-
8/14/2019 Miyashita Paper
1/7
Diabetes Research and Clinical Practice 65 (2004) 235241
Beneficial effect of low carbohydrate in low calorie diets
onvisceral fat reduction in type 2 diabetic patients with
obesity
Yoh Miyashita a, Nobukiyo Koide a, Masaki Ohtsukaa, Hiroshi
Ozaki a, Yoshiaki Itoh a,
Tomokazu Oyamaa
, Takako Uetakeb
, Kiyoko Arigab
, Kohji Shiraia,
a Center of Diabetes, Endocrine and Metabolism, Sakura Hospital,
School of Medicine, Toho University,
564-1 Shimoshizu, Sakura-City, Chiba 285-0841, Japanb Department
of Nutritione, Sakura Hospital, School of Medicine, Toho
University, Chiba, Japan
Received 15 March 2003; received in revised form 9 December
2003; accepted 29 January 2004
Abstract
The adequate composition of carbohydrate and fat in low calorie
diets for type 2 diabetes mellitus patients with obesity is not
fully established.The aimof this study was to investigate
theeffectsof lowcarbohydrate diet on glucose andlipid metabolism,
es-
pecially on visceral fat accumulation, andcomparing that of a
high carbohydrate diet. Obese subjects with type 2 diabetes
mellitus
were randomly assigned to take a low calorie and low
carbohydrate diet (n = 11, 1000 kcal per day,
protein:carbohydrate:fat =25:40:35) or a low calorie and high
carbohydrate diet (n = 11, 1000 kcal per day,
protein:carbohydrate:fat = 25:65:10) for 4
weeks. Similar decreases in body weight and serum glucose levels
were observed in both groups. Fasting serum insulin levels
were reduced in the low carbohydrate diet group compared to the
high carbohydrate diet group (30% versus10%, P < 0.05).
Total serum cholesterol and triglyceride levels decreased in
both groups, but were not significantly different from each
other.
High-density lipoproteincholesterol (HDLC) increased in the low
carbohydrate diet group but not in the high carbohydrate
diet group (+15% versus 0%, P < 0.01). There was a larger
decrease in visceral fat area measured by computed tomography
in the low carbohydrate diet group compared to the high
carbohydrate diet group (40cm2 versus 10cm2, P < 0.05). The
ratio of visceral fat area to subcutaneous fat area did not
change in the high carbohydrate diet group (from 0.70 to 0.68), but
it
decreased significantly in the low carbohydrate diet group (from
0.69 to 0.47, P < 0.05). These results suggest that, when
restrict
diet was made isocaloric, a low calorie/low carbohydrate diet
might be more effective treatment for a reduction of visceral
fat,
improved insulin sensitivity and increased in HDLC levels than
low calorie/high carbohydrate diet in obese subjects with type
2 diabetes mellitus.
2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Low carbohydrate diet; Low calorie diet; Type 2
diabetes mellitus; Obesity; Visceral fat
Corresponding author. Tel.: +81-43-462-8811;
fax: +81-43-489-9770.
E-mail address: [email protected] (K. Shirai).
1. Introduction
The distribution of body fat is known to be im-
portant in the development of obesity-associated
metabolic disorders. In particular, accumulation of
visceral fat is related to the development of insulin
0168-8227/$ see front matter 2004 Elsevier Ireland Ltd. All
rights reserved.
doi:10.1016/j.diabres.2004.01.008
-
8/14/2019 Miyashita Paper
2/7
236 Y. Miyashita et al. / Diabetes Research and Clinical
Practice 65 (2004) 235241
resistance [1,2] and to a high incidence of coronaryheart
disease [3,4].
