Embed Size (px)
Citation preview
The Journal of NutritionNutrient Physiology, Metabolism, and Nutrient-Nutrient Interactions
Multinutrient Supplementation IncreasesCollagen Synthesis during Early Wound Repairin a Randomized Controlled Trial in Patientswith Inguinal HerniaMarie Kjaer,1 Amalie Kruse Sigersted Frederiksen,1 Neel Ingemann Nissen,2 Nicholas Willumsen,2
Gerrit van Hall,3 Lars Nannestad Jorgensen,1 Jens Rikardt Andersen,4 and Magnus S Agren1,5,6
1Digestive Disease Center, Bispebjerg Hospital, University of Copenhagen, Copenhagen, Denmark; 2Nordic Bioscience A/S, Herlev,Denmark; 3Clinical Metabolomics Core Facility, Department of Clinical Biochemistry, Rigshospitalet, and Department of BiomedicalSciences, University of Copenhagen, Copenhagen, Denmark; 4Department of Nutrition, Exercise, and Sports, University of Copenhagen,Copenhagen, Denmark; 5Copenhagen Wound Healing Center, Bispebjerg Hospital, University of Copenhagen, Copenhagen, Denmark; and6Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark.
ABSTRACTBackground: Inguinal hernia disease is associated with an imbalanced collagen metabolism. Surgical stress has a
negative impact on nutrients important for collagen synthesis.
Objective: We hypothesized that supplementation with a combination of nutrients would enhance collagen
biosynthesis in inguinal hernia disease patients when undergoing hernia repair.
Methods: In this exploratory randomized controlled trial, 21 men (age: 55.2 ± 2.8 y; BMI: 25.0 ± 0.7 kg/m2) scheduled
for Lichtenstein inguinal hernia repair were assigned to multinutrient supplementation (n = 10; multinutrient group) or no
multinutrient supplementation (n = 11; control group). The multinutrient group received 14 g L-arginine, 14 g L-glutamine,
1250 mg vitamin C, and 55 mg zinc daily starting 14 d before surgery and ending 14 d after surgery. The multinutrient
and control groups received high-quality protein to ensure a daily intake of 1.5 g protein/kg. Collagen biosynthesis was
measured by the biomarkers type I procollagen propeptide (CICP), type III procollagen propeptide (PRO-C3), and type V
procollagen propeptide (PRO-C5) in the sera on days −14, 0, and 1, and in the wound fluids on postoperative days 1 and
2. Compliance was recorded after the 28-d intervention period.
Results: Serum PRO-C5 concentrations decreased (P < 0.05) postoperatively in the control but not the multinutrient
group. Neither CICP nor PRO-C3 serum concentrations differed significantly between the 2 groups. In wound fluid, the
CICP concentrations increased (P < 0.05) from days 1 to 2 in the multinutrient group and were 49% higher (P = 0.10)
than those in the control group on day 2. Wound fluid concentrations PRO-C3 and PRO-C5 showed no significant time
or group differences. The 28-d compliance was similar (P = 0.27) in the 2 groups.
Conclusion: Oral supplementation with arginine, glutamine, vitamin C, and zinc augment collagen synthesis during
the first 2 d after inguinal hernia repair. This trial was registered at clinicaltrials.gov as NCT03221686. J Nutr 2020;0:1–8.
Keywords: Collagen synthesis, wound healing, surgery, biomarkers, zinc, ascorbic acid, amino acids
Introduction
More than 20 million patients undergo inguinal hernia repairsworldwide each year (1). In men, the estimated lifetime riskof developing an inguinal hernia is 27% (2). The diseaseis multifactorial and associated with an altered collagenmetabolism, as exemplified by the lower turnover of typeV collagen in inguinal hernia patients than in hernia-freepatients (3). Moreover, altered collagen metabolism duringthe repair processes may be responsible for hernia recurrence(4). To the best of our knowledge, no previous studies haveattempted to therapeutically correct for this imbalance incollagen metabolism in hernia patients receiving surgical repair.
Collagens are central extracellular matrix (ECM) compo-nents for wound healing. Type I and III collagens are the majorconstituents of most ECMs. Type V collagen is essential forthe formation of type I collagen fibrils (5). Although type Vcollagen determines the resulting tissue quality (6), the roleof it in acute surgical wounds needs further exploration inhumans.
Collagen formation requires amino acid building blocks,vitamins, and trace minerals. The amino acids arginine andglutamine seem particularly important since they indirectlyprovide one of the major collagen constituents, proline (7).Glutamine may also improve cell uptake of vitamin C (8),
Copyright C© The Author(s) 2020.Manuscript received May 18, 2019. Initial review completed September 16, 2019. Revision accepted December 5, 2019.First published online 0, 2020; doi: https://doi.org/10.1093/jn/nxz324. 1
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020

which is a cofactor of prolyl hydroxylases that are necessaryfor the hydroxylation of proline during collagen biosynthesis(9). Zinc is a cofactor of the metalloenzymes that are requiredfor the extracellular processing of interstitial procollagensthat enable fibril formation (10). These factors all showreduced blood concentrations after surgical trauma (11–17),possibly reflecting the increased local demand during the tissuerebuilding process (12). Therefore, it has been hypothesized thatpreventing or mitigating this reduction would be beneficial forcollagen production and wound healing. This concept has beenpreviously explored, but only by administering 1 nutritionalfactor (14, 16, 17). To our knowledge, no previous studies havereported the combined effects of arginine, glutamine, vitamin C,and zinc supplementation on early collagen synthesis in surgicalpatients.
With this background in mind, we aimed to study the effectof a perioperative oral supplement composed of the above-mentioned nutrients on wound healing in patients undergoinginguinal hernia repair. Systemic and local type I, type III, andtype V collagen synthesis was determined by measuring theconcentrations of the propeptides of type I procollagen (CICP),type III procollagen (PRO-C3), and type V procollagen (PRO-C5), with serum CICP concentration as the primary outcome.We also studied the effect of the multinutrient supplement onre-epithelialization by making standardized epidermal woundsin the patients.
