Embed Size (px)
Citation preview

1
Routes of Cancer Dissemination in Metastatic Disease
Maura KennedyHarvard Medical School Year III
Gillian Lieberman, M.D.
Maura Kennedy November 2004
Gillian Lieberman, M.D.

2
Mechanisms of Cancer Spread
• Local Invasion– Infiltration, invasion and destruction of surrounding
tissue• Metastasis
– Lymphangitic Spread• carcinomas
– Hematagenous Spread• sarcomas
– Direct Seeding• peritoneum
Maura Kennedy November 2004
Gillian Lieberman, M.D.

3
Lymphangitic Spread
• Most common pathway for dissemination of carcinoma
• Follows natural route of drainage• Lymphadenopathy
– Spread and growth of cancer cells and/or– reactive hyperplasia
• Can be anterograde or retrograde
Maura Kennedy November 2004
Gillian Lieberman, M.D.

4
Lymphangitic Spread Patient #1
• Presented the end of 2003 with hemoptysis• 40 pack-year history of smoking• Chest Radiograph and CT
Maura Kennedy November 2004
Gillian Lieberman, M.D.

5
Lymphangitic Spread: Patient #1
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

6
Lymphangitic Spread: Patient #1
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

7
• Pleural lymphatics: – course over visceral pleural surface– drain into hilar nodes at medial
aspect of lung– anastamose with the parencyhmal
lymphatics• Parenchymal lymphatics:
– interlobular septal and bronchovascular bundles
– anastamose intralobular
interlobar lobar hilar nodes
• Hilar nodes drain to mediastinum
Lymphangitic Spread: Patient #1
Maura Kennedy November 2004
Gillian Lieberman, M.D.

8
Lymphangitic Spread: Patient #1
• RUL R paratracheal and anterior mediastinal LN
• RML and RLL subcarinal R paratracheal
and anterior mediastinal LN• LUL subaortic and
paraaortic LN• LLL subcarinal and
subaortic nodesMcLoud et al. Rad Clin N Am 1982; 20: 453-468
Maura Kennedy November 2004
Gillian Lieberman, M.D.

9
• Approx. 1 yr. later presents with new cough• New and enlarged lymphadenopathy
– Supraclavicular– Mediastinal– Pretracheal– Subcarinal– Hilar
Lymphangitic Spread: Patient #1
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

10Left Subclavicular LN (1.4 x 1.9 cm)
Lymphangitic Spread: Patient #1
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

11Right Subclavicular LN (1.1 x 1.4 cm)
Lymphangitic Spread: Patient #1
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

12
Right Hilar LN (1.5 x 1.5 cm)
Lymphangitic Spread: Patient #1
Left Hilar LN (2.2 x 2.2 cm)
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

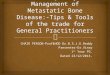
13
• Focal Narrowing of L lingular bronchus due to soft tissue mass 2.0 x 2.2 cm at left hilum
Lymphangitic Spread: Patient #1
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

14
Imaging Techniques and Staging
• CT: – PPV = 0.56– NPV = 0.83
• FDG PET– PPV 0.79– NPV 0.93
Nodal Status
Definition
N0 No regional LN metastasis
N1 Ipsilateral peribronchial, hilar, or intrapulmonary LN
N2 Ipsilateral mediastinal and/or subcarinal lymph LN
N3 Contralateral mediastinal or hilar LN or to ipsilateral or contralateral supraclavicular LN
Lymphangitic Spread: Patient #1
Maura Kennedy November 2004
Gillian Lieberman, M.D.

15
Patient #1 – Vertebral Metastases• Additional Sx: Back Pain• CT and Bone Scan confirmed metastases to
T12 and L pubic ramus
PACS, BIDMC
Maura Kennedy November 2004
Gillian Lieberman, M.D.

16
• Typical metastatic route for sarcomas• Veins more readily invaded than arteries
– Portal v. invasion/its tributary liver metastases
– IVC invasion/its tributaries lung metastases– Thyroid and prostate cancer can invade
invasion paravertebral plexus lung metastases
Hematagenous Spread
Maura Kennedy November 2004
Gillian Lieberman, M.D.

17
Hematagenous Spread: Patient #2
• Papillary Thyroid Carcinoma– diagnosed in childhood– s/p thyroidectomy– routine surveillance for recurrence
Maura Kennedy November 2004
Gillian Lieberman, M.D.

