Embed Size (px)
Citation preview

Juan Carlos Uribe O. MDInternista CES
Fellow Cardiología CES
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
MANEJO DE LA TERAPIA ANTITROMBÓTICA EN PACIENTES SOMETIDOS A
PROCEDIMIENTOS QUIRÚRGICOS
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• Población anticoagulada en aumento.
• Warfarina.
• Nuevos anticoagulantes.
• TAPD por SCA y stents → en aumento.
• 10% - 20% → Qx o procedimientos invasivos que requieren la suspensión temporal.
• Meta → minimizar eventos tromboembólicos y hemorragias mayores peri procedimiento.
200
400
600
800
1000
1200
1400
1980 1985 1990 1995 2000 2005 2009Años
Proc
edim
ientos
en m
iles
CoronariografíasPCI
Circulation 2012;125(1):e2- e220.
Anticoagulados
INTRODUCCIÓN
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

Antiplaquetarios
Vida media
Bloqueo del Rc
Inicio de acción
Fin acción
ASA Irreversible 30 min 7 d
Inhibidores P2Y12Inhibidores P2Y12Inhibidores P2Y12Inhibidores P2Y12Inhibidores P2Y12
Clopidogrel 6 h Irreversible 2 - 8 h 7 d
Prasugrel 7 h Irreversible 30 min - 4 h 7 d
Ticagrelor 8 - 12 h Reversible 30 min - 2 h 5 d
practise is significantly diminished as the consequence ofnew approaches to clopidogrel dosing (i.e. pretreatment,high loading doses), the availability of more potent anti-platelet agents than clopidogrel (i.e. prasugrel and ticagre-lor), and the lower risk of bleeding with alternativeantithrombotic option (i.e. bivalirudin) [20].
Limitations of aspirin, clopidogrel, and glycoproteinIIb/IIIa inhibitors have prompted a search for novel anti-platelet agents with a more favorable risk–benefit ratio.This article is aimed at providing an overview on new an-tiplatelet drugs in the setting of ACS and PCI, includingthe most recent advances on recently approved agents aswell as on emerging compounds in clinical development(Figs 1 and 2). A description of more established antiplat-elet therapies, including aspirin, clopidogrel, and glyco-protein IIb/IIIa inhibitors, antiplatelet drugs which donot have an approved indication for ACS/PCI (i.e.pentoxifylline, cilostazol, dipyridamole) as well as novelanticoagulant agents with no direct action on platelets gobeyond the scope of this manuscript and will not bediscussed.
Thromboxane a2 pathway inhibitors
Aspirin has been the cornerstone of treatment for patientswith various atherosclerotic disease manifestations. It
exerts its effects by blocking the COX-1 enzyme and thusinhibiting the synthesis of TXA2 from arachidonic acid[21,22]. Despite the undisputable clinical benefits of aspi-rin, the notion that a proportion of patients experiencesuboptimal antiplatelet effects while on aspirin therapyhas prompted investigations to identify agents that moreeffectively inhibit thromboxane-mediated platelet activa-tion processes [23].
Thromboxane and prostaglandin endoperoxide (TP)receptors are expressed in platelets, inflammatory cells,vascular wall, and atherosclerotic plaques [24]. This mayexplain why TP receptor inhibitors may exert additionaleffects beyond those on platelets, including regulatingendothelial cell activation and vascular smooth musclecell contraction [25]. Blockage of TP receptors not onlyinhibits the platelet interaction with TXA2 but also bind-ing of its cyclic endoperoxide precursors. Importantly,although aspirin blocks TXA2 synthesis in most individu-als, shuttling of endoperoxide intermediates to plateletsfrom other cells may account for some variability in theclinical response to aspirin. For this reason, blocking TPreceptors is theoretically more effective than simplyreducing the generation of TXA2 at the COX-1 level [26].Moreover, many TXA2 pathway inhibitors exert a dualpharmacological action, since they inhibit both TP recep-tors and TXA2 synthase, thereby resulting in a more com-
ADP
CURRENTLY AVAILABLE ANTIPLATELET AGENTS
Thrombin
ADP
5HT2
A
PGE
AA
G
P13K
cox-1
G
G
GG
G
TiclopidineClopidogrelPrasugrelTicagrelor
fibrinogen
Intracellular signaling
GPVI GP lb/IX/V
GP llb/IIIa
GP llB/IIIA INHIBITORS
AbciximabTirofiban
Eptifibatide
TxA2 INHIBITORS
P2Y12 INHIBITORS
cox-1 InhibitorsAspirin
TxA2
TxA2
Fig. 1. Sites of action of currently available agents for acute coronary syndromes or percutaneous coronary intervention. 5HT2A, serotonin;AA, arachidonic acid; ADP, adenosine diphosphate; COX-1, cyclooxygenase-1; G, G-protein; GP, glycoprotein; PG, prostaglandin; PI3K,phosphatidylinositol 3-kinase; TxA2, thromboxane A2. Reproduced with permission from Ferreiro et al., Circ Cardiovasc Interv. 2012;5:433–45[20].
© 2013 International Society on Thrombosis and Haemostasis
New directions in antiplatelet therapy 317
J Thromb Haemost 2013; 11 (Suppl. 1): 316–29.
ANTIPLAQUETARIOS
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13
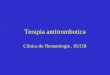
• Warfarina.
• Nuevos anticoagulantes:
Vida media Excreción renal
Rivaroxabán 5 - 13 h 66%
Apixabán 8 - 15 h 25%
Dabigatrán 12 - 14 h 80%
Anesthesiology 2013; 118:1466-74
Levy et al.
EDUCATION
increasingly replacing older parenteral agents and vitamin K antagonists in clinical practice, it is important to consider that patients treated with these agents will be exposed to di!er-ent clinical situations (spontaneous or postoperative bleeding, overdose, trauma, and elective or emergent surgical proce-dures) that require an intervention. "ere are also increasing concerns about managing patients on these therapeutic agents following trauma or in a perioperative setting. "e purpose of this review is (1) to examine the NOACs, focusing on key pharmacologic properties, and (2) to provide management approaches for users of NOACs in the perioperative and criti-cal care settings based on the available literature.
Oral Direct Thrombin Inhibitors"rombin has a pivotal role in hemostasis, making it an appealing target for anticoagulant drugs. When thrombin is activated from prothrombin, it converts soluble fibrinogen to insoluble fibrin; activates coagulation factors V, VIII, and XI (which generate more thrombin); and activates platelets (fig. 1).3 Dabigatran is a reversible direct thrombin inhibitor that directly inhibits free and fibrin-bound thrombin without the need for antithrombin. Dabigatran etexilate is a prodrug that has a rapid onset of action, no reported food interactions, few drug interaction, and does not require routine coagulation monitoring. "e peak plasma concentration is reached 1.25–3 h after administration, and it has a half-life of 12–14 h in healthy volunteers.4 Dabigatran is 35% bound to plasma proteins and undergoes renal excretion, with 80% of the drug entering the urine unchanged. "e anticoagulant e!ect of dabigatran accumulates in the setting of renal insu#ciency, and such bioaccumulation correlates well with the degree of renal dysfunction.5 In contrast to
other NOACs that are highly protein bound, the relatively low protein binding of dabigatran allows it to be eliminated to a large extent by hemodialysis.6 In cases of moderate hepatic impairment, dabigatran can be administered safely and no dose adjustment is necessary.7
Dabigatran is approved in the United States, Canada, Europe, and Japan for stroke prevention in patients with non-valvular AF based on the results of the Randomized Evaluation of Long-term anticoagulant therapY (RE-LY) trial in which 150 mg of dabigatran twice-daily was superior to dose-adjusted warfarin with a similar rate of major bleed-ing.8 Dabigatran, 75 mg twice-daily, is approved for use in the United States for patients with severe renal insu#ciency (CrCl 15–30 ml/min), based on indirect pharmacokinetic modeling and the assumed anticoagulant e!ect with this level of renal dysfunction. In Europe and Canada, the 75-mg dose is not approved for clinical use and dabigatran is con-traindicated in patients with a CrCl < 30 ml/min. Dabiga-tran is also is approved for VTE prophylaxis following total hip or knee replacement surgery in Europe and Canada, but not the United States. A recent indirect network meta-analy-sis suggests that treatment with dabigatran o!ers benefit for the prevention of stroke, systemic embolism, and mortality over antiplatelets and placebo without increased intracranial or extracranial hemorrhage compared to antiplatelet agents.9 Further investigations are needed to confirm these results.
Oral Direct Factor Xa InhibitorsFactor Xa is another important target for anticoagulant drugs due to its role as the rate-limiting factor in throm-bin generation and amplification, generating the Xa com-plex that converts prothrombin to thrombin (fig. 1).2 "e direct factor Xa inhibitors inhibit free Factor Xa, Factor Xa in the prothrombinase complex, and Factor Xa found in clots, independent of an antithrombin cofactor.2,10 "is is in contrast to low-molecular-weight heparin, unfractionated heparin, and fondaparinux, which all are dependent on anti-thrombin to inhibit Factor Xa.
RivaroxabanRivaroxaban is an oral, direct Factor Xa inhibitor that has good bioavailability (80%), is highly protein-bound, and has few drug interactions. Peak plasma concentrations occur within 2–4 h of administration, and rivaroxaban has a half-life of 5–9 h in healthy subjects and 11–13 h in the elderly.10 It is selective for Factor Xa in relation to other serine prote-ases.2 Clearance of rivaroxaban may be decreased to some extent in patients with renal impairment,11 but its primary mode of clearance is by non-renal mechanisms. It should be noted that although some reports may indicate that approxi-mately 67% of rivaroxaban is eliminated by the kidney, such total renal clearance reflects 33% clearance of active drug and 33% clearance of inactive rivaroxaban, which is not clin-ically important. "us, two-thirds of the active rivaroxaban
Fig. 1. Effect sites of anticoagulation agents. The new oral an-ticoagulation agents directly inhibit one of two major targets in the coagulation cascade. Rivaroxaban and apixaban directly inhibit factor Xa, and dabigatran directly inhibits thrombin. The parenteral anticoagulants that inhibit factor Xa include low-molecular-weight heparin (LMWH) and fondaparinux by antithrombin (AT)-dependent binding. Parenteral direct thrombin inhibitors include argatroban, bivalirudin, and de-sirudin that also directly inhibit thrombin independent of AT.
ANTICOAGULANTES
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• Conocer:
• Riesgo de sangrado.
• Riesgo tromboembólico.
• Terapia puente.
• Cuándo suspender y reiniciar la terapia antitrombótica.
Valorar el riesgo de eventos trombóticos durante el período en que se suspenden los agentes antitrombóticos.
CONCEPTOS GENERALES
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• Depende principalmente del tipo de procedimiento.
• Factores de riesgo asociados al paciente:
• Efecto residual de los antitrombóticos.
• Cáncer activo o QxTx.
• Historia de sangrado.
• Reintervención.
• HAS-BLED ≥ 3.
VALORACIÓN DEL RIESGO DE SANGRADO
J Thromb Haemost 2012;10:261- 7J Thromb Haemost. 2012;108:65–73
Característica Puntos
HTA 1
Alteración renal y/o hepática 1 o 2
ACV (Stroke) 1
Sangrado (Bleeding) 1
INR Labil 1
Edad 1
Drogas u OH 1 o 2
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