Materials and Methods
This open and prospective randomized controlled trial wasperformed at the Digestive Disease Center, Bispebjerg Hos-pital, University of Copenhagen, Copenhagen, Denmark.The trial was approved by the Committees of HealthResearch Ethics in the Capital Region of Denmark (H-15017272) and the Danish Data Protection Agency (2012-58-0004). The trial was registered at clinicaltrials.gov asNCT03221686.
Study participants
Patients 18 y or older who were referred for elective, primaryopen inguinal hernia repair performed with the Lichtensteintechnique were screened and included after providing their oraland written consent. Patients were excluded if they needed aninterpreter, had undergone previous surgery in the same groinwithin the last 5 y, or received systemic corticosteroid treatment.In addition, patients with known dementia, dysregulateddiabetes [glycated hemoglobin (HbA1c) >9%], hepatic disease,renal disease, or a cancer diagnosis within the last 5 y wereexcluded.
Funded by the Bispebjerg Hospital, Department of Nutrition, Exercise andSports, University of Copenhagen, and Medtrition Inc., Lancaster, PA.Author disclosures: The authors report no conflicts of interest.Supplemental Tables 1 and 2 are available from the “Supplementary data” linkin the online posting of the article and from the same link in the online table ofcontents at https://academic.oup.com/jn.Address correspondence to MSA (e-mail: [email protected]).Abbreviations used: CICP, C-terminal type I procollagen propeptide; CRP, C-reactive protein; ECM, extracellular matrix; HbA1c, glycated hemoglobin; LSD,least significant difference; PRO-C3, type III procollagen propeptide; PRO-C5,type V procollagen propeptide.
TABLE 1 Daily intake from the protein and multinutrientsupplements in the 2 groups and daily recommended intake formen (18)1
Multinutrientgroup (n = 10)
Control group(n = 11)
Daily recommendedintake
Protein, g/kg 1.5 1.5 0.8–1.5Arginine, g 15 22 NAGlutamine, g 18 32 NAVitamin C, mg 1250 22 75Zinc, mg 55 0 9
1NA, data not available.2Provided by the protein supplement (white, DAVA Foods).
Trial flow, interventions, and procedures
At baseline, on day −14, a blood sample was collected fromeach patient. The patients’ daily protein intake, estimated bya retrospective FFQ, was used to calculate the amount ofhigh-quality protein (white, DAVA Foods) needed to reach1.5 g protein/kg body weight and day (18). The patients werethen allocated to the multinutrient or control group usingsealed opaque envelopes mixed in a basket that containedequal numbers of envelopes for the 2 groups. The multinutrientgroup received a specialized wound healing formula twice aday (11220; ArgiMent AT, Medtrition), which provided 14 gl-arginine, 14 g l-glutamine, 500 mg vitamin C, 30 mg zinc,and 320 kcal per day. The patients also received 1 tabletthat contained 750 mg vitamin C as calcium ascorbate (Bio-C-Vitamin, Pharma Nord) and 2 tablets that each contained15 mg zinc as zinc gluconate (Bio-Zink, Pharma Nord) perday. Comparisons of these doses with the daily recommendedintakes are shown in Table 1 (18). The control groupreceived the protein supplement only. The patients wereprovided with 28 1-day portions of the supplements and wereinstructed to avoid dietary supplements that contained arginine,glutamine, vitamin C, or zinc during the 28-d supplementationperiod.
After 14 d of supplementation, on the day of herniasurgery (day 0), the second blood sample was obtained.The patients then underwent elective open surgery undergeneral anesthesia for inguinal hernia with monofilamentpolypropylene mesh (Parietene, Covidien) by surgeons blindedto the group allocation. A closed suction drain (Ch. 8) wasplaced into the subcutaneous wound cavity and connected toa 50-mL bellow (Mini Redon, Primed Medizintechnik) beforeskin closure. Within 4 hours after the hernia surgery, epidermalwounds were made using the suction–blister technique (19). Theskin of the nondominant medial forearm was cleansed with70% ethanol and two 10-mm suction blisters 10 mm apartwere induced using heated (40◦C) chambers maintained undera constant vacuum of 300 mm Hg. The accumulated blisterfluid was aspirated and stored at −80◦C. The blister roofswere excised, and the epidermal wounds were covered with anocclusive dressing (Mepore Pro, Mölnlycke Health Care). Thedressing was replaced daily.
On postoperative day 1, the third blood sample and woundfluid from the drain were procured. The patients were thendischarged from the hospital.
On postoperative day 2, the nonfasting patients returnedto the outpatient clinic for collection of the wound fluidthat had accumulated in the bellow from postoperativeday 1.
2 Kjaer et al.
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020

TABLE 2 Biochemical analyses performed on sera, woundfluids, and blister fluids1
AnalyteDay −14
(baseline) Day 0 Day 1 Day 2
SerumCICP
√ √ √2
PRO-C3√ √ √2
PRO-C5√ √ √2
CRP√ √ √2
Free amino acids√ √ √2
Zinc√ √ √2
Wound fluidCICP
√2 √2
PRO-C3√2 √2
PRO-C5√2 √2
Blister fluidCICP
√2
1CICP, C-terminal type I procollagen propeptide; CRP, C-reactive protein; PRO-C3,type III procollagen propeptide; PRO-C5, type V procollagen propeptide.2After surgery.
A summary of the biochemical analyses performed on thesera, wound fluids, and blister fluids is shown in Table 2.
Handling of blood samples and wound and blisterfluids
Venous blood was collected without stasis between 07:00 and12:00 after an overnight fast into 1 BD Vacutainer serum plastictube with clot activator (BD Diagnostics) and 1 zinc-free plasticBD Vacutainer trace element serum tube (BD Diagnostics). Thetubes were left standing for 20 min and then centrifuged at 3000or 1800 × g for 10 min at ambient temperature, respectively.The serum fractions were stored at −80◦C until analysis forCICP, PRO-C3, PRO-C5, C-reactive protein (CRP), free aminoacids, and zinc. The wound and blister fluid samples werecentrifuged at 3000 × g for 10 min at ambient temperature andstored at −80◦C until analysis.