A low calorie diet is recognized to be a fundamen-
tal therapy for type 2 diabetic patients with obesity
to improve insulin sensitivity by weight reduction. A
principle of this diet is to provide an adequate amount
of proteins, vitamins and minerals, and to restrict car-
bohydrates and fats as energy components. There have
been several reports concerning the role of nutrient
composition of the diet for weight reduction in obe-
sity [57]. For example, Rabast et al. [5] reported that
low carbohydrate diet is beneficial for weight reduc-
tion, which is associated with low insulin levels and a
suppression of appetite by ketone body formation. On
the other hand, Yong and Werner et al. reported that
low carbohydrate diet is not always superior to high
carbohydrate diet for body weight reduction [6,7]. As
a result, there is no definite evidence for appropriate
ratio of carbohydrate in low calorie diet.
Recently, in rats given a normal calorie diet, Zava-
roni and Reaven et al. [8] reported that a diet composed
of 60% carbohydrates raised glucose levels and de-
creased insulin sensitivity in rats. Furthermore, Coul-
ston and co-workers [9] reported that high carbohy-
drate diet increased serum glucose, insulin and triglyc-
eride levels, and decreased HDLC in diabetic pa-tients.
We have previously reported that low calorie diet
composed of low carbohydrate is preferable for an im-
provement of glucose and lipoprotein metabolism in
type 2 diabetes mellitus patients with obesity [10]. In
this paper, to clarify whether high or low carbohydrate
diet is more beneficial for type 2 diabetes mellitus pa-
tients with obesity, the effects of both diets on visceral
fat accumulation as well as parameters of glucose and
lipid metabolism were studied.
2. Subjects and methods
2.1. Subjects
Twenty-two obese subjects with type 2 diabetes
mellitus patients were recruited for the study (16
males, 6 females, mean body mass index 27 kg/m2).
The mean age was 52.4 13.0 years old. They were
all hospitalized and took no medication. All of sub-
jects gave informed consent.
2.2. Diet composition
The ratio of the low carbohydrate diet compositions
of protein, carbohydrate and fat was 25:39:35 (%), and
in high carbohydrate diet, the ratio was 26:62:10 (%).
The ratio of saturated fatty acids, monounsaturated
fatty acids and polyunsaturated fatty acids were 3:4:3
in both diets. Palmitic acid constituted about 70% of
the saturated fatty acids, oleic acid about 95% of the
monounsaturated fatty acids, and a linoleic acid about
70% of the polyunsaturated fatty acids. The content
of dietary fibers was about 18 g per day in the low
carbohydrate diet and about 20 g per day in the high
carbohydrate diet.
2.3. Program of diet therapy
The subjects were initially given a 3 day low calo-
rie diet composed of high carbohydrate (1000 kcal per
day, P:F:C = 26:10:62), after which they were divided
into two random groups. One group of subjects was
treated with a low calorie diet composed of low car-
bohydrate (=low carbohydrate diet group, n = 11),
and the other was treated with a low calorie diet com-
posed of high carbohydrate (=high carbohydrate diet
group, n = 11). The clinical profile of the subjectsat the start
of the different diet therapies is shown in
Table 1. There were no significant differences between
the two groups. The subjects were treated for 4 weeks
with these diets. During this study, all patients were
without medications and treated with exercise therapy
(walking, 30 min 2 times per day).
2.4. Blood sampling
Blood samples were taken in the morning after 12 h
of fasting. Serum was obtained within 1 h and samples
were used for measuring of blood sugar (FBS), insulin(basal
IRI), serum total cholesterol (TC), triglyceride
(TO) and HDLC.
2.5. Measurement of body weight and total body fat
Body weight and total body fat were measured in
the morning after 12 h of fasting. The percent body
fat (%) and lean body mass (LBM) were measured by
impedance method using Serkoimpemeter (SIF-93 1,
Serko, Japan).
-
8/14/2019 Miyashita Paper
3/7
Y. Miyashita et al. / Diabetes Research and Clinical Practice 65
(2004) 235241 237
Table 1Clinical profiles of low carbohydrate diet group or high
carbohydrate diet group before treatment
High carbohydrate group (n = 11) Low carbohydrate group (n = 11)
Significance
Body mass index 27 2 27 4 None
V/S ratioa 0.71 0.8 0.69 0.7 None
HbAlc (%) 9.8 2 10.2 2 None
Fasting blood sugar (mg/dl) 200 50 207 36 None
Basal IRI (U/ml) 5.9 1.0 6.2 0.9 None
Total cholesterol (mg/dl) 193 48 199 35 None
Triglyceride (mg/dl) 173 60 175 89 None
HDLC (mg/dl) 39 16 38 10 None
a The ratio of visceral fat area/subcutaneous fat area.
