Embed Size (px)
Citation preview
NO
SO IN
FOAssociation Belge pour lrsquoHygiegravene Hospitaliegravere Belgische Vereniging voor Ziekenhuishygieumlne
Groupement pour le Deacutepistage lrsquoEtude et la Preacutevention desInfections HospitaliegraveresGroep ter Opsporing Studie en Preventie van de Infecties inZiekenhuizen
De vooruitgang in de moderne geneeskunde maakt het grootschalig gebruik vanintravasculaire hulpmiddelen mogelijk en stelt de patieumlnt bloot aan bepaaldesoorten infectieuze complicaties Deze komen voor onder de vorm van lokaleinfecties en systeeminfecties daartoe behoren de besmettingen van deinsteekplaats septische thromboflebitis bacterieumlmieeumlnhellip In een studie over deprevalentie van infecties op de reanimatieafdeling een afdeling die bijzonderonderhevig is aan gevaar voor bijbesmetting wordt door JL Vincent aangetoonddat bacterieumlmieeumln de derde oorzaak uitmaken van verworven infecties na derespiratoire en de urineweginfecties Een belangrijk deel van deze bacterieumlmieeumln iskatheter gerelateerd Zoals Pittet gepubliceerd heeft liggen deze besmettingen aande basis van een verlenging van het verblijf op de intensieve zorgenafdeling meteen kostprijsstijging die wel kan oplopen tot euro 30000 en een niet te verwaarlozenmortaliteit Het gaat hier dus over een prioritair probleem binnen het kader vannosocomiale infecties te meer doordat het grootste deel van de besmettingencatheter gerelateerd zijn en dus theoretisch vermeden hadden kunnen worden
De perifeer veneuze catheters behoren tot de meest gebruikte intravasculairehulpmiddelen (prevalentie in Europa 63 J Hosp Infect 1983 4 338-349)Deincidentie van deze catheter gerelateerde infecties is gewoonlijk laag maar zondertwijfel niet verwaarloosbaar wegens het grote aantal geplaatste catheters In eenrecente multicenter- studie wordt door Hirchmann een laag aantal complicaties(namelijk 24) gerapporteerd voor infecties die gerelateerd zijn met deaanwezigheid van perifere veneuze catheters Voorts toont hij aan dat enerzijds hetdragen van handschoenen en anderzijds de handontsmetting het aantal van dezecomplicaties op significante wijze doet dalen (J Hosp infect 2001 49 199-203)Een werkgroep van de BVZH heeft een multicenter- studie ondernomen die hetbeheer van de perifeer veneuze catheters behandelt Er werden 24 indicatorenbestudeerd en hun resultaten worden verder in dit nummer gepubliceerd Ze zijnerg bemoedigend
De nieuwe items De Hoge Gezondheidsraad heeft in october 2000aanbevelingen gepubliceerd over de preventie van catheter gerelateerde infectiesHet CDC heeft net een ontwerptekst gepubliceerd met hun nieuwe aanbevelingenCorine Logghe heeft deze Amerikaanse richtlijnen vergeleken met deze van deHoge Gezondheidsraad en heeft ze in tabelvorm samengevat
In Belgieuml hebben we het geluk dat we reeds 10 jaar beschikken over een goedwerkend surveillance systeem voor septicemieeumln De komst van hetkwaliteitsdecreet van de Vlaamse gemeenschap heeft de resultaten enigszinsgewijzigd Carl Suetens analyseert de weerslag van dat decreet op de incidentie vande bacterieumlmieeumln veroorzaakt door coagulase negatieve Stafylokokken in hetNoorden en in het Zuiden
In dit nummer stellen we een mooi overzichtsartikel voor over de nosocomialeinfecties verbonden met de anesthesie Dit artikel is het werk van Dr Joseph Hajjaranesthesist en thans bekeerd tot het voorkomen van infecties
Anne Simon
INHOUDEDITORIAAL
11
2
8
10
18
Trimestrieel VOL VI ndeg 11ste kwartaal 2002
Uitgifte kantoor 1200 ndash BRUSSEL
Verantwoordelijke uitgever Dr Y GlupczynskiUCL - 5490 - MBLGHippocrateslaan 54B ndash 1200 - BRUSSEL
Met de steun van het Ministerie vanSociale Zaken Volksgezondheid enLeefmilieu Esplanadegebouw Pachecolaan 195 1010 BRUSSEL
14
25
Epidemiologie en preventie vannosocomiale infecties gerelateerdaan anesthesie
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk
CDC (Draft guideline for theprevention of intravascularcatheter-related )
Hogere incidentie septicemieenmet coagulase-negatieve stafylo-kokken na introductie kwaliteit-decreet in Vlaanderen
Aanbevelingen
Actualiteiten
Abstracts van 1ste augustus tot 31 october 2001
Wetenschappelijke agenda
Sites Web26
20
N O S O - i n f o v o l V I n deg 1 2 0 0 2
2
Epidemiologie en preventie van nosocomiale infecties gerelateerdaan anesthesieJ Hajjar Eidlin ndash HC Valence
De enquecircte die door de Franse Vereniging voor Anesthesieen Reanimatie in 1966 werd uitgevoerd schat het aantalanesthesies op acht miljoen per jaar In 75 van degevallen was dit in Frankrijk naar aanleiding van eenchirurgische ingreep (1) De post-operatieve wondinfectie(POWI) is de meest voorkomende complicatie in dechirurgie maar de geopereerde patieumlnt loopt anderzijdsook nog het risico van infectie op afstand van deoperatiewonde Tot deze laatste categorie behoren de ARIIn beide gevallen bestaan er meerdere factoren die hetoptreden ervan bevorderen Hoewel men thans deepidemiologie van de POWI goed kent (de incidentiewordt gemiddeld op 3 geschat alle soorten chirurgischeingrepen dooreen genomen) is de kennis over de ARI vanrecentere datum Het peri-operatieve gebeuren houdttevens voor zowel het chirurgisch als het anesthesieteameen potentieel risico in op besmetting metbloedoverdraagbare pathogenen Dit risico is uiteraardafhankelijk van de frequentie van de accidentieleblootstelling aan bloed Een betere inschatting van degevaren op ARI heeft het mogelijk gemaakt om specifiekerichtlijnen op te stellen De toepassing van deze richtlijnenis onmisbaar voor een doeltreffende preventie vaninfecties bij patieumlnten die een heelkundige ingreep moetenondergaan (2-5)
Epidemiologie van nosocomiale infecties als gevolg vande anesthesie
FrequentieVroeger kwamen de ARI voornamelijk als secundaire
epidemieeumln voor Deze werden veroorzaakt door hetgebruik van slecht gedesinfecteerde anesthesie circuitsdoor injectie van anesthetica uit besmette multidosisflacons of door het gebruik van spuiten die reeds langerdan 24 uur op voorhand waren klaargemaakt (67)
Aangezien de moleculaire typeringstechnieken op hetmoment van die publicaties nog niet bestonden dient mentoch voor enkele gevallen voorzichtig te zijn bij hettrekken van conclusies Met uitzondering van epidemischetoestanden waren de meeste enquecirctes retrospectief envaak tendentieus op vlak van de methodiek (8) Anderzijdshadden de prospectieve enquecirctes vooral betrekking op deepidurale verdovingIn een eerste prospectieve studie uitgevoerd op 400patieumlnten over een termijn van 10 maanden bedroeg deincidentie van infecties 15 bedroeg (deze infectieswerden microbiologisch gedocumenteerd) (9) Een recenteprospectieve multicenterstudie uitgevoerd op 7300patieumlnten uit 13 deelnemende instellingen kwam tot eenincidentie van 34 op 1000 anesthesies (10) Van de 7300patieumlnten werden er 25 geiumlnfecteerd (bij 9 was devasculaire kateter besmet 12 werden besmet via hetbeademingstoestel en bij 4 werd het oog en de mondholtegeiumlnfecteerd) Enkel de patieumlnten onderworpen aan eenanesthesie die langer duurde dan 2 uur of die eenbloedtransfusie kregen hadden een hogere incidentieDeze globale incidentie lijkt op het eerste gezicht laagmen dient dit echter in perspectief te brengen met hetenorm aantal ingrepen met anesthesie die jaarlijks inFrankrijk plaatshebben
ORIGINELE ARTIKEL
Hieronder geven wij U een origineel bericht weer dit metde toelating van de hoofdredakteur Dr J Fabry van Dr JHajjar anesthesist en nu ook overtuigd van de preventievan nosocomiale infecties
Dit artikel gepubliceerd in het blad HYGIENE (officieelblad van de franse instelling Klinische Hygieumlne) 2001 IXnr 5 spreekt over de niet dikwijls aangehaaldenosocomiale infecties bij anesthesie
AbstractPatieumlnten die een operatie hebben ondergaan zijn vatbaar voortwee types van nosocomiale infecties Enerzijds zijn er debesmettingen op de plaats van de ingreep en anderzijds zijn er deinfecties die zich situeren op afstand van de operatiewonde Totdeze laatste soort behoren de anesthesie gerelateerde infecties(ARI = Anesthaesia related infections) Een beter inzicht over hetaantal de plaats en de risicofactoren van de ARI hebben deanesthesisten doen beseffen dat er wel degelijk een probleembestaat Ondanks de geringe incidentie is het gezien het hogeaantal jaarlijks uitgevoerde anesthesies noodzakelijk om de doorde specialisten aanbevolen richtlijnen toe te passenSleutelwoorden Anesthesie ndash Nosocomiale infecties ndashPreventieve maatregelen ndash Voorschriften
Epidemiology and prevention of nosocomial infectionsassociated with anaesthesiaSummarySurgical patients are susceptible to two types of nosocomialinfections surgical site infections and distant infections such asthose associated with anaesthesia (IAA) Better knowledge of therates sites and risk factors of IAA allow anaesthesia teams to beconscious of the problem Despite a low incidence rate the highnumber of anaesthesias performed each year necessitates theimplementation of recommendations stipulated by professionalsof this specialty
Key-Words Anaesthestia ndash Cross infections ndash Prevention ndashGuidelines
Voornaamste soorten infecties en risicofactoren
Infecties ontstaan door gebruik van materieel gebruikt tercontrole van de luchtwegen en voor mechanischeventilatieHet materieel dat men gebruikt voor controle van deluchtwegen en voor mechanische ventilatie komt incontact met normale flora uit de slijmvliezen van debovenste luchtwegen en spijsvertering Het gaat hier meerbepaald om speeksel en tracheabronchiale secreties diesoms ook bloed kunnen bevatten Dit materieel omvatenerzijds de benodigdheden voor manuele ventilatie(maskers ventielen extremiteiten van de laryngoscopenendotracheale tubes enz) alsook de apparatuur voormechanische ventilatie (externe- en interne leidingen vande beademingstoestellen luchtbevochtigers enz) Eendeel van dit materieel heeft specifieke risicofactoren dieverband houden met de contaminatie door de amandelen(intrusie met ulceraties of contact van meer dan eacuteeacuten uur)en equivalente weefsels rond het scheidingsvlak tussenluchtwegen en spijsvertering Deze beschouwt men alsweefsels met verhoogd besmettingsgevaar voor nietconventioneel overdraagbare pathogenen (NCOP)Onaangepaste of ontoereikende manipulatie van ditmaterieel (al of niet met betrekking tot NCOP) enhandelingen door het verplegend personeel tijdens hetverstrekken van zorgen (intubatie extubatie aspiratie)kunnen aan de basis liggen van kruisbesmettingen metpathogenen Deze kunnen al of niet behoren tot denormale flora van de luchtwegen zoals weergegeven ineen publicatie waarbij men de transmissie van Hepatitis Cvirus heeft vastgesteld bij twee op elkaar volgendepatieumlnten via een beademingscircuit zonderantimicrobieumlle filter en zonder vervanging ervan tussen depatieumlnten (11)Dergelijke toestanden hebben het reeds verschillendejaren durende debat over de implicaties van de anesthesiecircuits omgebogen Deze kunnen een rol spelen in deoverdracht van micro-organismen infecties doen ontstaanen een gevaar betekenen voor kruisbesmettingen (in hetbijzonder met virussen) (12) Dit risico is voor vele auteursontegensprekelijk het bewijs wordt enerzijds geleverddoor de positiviteit van bacteriologische stalen afgenomentijdens het routinewerk en anderzijds door in vitro studiesMaar voor anderen vormen de leidingen zelfs al zijn zebesmet geen bron van besmetting Dit komt doordatgezien de ongunstige factoren voor ontwikkeling vanbacterieumln er geen significante hoeveelheid micro-organismen overgedragen wordtHet optreden van postoperatieve pneumopathieeumln vormthet meest gebruikte beoordelingscriterium uit studies overde rol van de anesthesie circuits Dit criterium is moeilijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
3
te hanteren om het risico van kruisbesmetting in teschatten Het is inderdaad een feit dat elke initieumllebijbesmetting van de anesthesie uitrusting buitenbeschouwing gelaten er tijdens de kunstmatigebeademing enkele erg belangrijke factoren aan de basiskunnen liggen van postoperatieve pneumopathieeumln Dezefactoren zijn een kortsluiting van de bovenste luchtwegendoor de endotracheale tube het gebruik van anestheticadoor inhalatie evenals de toediening van verdovendemedicatie die de ciliaire activiteit van het bronchialeepithelium onderdrukken en tenslotte de verspreiding vande normale pharyngiale flora naar de tracheaDe respiratoire antecedenten van de patieumlnt en het typevan heelkundige ingreep vormen de andere risicofactoren
Infecties gerelateerd met invasieve handelingen
Zowel de plaatsing van vasculaire catheters de cathetersvoor loco- regionale anesthesie als de intraveneuzemanipulatie van anesthetica kunnen infecties veroorzakenals de steriliteitregels niet in acht genomen wordenbull Omtrent de perifeer veneuze catheters De meeste
risicohoudende situaties worden enerzijds bepaalddoor de kwaliteit van de huidontsmetting op hetmoment van de catheterplaatsing en anderzijds detijdsduur van de catheterisatie De resultaten van eenstudie over catheters die in het operatiekwartierwerden geplaatst confirmeren deze bevindingen erwerd kolonisatie vastgesteld bij 31 van de 1138perifeer veneuze catheters Een antiseptischehuidbehandeling in vier fasen op het moment van deplaatsing (huidreiniging met een antiseptische zeepspoelen drogen en de toepassing van eenontsmettingsmiddel verenigbaar met de zeep)gekoppeld aan een plaatsingsduur van minder dan 72uur verklaart het erg laag kolonisatiecijfer (27) (13)In hoger genoemde studie was er 1 infectie op 1000operaties als gevolg van de aanwezigheid van eenperifeer veneuze catheter Alhoewel het verschilstatistisch niet significant is constateerde men slechtseacuteeacuten enkele perifeer veneuze catheterbesmetting opeacuteeacuten van de zes verpleegeenheden die de antiseptischehuidreiniging in vier fasen toepasten In vergelijkingdaarmee werden er vier besmettingen gerapporteerdop negen afdelingen die deze reinigingsprocedure niettoepasten (10) Hoewel het besmettingsgevaar op heteerste gezicht gering lijkt moet men toch aandachthebben voor de frequentie van de manipulaties Menmoet steeds voor ogen houden hoe ernstig de gevolgenkunnen zijn van een eventuele infectie bij een patieumlntmet een endovasculaire prothese
N O S O - i n f o v o l V I n deg 1 2 0 0 2
4
Tabel I Epidemische gevallen veroorzaakt door toediening van een injectie met een inspuitbaar anestheticum en doorintravasculaire procedures (volgens HERWALDT) (6)
Auteur (jaar)
Sack (1970)
Siboni (1979)
Maldonaldo (1989)
CDC (1990)
CDC (1990)
CDC (1990)
CDC (1990)
Maxi (1991)
Froggatt (1991)
Rudnick (1991)
Bron
Dezelfde IV oplossing voormeerdere patieumlnten
Fentanyl
Lidocaine(multidosis flacon)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Fentanyl(injectiespuit
vooraf gevuld)
Injectiespuitgemeenschappelijk voor
meerdere patieumlnten
Vooraf samengestelde arterieumlle drukset
Infectie
Bacteriemie
Bacteriemie
Hepatitis
Endophtalmie
Koorts
Bacteriemie
KoortsPostoperatieve wondinfectie
BacteriemiePosoperatieve wondinfectie
Hepatitis
Bacteriemie
Patieumlntsen (aantal)
5
16
5
4
2
13
8
3
6
9
Pathogene kiem
K pneumoniae
P cepacia
Virus heacutepatite B
C albicans
Moraxella
S aureus
S aureus
P picketti
Virus heacutepatite B
P aeruginosa
