Embed Size (px)
Citation preview
Management of Obstructive sleep
apnea syndrome in Diabetes
신원철
강동 경희대병원 신경과, 수면센터

Obstructive sleep apnea-hypopnea syndrome Vs DM
High blood pressure
Failing heart
….......

증례 ;55세 남자
• CC: 낮에 존다./1년전부터
• snoring : 20년전부터 • sleep apnea : 5년전부터
• 수면 - 10;30 - 12;00 취침. - 1분이내로 잠듬. - 아침 5;30 - 6;00 기상. - 중간에 2번 정도 깸. / 화장실 , 숨
이 막혀서 깸. - 자고 나면, 개운하지 않음. - dry mouth (+) in the morning - EDS (++) - 졸음 운전 (-)
• 20년 전 코골이 수술.. • 혈압약과 당뇨; 5년전 사회력> - 담배 ; 작년 5월 금연 - 술 : 주 1회 , 주량. 소주 2
병.. • Wt ; 100kg. - 1년동안 10kg.

Dx & Tx plan
• PSG
• Cephalometry
• ENT consult for nasal and oral evaluation
• Sleep conference







Contents
• 수면무호흡증이란
• 왜수면무호흡증이 발생하는가?
• 당뇨, 심혈관질환과 수면무호흡증 관계
• 수면무호흡증의 치료와 효과

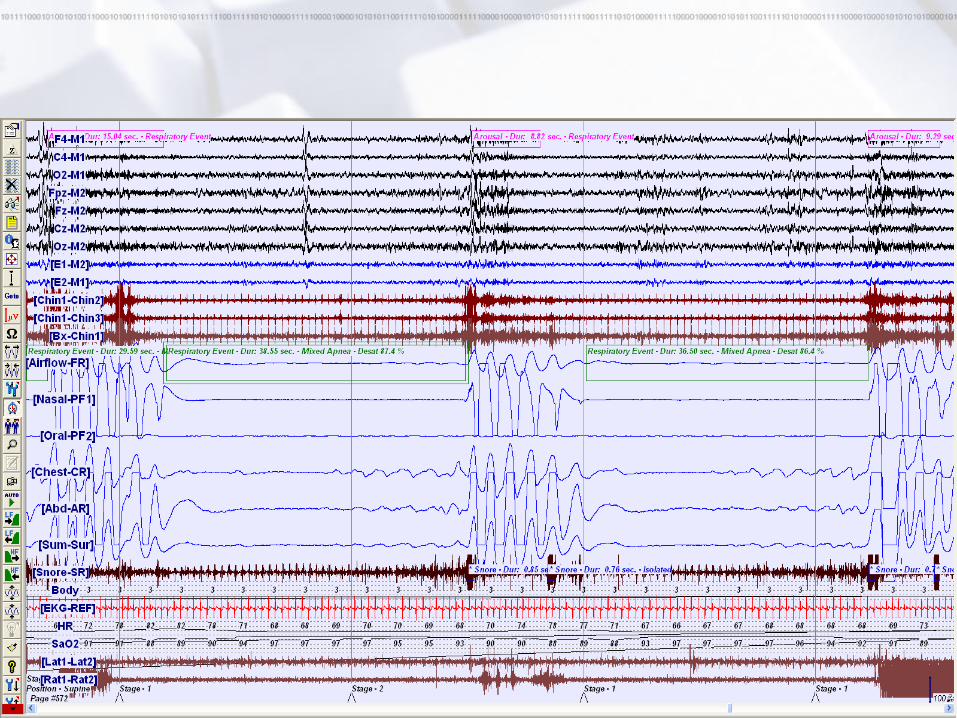
수면무호흡-저호흡 증후군
수면무호흡
: 수면 중 10초 이상 숨을 쉬지 않는 것.
수면무호흡-저호흡 증후군
; 잠자는 중, 수면무호흡이 시간당 5번 이상 발생 할 때.
수면무호흡-저호흡 지수 (AHI) : 수면 한시간 동안 무호흡 또는 저호흡 횟수
- AHI 5이하 : 정상
- AHI 5 – 15 : 경한 무호흡증
- AHI 15-30 : 중등도 무호흡증
- AHI 30 이상 : 심한 무호흡증

Sleep Apnea Syndrome;New ICSD-2
A At least one of the following apply:
i. Patient complains of unintentional sleep episodes during wakefulness, daytime sleepiness, unrefreshing sleep,fatigue, or Insomnia.
ii. Patient wakes with breath holds, gasping, or choking.
iii. Bedpartner-observed symptoms include loud snoring and/or breathing interruptions during the patient’s sleep.
B Polysomnographic recording shows the following:
i. Equal to or more than 5 scoreable respiratory events (i.e., apneas, hypopneas, RERAs) per hour of sleep.
ii. Evidence of respiratory effort during all or a portion of each respiratory event. (In the case of a RERA, this is best seen with use of esophageal manometry)
C The patient’s symptoms are not better explained by another sleep disorder, medical condition, mental disorder, substance abuse/dependence, or medication.