2.6. Measurement of adipose tissue distribution
To measure visceral and subcutaneous fat mass,
computed axial tomography was performed [1]. The
scan was performed at the position of the navel. Vis-
ceral fat area was measured by drawing a line within
the muscle wall surrounding the abdominal cavity. The
subcutaneous fat was calculated by subtracting the
amount of visceral fat from the total fat area. From
these values, a ratio of visceral fat area to subcuta-
neous fat area (V/S ratio) and an area of visceral fat
was obtained.
2.7. Statistical analysis
Statistical analysis was performed using Students
t-test and paired t-test. P values less than 0.05 were
considered significant.
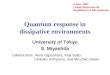
Fig. 1. Changes in body weight, body fat (%) and lean body mass
during low calorie diets in low carbohydrate diet group ( ) and
high
carbohydrate diet group (). (AC) Show changes of body weight,
body fat (%), and lean body mass, respectively. Data are shown
as
mean S.D.
3. Results
3.1. Change in the body weight, fat (%) and LBM
In the low carbohydrate and the high carbohydrate
diet groups, the body weight decreased from 73 to
64 kg, and from 71 to 64 kg, respectively, after low
calorie diet for 4 weeks (Fig. 1A). During these low
calorie diet therapies, fat (%) decreased in both groups,
with no change in LBM in either group (Fig. 1B).
These changes in body weight, body fat (%) and LBM
were not significantly different between the low and
high carbohydrate diet groups (Fig. 1A and B).
3.2. Change in FBS and basal IRI
In low carbohydrate and high carbohydrate diet
groups, FBS decreased from 207 to 104 mg/dl, and
-
8/14/2019 Miyashita Paper
4/7
238 Y. Miyashita et al. / Diabetes Research and Clinical
Practice 65 (2004) 235241
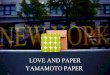
Fig. 2. Effect of the low carbohydrate diet () and the high
car-bohydrate diet () on fasting blood glucose levels. Fasting
blood
glucose levels were decreased in both groups with no
significant
difference between the two groups. Data are shown as
meanS.D.
from 200 to 102 mg/dl, respectively after low calorie
diet for 4 weeks. There was no significant difference
between two groups (Fig. 2).
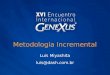
Basal IRI showed a larger decrease in low carbo-
hydrate diet group compared to the high carbohydrate
diet group (Fig. 3A). The decreasing rate of basal IRI
was significantly high in low carbohydrate diet group
compared to high carbohydrate group (Fig. 3B).
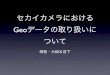
3.3. Change in serum lipids
TC and TG were decreased by about 20%, and
4050% in low carbohydrate diet group and high
carbohydrate diet group during low calorie diet, but
Fig. 3. Changes in IRI during low calorie diets in low
carbohydrate diet group (closed circle and solid bar) and high
carbohydrate diet
(open circle and open bar). (A and B) Show change and ratio of
decrease of basal IRI. Data are shown as mean S.D., P <
0.05.
no significant difference was observed between bothgroups (Fig.
4A and B).
HDLC was significantly increased in the low car-
bohydrate diet group compared to the high carbohy-
drate diet group (Fig. 4C).
3.4. The change in visceral fat, and V/S ratio
In the low carbohydrate diet group, the amount of
visceral fat area was significantly decreased from 124
to 84 cm2 (P < 0.05) after 4 weeks of diet, and V/S
ratio decreased from 0.47 to 0.69 (P < 0.05) during
the same period (Fig. 5A and B). In contrast, neither
the amount of visceral fat area or V/S ratio changed
significantly during diet in the high carbohydrate diet
group (Fig. 5A and B).