bull In de literatuur zijn reeds verschillende publicatiesverschenen over epidemieeumln veroorzaakt doorbacterieumln of schimmels (Tabel1) (8) Deze wordenin verband gebracht met de extrinsieke besmettingvan anesthetica door omgevingskiemen tijdensbereiding en manipulatie van de preparatenPROPOFOL is het meest onderhevig aanbijbesmetting aangezien het een olieachtigevloeistof is zonder conserveermiddel nochbacterieremmend product Daardoor wordt deontwikkeling van micro-organismen in de handgewerkt met als bijkomende risicofactor dat hetvooraf bereide preparaat langzaam via perfusiewordt toegediend Maar andere preparaten zoalsFENATYL of LIDOCAIumlNE worden evenzeer alsmogelijke bron van bijbesmetting gezien als eenzelfde oplossing wordt toegediend aanverschillende patieumlnten Het gebruik van dezelfdeinjectiespuit bij verschillende patieumlnten is de
oorzaak van besmettingen met Hepatitis B viruszelfs wanneer de injectienaalden vervangen zijnVerschillende studies hebben reeds de gevaren vandergelijke onaanvaardbare praktijken aangetoond(1415)
bull Hoewel secundaire besmettingen bij loco-regionale anesthesie potentieel ernstig kunnen zijnis de incidentie ervan niet precies gekend (1617)De waarden die men terugvindt hebben meestalbetrekking op epidurale verdoving bij bevallingenen varieumlren nogal sterk van 008 tot 00002 Inde literatuur worden op 28 infectieuzecomplicaties 21 gevallen beschreven metepidurale abcessen 6 met meningitis en eacuteeacuten gevalmet spondylitis (18) Als men de verwikkelingen bijrachianesthesie beschouwt rapporteren er zevenstudies vier gevallen van meningitis op een totaalvan 90000 patieumlnten een besmettingcijfer van
verpleegeenheid Men kan drie risicomomentenonderscheiden met name het toepassen van invasievetechnieken het ophalen van afval en het onderhoudvan bevuild materieel Het risico van seroconversie isafhankelijk van reeds hoger vernoemde factoren hetaantal infecties bij de patieumlnten en zodoende deprevalentie in de populatie het chronischedragerschap van virussen in het bloed van debesmette personen de kwantiteit en virulentie van hetinfectieus organisme en de aard van de accidenteleblootstelling (percutane verwonding door een prikinsnijding of contact met huid of slijmvlies) Devoornaamste factoren die tot een seroconversie leidenzijn eveneens gekend een diepe prikwonde door eenmet bloed besmette holle naald of een wonde metmaterieel dat gebruikt werd voor een vasculaireingreep bij een patieumlnt met een hoge antivirus titerHet niet dragen van handschoenen is daarbij eensupplementaire risicofactor Het professionelebesmettingsgevaar wordt door het personeel meestalhoger ingeschat voor HIV en meestal onderschat voorHBV Dit wordt aangetoond uit de resultaten van eenrondvraag die in 1995 werd ondernomen bij 300verpleegkundigen uit de anesthesie afdeling Metbetrekking tot HIV werd het risico door 18 vandeze verpleegkundigen geschat op groter dan of gelijkaan 30 (amper 29 hadden het cijfer juist) voorHBV werd door 30 gedacht dat het risico kleinerdan of gelijk was aan 03 (amper 21 hadden hetcijfer juist) Uit de groep van 42 professionele HIV-infecties die op 30 juni 1998 gerecenseerd werdenbetrof het in twee gevallen een anesthesist -reanimator op een totaal van 29 vermoede infecties(21)
Preventieve maatregelen en strategie bij hetimplementeren
De preventieve maatregelen die in 1997 door deFranse Vereniging voor Anesthesie en Reanimatiegepubliceerd werden zijn hoofdzakelijk toegespitstop de controle op exogene reservoirs en hetvoorkomen van overdracht (2)
Algemene aanbevelingenbull Men dient te beschikken over geschikte kledij en
een algemeen gedragspatroon vertonen passendbij het operatiekwartier Vooraleer de operatiezaalte betreden en gedurende de ganse duur van deingreep dient men op een correcte manier eenmasker te dragen en een passend haarbedekkendhoofddeksel aan te hebben Men dient deverplaatsingen minimaal te houden
bull Men dient de kiemoverdracht via de handen en
N O S O - i n f o v o l V I n deg 1 2 0 0 2
5
00045 In vergelijking met de risicofactoren bijvasculaire catheters is het waarschijnlijk dat destaat van de huid rond de insteekplaats deplaatsingsduur van de catheter en de frequentievan het herinspuiten zoveel factoren meer zijn diehet besmettingsrisico verhogen (19)
Het is belangrijk zich te herinneren dat hetzenuwstelsel (met inbegrip van het hersenvlies encerebrospinaal vocht) bijzonder gevoelig is voorbesmettingen veroorzaakt door niet conventioneleoverdraagbare pathogenen Het materieel datgebruikt wordt voor loco- regionale anesthesieschept de mogelijkheid van overdracht met dezekiemen
De professionele besmettingrisicorsquosHet gevaar van professionele besmetting bij hetanesthesiepersoneel wordt in hoofdzaak gevormddoor eventueel contact met de hepatitis virussen(meer in het bijzonder de types B en C) en met hethumane immunodeficieumlntie virus (HIV) als gevolgvan een accidenteel contact met bloed van eenpositieve patieumlnt Net als voor ander personeel uit hetoperatiekwartier worden uit de literatuur geenbesmettingen met cytomegalovirus parvovirus B19of retrovirus van een ander type dan HIVgerapporteerd De overdracht van andereviruspartikels lijkt mogelijk via rookontwikkeling bijgebruik van Laserapparatuur (Deze vorm vanbesmetting werd trouwens bevestigd door klinischestudies en door laboratoriumonderzoek Zo heeftmen kunnen aantonen dat er viruspartikels in de rookovergingen bij het wegbranden van condylomenlaryngale papillomen en van wratten) (20) Eenaccidentele microbieumlle besmetting met inbegrip vantuberculose is uitzonderlijk binnen de ruimte van hetoperatiekwartier In Frankrijk is er tot op heden geenbesmetting gekend veroorzaakt door nietconventionele overdraagbare pathogenen of doorprionen Wat de accidentele blootstelling met bloedbetreft is het werk van NELSING uit 1995 de enigestudie die handelt over de omstandigheden vanpercutane blootstelling die gerelateerd is met deanesthesie Hierin wordt het verband aangetoondtussen enerzijds het niet naleven van de universelevoorzorgsmaatregelen en anderzijds volgendefactoren onoplettendheid (41 ) ophalen van hetmaterieel (18 ) recapping van de naalden (14 )verkeerd plaatsen van de catheter (23 )inspuitingen (25 ) arterieumlle punctie (11 )veneuze punctie (8 ) spoedhandelingen (16 ) enonverwachte reacties van de patieumlnt (14 ) Deomstandigheden zijn vergelijkbaar met deze op een
het optreden van kruisbesmettingen tevoorkomen door toepassing van een strengdoorgedreven handhygieumlne het wassen (volgensde voorschriften met een zachte- of ontsmettendezeep) handontsmetting door wrijving (met eenalcoholische oplossing) vooral in de operatiezaalof in een noodsituatie en tenslotte het doordachtgebruik van handschoenen Men dient de handente schrobben en te desinfecteren op chirurgischewijze bij elke invasieve handeling die in verbandgebracht worden met chirurgie het plaatsen vaneen epidurale catheter centrale catheterisatiearterieumlle catheterisatie
bull Men dient de universele voorzorgsmaatregelen toete passen op alle patieumlnten
bull Men dient te werken op gereinigd en ontsmetteoppervlakten Dit dient te geschieden volgens deaanbevolen reinigingstechnieken en met eenfrequentie aangepast aan de verschillendeogenblikken van activiteit
bull Het werk dient te geschieden met onderlegdgevormd gemotiveerd en gecontroleerdpersoneel
Aanbevelingen voor het plaatsen van cathetersbereiding en gebruik van anestheticabull Men dient bij het plaatsen van catheters
(vasculaire ruggenmerg) de regels van dehuidontsmetting in acht te nemen wassen met eenontsmettende zeep spoelen (af)drogen en gebruikmaken van een ontsmettingsmiddel (van dezelfdesoort als de zeep) vanuit het middelste gedeeltenaar de periferie toe Niet afscheren met eenscheermes indien nodig verkiest men het epilerenof scheren met een scheerapparaat
bull Men trekt een steriele overjas aan bij de plaatsingvan een centraal veneuze catheter Dit geldteveneens bij de plaatsing van een catheter voorloco-regionale anesthesie
bull Men dient steriliteitregels in acht te nemen voor deontsmetting van flacondoppen voor perfusie ofanesthetica Dit geldt trouwens ook voor demanipulatie van driewegkranen
bull Men dient elke vorm van loco-regionaleanesthesie te vermijden in geval vanveralgemeende en bewezen sepsis en bij deaanwezigheid van infectieuze huidletsels terhoogte van de punctieplaatsMen dient de injectiespuiten tussen tweeopeenvolgende patieumlnten helemaal te vervangen(zelfs als de toediening van de anesthetica gebeurtvia een pompsysteem Dit geldt trouwens ookvoor de verlengleidingen) Het is niet voldoendevan enkel de naalden of een onderdeel van de
spuit te vervangen Indien de anesthetica viaperfusie toegediend worden dient men voor elkepatieumlnt zowel de perfusieleiding als de perfusiefleste vervangen
Aanbevelingen voor de behandeling van medischehulpmiddelenbull Het wegwerp materieel mag niet opnieuw
gebruikt wordenbull Voor anesthesie dient men enkel gebruik te maken
van gedecontamineerd en gereinigd materieelVervolgens dient men de benodigdheden teontsmetten of te steriliseren volgens devoorgeschreven procedure voor medischmaterieel in functie van aard en categorie van hetmateriaal
bull Om de kans ARI minimaal te houden dient mentijdens de verzorging de richtlijnen op te volgendie handelen over het contact van medischehulpmiddelen met weefsel met een verhoogdbesmettingsrisico door NCOP (omzendbriefDGS5CDHOSE22001138 van 14 maart 2001)
bull Men dient bij elke patieumlnt gebruik te maken vaneen antibacterieumlle- en antivirale filter die geplaatstwordt op het Y-vormig tussenstuk Dit is nodig omhet potentieumlle risico op kruisbesmetting tevoorkomen en ook om het beheer van devervanging van de anesthesiecircuits teverbeteren
Specifieke aanbevelingenbull Men dient de richtlijnen die toegepast worden
voor de andere vormen van nosocomiale infectiesin acht te nemen
bull Men dient isolatietechnieken verder toe te passenbij dragers van multiresistente kiemen inhoofdzaak door de voorzorgen bij het contact inacht te nemenPatieumlnten met tuberculose of verdacht vantuberculose dienen in isolatie beademd teworden
Aanbevelingen voor verblijf op de dagrecoverybull Men dient de richtlijnen die van toepassing zijn
voor de dagrecovery en die betrekking hebben opde situering (gelegen binnen of buiten hetoperatiekwartier) zodanig toe te passen dat hetrechtstreeks verkeer van zowel patieumlnten alspersoneel tussen het operatiekwartier en deverpleegeenheid vermeden wordt
bull Met dient er voor te zorgen dat er op dedagrecovery voldoende watervoorzieningspuntenbeschikbaar zijn maar voldoende verwijderd vanelke plaats waar zorgen toegediend worden om
N O S O - i n f o v o l V I n deg 1 2 0 0 2
6
besmettingen door aeumlrosolvorming te voorkomenbull Men dient de dagrecovery volgens dezelfde
procedures te onderhouden als de operatiezaalHet is echter niet aangewezen om het materieel tereinigen binnen de ruimte van de dagrecovery
Besluit
Het multifactorieel karakter van infecties bij degeopereerde patieumlnt stelt dat alle bewezenmaatregelen op het vlak van chirurgie en anesthesiemoet worden gevolgd (22-24) Wat deze laatstebetreft verklaart de moeilijkheid van een becijferderelatie tussen de ARI enerzijds en de gangbarepraktijken in de anesthesie anderzijds (25) demiskenning van het probleem door hetanesthesiepersoneelEen toepassing van de aanbevelingen gebeurt inverschillende stappen Deze houden in dat men eenpoging doet om kwalitatief betere zorgen toe tedienen Tijdens de opleiding van medisch enparamedisch personeel voor anesthesie wordt hetbesmettingsrisico binnen het operatiekwartierherkend en past men past preventieve maatregelentoe op basis van gevalideerde criteria volgensbeschreven procedures gevolgd door toezicht van deinfectiewaarden Daarna zal een audit vanberoepsmensen de toepassing van deze maatregelenevalueren Een optimale werkorganisatie binnen elkoperatiekwartier toepasselijk op vlak vanwerkbelasting en beschikbare middelen en geldendvoor zowel personeel als materieel is een onmisbaarelement voor het welslagen van deze betrachtingen
Bibliographie
1 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONLa pratique de lrsquoanestheacutesie en France en 1996 Ann Fr AnesthReacuteanim 1998 18 1299-13872 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONRecommandations concernant lrsquohygiegravene en anestheacutesie 1997 22pages3 CENTRE DE COORDINATION DE LA LUTTE CONTRE LESINFECTIONS NOSOCOMIALES DU SUD-EST Guide des bonnespratiques drsquohygiegravene en anestheacutesie Lyon 1996 64 pages4 AMERICAN SOCIETY OF ANESTHESIOLOGISTS Recommen-dations for infection control for the practice of anesthesiologyPark Ridge Illinois 1994 33 pages5 ASSOCIATION OF OPERATING ROOM NURSES Recommen-ded pratices Cleaning and processing anesthesia equipmentAORN J 1991 53 775-7776 OLDS JW KISCH AL EBERLE BJ WILSON JN Pseudomonasaeruginosa respiratory tract infection acquired from a contamina-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
7
ted anesthesia machine Am Rev Respir Dis 1972 105 628-6327 BENNET SN MCNEIL MM BLAND LA ARDUINO MJ VILLA-RINO ME PERROTTA DM Postoperative infections traced tocontamination of an intravenous anesthetic propofol N Engl JMed 1995 333 147-1548 HERWALDT LA POTTINGER J COFFIN SA Nosocomial infec-tions associated with anesthesia In Mayhall CG Ed Hospital epi-demiology and infection control Williams and Wilkins Balti-more 1996 655-6759 GORCE P De Abreu L PANNETIER C Evaluation du risqueinfectieux nosocomial lieacute agrave lrsquoanestheacutesie Abstract R240 37eCongregraves National de la Socieacuteteacute Franccedilaise drsquoAnestheacutesie et deReacuteanimation Paris 199510 HAJJAR J GIRARD R Surveillance des infections nosoco-miales lieacutees agrave lrsquoanestheacutesie Etude multicentrique Ann Fr AnesthReacuteanim 2000 1 47-5311 CHANT K KOCIUBA K MUNRO R CRONE S KEBRIDGE RQUIN J Investigation of possible patient-to-patient transmissionof hepatitis C in a hospital New South Wales Public Health Bul-letin 1994 5 47-5112 HAJJAR J HERNIGOU E GOUIN F Entretien et deacutesinfectiondu mateacuteriel neacutecessaire au controcircle des voies aeacuteriennes et agrave la ven-tilation meacutecanique Ann Fr Anesth Reacuteanim 1998 17 403-40713 MEFFRE C GIRARD R HAJJAR J Le risque de colonisationapregraves pose de catheacuteters veineux peacuteripheacuteriques est-il modifieacute selonlrsquoantiseptique utiliseacute lorsqursquoon applique un protocole en 4 temps HygiegraveneS 1995 9 4514 TREPANIER CA LESSARD MR BROCHU JG DENAULT PHRisk of cross-infection related to multiple use of disposablesyringes Can J Anaesth 1990 37 156-15915 ANONYME Changer drsquoaiguille et pas de seringue une pra-tique dangereuse BEH 1988 1 1-216 WEDEL DJ HERLOCKER TT Risks of regional anesthesia-infectious septic Reg Anesthes 1996 21(6) 57-6117 AUBOYER C Risque infectieux et anestheacutesie loco-reacutegionaleAnn Fr Anesth Reacuteanim 1998 17 1257-126018 MARSAUDON E BERTHIER F Meacuteningite agrave Staphylococcusaureus apregraves anestheacutesie peacuteridurale obsteacutetricale Ann Fr AnesthReacuteanim 1996 15 389-39019 HOLT HM ANDERSON SS ANDERSON O GARHN-HAN-SEN B SIBONI K Infection following epidural catheterization JHosp Infect 1995 30 253-26020 GARDEN JM OrsquoBANNION MK SHELNITZ LS ET AL Papil-loma virus in the vapor of carbon dioxide Laser-treated verrucaeJAMA 1988 8 1199-120221 LOT F DE BENOIST AC ABITEBOUL D Infections profes-sionnelles par le VIH en France chez le personnel de santeacute Lepoint au 30 juin 1998 BEH 1999 18 69-7022 BIMAR MC HAJJAR J POTTECHER B Risque infectieux noso-comial en anestheacutesie Recommandations geacuteneacuterales Ann fr AnesthReacuteanim 1998 17 392-40223 KORINEK AM Recommandations pour la pose des abordsvasculaires au bloc opeacuteratoire Voies veineuses et voies arteacuteriellespeacuteripheacuteriques Ann Fr Anesth Reacuteanim 1998 17 1250-125224 VEBER B Manipulation des agents anestheacutesiques et desseringues Recommandations et argumentations Ann Fr AnesthReacuteanim 1998 17 1253-125625 TAIT AR TUTTLE DB Preventing perioperative transmissionof infection a survey of anesthesiology practice Anesth Analg1995 80 764-769