Measurements of collagen synthesis biomarkers
CICP concentrations were quantified by use of an ELISA kit(Quidel Corporation), and PRO-C3 and PRO-C5 concentra-tions were assessed by solid-phase and competitive ELISAs(Nordic Bioscience) (3, 20).
CRP, free amino acid, and zinc measurements in serum
CRP was measured with an ELISA kit (DCRP00; R&D Systems)(21).
Our method of serum procurement for the free aminoacid analyses was validated in 6 healthy fasting men with amean ± SEM age of 58.5 ± 2.0 y. Blood samples (10 mL)were collected between 08:00 and 09:30 consecutively in1 plastic tube with clot activator at an ambient temperature andthen in a second chilled (0◦C) plastic tube with clot activator.One set of 6 tubes was treated according to our method, i.e.,the tubes were left standing for 20 min and then centrifugedat 3000 × g for 10 min at ambient temperature. The serumfractions (1.5 mL) were transferred to Eppendorf polypropylenecentrifuge tubes, and then 80 μL of ELGA ultrapure water wasadded and the samples were stored in polypropylene cryovialsat −80◦C. The other set of 6 tubes was immediately placedon ice for 20 min and then centrifuged at 3000 × g for10 min at 4◦C. The serum fractions (1.5 mL) were transferred to
Eppendorf polypropylene centrifuge tubes, and then 80 μL of60% (wt:vol) 5-sulfosalicylic acid dissolved in ELGA ultrapurewater was added. The sample was vortexed, kept on ice for 15min, and centrifuged at 10,000 × g for 10 min at 4◦C (22).The supernatants were aspirated and stored in polypropylenecryovials at −80◦C. The concentration of free amino acidswas measured by ultraperformance LC-MS/MS (23). For allanalyses, the thawed samples were immediately deproteinizedin the derivatization step.
The zinc concentrations of the sera (diluted 10 times with0.14 mol/L nitric acid) were determined by double-focusinginductively coupled plasma MS (24).
Clinical outcomes
The epidermal wounds were photographed daily with a15-megapixel camera (Canon EOS 500D) until healed. The timeto complete healing (the average time of the 2 wounds was usedfor the statistical analysis) was assessed from the photographsby a blinded investigator (MSA).
Any postoperative complications occurring within postop-erative day 30 and diagnosis and/or reoperation for herniarecurrence within 1 y postoperatively were recorded.
Compliance assessment and side effects of thesupplements
At the end of the 28-day supplementation period, the patientsreported side effects associated with the supplementationsand were instructed to return any leftover supplements andcompliance was calculated as follows: [1 − (x/28)] × 100, wherex is the number of 1-d supplement portions returned.
Statistical analyses
Two-way ANOVA was applied to serum CRP, CICP, PRO-C3,PRO-C5, amino acid, zinc, and wound fluid CICP, PRO-C3, andPRO-C5 concentrations followed by the Fisher’s least significantdifference (LSD) post hoc test when appropriate (25). Due tothe exploratory design of our trial, no corrections for family-wise error were carried out. CICP blister fluid concentrationswere compared using the unpaired t-test. The effects of infectionon serum CRP concentrations and patient healing time andcompliance were analyzed using the Mann–Whitney U test. The2-sided statistical analyses were performed using SPSS Statistics24.0 software (IBM). The level of statistical significance was P< 0.05. Variables are presented as the mean ± SEM or medianinterquartile range (IQR).
Results
Of the 254 patients screened from January 20, 2016, toJanuary 10, 2017, 21 patients were randomly assigned to themultinutrient group (n = 10) or the control group (n = 11)(Figure 1). One patient in the multinutrient group withdrewfrom the study before surgery on day 0, which resulted in9 patients in the multinutrient group and 11 patients in thecontrol group for the per-protocol analysis. The 2 groups werecomparable demographically and with respect to the durationof surgery and length of skin incisions (Table 3).
Collagen synthesis biomarkers
The CICP serum concentrations did not change over thepreoperative period from day −14 to day 0 or postoperativelyfrom day 0 to day 1 in the multinutrient or control groups(Figure 2A). The PRO-C3 serum concentrations did not change
Collagen synthesis during surgical wound healing 3
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020
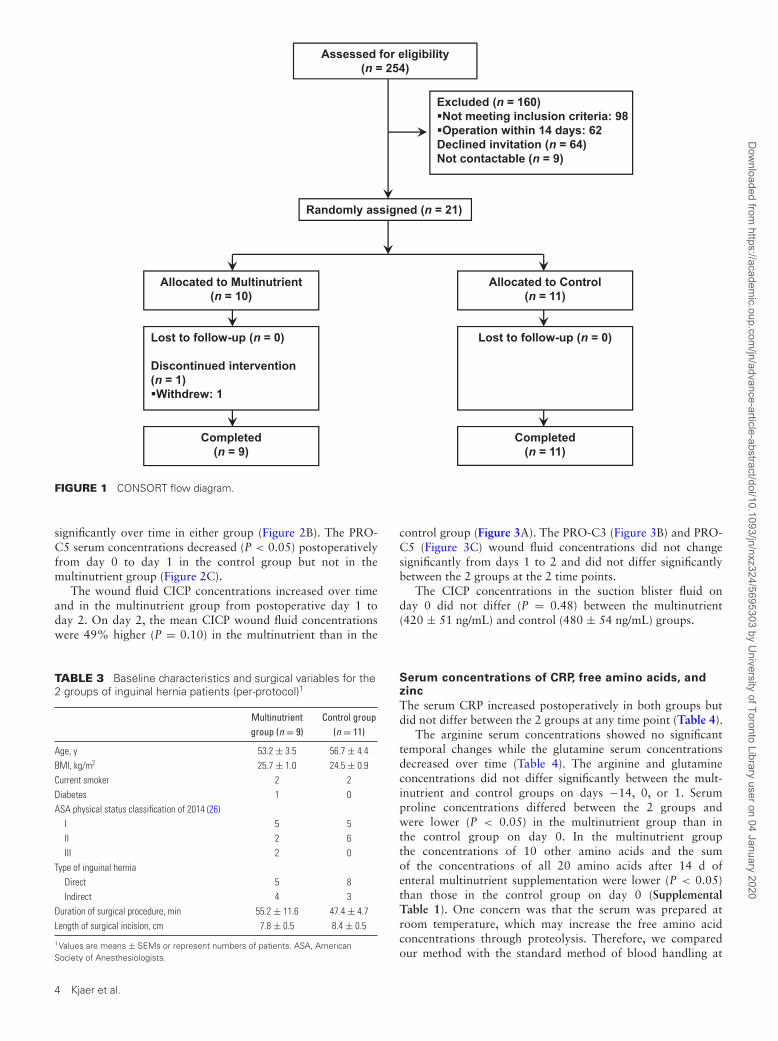
Assessed for eligibility(n = 254)
Randomly assigned (n = 21)
Completed(n = 9)
Allocated to Control(n = 11)
Completed(n = 11)
Lost to follow-up (n = 0)
Discontinued intervention(n = 1)�Withdrew: 1
Lost to follow-up (n = 0)
Allocated to Multinutrient(n = 10)
Excluded (n = 160)�Not meeting inclusion criteria: 98�Operation within 14 days: 62Declined invitation (n = 64)Not contactable (n = 9)
FIGURE 1 CONSORT flow diagram.