4. Discussion
In this study, we have shown for the first time a dif-
ference in effects of two low calorie diets with low
or high carbohydrate content on visceral fat loss and
serum insulin levels in obese patients with type 2 di-
abetes.
During both diet therapies, the body weights weredecreased
without a decrease in LBM, and FBS lev-
els decreased as well as TC and TG levels. However,
although the decrease in FBS were similar between
the high and low carbohydrate diet groups, basal IRI
levels were significantly lower in the low carbohy-
drate diet group compared to the high carbohydrate
-
8/14/2019 Miyashita Paper
5/7
Y. Miyashita et al. / Diabetes Research and Clinical Practice 65
(2004) 235241 239
Fig. 4. Changes in serum lipids during low calorie diets in low
carbohydrate diet group (
) and high carbohydrate diet group (
). (AC)Show changes of total cholesterol, triglyceride and HDLC.
Data are shown as mean S.D, P < 0.05 and P < 0.01.
diet group at the end of the study. The lower lev-
els of insulin with similar levels of blood glucose
indicate a larger improvement of insulin sensitivity
in the low carbohydrate diet group. The homeostasis
model assessment-ratio [11] of the low carbohydrate
diet group and the high carbohydrate diet group were
changed from 3.06 to 0.77, and from 2.96 to 1.21, re-
spectively (data not shown).
HDLC levels were also significantly increased af-
ter 4 weeks diet in the low carbohydrate diet group
compared with the high carbohydrate diet group but
there were no differences in the reduction of TC or
TO between the two groups. It is known that one of
mechanisms by which the HDLC is increased is by
enhanced catabolism of very low-density lipoproteins
[12]. Accordingly, it is possible that a diet low in
-
8/14/2019 Miyashita Paper
6/7
240 Y. Miyashita et al. / Diabetes Research and Clinical
Practice 65 (2004) 235241
Fig. 5. Changes in adipose tissue distribution measured by
computed tomography after low calorie diets for a month in low
carbohydratediet group () and high carbohydrate diet group (). (A
and B) Show changes of visceral fat and V/S ratio. Data are shown
as meanS.D.,P < 0.05.
carbohydrates could stimulate the catabolism of very
low-density lipoproteins. Another possibility is that
the activity of lipoprotein lipase might be improved,
accompanying with the increased insulin sensitivity
[13,14].
There were also differences in the effect on adi-
pose tissue distribution between the two groups. In
low carbohydrate diet group, the visceral fat area and
the V/S ratio were significantly decreased during diet,
but not in high carbohydrate diet group. As for themechanisms,
there are at least two possible explana-
tions. The first is that the low carbohydrate diet could
stimulate growth hormone secretion from the pituitary
gland [15]. This could explain the different effects of
the two diets on visceral fat mass since it has previ-
ously been shown that the lipolytic activity induced by
growth hormone is higher in visceral fat compared to
subcutaneous fat [16,17]. Consequently, in this study,
the secretion of growth hormone might be enhanced
to a larger extent by the low carbohydrate diet com-
pared to the high carbohydrate diet. Another possibil-
ity is a lower insulin requirement of the low carbohy-drate
diet. Hyperinsulinemia is reported to be associ-
ated with visceral fat [1,2] and a high level of fasting
insulin is reported to predict visceral fat accumulation
[18]. In our study, there was a larger decrease of basal
IRI by the low carbohydrate diet compared to the high
carbohydrate diet. Accordingly, low insulin secretion
in low carbohydrate diet might be beneficial for re-
duction of visceral fat accumulation.