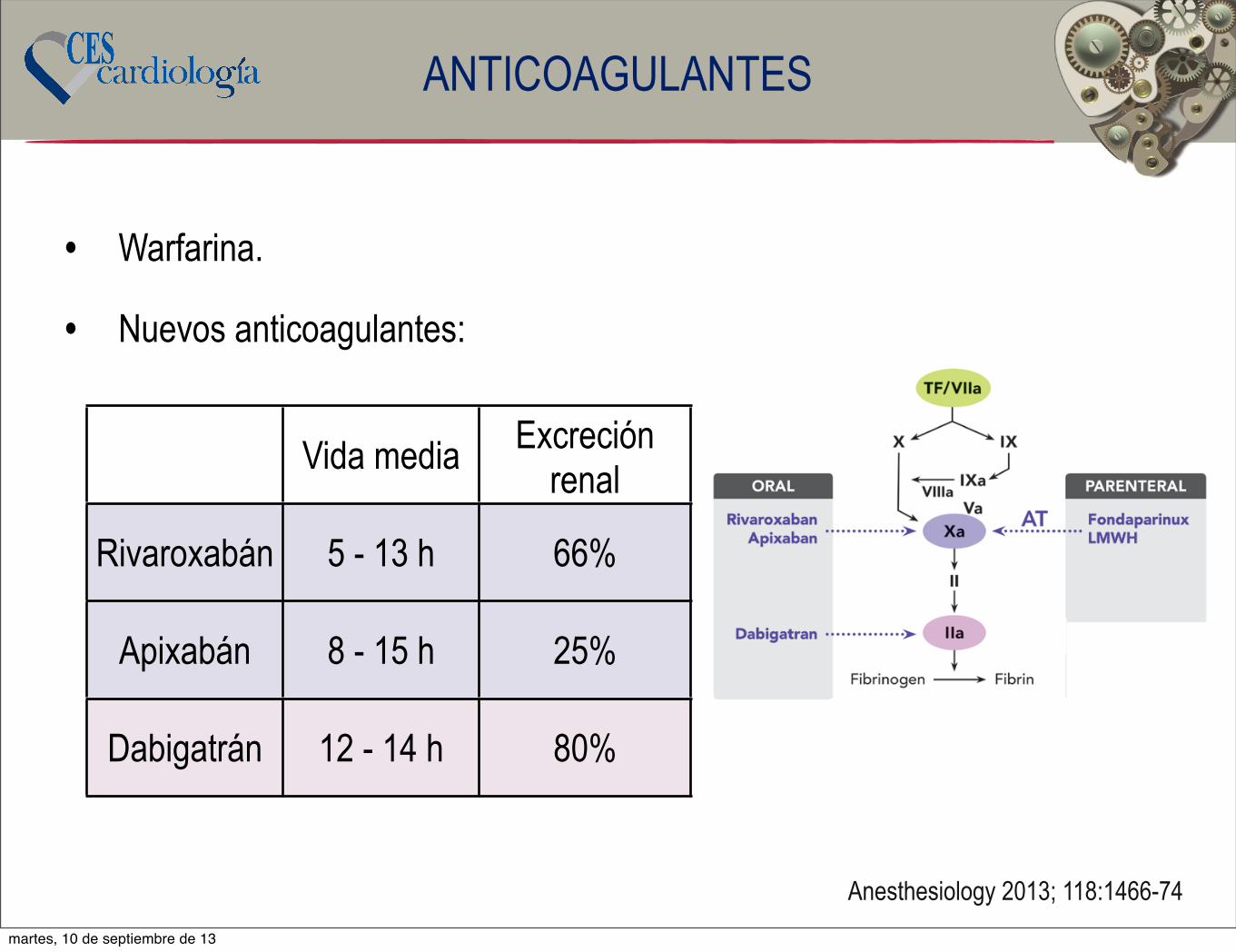
• Alto riesgo → riesgo > 1.5%.
• Procedimientos intracraneales, intraespinales, cámara posterior del ojo, retroperitoneo, intratorácicos.
VALORACIÓN DEL RIESGO DE SANGRADO
Circulation. 2012;126:486-490.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• Alto riesgo → riesgo > 1.5%.
• Procedimientos intracraneales, intraespinales, cámara posterior del ojo, retroperitoneo, intratorácicos.
VALORACIÓN DEL RIESGO DE SANGRADO
Circulation. 2012;126:486-490.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
DentalesExtracciones no complicadasEndodonciasPrótesisTerapia periodoncia
OftalmológicasQx de catarataTrabeculectomía
GastrointestinalEndoscopia superior c/s Bx.EnteroscopiaColonoscopia
Bajo Riesgo
martes, 10 de septiembre de 13