18
Hematagenous Spread: Patient #2
SVC
Vascular Invasion and distant metastases:• 10-15% papillary carcinoma
•metastases to lung, bone, and mediastinum
• Up to 50% follicular carcinomas•Metastases to lung, bone, brain
Moore and Agur. Essential Clinical Anatomy 2nd
Edition. Lippincott Williams and Wilkins. 2002
Maura Kennedy November 2004
Gillian Lieberman, M.D.

19Courtesy J Anthony Parker, M.D., Nuclear Medicine, BIDMC
Hematagenous Spread: Patient #2
5 days s/p I131
(CT: 8 small, non-specific pulmonary nodules bilaterally, < 4 mm
Maura Kennedy November 2004
Gillian Lieberman, M.D.

20
• I131 imaging
• Patient with metastatic follicular thyroid carcinoma
• Multiple skeletal and pulmonary metastases.
Hematagenous Spread: Thyroid Metastases
Sherman. Lancet 2003; 361: 501-511
Maura Kennedy November 2004
Gillian Lieberman, M.D.

21
I131 scan: diffuse metastatic pulmonary nodulesChest radiograph: diffuse nodularity. www. Auntminnie.com
Hematagenous Spread: Thyroid Metastases
Maura Kennedy November 2004
Gillian Lieberman, M.D.

22
Dissemination of Ovarian Cancer• Direct Spread• Intraperitoneal Dissemination• Lymphatics• Hematagenous SpreadFIGO Staging Criteria:I: confined to ovariesII: peritoneal metastasesIII: extrapelvic peritoneal masses, abdominopelvic nodal
massesIV: metastases outside abdomen and pelvis
Maura Kennedy November 2004
Gillian Lieberman, M.D.

23
• Surrounding Pelvic Tissue– Fallopian Tubes– Uterus– Contralateral Ovary
• Bladder• Rectum• Pelvic Sidewall
Ovarian Cancer: Direct Extension
Maura Kennedy November 2004
Gillian Lieberman, M.D.

24
• Black Arrow: Irregular border between left ovary and uterus
• Curved arrow: irregular nodularity in surrounding tissues.
• Ascites
Ovarian Cancer: Direct Extension
Woodward et al. Radiographics 2004; 24 (1): 225-245
Maura Kennedy November 2004
Gillian Lieberman, M.D.

25
Ovarian Cancer: Intraperitoneal Dissemination
• Present in up to 70% patients undergoing staging laparotomy
• Exfoliation of malignant cells into peritoneal fluid, following natural flow of peritoneal fluid in the peritoneal cavity
• Dissemination along mesentery and ligaments
Maura Kennedy November 2004
Gillian Lieberman, M.D.

26
Ovarian Cancer: Intraperitoneal Dissemination
Peritoneal Fluid Circulation:
• Caudal with gravity
• Cephalad with expiration
• Fluid directed by bowel peristalsis and peritoneal reflections and mesenteries
Raptopoulos, Gourtsoyiannis Eur Radiol (2001) 11:2195-2206
Maura Kennedy November 2004
Gillian Lieberman, M.D.

27Raptopoulos, Gourtsoyiannis Eur Radiol (2001) 11:2195-2206
Peritoneal Fluid Collections:• L infracolic pelvis• R infracolic ileoceccal jx
(overflow to Pouch of Douglas)
Peritoneal Seeding – Main Sites• pouch of Douglas• paracolic gutters• surface of small and large bowel• greater omentum• liver surface• subphrenic space
Ovarian Cancer: Intraperitoneal Dissemination
Maura Kennedy November 2004
Gillian Lieberman, M.D.

28
Radiographic Signs:• plaque like or nodular peritoneal, omental, mesenteric
implants• nodularity, thickening, or enhancement of peritoneal
surfaces• bowel wall thickening or distortion• capsular liver involvement: smooth, well defined,
elliptical, biconvesx appearance.• ascites is non-specific sign, but suggestive
Ovarian Cancer: Intraperitoneal Dissemination
Maura Kennedy November 2004
Gillian Lieberman, M.D.

29
Coakley. Radiol Clin N Am 40 (2002) 609-636
Ovarian Cancer: Intraperitoneal Dissemination
Woodward et al. Radiographics 2004; 24 (1): 225-245
Nodularity or scalloping of liver capsule; no parenchymal invasion
Maura Kennedy November 2004
Gillian Lieberman, M.D.

30
Ovarian Cancer: Intraperitoneal Dissemination
Coakley/Radiol Clin N Am 40 (2002) 609-636
Peritoneal implants in left pericolic gutter
Omental cake: peritoneal implants in greater omentum
Maura Kennedy November 2004
Gillian Lieberman, M.D.