왜 수면무호흡증이 발생하는가?
깨어 있을 때
잠자는 중

각성시, 깨어 있을 때 상기도
수면중 상기도


Risk factors for obstructive sleep apnea syndrome
Male gender
Obesity
Specific craniofacial disorders (Treacher-
Collins, Pierre-Robin syndrome)
Retroposed mandibule/maxillae
Adenotonsillar hypertrophy
Nasal problems : septal deviation,
allergic rhinitis
Endocrine abnormalities ; hypothyroidism,
acromegaly
Polycystic ovarian syndrome
Postmenopause
Down syndrome
Family aggregation
APOε4 allele (in subjects <65yr)
Pack AI. Am J Resp Crit Care Med 173;7-15, 2006

폐쇄성 수면무호흡증 (Obstructive Sleep Apnea: OSA)
• 40세 이상 한국인 5000명 대상 조사 – Apnea-hypopnea index (AHI)
: >5/hr sleep
– 남자: 27% (4.5%),
– 여자: 16.5% (3.5%)
• AHI > 10 (외국 보고) – 성인 남자 15%, 여자 5%
– 노인: 남자 70%, 여자 56%
• 증상 – 자주 깨고 수면 장애, 주간 졸림, 피로, 두통,
– 집중력, 기억력 저하, 반응 속도 느려짐
– 불면증, 야뇨증 , 사고 증가, 심장, 폐, 뇌졸중 증가
– 사망률 증가

Pathophysiology
Anatomical
narrowing
Aerodynamic change
Neuromuscular change
Cariovascular complication
Brain function change
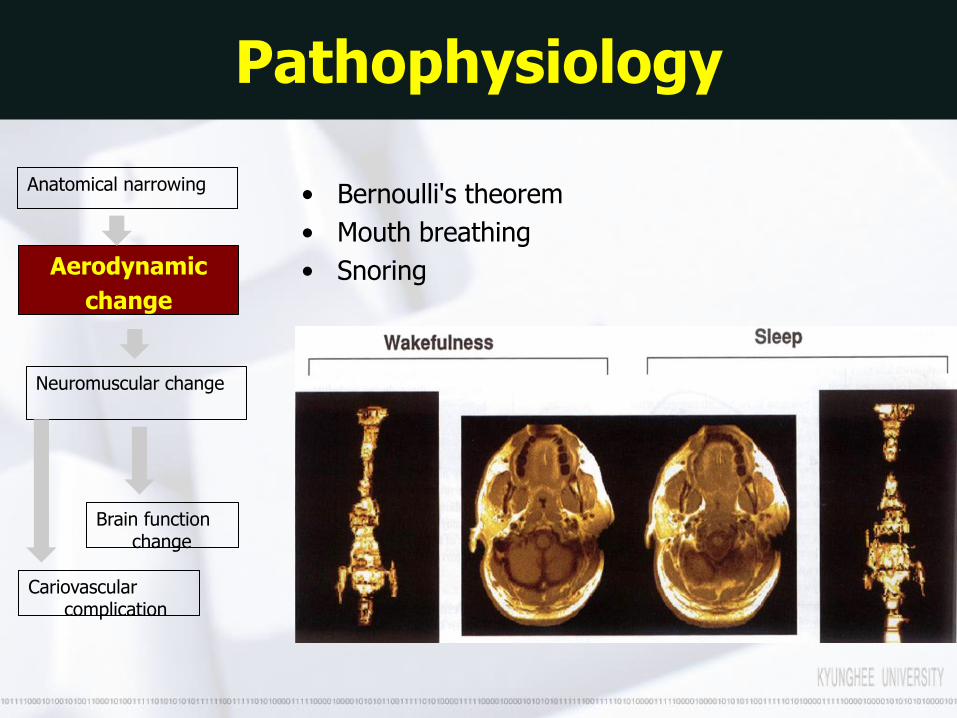
Anatomical narrowing
Aerodynamic
change
Neuromuscular change
Cariovascular complication
Brain function change
• Bernoulli's theorem
• Mouth breathing
• Snoring
Pathophysiology