• Alto riesgo → riesgo > 1.5%.
• Procedimientos intracraneales, intraespinales, cámara posterior del ojo, retroperitoneo, intratorácicos.
VALORACIÓN DEL RIESGO DE SANGRADO
Circulation. 2012;126:486-490.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
DentalesExtracciones no complicadasEndodonciasPrótesisTerapia periodoncia
OftalmológicasQx de catarataTrabeculectomía
GastrointestinalEndoscopia superior c/s Bx.EnteroscopiaColonoscopia
Bajo Riesgo
No
susp
ende
r
antit
rom
bótic
os
martes, 10 de septiembre de 13
• Alto riesgo → riesgo > 1.5%.
• Procedimientos intracraneales, intraespinales, cámara posterior del ojo, retroperitoneo, intratorácicos.
Alto RiesgoCABG o Reemplazo valvularQx intracraneal o espinalReparo de AAPuentes arteriales periféricosQx vascular mayorQx ortopédica mayorQx plástica reconstructivaQx mayor de cancerQx de próstata o vejigaBx de próstata o riñón
VALORACIÓN DEL RIESGO DE SANGRADO
Circulation. 2012;126:486-490.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
DentalesExtracciones no complicadasEndodonciasPrótesisTerapia periodoncia
OftalmológicasQx de catarataTrabeculectomía
GastrointestinalEndoscopia superior c/s Bx.EnteroscopiaColonoscopia
Bajo Riesgo
No
susp
ende
r
antit
rom
bótic
os
martes, 10 de septiembre de 13

• Alto riesgo → riesgo > 1.5%.
• Procedimientos intracraneales, intraespinales, cámara posterior del ojo, retroperitoneo, intratorácicos.
Alto RiesgoCABG o Reemplazo valvularQx intracraneal o espinalReparo de AAPuentes arteriales periféricosQx vascular mayorQx ortopédica mayorQx plástica reconstructivaQx mayor de cancerQx de próstata o vejigaBx de próstata o riñón
VALORACIÓN DEL RIESGO DE SANGRADO
Consid
erar
Te
rapia
Puen
teCirculation. 2012;126:486-490.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
DentalesExtracciones no complicadasEndodonciasPrótesisTerapia periodoncia
OftalmológicasQx de catarataTrabeculectomía
GastrointestinalEndoscopia superior c/s Bx.EnteroscopiaColonoscopia
Bajo Riesgo
No
susp
ende
r
antit
rom
bótic
os
martes, 10 de septiembre de 13

Guidelines for the management of patients on oral anticoagulants requiring dental surgery BRITISH DENTAL JOURNAL VOLUME 203 NO. 7 OCT 13 2007
Sangrado Trombosis
• Riesgo de sangrado bajo con INR 2 - 3.
• Realizar INR 24 h previo al procedimiento.
• Uso de surgicel, esponjas de colágeno y suturas para disminuir el sangrado.
• Enjuages con Ac tranexámico al 5%.
• No prescribir AINEs o COX-2.
martes, 10 de septiembre de 13

Guidelines for the management of patients on oral anticoagulants requiring dental surgery BRITISH DENTAL JOURNAL VOLUME 203 NO. 7 OCT 13 2007
0
0,2
0,4
0,6
0,8
1
Riesgo (%)
Sangrado Trombosis
• Riesgo de sangrado bajo con INR 2 - 3.
• Realizar INR 24 h previo al procedimiento.
• Uso de surgicel, esponjas de colágeno y suturas para disminuir el sangrado.
• Enjuages con Ac tranexámico al 5%.
• No prescribir AINEs o COX-2.
martes, 10 de septiembre de 13

Guidelines for the management of patients on oral anticoagulants requiring dental surgery BRITISH DENTAL JOURNAL VOLUME 203 NO. 7 OCT 13 2007
0
0,2
0,4
0,6
0,8
1
Riesgo (%)
Sangrado Trombosis
• Riesgo de sangrado bajo con INR 2 - 3.
• Realizar INR 24 h previo al procedimiento.
• Uso de surgicel, esponjas de colágeno y suturas para disminuir el sangrado.
• Enjuages con Ac tranexámico al 5%.
• No prescribir AINEs o COX-2.
martes, 10 de septiembre de 13

Guidelines for the management of patients on oral anticoagulants requiring dental surgery BRITISH DENTAL JOURNAL VOLUME 203 NO. 7 OCT 13 2007
0
0,2
0,4
0,6
0,8
1
Riesgo (%)
Sangrado Trombosis
• Riesgo de sangrado bajo con INR 2 - 3.
• Realizar INR 24 h previo al procedimiento.
• Uso de surgicel, esponjas de colágeno y suturas para disminuir el sangrado.
• Enjuages con Ac tranexámico al 5%.
• No prescribir AINEs o COX-2.
martes, 10 de septiembre de 13

Evaluation of the need to discontinue antiplateletand anticoagulant medications before cataract
surgeryJ Cataract Refract Surg 2010; 36:1115–1119
0
5
10
15
20
H subconjuntivalHifema
Hemorragia retiniana
En terapia Sin terapia
P = 0.0309
P = 0.3572
P = 0.6187
• Continuar terapia antitromboembólica.
• Riesgo de sangrado bajo con INR 2 - 3.
• Realizar INR 24 h previo al procedimiento.
• Anestesia local y/o sub tenoniana.
martes, 10 de septiembre de 13