significantly over time in either group (Figure 2B). The PRO-C5 serum concentrations decreased (P < 0.05) postoperativelyfrom day 0 to day 1 in the control group but not in themultinutrient group (Figure 2C).
The wound fluid CICP concentrations increased over timeand in the multinutrient group from postoperative day 1 today 2. On day 2, the mean CICP wound fluid concentrationswere 49% higher (P = 0.10) in the multinutrient than in the
TABLE 3 Baseline characteristics and surgical variables for the2 groups of inguinal hernia patients (per-protocol)1
Multinutrientgroup (n = 9)
Control group(n = 11)
Age, y 53.2 ± 3.5 56.7 ± 4.4BMI, kg/m2 25.7 ± 1.0 24.5 ± 0.9Current smoker 2 2Diabetes 1 0ASA physical status classification of 2014 (26)
I 5 5II 2 6III 2 0
Type of inguinal herniaDirect 5 8Indirect 4 3
Duration of surgical procedure, min 55.2 ± 11.6 47.4 ± 4.7Length of surgical incision, cm 7.8 ± 0.5 8.4 ± 0.5
1Values are means ± SEMs or represent numbers of patients. ASA, AmericanSociety of Anesthesiologists.
control group (Figure 3A). The PRO-C3 (Figure 3B) and PRO-C5 (Figure 3C) wound fluid concentrations did not changesignificantly from days 1 to 2 and did not differ significantlybetween the 2 groups at the 2 time points.
The CICP concentrations in the suction blister fluid onday 0 did not differ (P = 0.48) between the multinutrient(420 ± 51 ng/mL) and control (480 ± 54 ng/mL) groups.
Serum concentrations of CRP, free amino acids, andzinc
The serum CRP increased postoperatively in both groups butdid not differ between the 2 groups at any time point (Table 4).
The arginine serum concentrations showed no significanttemporal changes while the glutamine serum concentrationsdecreased over time (Table 4). The arginine and glutamineconcentrations did not differ significantly between the mult-inutrient and control groups on days −14, 0, or 1. Serumproline concentrations differed between the 2 groups andwere lower (P < 0.05) in the multinutrient group than inthe control group on day 0. In the multinutrient groupthe concentrations of 10 other amino acids and the sumof the concentrations of all 20 amino acids after 14 d ofenteral multinutrient supplementation were lower (P < 0.05)than those in the control group on day 0 (SupplementalTable 1). One concern was that the serum was prepared atroom temperature, which may increase the free amino acidconcentrations through proteolysis. Therefore, we comparedour method with the standard method of blood handling at
4 Kjaer et al.
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020
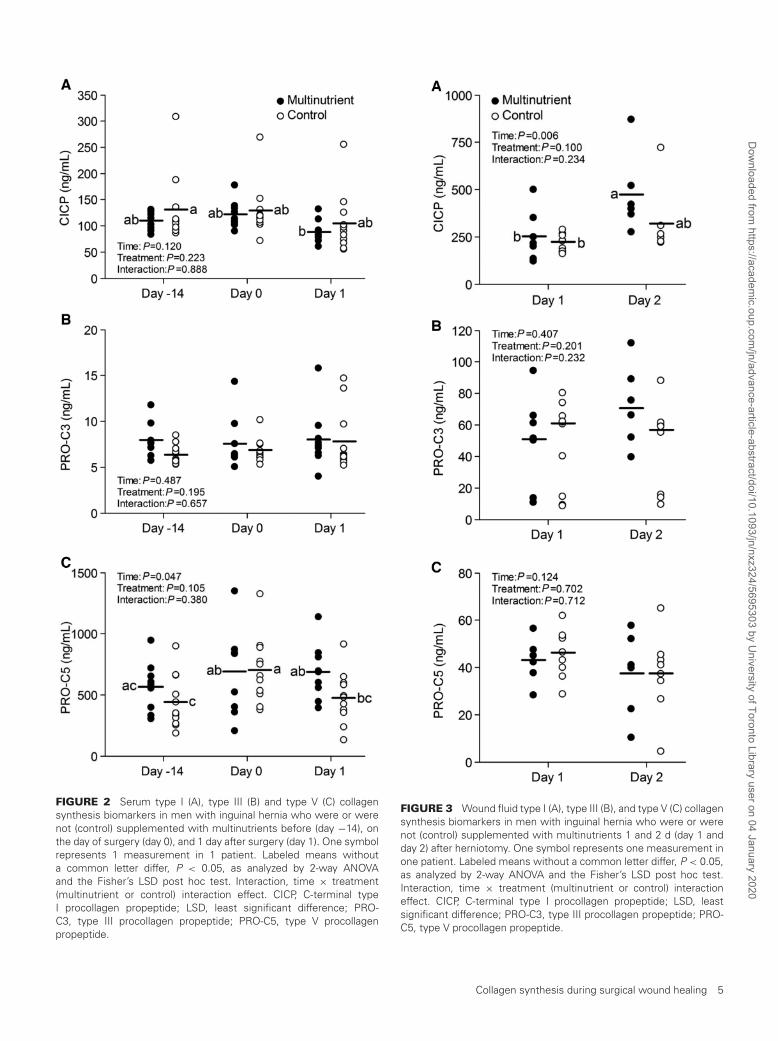
FIGURE 2 Serum type I (A), type III (B) and type V (C) collagensynthesis biomarkers in men with inguinal hernia who were or werenot (control) supplemented with multinutrients before (day −14), onthe day of surgery (day 0), and 1 day after surgery (day 1). One symbolrepresents 1 measurement in 1 patient. Labeled means withouta common letter differ, P < 0.05, as analyzed by 2-way ANOVAand the Fisher’s LSD post hoc test. Interaction, time × treatment(multinutrient or control) interaction effect. CICP, C-terminal typeI procollagen propeptide; LSD, least significant difference; PRO-C3, type III procollagen propeptide; PRO-C5, type V procollagenpropeptide.