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
N O S O - i n f o v o l V I n deg 1 2 0 0 2
2
Epidemiologie en preventie van nosocomiale infecties gerelateerdaan anesthesieJ Hajjar Eidlin ndash HC Valence
De enquecircte die door de Franse Vereniging voor Anesthesieen Reanimatie in 1966 werd uitgevoerd schat het aantalanesthesies op acht miljoen per jaar In 75 van degevallen was dit in Frankrijk naar aanleiding van eenchirurgische ingreep (1) De post-operatieve wondinfectie(POWI) is de meest voorkomende complicatie in dechirurgie maar de geopereerde patieumlnt loopt anderzijdsook nog het risico van infectie op afstand van deoperatiewonde Tot deze laatste categorie behoren de ARIIn beide gevallen bestaan er meerdere factoren die hetoptreden ervan bevorderen Hoewel men thans deepidemiologie van de POWI goed kent (de incidentiewordt gemiddeld op 3 geschat alle soorten chirurgischeingrepen dooreen genomen) is de kennis over de ARI vanrecentere datum Het peri-operatieve gebeuren houdttevens voor zowel het chirurgisch als het anesthesieteameen potentieel risico in op besmetting metbloedoverdraagbare pathogenen Dit risico is uiteraardafhankelijk van de frequentie van de accidentieleblootstelling aan bloed Een betere inschatting van degevaren op ARI heeft het mogelijk gemaakt om specifiekerichtlijnen op te stellen De toepassing van deze richtlijnenis onmisbaar voor een doeltreffende preventie vaninfecties bij patieumlnten die een heelkundige ingreep moetenondergaan (2-5)
Epidemiologie van nosocomiale infecties als gevolg vande anesthesie
FrequentieVroeger kwamen de ARI voornamelijk als secundaire
epidemieeumln voor Deze werden veroorzaakt door hetgebruik van slecht gedesinfecteerde anesthesie circuitsdoor injectie van anesthetica uit besmette multidosisflacons of door het gebruik van spuiten die reeds langerdan 24 uur op voorhand waren klaargemaakt (67)
Aangezien de moleculaire typeringstechnieken op hetmoment van die publicaties nog niet bestonden dient mentoch voor enkele gevallen voorzichtig te zijn bij hettrekken van conclusies Met uitzondering van epidemischetoestanden waren de meeste enquecirctes retrospectief envaak tendentieus op vlak van de methodiek (8) Anderzijdshadden de prospectieve enquecirctes vooral betrekking op deepidurale verdovingIn een eerste prospectieve studie uitgevoerd op 400patieumlnten over een termijn van 10 maanden bedroeg deincidentie van infecties 15 bedroeg (deze infectieswerden microbiologisch gedocumenteerd) (9) Een recenteprospectieve multicenterstudie uitgevoerd op 7300patieumlnten uit 13 deelnemende instellingen kwam tot eenincidentie van 34 op 1000 anesthesies (10) Van de 7300patieumlnten werden er 25 geiumlnfecteerd (bij 9 was devasculaire kateter besmet 12 werden besmet via hetbeademingstoestel en bij 4 werd het oog en de mondholtegeiumlnfecteerd) Enkel de patieumlnten onderworpen aan eenanesthesie die langer duurde dan 2 uur of die eenbloedtransfusie kregen hadden een hogere incidentieDeze globale incidentie lijkt op het eerste gezicht laagmen dient dit echter in perspectief te brengen met hetenorm aantal ingrepen met anesthesie die jaarlijks inFrankrijk plaatshebben
ORIGINELE ARTIKEL
Hieronder geven wij U een origineel bericht weer dit metde toelating van de hoofdredakteur Dr J Fabry van Dr JHajjar anesthesist en nu ook overtuigd van de preventievan nosocomiale infecties
Dit artikel gepubliceerd in het blad HYGIENE (officieelblad van de franse instelling Klinische Hygieumlne) 2001 IXnr 5 spreekt over de niet dikwijls aangehaaldenosocomiale infecties bij anesthesie
AbstractPatieumlnten die een operatie hebben ondergaan zijn vatbaar voortwee types van nosocomiale infecties Enerzijds zijn er debesmettingen op de plaats van de ingreep en anderzijds zijn er deinfecties die zich situeren op afstand van de operatiewonde Totdeze laatste soort behoren de anesthesie gerelateerde infecties(ARI = Anesthaesia related infections) Een beter inzicht over hetaantal de plaats en de risicofactoren van de ARI hebben deanesthesisten doen beseffen dat er wel degelijk een probleembestaat Ondanks de geringe incidentie is het gezien het hogeaantal jaarlijks uitgevoerde anesthesies noodzakelijk om de doorde specialisten aanbevolen richtlijnen toe te passenSleutelwoorden Anesthesie ndash Nosocomiale infecties ndashPreventieve maatregelen ndash Voorschriften
Epidemiology and prevention of nosocomial infectionsassociated with anaesthesiaSummarySurgical patients are susceptible to two types of nosocomialinfections surgical site infections and distant infections such asthose associated with anaesthesia (IAA) Better knowledge of therates sites and risk factors of IAA allow anaesthesia teams to beconscious of the problem Despite a low incidence rate the highnumber of anaesthesias performed each year necessitates theimplementation of recommendations stipulated by professionalsof this specialty
Key-Words Anaesthestia ndash Cross infections ndash Prevention ndashGuidelines
Voornaamste soorten infecties en risicofactoren
Infecties ontstaan door gebruik van materieel gebruikt tercontrole van de luchtwegen en voor mechanischeventilatieHet materieel dat men gebruikt voor controle van deluchtwegen en voor mechanische ventilatie komt incontact met normale flora uit de slijmvliezen van debovenste luchtwegen en spijsvertering Het gaat hier meerbepaald om speeksel en tracheabronchiale secreties diesoms ook bloed kunnen bevatten Dit materieel omvatenerzijds de benodigdheden voor manuele ventilatie(maskers ventielen extremiteiten van de laryngoscopenendotracheale tubes enz) alsook de apparatuur voormechanische ventilatie (externe- en interne leidingen vande beademingstoestellen luchtbevochtigers enz) Eendeel van dit materieel heeft specifieke risicofactoren dieverband houden met de contaminatie door de amandelen(intrusie met ulceraties of contact van meer dan eacuteeacuten uur)en equivalente weefsels rond het scheidingsvlak tussenluchtwegen en spijsvertering Deze beschouwt men alsweefsels met verhoogd besmettingsgevaar voor nietconventioneel overdraagbare pathogenen (NCOP)Onaangepaste of ontoereikende manipulatie van ditmaterieel (al of niet met betrekking tot NCOP) enhandelingen door het verplegend personeel tijdens hetverstrekken van zorgen (intubatie extubatie aspiratie)kunnen aan de basis liggen van kruisbesmettingen metpathogenen Deze kunnen al of niet behoren tot denormale flora van de luchtwegen zoals weergegeven ineen publicatie waarbij men de transmissie van Hepatitis Cvirus heeft vastgesteld bij twee op elkaar volgendepatieumlnten via een beademingscircuit zonderantimicrobieumlle filter en zonder vervanging ervan tussen depatieumlnten (11)Dergelijke toestanden hebben het reeds verschillendejaren durende debat over de implicaties van de anesthesiecircuits omgebogen Deze kunnen een rol spelen in deoverdracht van micro-organismen infecties doen ontstaanen een gevaar betekenen voor kruisbesmettingen (in hetbijzonder met virussen) (12) Dit risico is voor vele auteursontegensprekelijk het bewijs wordt enerzijds geleverddoor de positiviteit van bacteriologische stalen afgenomentijdens het routinewerk en anderzijds door in vitro studiesMaar voor anderen vormen de leidingen zelfs al zijn zebesmet geen bron van besmetting Dit komt doordatgezien de ongunstige factoren voor ontwikkeling vanbacterieumln er geen significante hoeveelheid micro-organismen overgedragen wordtHet optreden van postoperatieve pneumopathieeumln vormthet meest gebruikte beoordelingscriterium uit studies overde rol van de anesthesie circuits Dit criterium is moeilijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
3
te hanteren om het risico van kruisbesmetting in teschatten Het is inderdaad een feit dat elke initieumllebijbesmetting van de anesthesie uitrusting buitenbeschouwing gelaten er tijdens de kunstmatigebeademing enkele erg belangrijke factoren aan de basiskunnen liggen van postoperatieve pneumopathieeumln Dezefactoren zijn een kortsluiting van de bovenste luchtwegendoor de endotracheale tube het gebruik van anestheticadoor inhalatie evenals de toediening van verdovendemedicatie die de ciliaire activiteit van het bronchialeepithelium onderdrukken en tenslotte de verspreiding vande normale pharyngiale flora naar de tracheaDe respiratoire antecedenten van de patieumlnt en het typevan heelkundige ingreep vormen de andere risicofactoren
Infecties gerelateerd met invasieve handelingen
Zowel de plaatsing van vasculaire catheters de cathetersvoor loco- regionale anesthesie als de intraveneuzemanipulatie van anesthetica kunnen infecties veroorzakenals de steriliteitregels niet in acht genomen wordenbull Omtrent de perifeer veneuze catheters De meeste
risicohoudende situaties worden enerzijds bepaalddoor de kwaliteit van de huidontsmetting op hetmoment van de catheterplaatsing en anderzijds detijdsduur van de catheterisatie De resultaten van eenstudie over catheters die in het operatiekwartierwerden geplaatst confirmeren deze bevindingen erwerd kolonisatie vastgesteld bij 31 van de 1138perifeer veneuze catheters Een antiseptischehuidbehandeling in vier fasen op het moment van deplaatsing (huidreiniging met een antiseptische zeepspoelen drogen en de toepassing van eenontsmettingsmiddel verenigbaar met de zeep)gekoppeld aan een plaatsingsduur van minder dan 72uur verklaart het erg laag kolonisatiecijfer (27) (13)In hoger genoemde studie was er 1 infectie op 1000operaties als gevolg van de aanwezigheid van eenperifeer veneuze catheter Alhoewel het verschilstatistisch niet significant is constateerde men slechtseacuteeacuten enkele perifeer veneuze catheterbesmetting opeacuteeacuten van de zes verpleegeenheden die de antiseptischehuidreiniging in vier fasen toepasten In vergelijkingdaarmee werden er vier besmettingen gerapporteerdop negen afdelingen die deze reinigingsprocedure niettoepasten (10) Hoewel het besmettingsgevaar op heteerste gezicht gering lijkt moet men toch aandachthebben voor de frequentie van de manipulaties Menmoet steeds voor ogen houden hoe ernstig de gevolgenkunnen zijn van een eventuele infectie bij een patieumlntmet een endovasculaire prothese
N O S O - i n f o v o l V I n deg 1 2 0 0 2
4
Tabel I Epidemische gevallen veroorzaakt door toediening van een injectie met een inspuitbaar anestheticum en doorintravasculaire procedures (volgens HERWALDT) (6)
Auteur (jaar)
Sack (1970)
Siboni (1979)
Maldonaldo (1989)
CDC (1990)
CDC (1990)
CDC (1990)
CDC (1990)
Maxi (1991)
Froggatt (1991)
Rudnick (1991)
Bron
Dezelfde IV oplossing voormeerdere patieumlnten
Fentanyl
Lidocaine(multidosis flacon)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Fentanyl(injectiespuit
vooraf gevuld)
Injectiespuitgemeenschappelijk voor
meerdere patieumlnten
Vooraf samengestelde arterieumlle drukset
Infectie
Bacteriemie
Bacteriemie
Hepatitis
Endophtalmie
Koorts
Bacteriemie
KoortsPostoperatieve wondinfectie
BacteriemiePosoperatieve wondinfectie
Hepatitis
Bacteriemie
Patieumlntsen (aantal)
5
16
5
4
2
13
8
3
6
9
Pathogene kiem
K pneumoniae
P cepacia
Virus heacutepatite B
C albicans
Moraxella
S aureus
S aureus
P picketti
Virus heacutepatite B
P aeruginosa
bull In de literatuur zijn reeds verschillende publicatiesverschenen over epidemieeumln veroorzaakt doorbacterieumln of schimmels (Tabel1) (8) Deze wordenin verband gebracht met de extrinsieke besmettingvan anesthetica door omgevingskiemen tijdensbereiding en manipulatie van de preparatenPROPOFOL is het meest onderhevig aanbijbesmetting aangezien het een olieachtigevloeistof is zonder conserveermiddel nochbacterieremmend product Daardoor wordt deontwikkeling van micro-organismen in de handgewerkt met als bijkomende risicofactor dat hetvooraf bereide preparaat langzaam via perfusiewordt toegediend Maar andere preparaten zoalsFENATYL of LIDOCAIumlNE worden evenzeer alsmogelijke bron van bijbesmetting gezien als eenzelfde oplossing wordt toegediend aanverschillende patieumlnten Het gebruik van dezelfdeinjectiespuit bij verschillende patieumlnten is de
oorzaak van besmettingen met Hepatitis B viruszelfs wanneer de injectienaalden vervangen zijnVerschillende studies hebben reeds de gevaren vandergelijke onaanvaardbare praktijken aangetoond(1415)
bull Hoewel secundaire besmettingen bij loco-regionale anesthesie potentieel ernstig kunnen zijnis de incidentie ervan niet precies gekend (1617)De waarden die men terugvindt hebben meestalbetrekking op epidurale verdoving bij bevallingenen varieumlren nogal sterk van 008 tot 00002 Inde literatuur worden op 28 infectieuzecomplicaties 21 gevallen beschreven metepidurale abcessen 6 met meningitis en eacuteeacuten gevalmet spondylitis (18) Als men de verwikkelingen bijrachianesthesie beschouwt rapporteren er zevenstudies vier gevallen van meningitis op een totaalvan 90000 patieumlnten een besmettingcijfer van
verpleegeenheid Men kan drie risicomomentenonderscheiden met name het toepassen van invasievetechnieken het ophalen van afval en het onderhoudvan bevuild materieel Het risico van seroconversie isafhankelijk van reeds hoger vernoemde factoren hetaantal infecties bij de patieumlnten en zodoende deprevalentie in de populatie het chronischedragerschap van virussen in het bloed van debesmette personen de kwantiteit en virulentie van hetinfectieus organisme en de aard van de accidenteleblootstelling (percutane verwonding door een prikinsnijding of contact met huid of slijmvlies) Devoornaamste factoren die tot een seroconversie leidenzijn eveneens gekend een diepe prikwonde door eenmet bloed besmette holle naald of een wonde metmaterieel dat gebruikt werd voor een vasculaireingreep bij een patieumlnt met een hoge antivirus titerHet niet dragen van handschoenen is daarbij eensupplementaire risicofactor Het professionelebesmettingsgevaar wordt door het personeel meestalhoger ingeschat voor HIV en meestal onderschat voorHBV Dit wordt aangetoond uit de resultaten van eenrondvraag die in 1995 werd ondernomen bij 300verpleegkundigen uit de anesthesie afdeling Metbetrekking tot HIV werd het risico door 18 vandeze verpleegkundigen geschat op groter dan of gelijkaan 30 (amper 29 hadden het cijfer juist) voorHBV werd door 30 gedacht dat het risico kleinerdan of gelijk was aan 03 (amper 21 hadden hetcijfer juist) Uit de groep van 42 professionele HIV-infecties die op 30 juni 1998 gerecenseerd werdenbetrof het in twee gevallen een anesthesist -reanimator op een totaal van 29 vermoede infecties(21)
Preventieve maatregelen en strategie bij hetimplementeren