• Riesgo extrapolado según CHADS2 y CHA2DS2-VASc.
Puntaje Riesgo
0, 1 o 2 Bajo
≥ 3, Stroke o ICT en los 3 meses previos o enf. valvular severa
Alto
VALORACIÓN DEL RIESGO TROMBOEMBÓLICOFibrilación Auricular
JAMA. 2001 Jun 13;285(22):2864-70.CHEST 2010; 137(2):263–272.
Factor de Riesgo PuntajeFalla Cardíaca 1
HTA 1Edad (Age): 65 - 74 años 1
Diabetes 1ACV/ICT/Tromboembolismo (Stroke) 2
Enfermedad Vascular 1Edad (Age): ≥ 75 años 2
Sexo (Femenino) 1
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• Riesgo depende de:• Tipo de válvulas, número, localización.• Patologías asociadas: FA, falla cardíaca, historia de tromboembolismo o
trombos intracavitarios.
• En TEV mayor riesgo dentro de los primeros 3 meses.comparison with a baseline study or serial postoperative Dopplerechocardiographic studies is often helpful, particularly when the func-tion of the valve is in question (Table 2).
1. Clinical Data. The reason for the echocardiographic study andthe patient’s symptoms should be clearly documented. Furthermore,because Doppler findings and interpretation depend on the type andsize of the replacement valve, this information and the date of surgeryshould be incorporated in the report when available, as this can beused in subsequent studies. Blood pressure and heart rate should bemeasured. The heart rate of the cardiac cycles used for Doppler mea-surements is particularly important in mitral and tricuspid prostheticvalves, because the mean gradient is dependent on the diastolic fillingperiod. Finally, the patient’s height, weight, and body surface areashould be recorded to assess whether PPM is present and to interpretcardiac chamber size.
2. Echocardiographic Imaging. The echocardiographic assess-ment of patients with prosthetic valves includes standardized mea-surement and evaluation of the size of cardiac chambers, LV wallthickness and mass, and indices of LV systolic and diastolic function
per guidelines of the ASE.10 In patients with aortic prostheses, mea-surements of the aortic root and ascending aorta are recommended.Valves should be imaged from multiple views, with particular atten-tion to the following:
! the opening and closing motion of the moving parts of the prosthesis (leaf-lets for bioprosthesis and occluders for mechanical prostheses);! the presence of leaflet calcifications or abnormal echo density attached to
the sewing ring, occluder, leaflets, stents, or cage; and! the appearance of the sewing ring, including careful inspection for regions of
separation from the native annulus and for abnormal rocking motion duringthe cardiac cycle.
In general, magnification of real-time images is necessary for bettervisualization of the leaflets or occluder mechanism. Mild thickening isoften the first sign of primary failure of a biologic valve and is a signalto follow the patient more carefully.11 Occluder motion of a mechan-ical valve may not be well visualized by transthoracic echocardiogra-phy (TTE) because of artifact and reverberations. Nevertheless,optimal 2-dimensional (2D) echocardiographic visualization of oc-cluder motion in tilting disc valves in the mitral or tricuspid positionfrequently necessitates incremental rotation of the imaging plane
Figure 1 Examples of bileaflet, single-leaflet, and caged-ball mechanical valves and their transesophageal echocardiographic char-acteristics taken in the mitral position in diastole (middle) and in systole (right). The arrows in diastole point to the occluder mechanismof the valve and in systole to the characteristic physiologic regurgitation observed with each valve. Videos 1 to 6 show the motion andcolor flow patterns seen with these valves. View video clips online.
978 Zoghbi et al Journal of the American Society of EchocardiographySeptember 2009
Riesgo Bajo Riesgo Moderado Riesgo Alto
Válvulas mecánicas
Prótesis Aórticas sin FA, stroke o eventos embólicos o trombos
intracardíacos conocidos.
Prótesis aórticas bivalvas y FA.
Cualquier prótesis mitral, otras prótesis aórticas, múltiples válvulas mecánicas, ACV, ICT o eventos cardioembólicos.
TEV TEV > 12 m y sin otros FR.
TEV 3 - 12 m, trombofilia no severa
o TEV recurrente
TEV < 3 m, trombofilia severa,
TVE no provocado o cáncer activo.
VALORACIÓN DEL RIESGO TROMBOEMBÓLICOVálvulas mecánicas y TEV
N Engl J Med 2013;368:2113-24.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• Suspensión prematura → r iesgo de trombosis del stent.
• Muerte e infarto → 75%.
• Muerte 25%.
• Stents convencionales mayor riesgo en las primeras 6 semanas.
• DES mayor riesgo en los primeros 6 meses.
• SCA terapia antiplaquetaria dual al menos 1 año.
VALORACIÓN DEL RIESGO TROMBOEMBÓLICOStents coronarios
Circulation 2011;124(23):e574-e651Journal of Cardiology (2011) 57, 231—238
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• Suspensión prematura → r iesgo de trombosis del stent.
• Muerte e infarto → 75%.
• Muerte 25%.
• Stents convencionales mayor riesgo en las primeras 6 semanas.
• DES mayor riesgo en los primeros 6 meses.
• SCA terapia antiplaquetaria dual al menos 1 año.
VALORACIÓN DEL RIESGO TROMBOEMBÓLICOStents coronarios
Circulation 2011;124(23):e574-e651Journal of Cardiology (2011) 57, 231—238
Effect of coronary endothelial function on outcomes in patients undergoing percutaneous coronary intervention 233
3
2
stentSirolimus
Bare-metal stent
1
Pro
bab
ility
of
Ste
nt
Th
rom
bo
sis
(%)
0543210
Years after Minimum Duration of RecommendedDual Antiplatelet Therapy
Figure 1 Kaplan—Meier curves for stent thrombosis in thepooled population according to stent type and the duration ofdual antiplatelet therapy. The graph shows the probability ofstent thrombosis after the use of a trial-defined minimum dura-tion of recommended dual antiplatelet therapy, according tostent type.Adapted from Kastrati et al. [14].
for reintervention after the use of SES, the risk of stentthrombosis with SES is at least as great as that seen withBMS [14] (Fig. 1). Joner et al. [15] reported that first-generation DES caused a significant delay in arterial healingas a result of persistent fibrin deposition and delayed re-endothelialization when compared with BMS implantation.Indeed, LST in the context of first-generation DES is dueto a variety of factors, including delayed arterial healing,withdrawal of antiplatelet therapy, malapposition, incom-plete apposition, and bifurcation stenting. Finn et al. [16]reported that the most powerful histological predictor ofstent thrombosis was endothelial coverage on stent struts(Fig. 2). Non-uniformity of healing is a common finding infirst-generation DES with LST and VLST. Thus, incompletehealing of the stented segment may play a major role in thepathophysiology of LST.
DES and coronary endothelial dysfunction
In the first published clinical study of coronary endothe-lial dysfunction related to first-generation DES, Togni et al.[17] assessed exercise-induced coronary vasodilator func-tion in patients with known coronary artery disease after DESimplantation. This study indicated that vasodilatory capac-ity recovered quickly in atherosclerotic arteries stentedwith BMS, but not in those stented with SES. Addition-ally, other studies used an acetylcholine provocation test toshow that first-generation DES induced focal dysfunction ofendothelium-dependent vasodilation in both proximal anddistal non-stented reference segments of coronary arter-ies for 6—12 months post-stent implantation [18,19]. Obataet al. [20] investigated coronary vasomotor function at twoweeks post-SES implantation following successful reperfu-sion therapy after acute MI. More severe constriction ofdistal epicardial coronary arteries in response to acetyl-choline was seen in patients with SES when compared with
100
90
80
70
60
50
40
Per
cent
age
End
othe
lializ
ed
30
20
10
0>402017161511987654321
Duration in monthsDESBMS
Figure 2 Line chart comparing the percentage of endothe-lialization in drug-eluting stents (DES) versus bare-metal stent(BMS) as a function of time. Note that DES (solid line) consis-tently shows less endothelialization when compared with BMS(dashed line), regardless of time point. Even beyond 40 months,DES are not fully endothelialized, whereas BMS are completelyendothelialized by six to seven months.Adapted from Joner et al. [15].
those with BMS. Furthermore, coronary blood flow andvascular endothelial growth factor levels were also sig-nificantly diminished in patients with SES than in thosewith BMS. The authors concluded that SES implantationhad an adverse effect on endothelium-dependent vasodi-lation in both epicardial and resistance coronary arteriesand reduced vascular endothelial growth factor secretion.Kim et al. [21] reported that paclitaxel-eluting stent (PES)and SES both resulted in greater endothelium-dependentvasoconstriction at corresponding segments when comparedwith BMS, but that there was no significant difference inendothelium-independent vasodilation when comparing thedifferent stents.
The first-generation DES is associated with increasedvasoconstriction when compared with BMS, and thisvasoconstriction can have adverse effect on myocardial per-fusion. Indeed, severe diffuse coronary artery spasm aftereither SES or PES has been well documented in clinicalcase reports [22,23]. Coronary vasoconstriction would resultin reduction of coronary blood flow and deterioration ofnon-laminar flow within the stented vessel, which may beassociated with an increase in inflammation and thrombosis.
Secondary prevention in the era of DES
Effect of DES on prevention of cardiac events
DES result in decreased late luminal loss and angio-graphic restenosis when compared with BMS. This decreasereduces the need for subsequent revascularization pro-cedures [24,25]. In spite of these benefits, DES isassociated with several adverse arterial responses, includingdelayed endothelialization and hypersensitivity to the poly-meric coating that regulates drug-dose-and-release kinetics
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

