.
EndocrPract. 2006;12(Suppl 1):71-9.
14. Llag LL, Kerr L, Malone JK, Tan MH. Prandial premixed
insulinanalogue regimens versus basal insulin analogue regimens in
themanagement of type 2 diabetes: an evidence-based
combination.Clin Ther. 2007;29(6):1254-70.
15. Minze MG, Dalal K, Irons BK. Removing barriers to insulin
use.J Fam Pract. 2011;60(10):577-80.
MS