Anatomical narrowing
Aerodynamic
change
Neuromuscular change
Cariovascular complication
Brain function change
Pathophysiology

Anatomical narrowing
Aerodynamic change
Neuromuscular
change
Cariovascular complication
Brain function change
• Neuromuscular reflex (Reflexogenic Dilatation)
• Snoring – low frequency mechanical trauma
--- damage to reflex ( nerve ending)
• Evolution of OSAS from snoring to apnea
Pathophysiology

Anatomical narrowing
Aerodynamic change
Neuromuscular change
Cariovascular complication
Brain function change
• Type grouping and Grouped atrophy
• Denervation and degeneration
• Irreversible damage to dilating muscle
increased collapsibility
Irreversible change
Mod. ~Severe OSA
Mild ~ Mod OSA
Pathophysiology

Two kinds of Apnea
Anatomical narrowing
Aerodynamic change
Neuromuscular change
Cariovascular complication
Brain function change
Anatomical narrowing
Aerodynamic change
Neuromuscular
change
Cariovascular complication
Brain function change
mechanical narrowing of airway by Bernoulli's theorem
The another one is functional narrowing of airway
by evolution theory
REM & Position OSA,
Mild OSA
Mod ~ severe OSA
Esp, non-position
Pathophysiology

Obstructive apnea

수면무호흡
수면
저산소증 이산화탄소 농도 상승
뇌 각성 상기도
근육 긴장도 상승
비만, 작은 턱, 굵은 목, 술, 담배, 나이
다시 잠듬.

수면무호흡
수면
저산소증 이산화탄소 농도 상승
뇌 각성 상기도
근육 긴장도 상승
비만, 작은 턱, 굵은 목, 술, 담배, 나이
다시 잠듬.
교감신경계항진 ; 당뇨 저항성 증가
동맥경화증 심장의 부담증가
수면의 질 저하 주간졸음, 아침 두통, 기억력
저하, 집중력저하

Pathophysiology
• Arousal and sleep fragmentation sleep loss
• Hypoxia
• Hypertension • Cerebrovascular, anatomical changes • Increased intracranial pressure • Inflammation and cytokines • Oxidative stress • Hormonal changes

Acute physiological effects of OSA
• Sympathetic activity
• During apnea blood pressure ↓ with varying effect on heart rate
• Following apnea blood pressure and heart rate ↑↑

Chronic physiological effects of OSA Naughton MT. Drug Discovery Today:Therapeutic strategies 1:329,2004
• ↑ 24-h sympathetic nervous system activity
• ↓ Heart rate variability
• Endothelial damage and dysfunction
• Platelet activation and ↑ blood coagulability
• Insulin resistance

Sympathetic activation
• HR variability ↓
– ↑ risk of future hypertension
– ↑ mortality in patients with HF
• BP variability ↑
– ↑ risk for damage to target organs

Oxidative stress
• Intermittent hypoxia & reperfusion
– Activation of polymorphonuclear neutrophils
– Generation of highly reactive free oxygen radicals

Inflammation

Metabolic dysregulation
• Leptin ↑
– Platelet aggregation
– Weight gain
– CV risk ↑
• Glucose intolerance
– DM↑

OSA prevalence in variable medical conditions
• Obese 40-60%
• Bariatric surgery evaluation 71-87%
• Hypertension 38%
• Stable outpatient congestive heart failure >50%
• Coronary artery disease >50%
• Diabetes 50-70%
• Acute stroke 70%
• Sleep clinics 67%

주간 졸림
• 수면무호흡증이 심할 수록 주간졸음증이 심하다.
SHHS: AJRCCM 1999;159:502-507
졸
림
정
도
주 간 졸음 점수
수면무호흡-저호흡지수 (수면시간당)

고혈압 • Prospective study , Wisconsin Sleep Cohort Study) - 893명을 4-8년동안 추적 조사함.
1.42
2.03
2.89
0
0.5
1
1.5
2
2.5
3
AHI <5 AHI 5.0-14.9
AHI >15
AHI <5
AHI 5.0-14.9
AHI >15
Peppard PE, et al. NEJM 2000;342:1378-1384.
AHI가 높을 수록 고혈압 발생이 높아짐.
정상인에 비해 고혈압이 3배 증가

관상동맥질환 • 62 CAD
• 62 age-, sex-, & BMI-matched control
Peker, et al. Eur Respir J 1999;14:179-184.
9.8
4.23.1
0
2
4
6
8
10
CAD
Smoking DM OSA
OR
수면무호흡증에서
관상동맥질환이
3배 이상 증가