INTEGRACIÓN DEL RIESGO
CONTINUAR TERAPIA
CONTINUAR TERAPIA
SUSPENDER TERAPIA TERAPIA PUENTE
Bajo
Alto
Alto
Bajo
TROMBOEMBOLISMO
SAN
GR
AD
O
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13
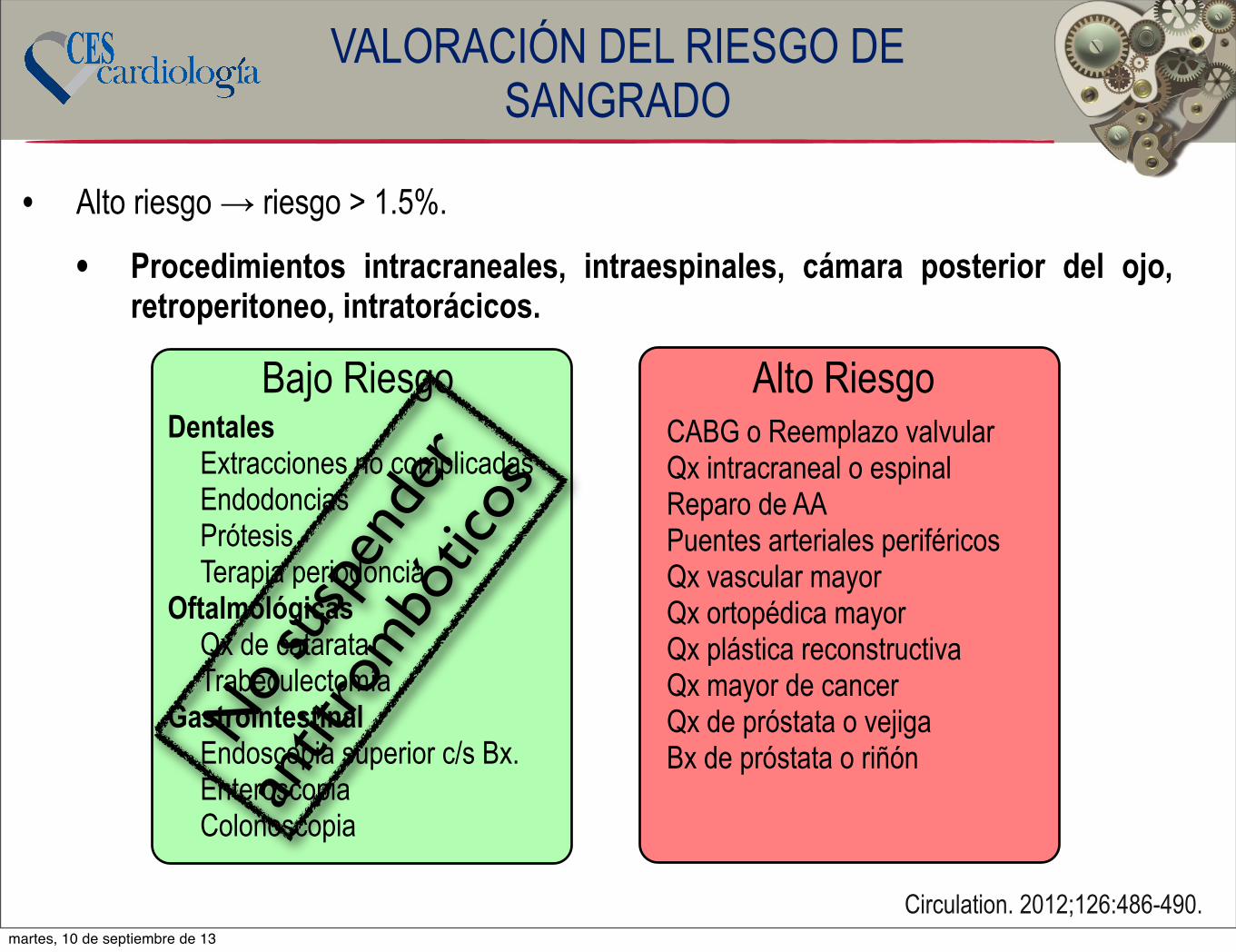
Condición Terapia puente No terapia puente
Válvulas mecánicas
Mitral, 2 o más válvulas, Reemplazo Ao (1 disco)
o con otros FR.
Prótesis aórticas (2 discos) sin FR adicionales.
FA no valvularACV o evento embólico, trombos intracardíacos,
CHADS2 ≥ 3.
No eventos embólicos, trombos o CHADS2 < 3.
TEV TEV < 3 m o trombofilia severa.
TEV > 3 m o no FR adicionales.
TERAPIA PUENTE
Circulation 2012; 126:1630-9.Thromb Haemost 2012;108: 213-6.Chest 2012;141:2 Suppl:e326S- e350S.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• En pacientes de alto riesgo de sangrado.
• Intervalo sin terapia anticoagulante lo mas corto posible.
• Considerar otros factores sobre la duración del efecto anticoagulante:
• Falla renal → dabigatran, rivaroxaban, apixaban, HBPM.
• Falla hepática → warfarina, rivaroxaban y apixaban.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?
Thromb Haemost 2012;107:803-5.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13
• 93% de los pacientes con INR 2 - 3.5 tienen un INR de 1.5 luego de 5 días de suspendida la warfarina.
• Hemostasia normal con INR de 1.5.
• INR < 1.5 → seguro para procedimientos de alto riesgo.
• INR < 1.2 → procedimientos de alto riesgo de sangrado en espacios cerrados.
• INR > 2 → ↑ en el riesgo de sangrado.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?Warfarina
Thromb J 2008;16:15
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13
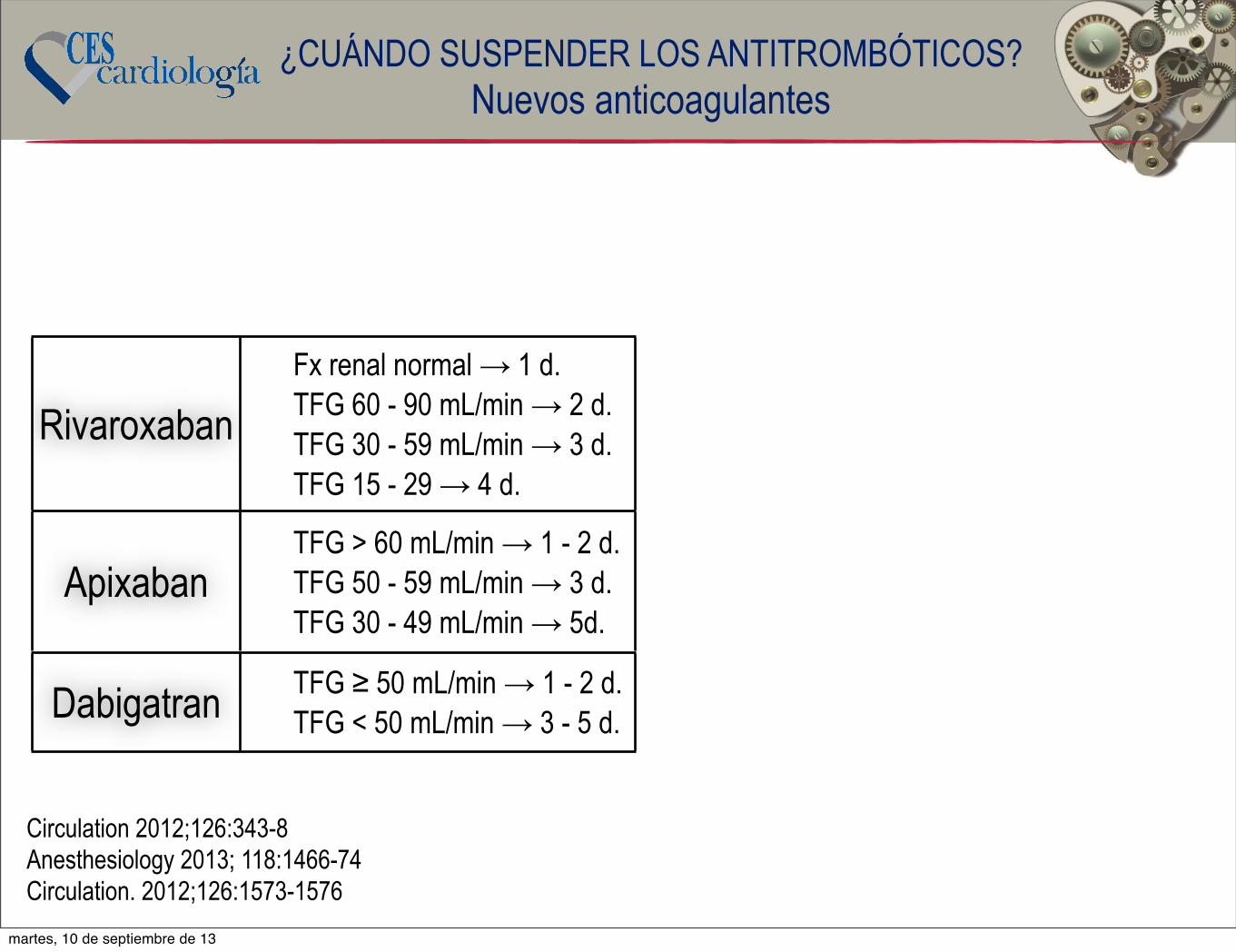
RivaroxabanFx renal normal → 1 d.TFG 60 - 90 mL/min → 2 d.TFG 30 - 59 mL/min → 3 d.TFG 15 - 29 → 4 d.
ApixabanTFG > 60 mL/min → 1 - 2 d.TFG 50 - 59 mL/min → 3 d.TFG 30 - 49 mL/min → 5d.
Dabigatran TFG ≥ 50 mL/min → 1 - 2 d.TFG < 50 mL/min → 3 - 5 d.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?Nuevos anticoagulantes
Circulation 2012;126:343-8Anesthesiology 2013; 118:1466-74Circulation. 2012;126:1573-1576
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