Bjorntorp and co-workers reported that an increased
flux of free fatty acids could cause insulin resistance
[19,20]. Consequently, the levels of free fatty acids
may be important factor during diet therapy. Free fatty
acids would be expected to increase during a low calo-
rie diet due to an increased fat mobilization. In our
study, the homeostasis model assessment-ratio in the
low carbohydrate diet is better compared to that in
the high carbohydrate diet. Hence, increased free fatty
acid levels during weight reduction by low calorie/low
carbohydrate diet did not deteriorate the insulin sensi-
tivity in these subjects. Furthermore, Reaven reportedthat high
carbohydrate intake would tend to increase
the risk of vascular complications [21,22], and high
carbohydrate diet is reported to increase blood glu-
cose, insulin, and TG levels and decrease HDLC in
diabetes mellitus patients [9]. In agreement with this,
our data suggest that a high carbohydrate intake would
not always be beneficial. In our study, the amount of
total intake of fat in the low carbohydrate diet was
about 40 g per day, which is not considered to be an
excessive fat intake, and is equal to that of 1600 kcal in
a high carbohydrate diet that is widely recommended.
Consequently, our data suggest that the more favor-able effect
on metabolism induced by the low carbo-
hydrate diet compared to the high carbohydrate diet
would be not due to be over-intake of fat, but rather
restriction of carbohydrate.
It is known that monounsaturated fatty acids is
preferable to saturated fatty acids for the diet therapy
of type 2 diabetes mellitus patients [23,24]. Reaven
also reported that substituting monounsaturated fats
for carbohydrates might be advantageous in reducing
the long-term complications, particularly coronary
-
8/14/2019 Miyashita Paper
7/7
Y. Miyashita et al. / Diabetes Research and Clinical Practice 65
(2004) 235241 241
heart disease, in type 2 diabetes mellitus patients [9].In our
study, intake of monounsaturated fats was not
always high, but low carbohydrate diet was more
beneficial than high carbohydrate diet for glucose and
lipid metabolism in type 2 diabetes mellitus. Further
studies regarding fat composition are required.
In summary, it is concluded that for type 2 diabetes
mellitus patients with obesity, low carbohydrate con-
tent in the low calorie diet showed more favorable ef-
fects on reducing visceral fat, lower serum insulin lev-
els and improving serum lipid levels compared to an
iso-caloric high carbohydrate diet.
Acknowledgements
This study is supported partly by a fund from the
Meeting of Obesity and Nutritional Disturbance.
References
[1] S. Yamashita, T. Nakamura, I. Shimomura, M. Nishida, S.
Yoshida, K. Kotani, K. Kameda, K. Tokunaga, Y. Maatsuzawa,
Insulin resistance and body fat distribution, Diab. Care 19
(1996) 287291.
[2] D.J. Evans, R.G. Hoffman, R.K. Kalkhoff, A.H. Kissebah,
Relationship of body fat topography to insulin sensitivity
and
metabolic profiles in premenopausal women, Metabolism 33
(1984) 6875.
[3] P. Ducimetire, J. Richard, F. Cambien, The pattern of
subcutaneous fat distribution in middle-aged men and the
risk
of coronary heart disease: the Paris Prospective Study, Int.
J.
Obes. 10 (1986) 229240.
[4] R.P. Donahue, R.D. Abbott, E. Bloom, D.M. Reed, K. Yano,
Central obesity and coronary heart disease in men, Lancet 4
(1987) 821824.
[5] U. Rabast, J. Schonbrn, H. Kasper, Diabetic treatment of
obesity with low and high-carbohydrate diets: comparative
studies and clinical results, Int. J. Obes. 3 (1979) 201211.
[6] M.U. Yang, V. Itallie, Composition of weight loss
duringshort-term weight reduction, J. Clin. Invest. 58 (1976)
722
730.
[7] S.B. Werner, Comparison between weight reduction on a
high
calorie high fat diet and on an isocaloric regimen high in
carbohydrate, N. Eng. J. Med. 66 (1955) 252.
[8] I. Zavaroni, Y.D. Chen, G.M. Reaven, Studies of the
mechanism of fructose-induced hypertriglyceridemia in the
rat, Metabolism 31 (1982) 10771083.
[9] A. Garg, J.P. Bantle, R.R. Henry, A.M. Coulston, K.A.