Insulin resistance in OSA

Insulin resistance in OSA

폐쇄성수면무호흡증후군 환자의 치명적 심혈관 합병증 승산비(Odds ratio) : 2.87(95% CI 1.17-7.51)
Lancet 365: 1046-53, 2005
치명적인 심뇌혈관질환 발병율
144개월후(12년후)
중증의 폐쇄성 수면 무호흡 환자는 치료받지 않으면 12년 동안 치명적 심혈관 합병증 17%로 급증한다.(수면무호흡증이 없거나, 단순 코골이만 있으면, 5%이내)

사망률 연구
Eur Respir J 2002;20:1511-1518
치료군
비치료군

무호흡증과 뇌졸중
• 뇌경색증, 일과성 허혈발작
– AHI > 10: 63-95%
– AHI > 20: 68-80%
• 주간 졸림, 피로
• 재활 장애
• 짜증, 화
• 뇌졸중 발병율
AHI > 10, 2.6배
• 사망률 증가
Arch Phys Med Rehabil Vol 76, January 1995

Tx of OSA
• 1. Weight control
• 2. positional therapy
• 3. oral device
• 4. surgery
• 5. CPAP

Weight control 체중 감량(비만조절) : 10-15 kg
체중감량 후 상기도의 MRI영상의 변화

Obesity : risk factors for the development of sleep apnea
• Obesity ; strongest risk factors for OSA, >70% of OSA
• OSA in obese - 40% of obese with no complaint of sleep disorders - 55% of all adolescents who underwent bariatic surgery - 71%> of morbid obese
• Increase in body weight Vs OSA • 10% Wt gain – 6-fold increase in the odds of developing OSA • 10% Wt loss 26% decrease in the AHI (Peppard PE et al, JAMA 2000)
• Neck circumference and central obesity ; Significant predictors of a higher AHI

Changes in apnea–hypopnea index in relation to changes in body weight
Tuomilehto et al. Lifestyle Intervention with Weight Reduction First-line Treatment in Mild Obstructive Sleep Apnea Am J Respir Crit Care Med. 2009: 320–327
• Randomization (N=81, 18~65 y, AHI=5~15, BMI 28~40)
• very low calorie diet vs control
• 12 months f/u
Institute for Clinical Nutrition

SLEEP POSITION & SURGERY

CPAP Vs Positional therapy effect for AHI CHEST 1999; 115:771–781

비강양압호흡 치료(nCPAP)

지속적기도양압술(CPAP)
Most widely accepted and effective therapy available for the treatment of OSA
PAP provides a “pneumatic splint” by delivering an intraluminal pressure that is positive with reference to the atmospheric pressure.

CPAP with/without Auto or C-flex
Respironics REMstar System One
ResMed S8 series ResMed S9 series
Hoffrichter Vector
위드메드
통일의료기 CPAP코리아

Nasal Mask
Respironics TrueBlue ResMed Mirage series FX, FX for her, SoftGel, Activa, Micro, Vista

Nasal Pillows
ResMed Swift� LT Nasal Pillows System with Headgear
Respironics ComfortLife
Respironics OptiLife

Effect of CPAP on OSAS


Benefits of PAP treatment
• Improvement in markets of systemic inflammation/ endocrine – decreased CRP and IL-6 – decreased Leptin – decreased VEGF – improved insulin sensitivity – type 2 DM glycemic control
• Benefits in patients with cardiovascular disease – decreased AF recurrence after cardioversion – improved EF in patients with cardiomyopathy + OSA – improvements in survival and neurocognitive function – APPLES (Apnea Positive Pressure Long-Term Efficacy Study)

J Clin Endocrinol Metab 96:365–374.2011)

118 men with obstructive sleep apnoea (Epworth score >9, and a >4% oxygen desaturation index of >10 per h) who were assigned to either therapeutic (n=59) or subtherapeutic (59) nCPAP (about 1 cm H2O pressure) for 1 month.
Lancet 2001; 359: 204–10

CPAP effect on insulin sensitivity
J Clin Endocrinol Metab 96: 365–374, 2011)

폐쇄성수면무호흡증후군 환자의 치명적 심혈관 합병증 승산비(Odds ratio) : 2.87(95% CI 1.17-7.51)
Lancet 365: 1046-53, 2005

Summary

putative pathways leading from sleep loss to diabetes and obesity risk

Risk factor clustering
OSA


Control Sleep Apnea:
Better Diabetes Control
• Improve insulin sensitivity
• Lower blood sugars
• Lower HbA1-c
• Lower dosages of oral hypoglycemic agents or less medicines




