FIGURE 3 Wound fluid type I (A), type III (B), and type V (C) collagensynthesis biomarkers in men with inguinal hernia who were or werenot (control) supplemented with multinutrients 1 and 2 d (day 1 andday 2) after herniotomy. One symbol represents one measurement inone patient. Labeled means without a common letter differ, P < 0.05,as analyzed by 2-way ANOVA and the Fisher’s LSD post hoc test.Interaction, time × treatment (multinutrient or control) interactioneffect. CICP, C-terminal type I procollagen propeptide; LSD, leastsignificant difference; PRO-C3, type III procollagen propeptide; PRO-C5, type V procollagen propeptide.
Collagen synthesis during surgical wound healing 5
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020
0–4◦C and deproteinization with sulfosalicylic acid in 6 age-matched healthy men. The results indicated that with ourmethod preparation at room temperature the free amino acidconcentrations were marginally but statistically (P < 0.005)lower (by 4.1%) than with preparation with the standardmethod (Supplemental Table 2). This difference was unrelatedto stability but was attributed to the physical properties ofthe proteinaceous and deproteinized serum samples, except foraspartate and tryptophan.
One control patient had a serum zinc concentration<9μmol/L on day −14. The amounts of serum zinc increasedby 14% from day −14 to day 0 in the multinutrient groupbut not in the control group. The serum zinc then decreasedpostoperatively in both groups. There were no significantdifferences between the serum zinc concentrations in the2 groups on individual days (Table 4).
Compliance, side effects, and clinical outcomes
The compliance with supplement intake was 95 ± 2.5%in the multinutrient group and 98 ± 1.0% in the controlgroup (P = 0.27). One patient in the multinutrient group and1 control patient reported unpleasant taste of the supplements.One patient had meteorism from the intake of Argiment AT.
The healing time of the epidermal wounds did not differ(P = 0.87) between the multinutrient (median: 7.8 d; IQR:7.0–8.3 d) and the control (median: 7.5 d; IQR: 7.0–8.8d) groups. Within the first 30 postoperative days, 1 patientin the multinutrient group and 2 control patients developeda surgical site infection that required antibiotic treatment.The CRP serum concentrations in these 3 patients were 78(70–94) mg/L compared with 26 (9.9–70) mg/L for the patientswithout infection (P = 0.08). Within 1 y, the patient in themultinutrient group with surgical site infection and 3 othercontrol patients reported hernia recurrence. These 4 patients allunderwent primary surgery for a direct inguinal hernia.
Discussion
Surgical stress negatively affects numerous factors required foroptimal collagen formation, as reflected by increased CRP. Inanother study on inguinal hernia patients undergoing Lichten-stein repair (27), CRP increased to 24 mg/L on postoperativeday 1, a value similar to our finding of a median CRP of 20 mg/L(n = 9). Furthermore, the serum PRO-C5 concentrationsdecreased postoperatively. Here, we perioperatively providedinguinal hernia patients with a mixture of essential nutrientsfor collagen synthesis with the aim of abolishing this effect ofsurgery. Multinutrient supplementation maintained the systemictype V collagen synthesis postoperatively. This finding is noveland important because decreased type V collagen turnover hasbeen reported in inguinal hernia patients (3, 20).
In the present study, the concentrations of CICP and PRO-C3 in wound fluid were higher than those in serum on day 1,which indicates the start of type I and type III collagen synthesisin the wound (28). The wound fluid concentrations of CICPbut not PRO-C3 increased further by day 2 compared withday 1 in the multinutrient group, indicating early stimulationof type I collagen synthesis in the wounds. Haukipuro etal. (28) also reported early increase in the concentrationsof CICP and PRO-C3 detected by using a similar collagenpropeptide immunoassay. In contrast, in our patients the PRO-C5 local concentrations remained below the serum PRO-C5concentrations and were not influenced by the multinutrient
supplement. Whether this finding reflects decreased type Vcollagen synthesis in the wound is unknown, as knowledge onthe kinetics of PRO-C5 in wound fluid is lacking. These resultsmay, for example, be due to excessive proteolysis of the releasedPRO-C5 peptides that is initiated by the inflammatory responsein the wound. On the other hand, the gene expression of type Vcollagen is delayed and transient in wounds in relation to bothtype I and type III collagen (29). One weakness of our study wasthat the collagen biomarkers were not examined beyond day 2.It has been found that wound fluid concentrations of both type Iand type III collagen propeptides show dramatic increases afterday 2 that last for at least the first 7 postoperative days (28).
We did not observe an effect on epidermal wound healing inthe multinutrient group, which indicates that the multinutrientsupplement acted primarily on the connective tissue cells. Inother reported studies, arginine supplementation did not affectepithelialization of partial-thickness skin wounds in healthyelderly volunteers (30) or in patients receiving reconstructiveplastic surgery (31).
On the other hand, arginine supplementation has beenreported to stimulate local collagen deposition (30). Arginine issynthesized from ornithine through citrulline and is a precursorfor proline during collagen synthesis (7, 32). It is possible thatthe reduced serum proline with multinutrient supplementationreflects increased utilization of proline in the synthesis ofcollagen molecules (7).