De preventieve maatregelen die in 1997 door deFranse Vereniging voor Anesthesie en Reanimatiegepubliceerd werden zijn hoofdzakelijk toegespitstop de controle op exogene reservoirs en hetvoorkomen van overdracht (2)
Algemene aanbevelingenbull Men dient te beschikken over geschikte kledij en
een algemeen gedragspatroon vertonen passendbij het operatiekwartier Vooraleer de operatiezaalte betreden en gedurende de ganse duur van deingreep dient men op een correcte manier eenmasker te dragen en een passend haarbedekkendhoofddeksel aan te hebben Men dient deverplaatsingen minimaal te houden
bull Men dient de kiemoverdracht via de handen en
N O S O - i n f o v o l V I n deg 1 2 0 0 2
5
00045 In vergelijking met de risicofactoren bijvasculaire catheters is het waarschijnlijk dat destaat van de huid rond de insteekplaats deplaatsingsduur van de catheter en de frequentievan het herinspuiten zoveel factoren meer zijn diehet besmettingsrisico verhogen (19)
Het is belangrijk zich te herinneren dat hetzenuwstelsel (met inbegrip van het hersenvlies encerebrospinaal vocht) bijzonder gevoelig is voorbesmettingen veroorzaakt door niet conventioneleoverdraagbare pathogenen Het materieel datgebruikt wordt voor loco- regionale anesthesieschept de mogelijkheid van overdracht met dezekiemen
De professionele besmettingrisicorsquosHet gevaar van professionele besmetting bij hetanesthesiepersoneel wordt in hoofdzaak gevormddoor eventueel contact met de hepatitis virussen(meer in het bijzonder de types B en C) en met hethumane immunodeficieumlntie virus (HIV) als gevolgvan een accidenteel contact met bloed van eenpositieve patieumlnt Net als voor ander personeel uit hetoperatiekwartier worden uit de literatuur geenbesmettingen met cytomegalovirus parvovirus B19of retrovirus van een ander type dan HIVgerapporteerd De overdracht van andereviruspartikels lijkt mogelijk via rookontwikkeling bijgebruik van Laserapparatuur (Deze vorm vanbesmetting werd trouwens bevestigd door klinischestudies en door laboratoriumonderzoek Zo heeftmen kunnen aantonen dat er viruspartikels in de rookovergingen bij het wegbranden van condylomenlaryngale papillomen en van wratten) (20) Eenaccidentele microbieumlle besmetting met inbegrip vantuberculose is uitzonderlijk binnen de ruimte van hetoperatiekwartier In Frankrijk is er tot op heden geenbesmetting gekend veroorzaakt door nietconventionele overdraagbare pathogenen of doorprionen Wat de accidentele blootstelling met bloedbetreft is het werk van NELSING uit 1995 de enigestudie die handelt over de omstandigheden vanpercutane blootstelling die gerelateerd is met deanesthesie Hierin wordt het verband aangetoondtussen enerzijds het niet naleven van de universelevoorzorgsmaatregelen en anderzijds volgendefactoren onoplettendheid (41 ) ophalen van hetmaterieel (18 ) recapping van de naalden (14 )verkeerd plaatsen van de catheter (23 )inspuitingen (25 ) arterieumlle punctie (11 )veneuze punctie (8 ) spoedhandelingen (16 ) enonverwachte reacties van de patieumlnt (14 ) Deomstandigheden zijn vergelijkbaar met deze op een
het optreden van kruisbesmettingen tevoorkomen door toepassing van een strengdoorgedreven handhygieumlne het wassen (volgensde voorschriften met een zachte- of ontsmettendezeep) handontsmetting door wrijving (met eenalcoholische oplossing) vooral in de operatiezaalof in een noodsituatie en tenslotte het doordachtgebruik van handschoenen Men dient de handente schrobben en te desinfecteren op chirurgischewijze bij elke invasieve handeling die in verbandgebracht worden met chirurgie het plaatsen vaneen epidurale catheter centrale catheterisatiearterieumlle catheterisatie
bull Men dient de universele voorzorgsmaatregelen toete passen op alle patieumlnten
bull Men dient te werken op gereinigd en ontsmetteoppervlakten Dit dient te geschieden volgens deaanbevolen reinigingstechnieken en met eenfrequentie aangepast aan de verschillendeogenblikken van activiteit
bull Het werk dient te geschieden met onderlegdgevormd gemotiveerd en gecontroleerdpersoneel
Aanbevelingen voor het plaatsen van cathetersbereiding en gebruik van anestheticabull Men dient bij het plaatsen van catheters
(vasculaire ruggenmerg) de regels van dehuidontsmetting in acht te nemen wassen met eenontsmettende zeep spoelen (af)drogen en gebruikmaken van een ontsmettingsmiddel (van dezelfdesoort als de zeep) vanuit het middelste gedeeltenaar de periferie toe Niet afscheren met eenscheermes indien nodig verkiest men het epilerenof scheren met een scheerapparaat
bull Men trekt een steriele overjas aan bij de plaatsingvan een centraal veneuze catheter Dit geldteveneens bij de plaatsing van een catheter voorloco-regionale anesthesie
bull Men dient steriliteitregels in acht te nemen voor deontsmetting van flacondoppen voor perfusie ofanesthetica Dit geldt trouwens ook voor demanipulatie van driewegkranen
bull Men dient elke vorm van loco-regionaleanesthesie te vermijden in geval vanveralgemeende en bewezen sepsis en bij deaanwezigheid van infectieuze huidletsels terhoogte van de punctieplaatsMen dient de injectiespuiten tussen tweeopeenvolgende patieumlnten helemaal te vervangen(zelfs als de toediening van de anesthetica gebeurtvia een pompsysteem Dit geldt trouwens ookvoor de verlengleidingen) Het is niet voldoendevan enkel de naalden of een onderdeel van de
spuit te vervangen Indien de anesthetica viaperfusie toegediend worden dient men voor elkepatieumlnt zowel de perfusieleiding als de perfusiefleste vervangen
Aanbevelingen voor de behandeling van medischehulpmiddelenbull Het wegwerp materieel mag niet opnieuw
gebruikt wordenbull Voor anesthesie dient men enkel gebruik te maken
van gedecontamineerd en gereinigd materieelVervolgens dient men de benodigdheden teontsmetten of te steriliseren volgens devoorgeschreven procedure voor medischmaterieel in functie van aard en categorie van hetmateriaal
bull Om de kans ARI minimaal te houden dient mentijdens de verzorging de richtlijnen op te volgendie handelen over het contact van medischehulpmiddelen met weefsel met een verhoogdbesmettingsrisico door NCOP (omzendbriefDGS5CDHOSE22001138 van 14 maart 2001)
bull Men dient bij elke patieumlnt gebruik te maken vaneen antibacterieumlle- en antivirale filter die geplaatstwordt op het Y-vormig tussenstuk Dit is nodig omhet potentieumlle risico op kruisbesmetting tevoorkomen en ook om het beheer van devervanging van de anesthesiecircuits teverbeteren
Specifieke aanbevelingenbull Men dient de richtlijnen die toegepast worden
voor de andere vormen van nosocomiale infectiesin acht te nemen
bull Men dient isolatietechnieken verder toe te passenbij dragers van multiresistente kiemen inhoofdzaak door de voorzorgen bij het contact inacht te nemenPatieumlnten met tuberculose of verdacht vantuberculose dienen in isolatie beademd teworden
Aanbevelingen voor verblijf op de dagrecoverybull Men dient de richtlijnen die van toepassing zijn
voor de dagrecovery en die betrekking hebben opde situering (gelegen binnen of buiten hetoperatiekwartier) zodanig toe te passen dat hetrechtstreeks verkeer van zowel patieumlnten alspersoneel tussen het operatiekwartier en deverpleegeenheid vermeden wordt
bull Met dient er voor te zorgen dat er op dedagrecovery voldoende watervoorzieningspuntenbeschikbaar zijn maar voldoende verwijderd vanelke plaats waar zorgen toegediend worden om
N O S O - i n f o v o l V I n deg 1 2 0 0 2
6
besmettingen door aeumlrosolvorming te voorkomenbull Men dient de dagrecovery volgens dezelfde
procedures te onderhouden als de operatiezaalHet is echter niet aangewezen om het materieel tereinigen binnen de ruimte van de dagrecovery
Besluit
Het multifactorieel karakter van infecties bij degeopereerde patieumlnt stelt dat alle bewezenmaatregelen op het vlak van chirurgie en anesthesiemoet worden gevolgd (22-24) Wat deze laatstebetreft verklaart de moeilijkheid van een becijferderelatie tussen de ARI enerzijds en de gangbarepraktijken in de anesthesie anderzijds (25) demiskenning van het probleem door hetanesthesiepersoneelEen toepassing van de aanbevelingen gebeurt inverschillende stappen Deze houden in dat men eenpoging doet om kwalitatief betere zorgen toe tedienen Tijdens de opleiding van medisch enparamedisch personeel voor anesthesie wordt hetbesmettingsrisico binnen het operatiekwartierherkend en past men past preventieve maatregelentoe op basis van gevalideerde criteria volgensbeschreven procedures gevolgd door toezicht van deinfectiewaarden Daarna zal een audit vanberoepsmensen de toepassing van deze maatregelenevalueren Een optimale werkorganisatie binnen elkoperatiekwartier toepasselijk op vlak vanwerkbelasting en beschikbare middelen en geldendvoor zowel personeel als materieel is een onmisbaarelement voor het welslagen van deze betrachtingen
Bibliographie
1 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONLa pratique de lrsquoanestheacutesie en France en 1996 Ann Fr AnesthReacuteanim 1998 18 1299-13872 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONRecommandations concernant lrsquohygiegravene en anestheacutesie 1997 22pages3 CENTRE DE COORDINATION DE LA LUTTE CONTRE LESINFECTIONS NOSOCOMIALES DU SUD-EST Guide des bonnespratiques drsquohygiegravene en anestheacutesie Lyon 1996 64 pages4 AMERICAN SOCIETY OF ANESTHESIOLOGISTS Recommen-dations for infection control for the practice of anesthesiologyPark Ridge Illinois 1994 33 pages5 ASSOCIATION OF OPERATING ROOM NURSES Recommen-ded pratices Cleaning and processing anesthesia equipmentAORN J 1991 53 775-7776 OLDS JW KISCH AL EBERLE BJ WILSON JN Pseudomonasaeruginosa respiratory tract infection acquired from a contamina-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
7
ted anesthesia machine Am Rev Respir Dis 1972 105 628-6327 BENNET SN MCNEIL MM BLAND LA ARDUINO MJ VILLA-RINO ME PERROTTA DM Postoperative infections traced tocontamination of an intravenous anesthetic propofol N Engl JMed 1995 333 147-1548 HERWALDT LA POTTINGER J COFFIN SA Nosocomial infec-tions associated with anesthesia In Mayhall CG Ed Hospital epi-demiology and infection control Williams and Wilkins Balti-more 1996 655-6759 GORCE P De Abreu L PANNETIER C Evaluation du risqueinfectieux nosocomial lieacute agrave lrsquoanestheacutesie Abstract R240 37eCongregraves National de la Socieacuteteacute Franccedilaise drsquoAnestheacutesie et deReacuteanimation Paris 199510 HAJJAR J GIRARD R Surveillance des infections nosoco-miales lieacutees agrave lrsquoanestheacutesie Etude multicentrique Ann Fr AnesthReacuteanim 2000 1 47-5311 CHANT K KOCIUBA K MUNRO R CRONE S KEBRIDGE RQUIN J Investigation of possible patient-to-patient transmissionof hepatitis C in a hospital New South Wales Public Health Bul-letin 1994 5 47-5112 HAJJAR J HERNIGOU E GOUIN F Entretien et deacutesinfectiondu mateacuteriel neacutecessaire au controcircle des voies aeacuteriennes et agrave la ven-tilation meacutecanique Ann Fr Anesth Reacuteanim 1998 17 403-40713 MEFFRE C GIRARD R HAJJAR J Le risque de colonisationapregraves pose de catheacuteters veineux peacuteripheacuteriques est-il modifieacute selonlrsquoantiseptique utiliseacute lorsqursquoon applique un protocole en 4 temps HygiegraveneS 1995 9 4514 TREPANIER CA LESSARD MR BROCHU JG DENAULT PHRisk of cross-infection related to multiple use of disposablesyringes Can J Anaesth 1990 37 156-15915 ANONYME Changer drsquoaiguille et pas de seringue une pra-tique dangereuse BEH 1988 1 1-216 WEDEL DJ HERLOCKER TT Risks of regional anesthesia-infectious septic Reg Anesthes 1996 21(6) 57-6117 AUBOYER C Risque infectieux et anestheacutesie loco-reacutegionaleAnn Fr Anesth Reacuteanim 1998 17 1257-126018 MARSAUDON E BERTHIER F Meacuteningite agrave Staphylococcusaureus apregraves anestheacutesie peacuteridurale obsteacutetricale Ann Fr AnesthReacuteanim 1996 15 389-39019 HOLT HM ANDERSON SS ANDERSON O GARHN-HAN-SEN B SIBONI K Infection following epidural catheterization JHosp Infect 1995 30 253-26020 GARDEN JM OrsquoBANNION MK SHELNITZ LS ET AL Papil-loma virus in the vapor of carbon dioxide Laser-treated verrucaeJAMA 1988 8 1199-120221 LOT F DE BENOIST AC ABITEBOUL D Infections profes-sionnelles par le VIH en France chez le personnel de santeacute Lepoint au 30 juin 1998 BEH 1999 18 69-7022 BIMAR MC HAJJAR J POTTECHER B Risque infectieux noso-comial en anestheacutesie Recommandations geacuteneacuterales Ann fr AnesthReacuteanim 1998 17 392-40223 KORINEK AM Recommandations pour la pose des abordsvasculaires au bloc opeacuteratoire Voies veineuses et voies arteacuteriellespeacuteripheacuteriques Ann Fr Anesth Reacuteanim 1998 17 1250-125224 VEBER B Manipulation des agents anestheacutesiques et desseringues Recommandations et argumentations Ann Fr AnesthReacuteanim 1998 17 1253-125625 TAIT AR TUTTLE DB Preventing perioperative transmissionof infection a survey of anesthesiology practice Anesth Analg1995 80 764-769
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

Voornaamste soorten infecties en risicofactoren
Infecties ontstaan door gebruik van materieel gebruikt tercontrole van de luchtwegen en voor mechanischeventilatieHet materieel dat men gebruikt voor controle van deluchtwegen en voor mechanische ventilatie komt incontact met normale flora uit de slijmvliezen van debovenste luchtwegen en spijsvertering Het gaat hier meerbepaald om speeksel en tracheabronchiale secreties diesoms ook bloed kunnen bevatten Dit materieel omvatenerzijds de benodigdheden voor manuele ventilatie(maskers ventielen extremiteiten van de laryngoscopenendotracheale tubes enz) alsook de apparatuur voormechanische ventilatie (externe- en interne leidingen vande beademingstoestellen luchtbevochtigers enz) Eendeel van dit materieel heeft specifieke risicofactoren dieverband houden met de contaminatie door de amandelen(intrusie met ulceraties of contact van meer dan eacuteeacuten uur)en equivalente weefsels rond het scheidingsvlak tussenluchtwegen en spijsvertering Deze beschouwt men alsweefsels met verhoogd besmettingsgevaar voor nietconventioneel overdraagbare pathogenen (NCOP)Onaangepaste of ontoereikende manipulatie van ditmaterieel (al of niet met betrekking tot NCOP) enhandelingen door het verplegend personeel tijdens hetverstrekken van zorgen (intubatie extubatie aspiratie)kunnen aan de basis liggen van kruisbesmettingen metpathogenen Deze kunnen al of niet behoren tot denormale flora van de luchtwegen zoals weergegeven ineen publicatie waarbij men de transmissie van Hepatitis Cvirus heeft vastgesteld bij twee op elkaar volgendepatieumlnten via een beademingscircuit zonderantimicrobieumlle filter en zonder vervanging ervan tussen depatieumlnten (11)Dergelijke toestanden hebben het reeds verschillendejaren durende debat over de implicaties van de anesthesiecircuits omgebogen Deze kunnen een rol spelen in deoverdracht van micro-organismen infecties doen ontstaanen een gevaar betekenen voor kruisbesmettingen (in hetbijzonder met virussen) (12) Dit risico is voor vele auteursontegensprekelijk het bewijs wordt enerzijds geleverddoor de positiviteit van bacteriologische stalen afgenomentijdens het routinewerk en anderzijds door in vitro studiesMaar voor anderen vormen de leidingen zelfs al zijn zebesmet geen bron van besmetting Dit komt doordatgezien de ongunstige factoren voor ontwikkeling vanbacterieumln er geen significante hoeveelheid micro-organismen overgedragen wordtHet optreden van postoperatieve pneumopathieeumln vormthet meest gebruikte beoordelingscriterium uit studies overde rol van de anesthesie circuits Dit criterium is moeilijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