RivaroxabanFx renal normal → 1 d.TFG 60 - 90 mL/min → 2 d.TFG 30 - 59 mL/min → 3 d.TFG 15 - 29 → 4 d.
ApixabanTFG > 60 mL/min → 1 - 2 d.TFG 50 - 59 mL/min → 3 d.TFG 30 - 49 mL/min → 5d.
Dabigatran TFG ≥ 50 mL/min → 1 - 2 d.TFG < 50 mL/min → 3 - 5 d.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?Nuevos anticoagulantes
Circulation 2012;126:343-8Anesthesiology 2013; 118:1466-74Circulation. 2012;126:1573-1576
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
patients who require periprocedural interruption of oral anti-coagulation and bridging. How should these data should beinterpreted and incorporated in clinical practice? A majorlimitation of the analysis is the heterogeneity of the data,which is a reflection of the high variation in current clinicalpractice. Under the term bridging, several different regimeswere used, including intermediate or prophylactic doses.Moreover, a number of different procedures have beenassessed with a wide range of periprocedural bleeding risk.Similarly, a variety of events were pooled under the termsbleeding and thromboembolism. Most importantly, it is un-clear how the estimated baseline risk for thromboembolism orbleeding affected outcomes, because the indications foranticoagulation varied and high risk was variably defined ineach study.
Also, Siegal et al11 assessed the outcome of bridgingtherapy in vitamin K antagonist–treated patients only, but theincreasing availability of novel oral anticoagulants, eitherdirect thrombin or factor Xa inhibitors, brings the question ofbridging therapy with the use of these drugs. Their shorterhalf-life compared with coumarins suggests that the manage-ment of bleeding complications and the antithrombotic regi-men during operations and invasive procedures could poten-tially become simpler with these drugs.13,14 Nevertheless, theoptimal periprocedural management strategies of patientstaking the novel oral anticoagulants undergoing invasive
procedures need to be based on adequate quality evidence,which is not currently available.
Only randomized trials can perhaps address the remaininguncertainty in periprocedural anticoagulation. Currently, thePERIOP-2 (A Double Blind Randomized Control Trial ofPost-Operative Low Molecular Weight Heparin BridgingTherapy Versus Placebo Bridging Therapy for PatientsWho Are at High Risk for Arterial Thromboembolism),BRIDGE (Effectiveness of Bridging Anticoagulation forSurgery), and BRUISECONTROL (Bridge or ContinueCoumadin for Device Surgery Randomized ControlledTrial), randomized trials comparing bridging with nobridging strategies in warfarin-treated patients who requireelective surgery, are ongoing.15–17 These ongoing studiesare designed to answer relevant questions on periproce-dural anticoagulation in specific settings using specificregimes. Moreover, they will evaluate periproceduralbridging using clearly defined efficacy and safety endpoints.
BRIDGE is a prospective randomized, double-blinded studywhich aims to recruit !3600 patients with atrial fibrillation/flutter and a major risk factor for thromboembolism who requireelective surgery or invasive procedure necessitating interruptionof their oral anticoagulant therapy.16 Patients will be random-ized perioperatively to receive either subcutaneous dalteparinor placebo, and primary end points include arterial thrombo-
Chronic oral anticoagulation
VKA New OAC
Assessing thrombotic risk
low Non low
Pre-operative:- no bridgning- stop warfarin 5 days prior- check INR morning of surgery
Post-operative:- assess haemostasis- restart warfarin when feasible- VTE prophylaxis if needed
Pre-operative:- stop warfarin 5 days prior- LMWH when INR subtherapeutic
- therapeutic dose/12h if MHV- therapeutic dose daily if AF/VTE- half dose 1 day prior
- check INR morning of surgery
Post-operative:- assess haemostasis- restart warfarin when feasible- delay LMWH restart !48h- VTE prophylaxis if needed
Elective procedure scheduled
Assess creatinine clearance
<50mL/min !50mL/min
Stop dabigatran 7 days priorStop rivaroxaban 5 days prior
Stop dabigatran 5 days priorStop rivaroxaban 3 days prior
Pre-operative:- no bridging therapy needed- if high bleeding risk procedure, check haemostasis on morning of procedure
Post-operative:- assess haemostasis- re-assess creatinine clearance- delay restart !48h- VTE prophylaxis if needed
Figure. Bridging algorithm for vitamin K antagonists and new oral anticoagulants. Adapted from Wysokinski et al.8 AF indicates atrialfibrillation; INR, International Normalized Ratio; LMWH, low-molecular-weight heparin; MHV, mechanic heart valve; OAC, oral anticoag-ulants; VKA, vitamin K antagonist; and VTE, venous thromboembolism.
1574 Circulation September 25, 2012
by guest on August 15, 2013http://circ.ahajournals.org/Downloaded from
martes, 10 de septiembre de 13