The serum concentration of the sum of all free aminoacids was significantly lower after 14 d in the multinutrientgroup compared with the control group. If we assume thatthe multinutrient supplement increases insulin secretion, thenthe net protein synthesis may be consuming other amino acids(33, 34). Glutamine serum concentrations declined over time,which was not surprising, given the abundance of glutaminein cells involved in wound healing (8, 12). This effect wasnot mitigated by multinutrient supplementation. Blass et al.(8) provided glutamine (20 g) to surgical patients for 14 d,which prevented the decline in serum glutamine concentrationsobserved in the patients receiving no supplement. No argininewas administered in that study, which could explain the paradoxbecause of the anabolic property of arginine during woundhealing (35). In our study the serum samples were preparedat room temperature and not at 4◦C, and they were notdeproteinized before being frozen at −80◦C. However, thisapproach did not seem to appreciably impact the free aminoacid concentrations, as indicated in a previous study (36).
Malnutrition is associated with increased infection ratesand decreased wound tensile strength (37). Therefore, themultinutrient supplementation and control groups receivedhigh-quality protein to maximize their baseline wound healingcapacity. The high intake of protein in both groups mightexplain the limited difference observed in the biomarkers ofcollagen synthesis in the multinutrient group compared withthe control group. In a similarly designed study, surgicalpatients with a daily protein intake of 0.6–0.7 g/kg receivedsupplementation with glutamine, vitamin C, and zinc butnot with protein and showed pronounced accelerated woundhealing (8). To determine whether the protein supplementationwas effective, a third arm including a control group that doesnot receive extra protein would be required. Nevertheless, thisapproach allowed us to specifically study the additional effectsof arginine, glutamine, vitamin C, and zinc.
We can only speculate on which of the constituents of themultinutrient supplement was responsible for the beneficialeffects on collagen synthesis. Vitamin C deficiency leads
6 Kjaer et al.
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020
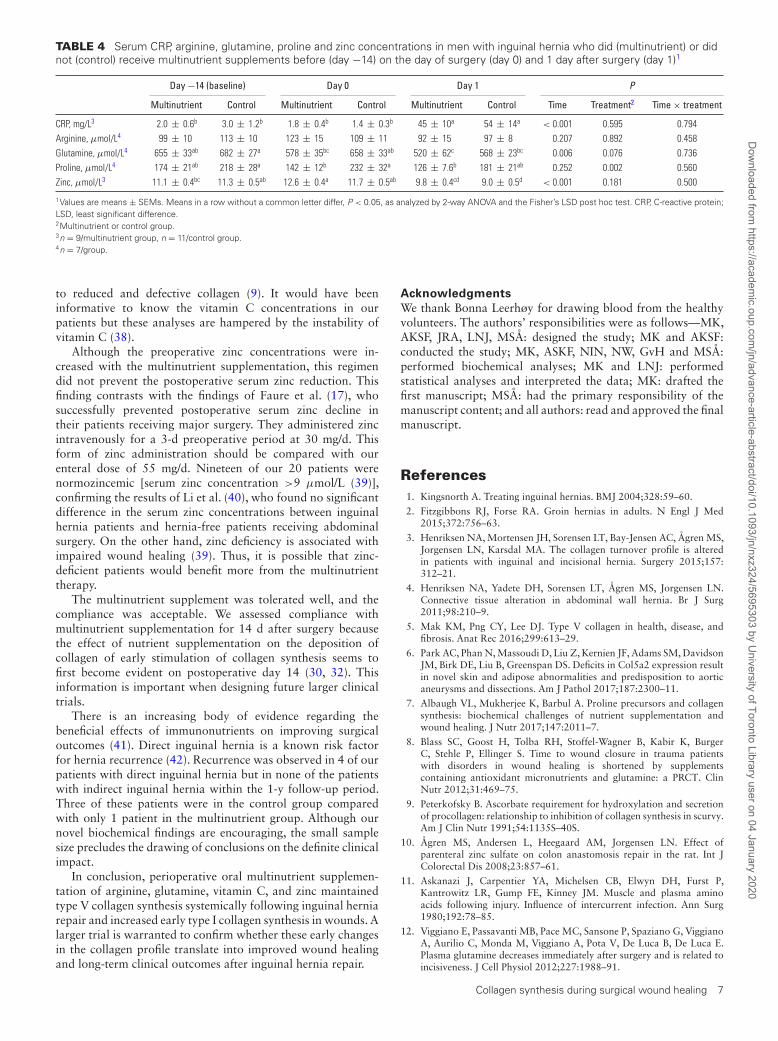
TABLE 4 Serum CRP, arginine, glutamine, proline and zinc concentrations in men with inguinal hernia who did (multinutrient) or didnot (control) receive multinutrient supplements before (day −14) on the day of surgery (day 0) and 1 day after surgery (day 1)1
Day −14 (baseline) Day 0 Day 1 P
Multinutrient Control Multinutrient Control Multinutrient Control Time Treatment2 Time × treatment
CRP, mg/L3 2.0 ± 0.6b 3.0 ± 1.2b 1.8 ± 0.4b 1.4 ± 0.3b 45 ± 10a 54 ± 14a < 0.001 0.595 0.794Arginine, μmol/L4 99 ± 10 113 ± 10 123 ± 15 109 ± 11 92 ± 15 97 ± 8 0.207 0.892 0.458Glutamine, μmol/L4 655 ± 33ab 682 ± 27a 578 ± 35bc 658 ± 33ab 520 ± 62c 568 ± 23bc 0.006 0.076 0.736Proline, μmol/L4 174 ± 21ab 218 ± 28a 142 ± 12b 232 ± 32a 126 ± 7.6b 181 ± 21ab 0.252 0.002 0.560Zinc, μmol/L3 11.1 ± 0.4bc 11.3 ± 0.5ab 12.6 ± 0.4a 11.7 ± 0.5ab 9.8 ± 0.4cd 9.0 ± 0.5d < 0.001 0.181 0.500
1Values are means ± SEMs. Means in a row without a common letter differ, P < 0.05, as analyzed by 2-way ANOVA and the Fisher’s LSD post hoc test. CRP, C-reactive protein;LSD, least significant difference.2Multinutrient or control group.3n = 9/multinutrient group, n = 11/control group.4n = 7/group.
to reduced and defective collagen (9). It would have beeninformative to know the vitamin C concentrations in ourpatients but these analyses are hampered by the instability ofvitamin C (38).