3
te hanteren om het risico van kruisbesmetting in teschatten Het is inderdaad een feit dat elke initieumllebijbesmetting van de anesthesie uitrusting buitenbeschouwing gelaten er tijdens de kunstmatigebeademing enkele erg belangrijke factoren aan de basiskunnen liggen van postoperatieve pneumopathieeumln Dezefactoren zijn een kortsluiting van de bovenste luchtwegendoor de endotracheale tube het gebruik van anestheticadoor inhalatie evenals de toediening van verdovendemedicatie die de ciliaire activiteit van het bronchialeepithelium onderdrukken en tenslotte de verspreiding vande normale pharyngiale flora naar de tracheaDe respiratoire antecedenten van de patieumlnt en het typevan heelkundige ingreep vormen de andere risicofactoren
Infecties gerelateerd met invasieve handelingen
Zowel de plaatsing van vasculaire catheters de cathetersvoor loco- regionale anesthesie als de intraveneuzemanipulatie van anesthetica kunnen infecties veroorzakenals de steriliteitregels niet in acht genomen wordenbull Omtrent de perifeer veneuze catheters De meeste
risicohoudende situaties worden enerzijds bepaalddoor de kwaliteit van de huidontsmetting op hetmoment van de catheterplaatsing en anderzijds detijdsduur van de catheterisatie De resultaten van eenstudie over catheters die in het operatiekwartierwerden geplaatst confirmeren deze bevindingen erwerd kolonisatie vastgesteld bij 31 van de 1138perifeer veneuze catheters Een antiseptischehuidbehandeling in vier fasen op het moment van deplaatsing (huidreiniging met een antiseptische zeepspoelen drogen en de toepassing van eenontsmettingsmiddel verenigbaar met de zeep)gekoppeld aan een plaatsingsduur van minder dan 72uur verklaart het erg laag kolonisatiecijfer (27) (13)In hoger genoemde studie was er 1 infectie op 1000operaties als gevolg van de aanwezigheid van eenperifeer veneuze catheter Alhoewel het verschilstatistisch niet significant is constateerde men slechtseacuteeacuten enkele perifeer veneuze catheterbesmetting opeacuteeacuten van de zes verpleegeenheden die de antiseptischehuidreiniging in vier fasen toepasten In vergelijkingdaarmee werden er vier besmettingen gerapporteerdop negen afdelingen die deze reinigingsprocedure niettoepasten (10) Hoewel het besmettingsgevaar op heteerste gezicht gering lijkt moet men toch aandachthebben voor de frequentie van de manipulaties Menmoet steeds voor ogen houden hoe ernstig de gevolgenkunnen zijn van een eventuele infectie bij een patieumlntmet een endovasculaire prothese
N O S O - i n f o v o l V I n deg 1 2 0 0 2
4
Tabel I Epidemische gevallen veroorzaakt door toediening van een injectie met een inspuitbaar anestheticum en doorintravasculaire procedures (volgens HERWALDT) (6)
Auteur (jaar)
Sack (1970)
Siboni (1979)
Maldonaldo (1989)
CDC (1990)
CDC (1990)
CDC (1990)
CDC (1990)
Maxi (1991)
Froggatt (1991)
Rudnick (1991)
Bron
Dezelfde IV oplossing voormeerdere patieumlnten
Fentanyl
Lidocaine(multidosis flacon)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Fentanyl(injectiespuit
vooraf gevuld)
Injectiespuitgemeenschappelijk voor
meerdere patieumlnten
Vooraf samengestelde arterieumlle drukset
Infectie
Bacteriemie
Bacteriemie
Hepatitis
Endophtalmie
Koorts
Bacteriemie
KoortsPostoperatieve wondinfectie
BacteriemiePosoperatieve wondinfectie
Hepatitis
Bacteriemie
Patieumlntsen (aantal)
5
16
5
4
2
13
8
3
6
9
Pathogene kiem
K pneumoniae
P cepacia
Virus heacutepatite B
C albicans
Moraxella
S aureus
S aureus
P picketti
Virus heacutepatite B
P aeruginosa
bull In de literatuur zijn reeds verschillende publicatiesverschenen over epidemieeumln veroorzaakt doorbacterieumln of schimmels (Tabel1) (8) Deze wordenin verband gebracht met de extrinsieke besmettingvan anesthetica door omgevingskiemen tijdensbereiding en manipulatie van de preparatenPROPOFOL is het meest onderhevig aanbijbesmetting aangezien het een olieachtigevloeistof is zonder conserveermiddel nochbacterieremmend product Daardoor wordt deontwikkeling van micro-organismen in de handgewerkt met als bijkomende risicofactor dat hetvooraf bereide preparaat langzaam via perfusiewordt toegediend Maar andere preparaten zoalsFENATYL of LIDOCAIumlNE worden evenzeer alsmogelijke bron van bijbesmetting gezien als eenzelfde oplossing wordt toegediend aanverschillende patieumlnten Het gebruik van dezelfdeinjectiespuit bij verschillende patieumlnten is de
oorzaak van besmettingen met Hepatitis B viruszelfs wanneer de injectienaalden vervangen zijnVerschillende studies hebben reeds de gevaren vandergelijke onaanvaardbare praktijken aangetoond(1415)
bull Hoewel secundaire besmettingen bij loco-regionale anesthesie potentieel ernstig kunnen zijnis de incidentie ervan niet precies gekend (1617)De waarden die men terugvindt hebben meestalbetrekking op epidurale verdoving bij bevallingenen varieumlren nogal sterk van 008 tot 00002 Inde literatuur worden op 28 infectieuzecomplicaties 21 gevallen beschreven metepidurale abcessen 6 met meningitis en eacuteeacuten gevalmet spondylitis (18) Als men de verwikkelingen bijrachianesthesie beschouwt rapporteren er zevenstudies vier gevallen van meningitis op een totaalvan 90000 patieumlnten een besmettingcijfer van
verpleegeenheid Men kan drie risicomomentenonderscheiden met name het toepassen van invasievetechnieken het ophalen van afval en het onderhoudvan bevuild materieel Het risico van seroconversie isafhankelijk van reeds hoger vernoemde factoren hetaantal infecties bij de patieumlnten en zodoende deprevalentie in de populatie het chronischedragerschap van virussen in het bloed van debesmette personen de kwantiteit en virulentie van hetinfectieus organisme en de aard van de accidenteleblootstelling (percutane verwonding door een prikinsnijding of contact met huid of slijmvlies) Devoornaamste factoren die tot een seroconversie leidenzijn eveneens gekend een diepe prikwonde door eenmet bloed besmette holle naald of een wonde metmaterieel dat gebruikt werd voor een vasculaireingreep bij een patieumlnt met een hoge antivirus titerHet niet dragen van handschoenen is daarbij eensupplementaire risicofactor Het professionelebesmettingsgevaar wordt door het personeel meestalhoger ingeschat voor HIV en meestal onderschat voorHBV Dit wordt aangetoond uit de resultaten van eenrondvraag die in 1995 werd ondernomen bij 300verpleegkundigen uit de anesthesie afdeling Metbetrekking tot HIV werd het risico door 18 vandeze verpleegkundigen geschat op groter dan of gelijkaan 30 (amper 29 hadden het cijfer juist) voorHBV werd door 30 gedacht dat het risico kleinerdan of gelijk was aan 03 (amper 21 hadden hetcijfer juist) Uit de groep van 42 professionele HIV-infecties die op 30 juni 1998 gerecenseerd werdenbetrof het in twee gevallen een anesthesist -reanimator op een totaal van 29 vermoede infecties(21)
Preventieve maatregelen en strategie bij hetimplementeren
De preventieve maatregelen die in 1997 door deFranse Vereniging voor Anesthesie en Reanimatiegepubliceerd werden zijn hoofdzakelijk toegespitstop de controle op exogene reservoirs en hetvoorkomen van overdracht (2)
Algemene aanbevelingenbull Men dient te beschikken over geschikte kledij en
een algemeen gedragspatroon vertonen passendbij het operatiekwartier Vooraleer de operatiezaalte betreden en gedurende de ganse duur van deingreep dient men op een correcte manier eenmasker te dragen en een passend haarbedekkendhoofddeksel aan te hebben Men dient deverplaatsingen minimaal te houden
bull Men dient de kiemoverdracht via de handen en
N O S O - i n f o v o l V I n deg 1 2 0 0 2
5
00045 In vergelijking met de risicofactoren bijvasculaire catheters is het waarschijnlijk dat destaat van de huid rond de insteekplaats deplaatsingsduur van de catheter en de frequentievan het herinspuiten zoveel factoren meer zijn diehet besmettingsrisico verhogen (19)
Het is belangrijk zich te herinneren dat hetzenuwstelsel (met inbegrip van het hersenvlies encerebrospinaal vocht) bijzonder gevoelig is voorbesmettingen veroorzaakt door niet conventioneleoverdraagbare pathogenen Het materieel datgebruikt wordt voor loco- regionale anesthesieschept de mogelijkheid van overdracht met dezekiemen
De professionele besmettingrisicorsquosHet gevaar van professionele besmetting bij hetanesthesiepersoneel wordt in hoofdzaak gevormddoor eventueel contact met de hepatitis virussen(meer in het bijzonder de types B en C) en met hethumane immunodeficieumlntie virus (HIV) als gevolgvan een accidenteel contact met bloed van eenpositieve patieumlnt Net als voor ander personeel uit hetoperatiekwartier worden uit de literatuur geenbesmettingen met cytomegalovirus parvovirus B19of retrovirus van een ander type dan HIVgerapporteerd De overdracht van andereviruspartikels lijkt mogelijk via rookontwikkeling bijgebruik van Laserapparatuur (Deze vorm vanbesmetting werd trouwens bevestigd door klinischestudies en door laboratoriumonderzoek Zo heeftmen kunnen aantonen dat er viruspartikels in de rookovergingen bij het wegbranden van condylomenlaryngale papillomen en van wratten) (20) Eenaccidentele microbieumlle besmetting met inbegrip vantuberculose is uitzonderlijk binnen de ruimte van hetoperatiekwartier In Frankrijk is er tot op heden geenbesmetting gekend veroorzaakt door nietconventionele overdraagbare pathogenen of doorprionen Wat de accidentele blootstelling met bloedbetreft is het werk van NELSING uit 1995 de enigestudie die handelt over de omstandigheden vanpercutane blootstelling die gerelateerd is met deanesthesie Hierin wordt het verband aangetoondtussen enerzijds het niet naleven van de universelevoorzorgsmaatregelen en anderzijds volgendefactoren onoplettendheid (41 ) ophalen van hetmaterieel (18 ) recapping van de naalden (14 )verkeerd plaatsen van de catheter (23 )inspuitingen (25 ) arterieumlle punctie (11 )veneuze punctie (8 ) spoedhandelingen (16 ) enonverwachte reacties van de patieumlnt (14 ) Deomstandigheden zijn vergelijkbaar met deze op een
het optreden van kruisbesmettingen tevoorkomen door toepassing van een strengdoorgedreven handhygieumlne het wassen (volgensde voorschriften met een zachte- of ontsmettendezeep) handontsmetting door wrijving (met eenalcoholische oplossing) vooral in de operatiezaalof in een noodsituatie en tenslotte het doordachtgebruik van handschoenen Men dient de handente schrobben en te desinfecteren op chirurgischewijze bij elke invasieve handeling die in verbandgebracht worden met chirurgie het plaatsen vaneen epidurale catheter centrale catheterisatiearterieumlle catheterisatie
bull Men dient de universele voorzorgsmaatregelen toete passen op alle patieumlnten
bull Men dient te werken op gereinigd en ontsmetteoppervlakten Dit dient te geschieden volgens deaanbevolen reinigingstechnieken en met eenfrequentie aangepast aan de verschillendeogenblikken van activiteit
bull Het werk dient te geschieden met onderlegdgevormd gemotiveerd en gecontroleerdpersoneel
Aanbevelingen voor het plaatsen van cathetersbereiding en gebruik van anestheticabull Men dient bij het plaatsen van catheters
(vasculaire ruggenmerg) de regels van dehuidontsmetting in acht te nemen wassen met eenontsmettende zeep spoelen (af)drogen en gebruikmaken van een ontsmettingsmiddel (van dezelfdesoort als de zeep) vanuit het middelste gedeeltenaar de periferie toe Niet afscheren met eenscheermes indien nodig verkiest men het epilerenof scheren met een scheerapparaat
bull Men trekt een steriele overjas aan bij de plaatsingvan een centraal veneuze catheter Dit geldteveneens bij de plaatsing van een catheter voorloco-regionale anesthesie
bull Men dient steriliteitregels in acht te nemen voor deontsmetting van flacondoppen voor perfusie ofanesthetica Dit geldt trouwens ook voor demanipulatie van driewegkranen
bull Men dient elke vorm van loco-regionaleanesthesie te vermijden in geval vanveralgemeende en bewezen sepsis en bij deaanwezigheid van infectieuze huidletsels terhoogte van de punctieplaatsMen dient de injectiespuiten tussen tweeopeenvolgende patieumlnten helemaal te vervangen(zelfs als de toediening van de anesthetica gebeurtvia een pompsysteem Dit geldt trouwens ookvoor de verlengleidingen) Het is niet voldoendevan enkel de naalden of een onderdeel van de
spuit te vervangen Indien de anesthetica viaperfusie toegediend worden dient men voor elkepatieumlnt zowel de perfusieleiding als de perfusiefleste vervangen
Aanbevelingen voor de behandeling van medischehulpmiddelenbull Het wegwerp materieel mag niet opnieuw
gebruikt wordenbull Voor anesthesie dient men enkel gebruik te maken
van gedecontamineerd en gereinigd materieelVervolgens dient men de benodigdheden teontsmetten of te steriliseren volgens devoorgeschreven procedure voor medischmaterieel in functie van aard en categorie van hetmateriaal
bull Om de kans ARI minimaal te houden dient mentijdens de verzorging de richtlijnen op te volgendie handelen over het contact van medischehulpmiddelen met weefsel met een verhoogdbesmettingsrisico door NCOP (omzendbriefDGS5CDHOSE22001138 van 14 maart 2001)
bull Men dient bij elke patieumlnt gebruik te maken vaneen antibacterieumlle- en antivirale filter die geplaatstwordt op het Y-vormig tussenstuk Dit is nodig omhet potentieumlle risico op kruisbesmetting tevoorkomen en ook om het beheer van devervanging van de anesthesiecircuits teverbeteren
Specifieke aanbevelingenbull Men dient de richtlijnen die toegepast worden
voor de andere vormen van nosocomiale infectiesin acht te nemen
bull Men dient isolatietechnieken verder toe te passenbij dragers van multiresistente kiemen inhoofdzaak door de voorzorgen bij het contact inacht te nemenPatieumlnten met tuberculose of verdacht vantuberculose dienen in isolatie beademd teworden
Aanbevelingen voor verblijf op de dagrecoverybull Men dient de richtlijnen die van toepassing zijn
voor de dagrecovery en die betrekking hebben opde situering (gelegen binnen of buiten hetoperatiekwartier) zodanig toe te passen dat hetrechtstreeks verkeer van zowel patieumlnten alspersoneel tussen het operatiekwartier en deverpleegeenheid vermeden wordt
bull Met dient er voor te zorgen dat er op dedagrecovery voldoende watervoorzieningspuntenbeschikbaar zijn maar voldoende verwijderd vanelke plaats waar zorgen toegediend worden om
N O S O - i n f o v o l V I n deg 1 2 0 0 2
6
besmettingen door aeumlrosolvorming te voorkomenbull Men dient de dagrecovery volgens dezelfde
procedures te onderhouden als de operatiezaalHet is echter niet aangewezen om het materieel tereinigen binnen de ruimte van de dagrecovery
Besluit
Het multifactorieel karakter van infecties bij degeopereerde patieumlnt stelt dat alle bewezenmaatregelen op het vlak van chirurgie en anesthesiemoet worden gevolgd (22-24) Wat deze laatstebetreft verklaart de moeilijkheid van een becijferderelatie tussen de ARI enerzijds en de gangbarepraktijken in de anesthesie anderzijds (25) demiskenning van het probleem door hetanesthesiepersoneelEen toepassing van de aanbevelingen gebeurt inverschillende stappen Deze houden in dat men eenpoging doet om kwalitatief betere zorgen toe tedienen Tijdens de opleiding van medisch enparamedisch personeel voor anesthesie wordt hetbesmettingsrisico binnen het operatiekwartierherkend en past men past preventieve maatregelentoe op basis van gevalideerde criteria volgensbeschreven procedures gevolgd door toezicht van deinfectiewaarden Daarna zal een audit vanberoepsmensen de toepassing van deze maatregelenevalueren Een optimale werkorganisatie binnen elkoperatiekwartier toepasselijk op vlak vanwerkbelasting en beschikbare middelen en geldendvoor zowel personeel als materieel is een onmisbaarelement voor het welslagen van deze betrachtingen