RivaroxabanFx renal normal → 1 d.TFG 60 - 90 mL/min → 2 d.TFG 30 - 59 mL/min → 3 d.TFG 15 - 29 → 4 d.
ApixabanTFG > 60 mL/min → 1 - 2 d.TFG 50 - 59 mL/min → 3 d.TFG 30 - 49 mL/min → 5d.
Dabigatran TFG ≥ 50 mL/min → 1 - 2 d.TFG < 50 mL/min → 3 - 5 d.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?Nuevos anticoagulantes
Circulation 2012;126:343-8Anesthesiology 2013; 118:1466-74Circulation. 2012;126:1573-1576
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
patients who require periprocedural interruption of oral anti-coagulation and bridging. How should these data should beinterpreted and incorporated in clinical practice? A majorlimitation of the analysis is the heterogeneity of the data,which is a reflection of the high variation in current clinicalpractice. Under the term bridging, several different regimeswere used, including intermediate or prophylactic doses.Moreover, a number of different procedures have beenassessed with a wide range of periprocedural bleeding risk.Similarly, a variety of events were pooled under the termsbleeding and thromboembolism. Most importantly, it is un-clear how the estimated baseline risk for thromboembolism orbleeding affected outcomes, because the indications foranticoagulation varied and high risk was variably defined ineach study.
Also, Siegal et al11 assessed the outcome of bridgingtherapy in vitamin K antagonist–treated patients only, but theincreasing availability of novel oral anticoagulants, eitherdirect thrombin or factor Xa inhibitors, brings the question ofbridging therapy with the use of these drugs. Their shorterhalf-life compared with coumarins suggests that the manage-ment of bleeding complications and the antithrombotic regi-men during operations and invasive procedures could poten-tially become simpler with these drugs.13,14 Nevertheless, theoptimal periprocedural management strategies of patientstaking the novel oral anticoagulants undergoing invasive
procedures need to be based on adequate quality evidence,which is not currently available.
Only randomized trials can perhaps address the remaininguncertainty in periprocedural anticoagulation. Currently, thePERIOP-2 (A Double Blind Randomized Control Trial ofPost-Operative Low Molecular Weight Heparin BridgingTherapy Versus Placebo Bridging Therapy for PatientsWho Are at High Risk for Arterial Thromboembolism),BRIDGE (Effectiveness of Bridging Anticoagulation forSurgery), and BRUISECONTROL (Bridge or ContinueCoumadin for Device Surgery Randomized ControlledTrial), randomized trials comparing bridging with nobridging strategies in warfarin-treated patients who requireelective surgery, are ongoing.15–17 These ongoing studiesare designed to answer relevant questions on periproce-dural anticoagulation in specific settings using specificregimes. Moreover, they will evaluate periproceduralbridging using clearly defined efficacy and safety endpoints.
BRIDGE is a prospective randomized, double-blinded studywhich aims to recruit !3600 patients with atrial fibrillation/flutter and a major risk factor for thromboembolism who requireelective surgery or invasive procedure necessitating interruptionof their oral anticoagulant therapy.16 Patients will be random-ized perioperatively to receive either subcutaneous dalteparinor placebo, and primary end points include arterial thrombo-
Chronic oral anticoagulation
VKA New OAC
Assessing thrombotic risk
low Non low
Pre-operative:- no bridgning- stop warfarin 5 days prior- check INR morning of surgery
Post-operative:- assess haemostasis- restart warfarin when feasible- VTE prophylaxis if needed
Pre-operative:- stop warfarin 5 days prior- LMWH when INR subtherapeutic
- therapeutic dose/12h if MHV- therapeutic dose daily if AF/VTE- half dose 1 day prior
- check INR morning of surgery
Post-operative:- assess haemostasis- restart warfarin when feasible- delay LMWH restart !48h- VTE prophylaxis if needed
Elective procedure scheduled
Assess creatinine clearance
<50mL/min !50mL/min
Stop dabigatran 7 days priorStop rivaroxaban 5 days prior
Stop dabigatran 5 days priorStop rivaroxaban 3 days prior
Pre-operative:- no bridging therapy needed- if high bleeding risk procedure, check haemostasis on morning of procedure
Post-operative:- assess haemostasis- re-assess creatinine clearance- delay restart !48h- VTE prophylaxis if needed
Figure. Bridging algorithm for vitamin K antagonists and new oral anticoagulants. Adapted from Wysokinski et al.8 AF indicates atrialfibrillation; INR, International Normalized Ratio; LMWH, low-molecular-weight heparin; MHV, mechanic heart valve; OAC, oral anticoag-ulants; VKA, vitamin K antagonist; and VTE, venous thromboembolism.
1574 Circulation September 25, 2012
by guest on August 15, 2013http://circ.ahajournals.org/Downloaded from
?martes, 10 de septiembre de 13

• En pacientes con depuración de Cr < 30 se prefiere la HNF.
• Protocolo con HBPM:
• Suspender warfarina 5 días antes del procedimiento de alto riesgo.
• En pacientes con nuevos anticoagulantes iniciar 12 horas luego de la última dosis.
• Iniciar HBPM cuando el INR esté por debajo del rango terapéutico:
• Válvulas mecánicas o FA → Enoxa 1mg/kg o Dalte 100U/kg cada 12 horas.
• TEV →1.5mg/kg o Dalte 200U/kg cada 24 horas.
24 h antes del procedimiento}
TERAPIA PUENTE
Transfusion 2012;52:Suppl 1: 45S-55SChest 2012;141:2 Suppl:e326S- e350S
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• HNF
• Vida ½ IV → 60 - 90 min.
• Suspender 4 - 6 h antes de procedimientos de alto riesgo.
• HBPM
• Vida ½ 4 horas.
• Suspender 24 horas antes del procedimiento.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?Heparinas
Chest 2012;141:2 Suppl:e326S- e350S
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

• ASA
• Dosis bajas solas → no aumento importante del riesgo de sangrado.
• Cilostazol
• No aumento del riesgo cuando se usa solo.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?Antiplaquetarios
N Engl J Med 2013;368:2113-24.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

ASA 7 días
Cilostazol 2 días
Inhibidores P2Y12Clopidogrel o ticagrelor 5 días.
Prasugrel 7 días.
¿CUÁNDO SUSPENDER LOS ANTITROMBÓTICOS?Antiplaquetarios
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