Griver,
B.A. Huet, G.M. Reaven, Effects of varying carbohydrate
content of diet in patients with non-insulin-dependent
diabetes
mellitus, JAMA 271 (1994) 14211428.
[10] Y. Miyashita, Y. Itoh, S. Hashiguchi, M. Totsuka, T.
Murano,K. Ariga, T. Uetake, C. Nagai, H. Tomioka, K. Shirai,
Effects
of low carbohydrate content of low calory diet for obese
non-insulin-dependent diabetes mellitus patients on glucose
and lipid metabolism, J. Jpn. Diab. Soc. 41 (1998) 885890.
[11] R.C. Turner, R.R. Holman, D. Matthews, T.D. Hockaday,
J.
Peto, Insulin deficiency and insulin resistance interaction
in
diabetes: estimation of their relative contribution by
feedback
analysis from basal plasma insulin and glucose
concentrations,
Metabolism 11 (1979) 10861096.
[12] B. Staels, J. Dallongeville, J. Auwerx, K. Schoonjans,
E.
Leitersdorf, J.C. Fruchart, Mechanism of action of fibrates
on lipid and lipoprotein metabolism, Circulation 19 (1998)
20882093.
[13] J.R. Mead, S.A. Irvine, D.P. Ramji, Lipoprotein lipase:
structure, function, regulation, and role in disease, J.
Mol.Med. 80 (2002) 753769.
[14] L.K. Pulawa, R.H. Eckel, Over expression of muscle
lipoprotein lipase and insulin sensitivity, Curr. Opin.
Clin.
Nutr. Metab. Care 5 (2002) 569574.
[15] J.L. Langfort, R. Zarzeczny, K. Nazar, H.
Kaciuba-Uscilko,
The effect of low-carbohydrate diet on the pattern of
hormonal
changes during incremental, graded exercise in young men,
Int. J. Sport Nutr. Exerc. Metab. 11 (2001) 248257.
[16] Y. Itoh, K. Shiai, Preferential lipolysis in rat visceral
adipose
tissues by growth hormone, Endocrinol. Metab. 4 (1997) 61
67.
[17] P. Lucidi, N. Parlanti, F. Piccioni, F. Snateusanio, P.
De
Feo, Short-term treatment with low doses of recombinant
human GH stimulates lipolysis in visceral obese men, J.
Clin.
Endocrinol. Metab. 87 (2002) 31053109.[18] E.J. Boyko, D.L.
Leonetti, R.W. Bergstrom, L. Newell-Morris,
W.Y. Fujimoto, Low insulin secretion and high fasting
insulin and C-peptide levels predict increased visceral
adiposity. %-year follow-up among initially nondiabetic
Japanese-American men, Diabetes 45 (1996) 10101015.
[19] M. Rebuffe-Scrive, B. Anderson, L. Olbe, P. Bjorntorp,
Metabolism of adipose tissue in intraabdominal deposits in
severely obese men and women, Metabolism 39 (1990) 570
574.
[20] J. Svedberg, P. Bjomtorp, U. Smith, P. Lonnroth,
Free-fatty
acid inhibition of insulin binding, degradation, and action
in
isolated rat hepatocytes, Diabetes 39 (1990) 570574.
[21] G.M. Reaven, The role of insulin resistance and
hyperinsulinemia in coronary heart disease, Metabolism 41
(1992) 1619.[22] R.W. Stout, Insulin and atheroma: 20-year
perspective, Diab.
Care 13 (1990) 631654.
[23] A. Gang, A. Bonanome, S.M. Grundy, Z.J. Zhang, R.H.
Unger, Comparison of a high-carbohydrate diet with a
high-monounsaturated-fat diet in patients with non-insulin-
dependent diabetes mellitus, N. Engl. J. Med. 319 (1988)
829834.
[24] M. Parillo, A.A. Rivellese, A.V. Ciardullo, A
high-monoun-
saturated-fat/low-carbohydrate diet improves peripheral
insulin sensitivity in non-insulin-dependent diabetic
patients,
Metabolism 41 (1992) 13731378.