Bibliographie
1 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONLa pratique de lrsquoanestheacutesie en France en 1996 Ann Fr AnesthReacuteanim 1998 18 1299-13872 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONRecommandations concernant lrsquohygiegravene en anestheacutesie 1997 22pages3 CENTRE DE COORDINATION DE LA LUTTE CONTRE LESINFECTIONS NOSOCOMIALES DU SUD-EST Guide des bonnespratiques drsquohygiegravene en anestheacutesie Lyon 1996 64 pages4 AMERICAN SOCIETY OF ANESTHESIOLOGISTS Recommen-dations for infection control for the practice of anesthesiologyPark Ridge Illinois 1994 33 pages5 ASSOCIATION OF OPERATING ROOM NURSES Recommen-ded pratices Cleaning and processing anesthesia equipmentAORN J 1991 53 775-7776 OLDS JW KISCH AL EBERLE BJ WILSON JN Pseudomonasaeruginosa respiratory tract infection acquired from a contamina-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
7
ted anesthesia machine Am Rev Respir Dis 1972 105 628-6327 BENNET SN MCNEIL MM BLAND LA ARDUINO MJ VILLA-RINO ME PERROTTA DM Postoperative infections traced tocontamination of an intravenous anesthetic propofol N Engl JMed 1995 333 147-1548 HERWALDT LA POTTINGER J COFFIN SA Nosocomial infec-tions associated with anesthesia In Mayhall CG Ed Hospital epi-demiology and infection control Williams and Wilkins Balti-more 1996 655-6759 GORCE P De Abreu L PANNETIER C Evaluation du risqueinfectieux nosocomial lieacute agrave lrsquoanestheacutesie Abstract R240 37eCongregraves National de la Socieacuteteacute Franccedilaise drsquoAnestheacutesie et deReacuteanimation Paris 199510 HAJJAR J GIRARD R Surveillance des infections nosoco-miales lieacutees agrave lrsquoanestheacutesie Etude multicentrique Ann Fr AnesthReacuteanim 2000 1 47-5311 CHANT K KOCIUBA K MUNRO R CRONE S KEBRIDGE RQUIN J Investigation of possible patient-to-patient transmissionof hepatitis C in a hospital New South Wales Public Health Bul-letin 1994 5 47-5112 HAJJAR J HERNIGOU E GOUIN F Entretien et deacutesinfectiondu mateacuteriel neacutecessaire au controcircle des voies aeacuteriennes et agrave la ven-tilation meacutecanique Ann Fr Anesth Reacuteanim 1998 17 403-40713 MEFFRE C GIRARD R HAJJAR J Le risque de colonisationapregraves pose de catheacuteters veineux peacuteripheacuteriques est-il modifieacute selonlrsquoantiseptique utiliseacute lorsqursquoon applique un protocole en 4 temps HygiegraveneS 1995 9 4514 TREPANIER CA LESSARD MR BROCHU JG DENAULT PHRisk of cross-infection related to multiple use of disposablesyringes Can J Anaesth 1990 37 156-15915 ANONYME Changer drsquoaiguille et pas de seringue une pra-tique dangereuse BEH 1988 1 1-216 WEDEL DJ HERLOCKER TT Risks of regional anesthesia-infectious septic Reg Anesthes 1996 21(6) 57-6117 AUBOYER C Risque infectieux et anestheacutesie loco-reacutegionaleAnn Fr Anesth Reacuteanim 1998 17 1257-126018 MARSAUDON E BERTHIER F Meacuteningite agrave Staphylococcusaureus apregraves anestheacutesie peacuteridurale obsteacutetricale Ann Fr AnesthReacuteanim 1996 15 389-39019 HOLT HM ANDERSON SS ANDERSON O GARHN-HAN-SEN B SIBONI K Infection following epidural catheterization JHosp Infect 1995 30 253-26020 GARDEN JM OrsquoBANNION MK SHELNITZ LS ET AL Papil-loma virus in the vapor of carbon dioxide Laser-treated verrucaeJAMA 1988 8 1199-120221 LOT F DE BENOIST AC ABITEBOUL D Infections profes-sionnelles par le VIH en France chez le personnel de santeacute Lepoint au 30 juin 1998 BEH 1999 18 69-7022 BIMAR MC HAJJAR J POTTECHER B Risque infectieux noso-comial en anestheacutesie Recommandations geacuteneacuterales Ann fr AnesthReacuteanim 1998 17 392-40223 KORINEK AM Recommandations pour la pose des abordsvasculaires au bloc opeacuteratoire Voies veineuses et voies arteacuteriellespeacuteripheacuteriques Ann Fr Anesth Reacuteanim 1998 17 1250-125224 VEBER B Manipulation des agents anestheacutesiques et desseringues Recommandations et argumentations Ann Fr AnesthReacuteanim 1998 17 1253-125625 TAIT AR TUTTLE DB Preventing perioperative transmissionof infection a survey of anesthesiology practice Anesth Analg1995 80 764-769
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
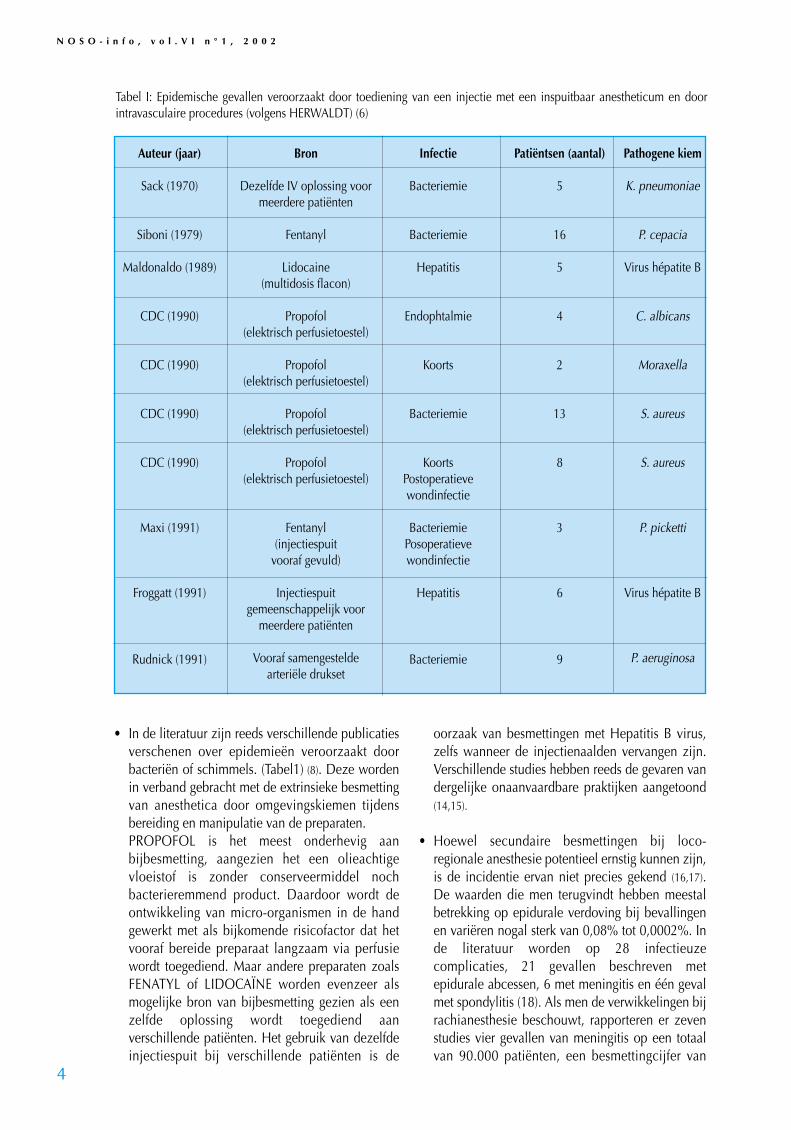
N O S O - i n f o v o l V I n deg 1 2 0 0 2
4
Tabel I Epidemische gevallen veroorzaakt door toediening van een injectie met een inspuitbaar anestheticum en doorintravasculaire procedures (volgens HERWALDT) (6)
Auteur (jaar)
Sack (1970)
Siboni (1979)
Maldonaldo (1989)
CDC (1990)
CDC (1990)
CDC (1990)
CDC (1990)
Maxi (1991)
Froggatt (1991)
Rudnick (1991)
Bron
Dezelfde IV oplossing voormeerdere patieumlnten
Fentanyl
Lidocaine(multidosis flacon)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Propofol(elektrisch perfusietoestel)
Fentanyl(injectiespuit
vooraf gevuld)
Injectiespuitgemeenschappelijk voor
meerdere patieumlnten
Vooraf samengestelde arterieumlle drukset
Infectie
Bacteriemie
Bacteriemie
Hepatitis
Endophtalmie
Koorts
Bacteriemie
KoortsPostoperatieve wondinfectie
BacteriemiePosoperatieve wondinfectie
Hepatitis
Bacteriemie
Patieumlntsen (aantal)
5
16
5
4
2
13
8
3
6
9
Pathogene kiem
K pneumoniae
P cepacia
Virus heacutepatite B
C albicans
Moraxella
S aureus
S aureus
P picketti
Virus heacutepatite B
P aeruginosa
bull In de literatuur zijn reeds verschillende publicatiesverschenen over epidemieeumln veroorzaakt doorbacterieumln of schimmels (Tabel1) (8) Deze wordenin verband gebracht met de extrinsieke besmettingvan anesthetica door omgevingskiemen tijdensbereiding en manipulatie van de preparatenPROPOFOL is het meest onderhevig aanbijbesmetting aangezien het een olieachtigevloeistof is zonder conserveermiddel nochbacterieremmend product Daardoor wordt deontwikkeling van micro-organismen in de handgewerkt met als bijkomende risicofactor dat hetvooraf bereide preparaat langzaam via perfusiewordt toegediend Maar andere preparaten zoalsFENATYL of LIDOCAIumlNE worden evenzeer alsmogelijke bron van bijbesmetting gezien als eenzelfde oplossing wordt toegediend aanverschillende patieumlnten Het gebruik van dezelfdeinjectiespuit bij verschillende patieumlnten is de
oorzaak van besmettingen met Hepatitis B viruszelfs wanneer de injectienaalden vervangen zijnVerschillende studies hebben reeds de gevaren vandergelijke onaanvaardbare praktijken aangetoond(1415)
bull Hoewel secundaire besmettingen bij loco-regionale anesthesie potentieel ernstig kunnen zijnis de incidentie ervan niet precies gekend (1617)De waarden die men terugvindt hebben meestalbetrekking op epidurale verdoving bij bevallingenen varieumlren nogal sterk van 008 tot 00002 Inde literatuur worden op 28 infectieuzecomplicaties 21 gevallen beschreven metepidurale abcessen 6 met meningitis en eacuteeacuten gevalmet spondylitis (18) Als men de verwikkelingen bijrachianesthesie beschouwt rapporteren er zevenstudies vier gevallen van meningitis op een totaalvan 90000 patieumlnten een besmettingcijfer van
verpleegeenheid Men kan drie risicomomentenonderscheiden met name het toepassen van invasievetechnieken het ophalen van afval en het onderhoudvan bevuild materieel Het risico van seroconversie isafhankelijk van reeds hoger vernoemde factoren hetaantal infecties bij de patieumlnten en zodoende deprevalentie in de populatie het chronischedragerschap van virussen in het bloed van debesmette personen de kwantiteit en virulentie van hetinfectieus organisme en de aard van de accidenteleblootstelling (percutane verwonding door een prikinsnijding of contact met huid of slijmvlies) Devoornaamste factoren die tot een seroconversie leidenzijn eveneens gekend een diepe prikwonde door eenmet bloed besmette holle naald of een wonde metmaterieel dat gebruikt werd voor een vasculaireingreep bij een patieumlnt met een hoge antivirus titerHet niet dragen van handschoenen is daarbij eensupplementaire risicofactor Het professionelebesmettingsgevaar wordt door het personeel meestalhoger ingeschat voor HIV en meestal onderschat voorHBV Dit wordt aangetoond uit de resultaten van eenrondvraag die in 1995 werd ondernomen bij 300verpleegkundigen uit de anesthesie afdeling Metbetrekking tot HIV werd het risico door 18 vandeze verpleegkundigen geschat op groter dan of gelijkaan 30 (amper 29 hadden het cijfer juist) voorHBV werd door 30 gedacht dat het risico kleinerdan of gelijk was aan 03 (amper 21 hadden hetcijfer juist) Uit de groep van 42 professionele HIV-infecties die op 30 juni 1998 gerecenseerd werdenbetrof het in twee gevallen een anesthesist -reanimator op een totaal van 29 vermoede infecties(21)
Preventieve maatregelen en strategie bij hetimplementeren
De preventieve maatregelen die in 1997 door deFranse Vereniging voor Anesthesie en Reanimatiegepubliceerd werden zijn hoofdzakelijk toegespitstop de controle op exogene reservoirs en hetvoorkomen van overdracht (2)
Algemene aanbevelingenbull Men dient te beschikken over geschikte kledij en
een algemeen gedragspatroon vertonen passendbij het operatiekwartier Vooraleer de operatiezaalte betreden en gedurende de ganse duur van deingreep dient men op een correcte manier eenmasker te dragen en een passend haarbedekkendhoofddeksel aan te hebben Men dient deverplaatsingen minimaal te houden
bull Men dient de kiemoverdracht via de handen en
N O S O - i n f o v o l V I n deg 1 2 0 0 2
5
00045 In vergelijking met de risicofactoren bijvasculaire catheters is het waarschijnlijk dat destaat van de huid rond de insteekplaats deplaatsingsduur van de catheter en de frequentievan het herinspuiten zoveel factoren meer zijn diehet besmettingsrisico verhogen (19)
Het is belangrijk zich te herinneren dat hetzenuwstelsel (met inbegrip van het hersenvlies encerebrospinaal vocht) bijzonder gevoelig is voorbesmettingen veroorzaakt door niet conventioneleoverdraagbare pathogenen Het materieel datgebruikt wordt voor loco- regionale anesthesieschept de mogelijkheid van overdracht met dezekiemen
De professionele besmettingrisicorsquosHet gevaar van professionele besmetting bij hetanesthesiepersoneel wordt in hoofdzaak gevormddoor eventueel contact met de hepatitis virussen(meer in het bijzonder de types B en C) en met hethumane immunodeficieumlntie virus (HIV) als gevolgvan een accidenteel contact met bloed van eenpositieve patieumlnt Net als voor ander personeel uit hetoperatiekwartier worden uit de literatuur geenbesmettingen met cytomegalovirus parvovirus B19of retrovirus van een ander type dan HIVgerapporteerd De overdracht van andereviruspartikels lijkt mogelijk via rookontwikkeling bijgebruik van Laserapparatuur (Deze vorm vanbesmetting werd trouwens bevestigd door klinischestudies en door laboratoriumonderzoek Zo heeftmen kunnen aantonen dat er viruspartikels in de rookovergingen bij het wegbranden van condylomenlaryngale papillomen en van wratten) (20) Eenaccidentele microbieumlle besmetting met inbegrip vantuberculose is uitzonderlijk binnen de ruimte van hetoperatiekwartier In Frankrijk is er tot op heden geenbesmetting gekend veroorzaakt door nietconventionele overdraagbare pathogenen of doorprionen Wat de accidentele blootstelling met bloedbetreft is het werk van NELSING uit 1995 de enigestudie die handelt over de omstandigheden vanpercutane blootstelling die gerelateerd is met deanesthesie Hierin wordt het verband aangetoondtussen enerzijds het niet naleven van de universelevoorzorgsmaatregelen en anderzijds volgendefactoren onoplettendheid (41 ) ophalen van hetmaterieel (18 ) recapping van de naalden (14 )verkeerd plaatsen van de catheter (23 )inspuitingen (25 ) arterieumlle punctie (11 )veneuze punctie (8 ) spoedhandelingen (16 ) enonverwachte reacties van de patieumlnt (14 ) Deomstandigheden zijn vergelijkbaar met deze op een
het optreden van kruisbesmettingen tevoorkomen door toepassing van een strengdoorgedreven handhygieumlne het wassen (volgensde voorschriften met een zachte- of ontsmettendezeep) handontsmetting door wrijving (met eenalcoholische oplossing) vooral in de operatiezaalof in een noodsituatie en tenslotte het doordachtgebruik van handschoenen Men dient de handente schrobben en te desinfecteren op chirurgischewijze bij elke invasieve handeling die in verbandgebracht worden met chirurgie het plaatsen vaneen epidurale catheter centrale catheterisatiearterieumlle catheterisatie
bull Men dient de universele voorzorgsmaatregelen toete passen op alle patieumlnten
bull Men dient te werken op gereinigd en ontsmetteoppervlakten Dit dient te geschieden volgens deaanbevolen reinigingstechnieken en met eenfrequentie aangepast aan de verschillendeogenblikken van activiteit
bull Het werk dient te geschieden met onderlegdgevormd gemotiveerd en gecontroleerdpersoneel
Aanbevelingen voor het plaatsen van cathetersbereiding en gebruik van anestheticabull Men dient bij het plaatsen van catheters
(vasculaire ruggenmerg) de regels van dehuidontsmetting in acht te nemen wassen met eenontsmettende zeep spoelen (af)drogen en gebruikmaken van een ontsmettingsmiddel (van dezelfdesoort als de zeep) vanuit het middelste gedeeltenaar de periferie toe Niet afscheren met eenscheermes indien nodig verkiest men het epilerenof scheren met een scheerapparaat
bull Men trekt een steriele overjas aan bij de plaatsingvan een centraal veneuze catheter Dit geldteveneens bij de plaatsing van een catheter voorloco-regionale anesthesie
bull Men dient steriliteitregels in acht te nemen voor deontsmetting van flacondoppen voor perfusie ofanesthetica Dit geldt trouwens ook voor demanipulatie van driewegkranen
bull Men dient elke vorm van loco-regionaleanesthesie te vermijden in geval vanveralgemeende en bewezen sepsis en bij deaanwezigheid van infectieuze huidletsels terhoogte van de punctieplaatsMen dient de injectiespuiten tussen tweeopeenvolgende patieumlnten helemaal te vervangen(zelfs als de toediening van de anesthetica gebeurtvia een pompsysteem Dit geldt trouwens ookvoor de verlengleidingen) Het is niet voldoendevan enkel de naalden of een onderdeel van de
spuit te vervangen Indien de anesthetica viaperfusie toegediend worden dient men voor elkepatieumlnt zowel de perfusieleiding als de perfusiefleste vervangen
Aanbevelingen voor de behandeling van medischehulpmiddelenbull Het wegwerp materieel mag niet opnieuw
gebruikt wordenbull Voor anesthesie dient men enkel gebruik te maken
van gedecontamineerd en gereinigd materieelVervolgens dient men de benodigdheden teontsmetten of te steriliseren volgens devoorgeschreven procedure voor medischmaterieel in functie van aard en categorie van hetmateriaal
bull Om de kans ARI minimaal te houden dient mentijdens de verzorging de richtlijnen op te volgendie handelen over het contact van medischehulpmiddelen met weefsel met een verhoogdbesmettingsrisico door NCOP (omzendbriefDGS5CDHOSE22001138 van 14 maart 2001)