Although the preoperative zinc concentrations were in-creased with the multinutrient supplementation, this regimendid not prevent the postoperative serum zinc reduction. Thisfinding contrasts with the findings of Faure et al. (17), whosuccessfully prevented postoperative serum zinc decline intheir patients receiving major surgery. They administered zincintravenously for a 3-d preoperative period at 30 mg/d. Thisform of zinc administration should be compared with ourenteral dose of 55 mg/d. Nineteen of our 20 patients werenormozincemic [serum zinc concentration >9 μmol/L (39)],confirming the results of Li et al. (40), who found no significantdifference in the serum zinc concentrations between inguinalhernia patients and hernia-free patients receiving abdominalsurgery. On the other hand, zinc deficiency is associated withimpaired wound healing (39). Thus, it is possible that zinc-deficient patients would benefit more from the multinutrienttherapy.
The multinutrient supplement was tolerated well, and thecompliance was acceptable. We assessed compliance withmultinutrient supplementation for 14 d after surgery becausethe effect of nutrient supplementation on the deposition ofcollagen of early stimulation of collagen synthesis seems tofirst become evident on postoperative day 14 (30, 32). Thisinformation is important when designing future larger clinicaltrials.
There is an increasing body of evidence regarding thebeneficial effects of immunonutrients on improving surgicaloutcomes (41). Direct inguinal hernia is a known risk factorfor hernia recurrence (42). Recurrence was observed in 4 of ourpatients with direct inguinal hernia but in none of the patientswith indirect inguinal hernia within the 1-y follow-up period.Three of these patients were in the control group comparedwith only 1 patient in the multinutrient group. Although ournovel biochemical findings are encouraging, the small samplesize precludes the drawing of conclusions on the definite clinicalimpact.
In conclusion, perioperative oral multinutrient supplemen-tation of arginine, glutamine, vitamin C, and zinc maintainedtype V collagen synthesis systemically following inguinal herniarepair and increased early type I collagen synthesis in wounds. Alarger trial is warranted to confirm whether these early changesin the collagen profile translate into improved wound healingand long-term clinical outcomes after inguinal hernia repair.
Acknowledgments
We thank Bonna Leerhøy for drawing blood from the healthyvolunteers. The authors’ responsibilities were as follows—MK,AKSF, JRA, LNJ, MSA: designed the study; MK and AKSF:conducted the study; MK, ASKF, NIN, NW, GvH and MSA:performed biochemical analyses; MK and LNJ: performedstatistical analyses and interpreted the data; MK: drafted thefirst manuscript; MSA: had the primary responsibility of themanuscript content; and all authors: read and approved the finalmanuscript.
References1. Kingsnorth A. Treating inguinal hernias. BMJ 2004;328:59–60.
2. Fitzgibbons RJ, Forse RA. Groin hernias in adults. N Engl J Med2015;372:756–63.
3. Henriksen NA, Mortensen JH, Sorensen LT, Bay-Jensen AC, Agren MS,Jorgensen LN, Karsdal MA. The collagen turnover profile is alteredin patients with inguinal and incisional hernia. Surgery 2015;157:312–21.
4. Henriksen NA, Yadete DH, Sorensen LT, Agren MS, Jorgensen LN.Connective tissue alteration in abdominal wall hernia. Br J Surg2011;98:210–9.
5. Mak KM, Png CY, Lee DJ. Type V collagen in health, disease, andfibrosis. Anat Rec 2016;299:613–29.
6. Park AC, Phan N, Massoudi D, Liu Z, Kernien JF, Adams SM, DavidsonJM, Birk DE, Liu B, Greenspan DS. Deficits in Col5a2 expression resultin novel skin and adipose abnormalities and predisposition to aorticaneurysms and dissections. Am J Pathol 2017;187:2300–11.
7. Albaugh VL, Mukherjee K, Barbul A. Proline precursors and collagensynthesis: biochemical challenges of nutrient supplementation andwound healing. J Nutr 2017;147:2011–7.
8. Blass SC, Goost H, Tolba RH, Stoffel-Wagner B, Kabir K, BurgerC, Stehle P, Ellinger S. Time to wound closure in trauma patientswith disorders in wound healing is shortened by supplementscontaining antioxidant micronutrients and glutamine: a PRCT. ClinNutr 2012;31:469–75.
9. Peterkofsky B. Ascorbate requirement for hydroxylation and secretionof procollagen: relationship to inhibition of collagen synthesis in scurvy.Am J Clin Nutr 1991;54:1135S–40S.
10. Agren MS, Andersen L, Heegaard AM, Jorgensen LN. Effect ofparenteral zinc sulfate on colon anastomosis repair in the rat. Int JColorectal Dis 2008;23:857–61.
11. Askanazi J, Carpentier YA, Michelsen CB, Elwyn DH, Furst P,Kantrowitz LR, Gump FE, Kinney JM. Muscle and plasma aminoacids following injury. Influence of intercurrent infection. Ann Surg1980;192:78–85.
12. Viggiano E, Passavanti MB, Pace MC, Sansone P, Spaziano G, ViggianoA, Aurilio C, Monda M, Viggiano A, Pota V, De Luca B, De Luca E.Plasma glutamine decreases immediately after surgery and is related toincisiveness. J Cell Physiol 2012;227:1988–91.
Collagen synthesis during surgical wound healing 7
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020

13. Pribis JP, Zhu X, Vodovotz Y, Ochoa JB. Systemic arginine depletionafter a murine model of surgery or trauma. J Parenter Enter Nutr2012;36:53–9.
14. Oguz M, Kerem M, Bedirli A, Mentes BB, Sakrak O, Salman B, BostanciH. L-alanin-L-glutamine supplementation improves the outcome aftercolorectal surgery for cancer. Colorectal Dis 2007;9:515–20.
15. Fukushima R, Yamazaki E. Vitamin C requirement in surgical patients.Curr Opin Clin Nutr Metab Care 2010;13:669–76.
16. Yamazaki E, Horikawa M, Fukushima R. Vitamin C supplementation inpatients receiving peripheral parenteral nutrition after gastrointestinalsurgery. Nutrition 2011;27:435–9.
