Embed Size (px)
Citation preview

Figure 2. Ultrasound biomicroscopy performed 18 days after the second operation confirms that the ciliochoroi-dal detachment has disappeared.
In our patient, treatment of persistent hypotony after uncomplicated vitreous surgery required excision of the residual anteroperipheral vitreous combined with fluid-gas exchange and diathermy around the sites of sclerotomy to resolve the fractional forces and achieve the adhesion of the ciliary body to the sclera. Images obtained by ultrasound biomicroscopy in this patient clearly showed ciliochoroidal detachment and its regression, which had not been observed by ophthalmoscopy.
REFERENCES
1. Zarbin MA, Michels RG, Green WR. Dissection of epiciliary tissue to treat chronic hypotony after surgery for retinal detachment with proliferative vitreoretinopathy. Retina 1991;11:208-213.
2. Aaberg TM. Management of anterior and posterior proliferative vitreoretinopathy. XLV Edward Jackson Memorial Lecture. Am ] Ophthalmol 1988;106:519-532.
Nocardia Scleritis C. Michele Knox, MD, FRCSC, John P. Whitcher, MD, MPH, Vickey Cevellos, MT, Todd P. Margolis, MD, PhD, and Alex R. Irvine, MD
PURPOSE: To describe a case of Nocardia scleritis, an unusual ocular infection.
METHODS: Case report and review of pertinent literature. RESULTS: An 83-year-old man with leukocyto-clastic vasculitis was initially examined for infectious necrotizing scleritis after explantation of an extruded scleral buckle. The patient was successfully treated with sulfonamides. CONCLUSIONS: Nocardia asteroides may cause infectious scleritis in the absence of cataract surgery or trauma. Treatment with sulfonamides can result in a satisfactory outcome.
I NFECTIOUS SCLERITIS IS UNCOMMON, PARTICULARLY
in the absence of infectious keratitis. We describe a case of infectious scleritis caused by Nocardia asteroides.
An 83-year-old man with bilateral retinal detachment surgery 10 years previously was initially examined for pain and discharge of 5 weeks' duration in his left eye. In the left eye, the scleral buckle was exposed, then explanted 1 week later. After surgery, the patient had a superotemporal conjunctival defect, with pain and discharge despite treatment with ciprofloxacin 0.03% and gentamicin 0.3% eyedrops. Medical history was remarkable for low-grade leukocytoclastic vasculitis, with positive antinuclear antibody (1:640 speckled) and perinuclear antineutrophil cytoplasmic antibody (1:80). Medications included oral hydroxy-chloroquine and dexamethasone (0.50 mg daily).
Best-corrected visual acuity was LE, 20/100, with mucopurulent material in the conjunctival fornix. The conjunctiva was markedly injected with a 4 X 4-mm area of scleral necrosis superotemporally. The cornea was clear. A moderate cellular reaction was present in the anterior chamber, with one posterior synechia and nuclear sclerosis. The vitreous had no cellular reaction, and results of dilated ophthalmo-scopic examination were unremarkable. Scrapings from the necrotic sclera were taken for stains and culture. Vancomycin, 50 mg/ml, and gentamicin, 14
Accepted for publication Dec 13, 1996. Department of Ophthalmology (C.M.K., J.P.W., T.P.M., A.R.I.) and
the Francis I. Proctor Foundation (C.M.K., J.P.W., V.C., T.P.M.), University of California, San Francisco. Presented as a case at the meeting of the Ocular Microbiology and Immunology Group, Chicago, Illinois, October 26, 1996.
Inquiries to John P. Whitcher, MD, MPH, Proctor Foundation, 95 Kirkham, University of California, San Francisco, CA 94122-0944; fax: (415) 502-2521; e-mail: [email protected]
VOL.123, No. 5 BRIEF REPORTS 713

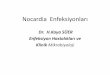
Figure 1. Nocardia asteroides, gram stain from culture, showing filamentous organisms.
mg/ml, eyedrops were begun hourly. The preliminary laboratory identification was Nocardia; vancomycin was discontinued and gentamicin was changed to amikacin, 13.4 mg/ml eyedrops. A subconjunctival injection of amikacin, 25 mg, was given. Trimetho-prim (160 mg)-sulfamethoxazole (800 mg) tablets were begun twice daily, and sodium sulfacetamide 30% eyedrops were begun hourly.
The laboratory diagnosis was later confirmed as N asteroides (Figure 1). The necrotic sclera sloughed with granulation tissue forming in the scleral bed (Figure 2) during a period of 6 weeks; antibiotics were then tapered. Final dimensions of the affected scleral area measured 10 X 6 mm.
The clinical course was complicated by a sterile corneal epithelial defect that developed after 1 week of amikacin eyedrops. A corneal facet persisted. Best-corrected visual acuity 6 months after referral had improved to LE, 20/60. The right eye remained free of inflammation throughout the episode of infectious scleritis in the left eye.
To our knowledge, three cases of Nocardia scleritis have been described. Two cases1,2 occurred within 2 weeks of cataract surgery, and a third case occurred after trauma with vegetable matter.3 Our patient is unique in that he had neither a history of cataract surgery nor trauma. Nocardia asteroides infection immediately after scleral buckling surgery has been
714 AMERICAN JOURNAL
Figure 2. Left eye, showing area of necrotizing scleritis, with granulation tissue, caused by N asteroides.
reported4 but is presumed to be caused by organisms introduced at the time of surgery.
Susceptibility testing for medically important No' cardia species shows sulfamethoxazole and amikacin to be the best antibiotic choices.5 High doses for extended periods are recommended, but complications may result, as shown by the amikacin-related corneal epithelial defect in our patient. However, one case previously described resulted in loss of the eye despite intravenous and topical sulfamethoxazole and trimethoprim.1 One other case previously described was successfully treated with cephazolin, and the Nocardia species was sensitive to only this antibiotic.3
Nocardia asteroides may cause infectious scleritis in the absence of preceding cataract surgery or trauma. In this case, treatment with sulfonamides resulted in a satisfactory outcome.
REFERENCES
1. Katten HM, Pflugfelder SC. Nocardia scleritis. Am J Ophthal-mol 1990;110:446-447.
2. Brooks JGJ, Mills RAD, Coster DJ. Nocardial scleritis. Am J Ophthalmol 1992;114:371-372.
3. Basti S, Gopinathan U, Gupta S. Nocardial necrotizing scleritis after trauma. Cornea 1994;13:274-275.
4. King LP, Furlong WB, Gilbert WS, et al. Nocardia asteroides infection following scleral buckling. Ophthalmic Surg 1991; 22:150-152.
5. McNeil MM, Brown JM. The medically important aerobic actinomycetes: epidemiology and microbiology. Clin Microbiol Rev 1994;7:357-417.
OPHTHALMOLOGY MAY 1997





![Presentaci n Micetoma 2010 [Modo de compatibilidad]micofbioyf.wikispaces.com/file/view/micetomas+PW.pdf · microscópica Nocardia brasiliensis Blanco a amarillo ,, lobulado, ... Identificación](https://img.pdfslide.tips/doc/110x75/5afc62ea7f8b9a8b4d8c11ae/presentaci-n-micetoma-2010-modo-de-compatibilidad-pwpdfmicroscpica-nocardia-brasiliensis.jpg)