bull Men dient bij elke patieumlnt gebruik te maken vaneen antibacterieumlle- en antivirale filter die geplaatstwordt op het Y-vormig tussenstuk Dit is nodig omhet potentieumlle risico op kruisbesmetting tevoorkomen en ook om het beheer van devervanging van de anesthesiecircuits teverbeteren
Specifieke aanbevelingenbull Men dient de richtlijnen die toegepast worden
voor de andere vormen van nosocomiale infectiesin acht te nemen
bull Men dient isolatietechnieken verder toe te passenbij dragers van multiresistente kiemen inhoofdzaak door de voorzorgen bij het contact inacht te nemenPatieumlnten met tuberculose of verdacht vantuberculose dienen in isolatie beademd teworden
Aanbevelingen voor verblijf op de dagrecoverybull Men dient de richtlijnen die van toepassing zijn
voor de dagrecovery en die betrekking hebben opde situering (gelegen binnen of buiten hetoperatiekwartier) zodanig toe te passen dat hetrechtstreeks verkeer van zowel patieumlnten alspersoneel tussen het operatiekwartier en deverpleegeenheid vermeden wordt
bull Met dient er voor te zorgen dat er op dedagrecovery voldoende watervoorzieningspuntenbeschikbaar zijn maar voldoende verwijderd vanelke plaats waar zorgen toegediend worden om
N O S O - i n f o v o l V I n deg 1 2 0 0 2
6
besmettingen door aeumlrosolvorming te voorkomenbull Men dient de dagrecovery volgens dezelfde
procedures te onderhouden als de operatiezaalHet is echter niet aangewezen om het materieel tereinigen binnen de ruimte van de dagrecovery
Besluit
Het multifactorieel karakter van infecties bij degeopereerde patieumlnt stelt dat alle bewezenmaatregelen op het vlak van chirurgie en anesthesiemoet worden gevolgd (22-24) Wat deze laatstebetreft verklaart de moeilijkheid van een becijferderelatie tussen de ARI enerzijds en de gangbarepraktijken in de anesthesie anderzijds (25) demiskenning van het probleem door hetanesthesiepersoneelEen toepassing van de aanbevelingen gebeurt inverschillende stappen Deze houden in dat men eenpoging doet om kwalitatief betere zorgen toe tedienen Tijdens de opleiding van medisch enparamedisch personeel voor anesthesie wordt hetbesmettingsrisico binnen het operatiekwartierherkend en past men past preventieve maatregelentoe op basis van gevalideerde criteria volgensbeschreven procedures gevolgd door toezicht van deinfectiewaarden Daarna zal een audit vanberoepsmensen de toepassing van deze maatregelenevalueren Een optimale werkorganisatie binnen elkoperatiekwartier toepasselijk op vlak vanwerkbelasting en beschikbare middelen en geldendvoor zowel personeel als materieel is een onmisbaarelement voor het welslagen van deze betrachtingen
Bibliographie
1 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONLa pratique de lrsquoanestheacutesie en France en 1996 Ann Fr AnesthReacuteanim 1998 18 1299-13872 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONRecommandations concernant lrsquohygiegravene en anestheacutesie 1997 22pages3 CENTRE DE COORDINATION DE LA LUTTE CONTRE LESINFECTIONS NOSOCOMIALES DU SUD-EST Guide des bonnespratiques drsquohygiegravene en anestheacutesie Lyon 1996 64 pages4 AMERICAN SOCIETY OF ANESTHESIOLOGISTS Recommen-dations for infection control for the practice of anesthesiologyPark Ridge Illinois 1994 33 pages5 ASSOCIATION OF OPERATING ROOM NURSES Recommen-ded pratices Cleaning and processing anesthesia equipmentAORN J 1991 53 775-7776 OLDS JW KISCH AL EBERLE BJ WILSON JN Pseudomonasaeruginosa respiratory tract infection acquired from a contamina-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
7
ted anesthesia machine Am Rev Respir Dis 1972 105 628-6327 BENNET SN MCNEIL MM BLAND LA ARDUINO MJ VILLA-RINO ME PERROTTA DM Postoperative infections traced tocontamination of an intravenous anesthetic propofol N Engl JMed 1995 333 147-1548 HERWALDT LA POTTINGER J COFFIN SA Nosocomial infec-tions associated with anesthesia In Mayhall CG Ed Hospital epi-demiology and infection control Williams and Wilkins Balti-more 1996 655-6759 GORCE P De Abreu L PANNETIER C Evaluation du risqueinfectieux nosocomial lieacute agrave lrsquoanestheacutesie Abstract R240 37eCongregraves National de la Socieacuteteacute Franccedilaise drsquoAnestheacutesie et deReacuteanimation Paris 199510 HAJJAR J GIRARD R Surveillance des infections nosoco-miales lieacutees agrave lrsquoanestheacutesie Etude multicentrique Ann Fr AnesthReacuteanim 2000 1 47-5311 CHANT K KOCIUBA K MUNRO R CRONE S KEBRIDGE RQUIN J Investigation of possible patient-to-patient transmissionof hepatitis C in a hospital New South Wales Public Health Bul-letin 1994 5 47-5112 HAJJAR J HERNIGOU E GOUIN F Entretien et deacutesinfectiondu mateacuteriel neacutecessaire au controcircle des voies aeacuteriennes et agrave la ven-tilation meacutecanique Ann Fr Anesth Reacuteanim 1998 17 403-40713 MEFFRE C GIRARD R HAJJAR J Le risque de colonisationapregraves pose de catheacuteters veineux peacuteripheacuteriques est-il modifieacute selonlrsquoantiseptique utiliseacute lorsqursquoon applique un protocole en 4 temps HygiegraveneS 1995 9 4514 TREPANIER CA LESSARD MR BROCHU JG DENAULT PHRisk of cross-infection related to multiple use of disposablesyringes Can J Anaesth 1990 37 156-15915 ANONYME Changer drsquoaiguille et pas de seringue une pra-tique dangereuse BEH 1988 1 1-216 WEDEL DJ HERLOCKER TT Risks of regional anesthesia-infectious septic Reg Anesthes 1996 21(6) 57-6117 AUBOYER C Risque infectieux et anestheacutesie loco-reacutegionaleAnn Fr Anesth Reacuteanim 1998 17 1257-126018 MARSAUDON E BERTHIER F Meacuteningite agrave Staphylococcusaureus apregraves anestheacutesie peacuteridurale obsteacutetricale Ann Fr AnesthReacuteanim 1996 15 389-39019 HOLT HM ANDERSON SS ANDERSON O GARHN-HAN-SEN B SIBONI K Infection following epidural catheterization JHosp Infect 1995 30 253-26020 GARDEN JM OrsquoBANNION MK SHELNITZ LS ET AL Papil-loma virus in the vapor of carbon dioxide Laser-treated verrucaeJAMA 1988 8 1199-120221 LOT F DE BENOIST AC ABITEBOUL D Infections profes-sionnelles par le VIH en France chez le personnel de santeacute Lepoint au 30 juin 1998 BEH 1999 18 69-7022 BIMAR MC HAJJAR J POTTECHER B Risque infectieux noso-comial en anestheacutesie Recommandations geacuteneacuterales Ann fr AnesthReacuteanim 1998 17 392-40223 KORINEK AM Recommandations pour la pose des abordsvasculaires au bloc opeacuteratoire Voies veineuses et voies arteacuteriellespeacuteripheacuteriques Ann Fr Anesth Reacuteanim 1998 17 1250-125224 VEBER B Manipulation des agents anestheacutesiques et desseringues Recommandations et argumentations Ann Fr AnesthReacuteanim 1998 17 1253-125625 TAIT AR TUTTLE DB Preventing perioperative transmissionof infection a survey of anesthesiology practice Anesth Analg1995 80 764-769
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

verpleegeenheid Men kan drie risicomomentenonderscheiden met name het toepassen van invasievetechnieken het ophalen van afval en het onderhoudvan bevuild materieel Het risico van seroconversie isafhankelijk van reeds hoger vernoemde factoren hetaantal infecties bij de patieumlnten en zodoende deprevalentie in de populatie het chronischedragerschap van virussen in het bloed van debesmette personen de kwantiteit en virulentie van hetinfectieus organisme en de aard van de accidenteleblootstelling (percutane verwonding door een prikinsnijding of contact met huid of slijmvlies) Devoornaamste factoren die tot een seroconversie leidenzijn eveneens gekend een diepe prikwonde door eenmet bloed besmette holle naald of een wonde metmaterieel dat gebruikt werd voor een vasculaireingreep bij een patieumlnt met een hoge antivirus titerHet niet dragen van handschoenen is daarbij eensupplementaire risicofactor Het professionelebesmettingsgevaar wordt door het personeel meestalhoger ingeschat voor HIV en meestal onderschat voorHBV Dit wordt aangetoond uit de resultaten van eenrondvraag die in 1995 werd ondernomen bij 300verpleegkundigen uit de anesthesie afdeling Metbetrekking tot HIV werd het risico door 18 vandeze verpleegkundigen geschat op groter dan of gelijkaan 30 (amper 29 hadden het cijfer juist) voorHBV werd door 30 gedacht dat het risico kleinerdan of gelijk was aan 03 (amper 21 hadden hetcijfer juist) Uit de groep van 42 professionele HIV-infecties die op 30 juni 1998 gerecenseerd werdenbetrof het in twee gevallen een anesthesist -reanimator op een totaal van 29 vermoede infecties(21)
Preventieve maatregelen en strategie bij hetimplementeren
De preventieve maatregelen die in 1997 door deFranse Vereniging voor Anesthesie en Reanimatiegepubliceerd werden zijn hoofdzakelijk toegespitstop de controle op exogene reservoirs en hetvoorkomen van overdracht (2)
Algemene aanbevelingenbull Men dient te beschikken over geschikte kledij en
een algemeen gedragspatroon vertonen passendbij het operatiekwartier Vooraleer de operatiezaalte betreden en gedurende de ganse duur van deingreep dient men op een correcte manier eenmasker te dragen en een passend haarbedekkendhoofddeksel aan te hebben Men dient deverplaatsingen minimaal te houden
bull Men dient de kiemoverdracht via de handen en
N O S O - i n f o v o l V I n deg 1 2 0 0 2
5
00045 In vergelijking met de risicofactoren bijvasculaire catheters is het waarschijnlijk dat destaat van de huid rond de insteekplaats deplaatsingsduur van de catheter en de frequentievan het herinspuiten zoveel factoren meer zijn diehet besmettingsrisico verhogen (19)
Het is belangrijk zich te herinneren dat hetzenuwstelsel (met inbegrip van het hersenvlies encerebrospinaal vocht) bijzonder gevoelig is voorbesmettingen veroorzaakt door niet conventioneleoverdraagbare pathogenen Het materieel datgebruikt wordt voor loco- regionale anesthesieschept de mogelijkheid van overdracht met dezekiemen
De professionele besmettingrisicorsquosHet gevaar van professionele besmetting bij hetanesthesiepersoneel wordt in hoofdzaak gevormddoor eventueel contact met de hepatitis virussen(meer in het bijzonder de types B en C) en met hethumane immunodeficieumlntie virus (HIV) als gevolgvan een accidenteel contact met bloed van eenpositieve patieumlnt Net als voor ander personeel uit hetoperatiekwartier worden uit de literatuur geenbesmettingen met cytomegalovirus parvovirus B19of retrovirus van een ander type dan HIVgerapporteerd De overdracht van andereviruspartikels lijkt mogelijk via rookontwikkeling bijgebruik van Laserapparatuur (Deze vorm vanbesmetting werd trouwens bevestigd door klinischestudies en door laboratoriumonderzoek Zo heeftmen kunnen aantonen dat er viruspartikels in de rookovergingen bij het wegbranden van condylomenlaryngale papillomen en van wratten) (20) Eenaccidentele microbieumlle besmetting met inbegrip vantuberculose is uitzonderlijk binnen de ruimte van hetoperatiekwartier In Frankrijk is er tot op heden geenbesmetting gekend veroorzaakt door nietconventionele overdraagbare pathogenen of doorprionen Wat de accidentele blootstelling met bloedbetreft is het werk van NELSING uit 1995 de enigestudie die handelt over de omstandigheden vanpercutane blootstelling die gerelateerd is met deanesthesie Hierin wordt het verband aangetoondtussen enerzijds het niet naleven van de universelevoorzorgsmaatregelen en anderzijds volgendefactoren onoplettendheid (41 ) ophalen van hetmaterieel (18 ) recapping van de naalden (14 )verkeerd plaatsen van de catheter (23 )inspuitingen (25 ) arterieumlle punctie (11 )veneuze punctie (8 ) spoedhandelingen (16 ) enonverwachte reacties van de patieumlnt (14 ) Deomstandigheden zijn vergelijkbaar met deze op een
het optreden van kruisbesmettingen tevoorkomen door toepassing van een strengdoorgedreven handhygieumlne het wassen (volgensde voorschriften met een zachte- of ontsmettendezeep) handontsmetting door wrijving (met eenalcoholische oplossing) vooral in de operatiezaalof in een noodsituatie en tenslotte het doordachtgebruik van handschoenen Men dient de handente schrobben en te desinfecteren op chirurgischewijze bij elke invasieve handeling die in verbandgebracht worden met chirurgie het plaatsen vaneen epidurale catheter centrale catheterisatiearterieumlle catheterisatie
bull Men dient de universele voorzorgsmaatregelen toete passen op alle patieumlnten
bull Men dient te werken op gereinigd en ontsmetteoppervlakten Dit dient te geschieden volgens deaanbevolen reinigingstechnieken en met eenfrequentie aangepast aan de verschillendeogenblikken van activiteit
bull Het werk dient te geschieden met onderlegdgevormd gemotiveerd en gecontroleerdpersoneel
Aanbevelingen voor het plaatsen van cathetersbereiding en gebruik van anestheticabull Men dient bij het plaatsen van catheters
(vasculaire ruggenmerg) de regels van dehuidontsmetting in acht te nemen wassen met eenontsmettende zeep spoelen (af)drogen en gebruikmaken van een ontsmettingsmiddel (van dezelfdesoort als de zeep) vanuit het middelste gedeeltenaar de periferie toe Niet afscheren met eenscheermes indien nodig verkiest men het epilerenof scheren met een scheerapparaat
bull Men trekt een steriele overjas aan bij de plaatsingvan een centraal veneuze catheter Dit geldteveneens bij de plaatsing van een catheter voorloco-regionale anesthesie
bull Men dient steriliteitregels in acht te nemen voor deontsmetting van flacondoppen voor perfusie ofanesthetica Dit geldt trouwens ook voor demanipulatie van driewegkranen
bull Men dient elke vorm van loco-regionaleanesthesie te vermijden in geval vanveralgemeende en bewezen sepsis en bij deaanwezigheid van infectieuze huidletsels terhoogte van de punctieplaatsMen dient de injectiespuiten tussen tweeopeenvolgende patieumlnten helemaal te vervangen(zelfs als de toediening van de anesthetica gebeurtvia een pompsysteem Dit geldt trouwens ookvoor de verlengleidingen) Het is niet voldoendevan enkel de naalden of een onderdeel van de
spuit te vervangen Indien de anesthetica viaperfusie toegediend worden dient men voor elkepatieumlnt zowel de perfusieleiding als de perfusiefleste vervangen
Aanbevelingen voor de behandeling van medischehulpmiddelenbull Het wegwerp materieel mag niet opnieuw
gebruikt wordenbull Voor anesthesie dient men enkel gebruik te maken
van gedecontamineerd en gereinigd materieelVervolgens dient men de benodigdheden teontsmetten of te steriliseren volgens devoorgeschreven procedure voor medischmaterieel in functie van aard en categorie van hetmateriaal
bull Om de kans ARI minimaal te houden dient mentijdens de verzorging de richtlijnen op te volgendie handelen over het contact van medischehulpmiddelen met weefsel met een verhoogdbesmettingsrisico door NCOP (omzendbriefDGS5CDHOSE22001138 van 14 maart 2001)
bull Men dient bij elke patieumlnt gebruik te maken vaneen antibacterieumlle- en antivirale filter die geplaatstwordt op het Y-vormig tussenstuk Dit is nodig omhet potentieumlle risico op kruisbesmetting tevoorkomen en ook om het beheer van devervanging van de anesthesiecircuits teverbeteren
Specifieke aanbevelingenbull Men dient de richtlijnen die toegepast worden
voor de andere vormen van nosocomiale infectiesin acht te nemen
bull Men dient isolatietechnieken verder toe te passenbij dragers van multiresistente kiemen inhoofdzaak door de voorzorgen bij het contact inacht te nemenPatieumlnten met tuberculose of verdacht vantuberculose dienen in isolatie beademd teworden
Aanbevelingen voor verblijf op de dagrecoverybull Men dient de richtlijnen die van toepassing zijn