Thrombosis and Haemostasis 105.5/2011
743 © Schattauer 2011Consensus Document
Peri-operative management of antiplatelet therapy in patients with coronary artery disease Joint position paper by members of the working group on Perioperative Haemostasis of the Society on Thrombosis and Haemostasis Research (GTH), the working group on Perioperative Coagulation of the Austrian Society for Anesthesiology, Resuscitation and Intensive Care (ÖGARI) and the Working Group Thrombosis of the European Society for Cardiology (ESC)
Wolfgang Korte1; Marco Cattaneo2; Pierre-Guy Chassot3; Sabine Eichinger4; Christian von Heymann5; Niklaus Hofmann6; Hans Rickli7; Michael Spannagl8; Bernhard Ziegler9; Freek Verheugt10; Kurt Huber11 1Center for Laboratory Medicine, Kantonsspital St. Gallen, Switzerland; 2Medicina 3, Ospedale San Paolo, Department of Medicine, Surgery and Dentistry, Università degli Studi di Milano, Milan, Italy; 3Departement of Anesthesiology, University Hospital Lausanne, Switzerland; 4Department of Medicine I, Division of Hematology, Medical University of Vienna, Austria; 5Department of Anesthesiology and Intensive Care, Charité-Universitätsmedizin Berlin, Germany; 6Department of Anesthesiology, Diakonissen-Krankenhaus Salzburg, Austria; 7Division of Cardiology, Kantonsspital St. Gallen, Switzerland; 8Division of Haemostaseology, University of Munich, Germany; 9Department of Anesthesiology, Landeskliniken Salzburg, Austria; 10Department of Cardiology, Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands; 113rd Medical Department, Cardiology and Emergency Medicine, Wilhelminenspital, Vienna, Austria
Summary An increasing number of patients suffering from cardiovascular dis-ease, especially coronary artery disease (CAD), are treated with aspirin and/or clopidogrel for the prevention of major adverse events. Unfor-tunately, there are no specific, widely accepted recommendations for the perioperative management of patients receiving antiplatelet ther-apy. Therefore, members of the Perioperative Haemostasis Group of the Society on Thrombosis and Haemostasis Research (GTH), the Perioper-ative Coagulation Group of the Austrian Society for Anesthesiology, Reanimation and Intensive Care (ÖGARI) and the Working Group Thrombosis of the European Society of Cardiology (ESC) have created this consensus position paper to provide clear recommendations on the perioperative use of anti-platelet agents (specifically with semi-urgent and urgent surgery), strongly supporting a multidisciplinary approach to optimize the treatment of individual patients with coronary artery disease who need major cardiac and non-cardiac surgery. With planned
Correspondence to: PD Dr. Wolfgang Korte Center for Laboratory Medicine Kantonsspital St. Gallen CH-9007 St. Gallen, Switzerland Tel.: +41 71 494 39 33, Fax: +41 71 494 39 00 E-mail: [email protected]
surgery, drug eluting stents (DES) should not be used unless surgery can be delayed for !12 months after DES implantation. If surgery cannot be delayed, surgical revascularisation, bare-metal stents or pure balloon angioplasty should be considered. During ongoing antiplatelet therapy, elective surgery should be delayed for the recommended duration of treatment. In patients with semi-urgent surgery, the decision to pre-maturely stop one or both antiplatelet agents (at least 5 days pre-oper-atively) has to be taken after multidisciplinary consultation, evaluating the individual thrombotic and bleeding risk. Urgently needed surgery has to take place under full antiplatelet therapy despite the increased bleeding risk. A multidisciplinary approach for optimal antithrombotic and haemostatic patient management is thus mandatory.
Keywords Antiplatelet agents, surgery, atherothrombosis, coronary syndrome, atherosclerosis
Financial support: The meeting that allowed this manuscript to be formulated was supported by sanofi aventis (suisse) sa (a manufacturer of clopidogrel and enoxaparin). However, sanofi aventis had no influence whatsoever on the contents of this mansucript. Received: April 7, 2010 Accepted after major revision: January 28, 2011 Prepublished online: March 24, 2011
doi:10.1160/TH10-04-0217 Thromb Haemost 2011; 105: 743–749
Introduction
An increasing number of patients who are suffering from or are at risk for cardiovascular disease, especially coronary artery disease (CAD), is treated with aspirin or clopidogrel for the prevention of major adverse events. In congruence, the number of patients that receive percutaneous coronary intervention (PCI) with stent im-plantation continues to increase and therefore, the need for treat-ment with dual antiplatelet therapy (usually aspirin plus clopido-
grel) is also augmented. In addition, an increased use of new and possibly more effective antiplatelet agents, e.g. prasugrel or ticagre-lor, can be expected in the near future (1, 2). At present, 6–8% of patients with dual antiplatelet therapy also need oral anticoagu-lation with vitamin K antagonists (VKA) due to atrial fibrillation, mechanical heart valves or a history of venous thromboembolism. Given these facts, physicians nowadays face situations in which the peri-operative bleeding risk has to be balanced against the individ-ual risk of thrombotic complications. Although the pathophysiol-
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.thrombosis-online.com on 2013-07-08 | IP: 190.29.20.198
Qx menor: No suspender TAP.HBPM: No son útiles para la inhibición plaquetaria.
Qx menor: No suspender TAP.HBPM: No son útiles para la inhibición plaquetaria.
Qx menor: No suspender TAP.HBPM: No son útiles para la inhibición plaquetaria.
Qx menor: No suspender TAP.HBPM: No son útiles para la inhibición plaquetaria.
Qx mayor y Que hacer Excepciones Que hacerASA para
prevención primariaSuspender ASA 5 d antes de la cirugía
ASA en pacientes de alto riesgo Continuar ASA
Qx en espacios cerrados o alto
riesgo de sangrado
Suspender ASA 5 d antes de la cirugía.
Considerar el reinicio a las 24 horas.
ASA + Clopidogrel en pacientes de
alto riesgo
1.Qx electiva: Aplazar.2.Qx semi urgente: continúe
ASA ± Clopidogrel según sea el caso.
3.Qx urgente (24 horas): Continúe ASA y clopidogrel.
Qx en espacios cerrados o alto
riesgo de sangrado
Si no es posible aplazar la Qx / Qx semi urgente:
1. Suspender el clopidogrel 5 d antes.
2. Considerar continuar ASA.3. Considerar reinicio de TAPD
lo antes posible.
Thromb Haemost 2011; 105: 743–749martes, 10 de septiembre de 13

• Determinante del riesgo de sangrado postQx.
• Profilaxis → reiniciar una vez se garantice la hemostasia.
• Heparina → reiniciar a las 24 - 48 horas.
• Warfarina → reiniciar al día siguiente del procedimiento.
• Dabigatran, rivarixaban o apixaban → reiniciar a las 48 horas luego de procedimientos de alto riesgo de sangrado.
• Clopidogrel → 24 h luego del procedimiento.
¿CUÁNDO REINICIAR LOS ANTITROMBÓTICOS?
N Engl J Med 2013;368:2113-24.
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13

Procedimiento de bajo riesgo de sangrado
Warfarina TAPD
ContinuarContinuar
Bajo riesgo tromboemból
• Suspender warfarina
• Reiniciar al otro día del procedimiento.
• Medir INR a la semana.
Procedimiento de alto riesgo de
sangrado
Warfarina TAPD
Alto riesgo tromboemból
Bajo riesgo tromboemból
Alto riesgo tromboemból
Terapia puente
• Suspender clopidogrel 5 días antes.
• Continuar ASA.
• Considerar suspender clopidogrel y/o ASA 5 días antes.
• Considerar Terapia puente.
EN RESUMEN...
Informes: CES-CARDIOLOGÍA Cr. 43 No 36 - 02 Of. 1101 Tels: (4) 4447378 (4) 576 73 86
Aliar Comunicaciones (Firma operadora del evento) Tel: (4) 444 22 60.
PROGRAMACIÓN
XVI CONGRESO ESTADO ACTUAL EN ENFERMEDADES CARDÍACAS Y VASCULARES 2013.
Plaza Mayor Medellín 14,15 y 16 de Agosto de 2013 Miércoles 14 de Agosto Salones 5 y 6 Simposio: Hemodinamia, Cardiología Intervencionista y Vascular Periférico 2 a 6 p.m.: Coordinador César Hernández, MD. 2:00 - 2:30 p.m. Ablación simpática renal, muchos dispositivos pocos pacientes Álvaro Escobar, MD. 2:30 - 3:00 p.m. Cierre de Foramen Ovale, Decisión multidisciplinaria?
Diego Velásquez, MD. 3:00 - 3:30 p.m. Stents medicados: Estado Actual
César Hernández, MD. 3:30 - 4:00 p.m. Intervención percutánea en válvula mitral: Mitraclip y más
Iván Rendón, MD.
4:00 - 4:30 p.m. Descanso 4:30 - 5:00 p.m. Actualización en antiplaquetarios: un medicamento para cada
paciente? César Hernández, MD.
5:00 - 5:50 p.m. Revascularización coronaria en Diabéticos. Debate. Quirúrgica Luis Andrés Vélez, MD.
Percutánea Álvaro Escobar, MD. Manejo Médico Alex Londoño, MD.
martes, 10 de septiembre de 13