17. Faure H, Peyrin JC, Richard MJ, Favier A. Parenteral supplementationwith zinc in surgical patients corrects postoperative serum-zinc drop.Biol Trace Elem Res 1991;30:37–45.
18. Nordic Council of Ministers . Nordic nutrition recommendations 2012:integrating nutrition and physical activity, 5th edn. Copenhagen: NordicCouncil of Ministers, 2014.
19. Larsen HF, Ahlström MG, Gjerdrum LMR, Mogensen M,Ghathian K, Calum H, Sørensen AL, Forman JL, VandevenM, Holerca MN, et al. Noninvasive measurement ofreepithelialization and microvascularity of suction-blister woundswith benchmarking to histology. Wound Repair Regen 2017;25:984–93.
20. Lorentzen L, Henriksen NA, Juhl P, Mortensen JH, Agren MS, KarsdalMA, Jorgensen LN. Type V collagen is persistently altered after inguinalhernia repair. Scand J Surg 2018;107:212–7.
21. Mirastschijski U, Martin A, Jorgensen LN, Sampson B, Agren MS. Zinc,copper, and selenium tissue levels and their relation to subcutaneousabscess, minor surgery, and wound healing in humans. Biol Trace ElemRes 2013;153:76–83.
22. Schadewaldt P. Analysis of (S)- and (R)-3-methyl-2-oxopentanoateenantiomorphs in body fluids. Methods Enzymol 2000;324:33–9.
23. Bornø A, van Hall G. Quantitative amino acid profiling and stableisotopically labeled amino acid tracer enrichment used for in vivohuman systemic and tissue kinetics measurements. J Chromatogr BAnalyt Technol Biomed Life Sci 2014;951–952:69–77.
24. Rodushkin I, Odman F. Application of inductively coupled plasmasector field mass spectrometry for elemental analysis of urine. J TraceElem Med Biol 2001;14:241–7.
25. Assaad HI, Hou Y, Zhou L, Carroll RJ, Wu G. Rapid publication-readyMS-Word tables for two-way ANOVA. Springerplus 2015;4:33.
26. Mayhew D, Mendonca V, Murthy BVS. A review of ASA physicalstatus—historical perspectives and modern developments. Anaesthesia2019;74:373–9.
27. Vats M, Pandey D, Saha S, Talwar N, Saurabh G, Andley M,Kumar A. Assessment of systemic inflammatory response after total
extraperitoneal repair and Lichtenstein repair for inguinal hernia.Hernia 2017;21:65–71.
28. Haukipuro K, Melkkocand J, Risteli L, Kairaluoma MI, Risteli J.Synthesis of type I collagen in healing wounds in humans. Ann Surg1991;213:75–80.
29. Sumiyoshi H, Kitamura H, Matsuo N, Tatsukawa S, Ishikawa K,Okamoto O, Fujikura Y, Fujiwara S, Yoshioka H. Transient expressionof mouse pro-α3(V) collagen gene (col5a3) in wound healing. ConnectTissue Res 2012;53:313–7.
30. Kirk SJ, Hurson M, Regan MC, Holt DR, Wasserkrug HL, Barbul A.Arginine stimulates wound healing and immune function in elderlyhuman beings. Surgery 1993;114:155–9.
31. Debats IB, Booi DI, Wehrens KM, Cleutjens J, Deutz NE, van de HogenE, Bemelmans M, van der Hulst RW. Oral arginine supplementation andthe effect on skin graft donor sites: a randomized clinical pilot study. JBurn Care Res 2009;30:417–26.
32. Williams JZ, Abumrad N, Barbul A. Effect of a specialized amino acidmixture on human collagen deposition. Ann Surg 2002;236:369–74.
33. Floyd JC, Jr, Fajans SS, Conn JW, Knopf RF, Rull J. Stimulationof insulin secretion by amino acids. J Clin Invest 1966;45:1487–502.
34. Rickels MR, Naji A, Teff KL. Acute insulin responses to glucose andarginine as predictors of beta-cell secretory capacity in human islettransplantation. Transplantation 2007;84:1357–60.
35. Zhang XJ, Chinkes DL, Wolfe RR. The anabolic effect of arginineon proteins in skin wound and muscle is independent of nitric oxideproduction. Clin Nutr 2008;27:649–56.
36. Kornhuber ME, Balabanova S, Heiligensetzer GV, Kornhuber C,Zettlmeissl H, Kornhuber AW. Stability of human blood serumaminoacids after storage at different pH and temperature conditions.Clin Chim Acta 1991;197:189–200.
37. Guo S, DiPietro LA. Factors affecting wound healing. J Dent Res2010;89:219–29.
38. Karlsen A, Blomhoff R, Gundersen TE. Stability of whole blood andplasma ascorbic acid. Eur J Clin Nutr 2007;61:1233–6.
39. Lansdown ABG, Mirastschijski U, Stubbs N, Scanlon E, Agren MS. Zincin wound healing: theoretical, experimental, and clinical aspects. WoundRepair Regen 2007;15:2–16.
40. Li J, Zhang X, Sun Q, Li W, Yu A, Fu H, Chen K. Circulating matrixmetalloproteinases and procollagen propeptides in inguinal hernia.Hernia 2018;22:541–7.
41. Drover JW, Dhaliwal R, Weitzel L, Wischmeyer PE, Ochoa JB, HeylandDK. Perioperative use of arginine-supplemented diets: a systematicreview of the evidence. J Am Coll Surg 2011;212:385–99.
42. Burcharth J, Andresen K, Pommergaard HC, Bisgaard T, RosenbergJ. Recurrence patterns of direct and indirect inguinal hernias in anationwide population in Denmark. Surgery 2014;155:173–7.
8 Kjaer et al.
Dow
nloaded from https://academ
ic.oup.com/jn/advance-article-abstract/doi/10.1093/jn/nxz324/5695303 by U
niversity of Toronto Library user on 04 January 2020





