31Mesenteric Infilitration
Sheth et al. RadioGraphics 2003; 23: 457-473
Ovarian Cancer: Intraperitoneal Dissemination
Maura Kennedy November 2004
Gillian Lieberman, M.D.

32
Summary
• Local Invasion– Example: ovarian cancer
• Metastasis– Lymphangitic Spread
• Example: lung cancer– Hematagenous Spread
• Example: thyroid cancer– Direct Seeding
• Example: ovarian cancer
Maura Kennedy November 2004
Gillian Lieberman, M.D.

33
Summary
• Understanding mechanisms of metastatic spread of cancers can assist the radiologist– Evaluation of radiologic studies for evidence of
metastatic or recurrent disease– Assist surgeon/oncologist in cancer staging– Identify primary cancer in patient presenting
with metastatic cancer of unknown origin
Maura Kennedy November 2004
Gillian Lieberman, M.D.

34
Acknowledgements
Special thanks to:• Jesse Wei, M.D.• J. Anthony Parker, M.D.• Gillian Lieberman, M.D.• Pamela Lepkowski• Larry Barbaras
Maura Kennedy November 2004
Gillian Lieberman, M.D.

35
References• McLoud TC and Meyer JE. Mediastinal Metastases. Rad Clin N Am
1982; 20: 453-468• Chen L, Berek J. Clinical Manifestations, diagnosis, and staging of
ovarian cancer. UpToDate 2004.• Coakley FV. Staging ovarian cancer: role of imaging. Radiol Clin N.
Am, 2002; 40: 609-636• Park CM, Kim SH, Kim SH, Moon MH, Kim KW, Choi HJ.
Recurrent ovarian malignancy: patterns and spectrum of imaging findings.Raptopoulus V, Gourtsoyiannis N. Eur Radiol 2001; 11: 2195-2206.
• Sharma A et al. Patterns of Lympadenopathy in Thoracic Malignancies. Radiographics 2004; 24: 419-434
• Sherman SI. Thyroid Carcinoma. Lancet 2003; 361: 501-511
Maura Kennedy November 2004
Gillian Lieberman, M.D.

36
References (cont)• Sheth S, Horton KM, Garland MR, Fishman EK. Mesenteric
Neoplasms: CT Appearances of Primary and Secondary Tumors and Differential Diagnosis. Radiographics 2003; 23: 457-473.
• Woodward PJ, Hosseinzadeh K, Saenger JS. From the Archives of the AFIP Radiologic Staging of Ovarian Carcinoma with Pathologic Correlation. RadioGraphics 2004; 24: 225-246
• Intraperitoneal Spread of Malignancies. In Dynamic Radiology of the Abdomen: Normal and Pathology Anatomy, 4th Edition. Myers MA. © 1994, Springer-Verlag, NY.
• Neoplasia. In Robbins Pathologic Basis of Disease, 6th Edition. Cotran RS, Kumar V, and Collins T (ed). © 1999. W.B. Saunders Co. Philadelphia
• www.auntminnie.com. Thyroid Carcinoma
Maura Kennedy November 2004
Gillian Lieberman, M.D.

37
Lymphatic drainage routes:1. Along ovarian vessels
retroperitoneal paraaortic and paracaval LN
2. Laterally along broad ligament
internal iliac and obturator LN of pelvic side wall
3. Along round ligament inguinal nodes groin metastases
4. 80% peritoneal fluid drains via diaphragmatic LN LAD of anterior diaphragmatic nodes behind sternum and lateral diaphragmatic LN near phrenic nerves
Ovarian Cancer: Lymphangetic Spread
Moore and Agur. Essential Clinical Anatomy 2nd
Edition. Lippincott Williams and Wilkins. 2002
3
2
14
Maura Kennedy November 2004
Gillian Lieberman, M.D.

38
Ovarian Cancer: Lymphangetic Spread
Lymphatic metastases along obturator lymphatic chain
Lymph node metastases in retroperitoneum
Coakley. Radiol Clin N Am 40 (2002) 609-636
Maura Kennedy November 2004
Gillian Lieberman, M.D.

39
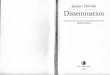
Ovarian Cancer: Hematagenous Spread
• Least common metastatic mode for ovarian cancer
• Most common site = liver– Left ovarian vein left renal vein portal
veins• 2nd most common site = lung
– Right ovarian vein IVC lung metastases
Maura Kennedy November 2004
Gillian Lieberman, M.D.

40Coakley. Radiol Clin N Am 40 (2002) 609-636
Ovarian Cancer: Hematagenous Spread to Liver
Maura Kennedy November 2004
Gillian Lieberman, M.D.