voor de dagrecovery en die betrekking hebben opde situering (gelegen binnen of buiten hetoperatiekwartier) zodanig toe te passen dat hetrechtstreeks verkeer van zowel patieumlnten alspersoneel tussen het operatiekwartier en deverpleegeenheid vermeden wordt
bull Met dient er voor te zorgen dat er op dedagrecovery voldoende watervoorzieningspuntenbeschikbaar zijn maar voldoende verwijderd vanelke plaats waar zorgen toegediend worden om
N O S O - i n f o v o l V I n deg 1 2 0 0 2
6
besmettingen door aeumlrosolvorming te voorkomenbull Men dient de dagrecovery volgens dezelfde
procedures te onderhouden als de operatiezaalHet is echter niet aangewezen om het materieel tereinigen binnen de ruimte van de dagrecovery
Besluit
Het multifactorieel karakter van infecties bij degeopereerde patieumlnt stelt dat alle bewezenmaatregelen op het vlak van chirurgie en anesthesiemoet worden gevolgd (22-24) Wat deze laatstebetreft verklaart de moeilijkheid van een becijferderelatie tussen de ARI enerzijds en de gangbarepraktijken in de anesthesie anderzijds (25) demiskenning van het probleem door hetanesthesiepersoneelEen toepassing van de aanbevelingen gebeurt inverschillende stappen Deze houden in dat men eenpoging doet om kwalitatief betere zorgen toe tedienen Tijdens de opleiding van medisch enparamedisch personeel voor anesthesie wordt hetbesmettingsrisico binnen het operatiekwartierherkend en past men past preventieve maatregelentoe op basis van gevalideerde criteria volgensbeschreven procedures gevolgd door toezicht van deinfectiewaarden Daarna zal een audit vanberoepsmensen de toepassing van deze maatregelenevalueren Een optimale werkorganisatie binnen elkoperatiekwartier toepasselijk op vlak vanwerkbelasting en beschikbare middelen en geldendvoor zowel personeel als materieel is een onmisbaarelement voor het welslagen van deze betrachtingen
Bibliographie
1 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONLa pratique de lrsquoanestheacutesie en France en 1996 Ann Fr AnesthReacuteanim 1998 18 1299-13872 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONRecommandations concernant lrsquohygiegravene en anestheacutesie 1997 22pages3 CENTRE DE COORDINATION DE LA LUTTE CONTRE LESINFECTIONS NOSOCOMIALES DU SUD-EST Guide des bonnespratiques drsquohygiegravene en anestheacutesie Lyon 1996 64 pages4 AMERICAN SOCIETY OF ANESTHESIOLOGISTS Recommen-dations for infection control for the practice of anesthesiologyPark Ridge Illinois 1994 33 pages5 ASSOCIATION OF OPERATING ROOM NURSES Recommen-ded pratices Cleaning and processing anesthesia equipmentAORN J 1991 53 775-7776 OLDS JW KISCH AL EBERLE BJ WILSON JN Pseudomonasaeruginosa respiratory tract infection acquired from a contamina-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
7
ted anesthesia machine Am Rev Respir Dis 1972 105 628-6327 BENNET SN MCNEIL MM BLAND LA ARDUINO MJ VILLA-RINO ME PERROTTA DM Postoperative infections traced tocontamination of an intravenous anesthetic propofol N Engl JMed 1995 333 147-1548 HERWALDT LA POTTINGER J COFFIN SA Nosocomial infec-tions associated with anesthesia In Mayhall CG Ed Hospital epi-demiology and infection control Williams and Wilkins Balti-more 1996 655-6759 GORCE P De Abreu L PANNETIER C Evaluation du risqueinfectieux nosocomial lieacute agrave lrsquoanestheacutesie Abstract R240 37eCongregraves National de la Socieacuteteacute Franccedilaise drsquoAnestheacutesie et deReacuteanimation Paris 199510 HAJJAR J GIRARD R Surveillance des infections nosoco-miales lieacutees agrave lrsquoanestheacutesie Etude multicentrique Ann Fr AnesthReacuteanim 2000 1 47-5311 CHANT K KOCIUBA K MUNRO R CRONE S KEBRIDGE RQUIN J Investigation of possible patient-to-patient transmissionof hepatitis C in a hospital New South Wales Public Health Bul-letin 1994 5 47-5112 HAJJAR J HERNIGOU E GOUIN F Entretien et deacutesinfectiondu mateacuteriel neacutecessaire au controcircle des voies aeacuteriennes et agrave la ven-tilation meacutecanique Ann Fr Anesth Reacuteanim 1998 17 403-40713 MEFFRE C GIRARD R HAJJAR J Le risque de colonisationapregraves pose de catheacuteters veineux peacuteripheacuteriques est-il modifieacute selonlrsquoantiseptique utiliseacute lorsqursquoon applique un protocole en 4 temps HygiegraveneS 1995 9 4514 TREPANIER CA LESSARD MR BROCHU JG DENAULT PHRisk of cross-infection related to multiple use of disposablesyringes Can J Anaesth 1990 37 156-15915 ANONYME Changer drsquoaiguille et pas de seringue une pra-tique dangereuse BEH 1988 1 1-216 WEDEL DJ HERLOCKER TT Risks of regional anesthesia-infectious septic Reg Anesthes 1996 21(6) 57-6117 AUBOYER C Risque infectieux et anestheacutesie loco-reacutegionaleAnn Fr Anesth Reacuteanim 1998 17 1257-126018 MARSAUDON E BERTHIER F Meacuteningite agrave Staphylococcusaureus apregraves anestheacutesie peacuteridurale obsteacutetricale Ann Fr AnesthReacuteanim 1996 15 389-39019 HOLT HM ANDERSON SS ANDERSON O GARHN-HAN-SEN B SIBONI K Infection following epidural catheterization JHosp Infect 1995 30 253-26020 GARDEN JM OrsquoBANNION MK SHELNITZ LS ET AL Papil-loma virus in the vapor of carbon dioxide Laser-treated verrucaeJAMA 1988 8 1199-120221 LOT F DE BENOIST AC ABITEBOUL D Infections profes-sionnelles par le VIH en France chez le personnel de santeacute Lepoint au 30 juin 1998 BEH 1999 18 69-7022 BIMAR MC HAJJAR J POTTECHER B Risque infectieux noso-comial en anestheacutesie Recommandations geacuteneacuterales Ann fr AnesthReacuteanim 1998 17 392-40223 KORINEK AM Recommandations pour la pose des abordsvasculaires au bloc opeacuteratoire Voies veineuses et voies arteacuteriellespeacuteripheacuteriques Ann Fr Anesth Reacuteanim 1998 17 1250-125224 VEBER B Manipulation des agents anestheacutesiques et desseringues Recommandations et argumentations Ann Fr AnesthReacuteanim 1998 17 1253-125625 TAIT AR TUTTLE DB Preventing perioperative transmissionof infection a survey of anesthesiology practice Anesth Analg1995 80 764-769
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
het optreden van kruisbesmettingen tevoorkomen door toepassing van een strengdoorgedreven handhygieumlne het wassen (volgensde voorschriften met een zachte- of ontsmettendezeep) handontsmetting door wrijving (met eenalcoholische oplossing) vooral in de operatiezaalof in een noodsituatie en tenslotte het doordachtgebruik van handschoenen Men dient de handente schrobben en te desinfecteren op chirurgischewijze bij elke invasieve handeling die in verbandgebracht worden met chirurgie het plaatsen vaneen epidurale catheter centrale catheterisatiearterieumlle catheterisatie
bull Men dient de universele voorzorgsmaatregelen toete passen op alle patieumlnten
bull Men dient te werken op gereinigd en ontsmetteoppervlakten Dit dient te geschieden volgens deaanbevolen reinigingstechnieken en met eenfrequentie aangepast aan de verschillendeogenblikken van activiteit
bull Het werk dient te geschieden met onderlegdgevormd gemotiveerd en gecontroleerdpersoneel
Aanbevelingen voor het plaatsen van cathetersbereiding en gebruik van anestheticabull Men dient bij het plaatsen van catheters
(vasculaire ruggenmerg) de regels van dehuidontsmetting in acht te nemen wassen met eenontsmettende zeep spoelen (af)drogen en gebruikmaken van een ontsmettingsmiddel (van dezelfdesoort als de zeep) vanuit het middelste gedeeltenaar de periferie toe Niet afscheren met eenscheermes indien nodig verkiest men het epilerenof scheren met een scheerapparaat
bull Men trekt een steriele overjas aan bij de plaatsingvan een centraal veneuze catheter Dit geldteveneens bij de plaatsing van een catheter voorloco-regionale anesthesie
bull Men dient steriliteitregels in acht te nemen voor deontsmetting van flacondoppen voor perfusie ofanesthetica Dit geldt trouwens ook voor demanipulatie van driewegkranen
bull Men dient elke vorm van loco-regionaleanesthesie te vermijden in geval vanveralgemeende en bewezen sepsis en bij deaanwezigheid van infectieuze huidletsels terhoogte van de punctieplaatsMen dient de injectiespuiten tussen tweeopeenvolgende patieumlnten helemaal te vervangen(zelfs als de toediening van de anesthetica gebeurtvia een pompsysteem Dit geldt trouwens ookvoor de verlengleidingen) Het is niet voldoendevan enkel de naalden of een onderdeel van de
spuit te vervangen Indien de anesthetica viaperfusie toegediend worden dient men voor elkepatieumlnt zowel de perfusieleiding als de perfusiefleste vervangen
Aanbevelingen voor de behandeling van medischehulpmiddelenbull Het wegwerp materieel mag niet opnieuw
gebruikt wordenbull Voor anesthesie dient men enkel gebruik te maken
van gedecontamineerd en gereinigd materieelVervolgens dient men de benodigdheden teontsmetten of te steriliseren volgens devoorgeschreven procedure voor medischmaterieel in functie van aard en categorie van hetmateriaal
bull Om de kans ARI minimaal te houden dient mentijdens de verzorging de richtlijnen op te volgendie handelen over het contact van medischehulpmiddelen met weefsel met een verhoogdbesmettingsrisico door NCOP (omzendbriefDGS5CDHOSE22001138 van 14 maart 2001)
bull Men dient bij elke patieumlnt gebruik te maken vaneen antibacterieumlle- en antivirale filter die geplaatstwordt op het Y-vormig tussenstuk Dit is nodig omhet potentieumlle risico op kruisbesmetting tevoorkomen en ook om het beheer van devervanging van de anesthesiecircuits teverbeteren
Specifieke aanbevelingenbull Men dient de richtlijnen die toegepast worden
voor de andere vormen van nosocomiale infectiesin acht te nemen
bull Men dient isolatietechnieken verder toe te passenbij dragers van multiresistente kiemen inhoofdzaak door de voorzorgen bij het contact inacht te nemenPatieumlnten met tuberculose of verdacht vantuberculose dienen in isolatie beademd teworden
Aanbevelingen voor verblijf op de dagrecoverybull Men dient de richtlijnen die van toepassing zijn
voor de dagrecovery en die betrekking hebben opde situering (gelegen binnen of buiten hetoperatiekwartier) zodanig toe te passen dat hetrechtstreeks verkeer van zowel patieumlnten alspersoneel tussen het operatiekwartier en deverpleegeenheid vermeden wordt
bull Met dient er voor te zorgen dat er op dedagrecovery voldoende watervoorzieningspuntenbeschikbaar zijn maar voldoende verwijderd vanelke plaats waar zorgen toegediend worden om
N O S O - i n f o v o l V I n deg 1 2 0 0 2
6
besmettingen door aeumlrosolvorming te voorkomenbull Men dient de dagrecovery volgens dezelfde
procedures te onderhouden als de operatiezaalHet is echter niet aangewezen om het materieel tereinigen binnen de ruimte van de dagrecovery
Besluit
Het multifactorieel karakter van infecties bij degeopereerde patieumlnt stelt dat alle bewezenmaatregelen op het vlak van chirurgie en anesthesiemoet worden gevolgd (22-24) Wat deze laatstebetreft verklaart de moeilijkheid van een becijferderelatie tussen de ARI enerzijds en de gangbarepraktijken in de anesthesie anderzijds (25) demiskenning van het probleem door hetanesthesiepersoneelEen toepassing van de aanbevelingen gebeurt inverschillende stappen Deze houden in dat men eenpoging doet om kwalitatief betere zorgen toe tedienen Tijdens de opleiding van medisch enparamedisch personeel voor anesthesie wordt hetbesmettingsrisico binnen het operatiekwartierherkend en past men past preventieve maatregelentoe op basis van gevalideerde criteria volgensbeschreven procedures gevolgd door toezicht van deinfectiewaarden Daarna zal een audit vanberoepsmensen de toepassing van deze maatregelenevalueren Een optimale werkorganisatie binnen elkoperatiekwartier toepasselijk op vlak vanwerkbelasting en beschikbare middelen en geldendvoor zowel personeel als materieel is een onmisbaarelement voor het welslagen van deze betrachtingen
Bibliographie
1 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONLa pratique de lrsquoanestheacutesie en France en 1996 Ann Fr AnesthReacuteanim 1998 18 1299-13872 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONRecommandations concernant lrsquohygiegravene en anestheacutesie 1997 22pages3 CENTRE DE COORDINATION DE LA LUTTE CONTRE LESINFECTIONS NOSOCOMIALES DU SUD-EST Guide des bonnespratiques drsquohygiegravene en anestheacutesie Lyon 1996 64 pages4 AMERICAN SOCIETY OF ANESTHESIOLOGISTS Recommen-dations for infection control for the practice of anesthesiologyPark Ridge Illinois 1994 33 pages5 ASSOCIATION OF OPERATING ROOM NURSES Recommen-ded pratices Cleaning and processing anesthesia equipmentAORN J 1991 53 775-7776 OLDS JW KISCH AL EBERLE BJ WILSON JN Pseudomonasaeruginosa respiratory tract infection acquired from a contamina-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
7
ted anesthesia machine Am Rev Respir Dis 1972 105 628-6327 BENNET SN MCNEIL MM BLAND LA ARDUINO MJ VILLA-RINO ME PERROTTA DM Postoperative infections traced tocontamination of an intravenous anesthetic propofol N Engl JMed 1995 333 147-1548 HERWALDT LA POTTINGER J COFFIN SA Nosocomial infec-tions associated with anesthesia In Mayhall CG Ed Hospital epi-demiology and infection control Williams and Wilkins Balti-more 1996 655-6759 GORCE P De Abreu L PANNETIER C Evaluation du risqueinfectieux nosocomial lieacute agrave lrsquoanestheacutesie Abstract R240 37eCongregraves National de la Socieacuteteacute Franccedilaise drsquoAnestheacutesie et deReacuteanimation Paris 199510 HAJJAR J GIRARD R Surveillance des infections nosoco-miales lieacutees agrave lrsquoanestheacutesie Etude multicentrique Ann Fr AnesthReacuteanim 2000 1 47-5311 CHANT K KOCIUBA K MUNRO R CRONE S KEBRIDGE RQUIN J Investigation of possible patient-to-patient transmissionof hepatitis C in a hospital New South Wales Public Health Bul-letin 1994 5 47-5112 HAJJAR J HERNIGOU E GOUIN F Entretien et deacutesinfectiondu mateacuteriel neacutecessaire au controcircle des voies aeacuteriennes et agrave la ven-tilation meacutecanique Ann Fr Anesth Reacuteanim 1998 17 403-40713 MEFFRE C GIRARD R HAJJAR J Le risque de colonisationapregraves pose de catheacuteters veineux peacuteripheacuteriques est-il modifieacute selonlrsquoantiseptique utiliseacute lorsqursquoon applique un protocole en 4 temps HygiegraveneS 1995 9 4514 TREPANIER CA LESSARD MR BROCHU JG DENAULT PHRisk of cross-infection related to multiple use of disposablesyringes Can J Anaesth 1990 37 156-15915 ANONYME Changer drsquoaiguille et pas de seringue une pra-tique dangereuse BEH 1988 1 1-216 WEDEL DJ HERLOCKER TT Risks of regional anesthesia-infectious septic Reg Anesthes 1996 21(6) 57-6117 AUBOYER C Risque infectieux et anestheacutesie loco-reacutegionaleAnn Fr Anesth Reacuteanim 1998 17 1257-126018 MARSAUDON E BERTHIER F Meacuteningite agrave Staphylococcusaureus apregraves anestheacutesie peacuteridurale obsteacutetricale Ann Fr AnesthReacuteanim 1996 15 389-39019 HOLT HM ANDERSON SS ANDERSON O GARHN-HAN-SEN B SIBONI K Infection following epidural catheterization JHosp Infect 1995 30 253-26020 GARDEN JM OrsquoBANNION MK SHELNITZ LS ET AL Papil-loma virus in the vapor of carbon dioxide Laser-treated verrucaeJAMA 1988 8 1199-120221 LOT F DE BENOIST AC ABITEBOUL D Infections profes-sionnelles par le VIH en France chez le personnel de santeacute Lepoint au 30 juin 1998 BEH 1999 18 69-7022 BIMAR MC HAJJAR J POTTECHER B Risque infectieux noso-comial en anestheacutesie Recommandations geacuteneacuterales Ann fr AnesthReacuteanim 1998 17 392-40223 KORINEK AM Recommandations pour la pose des abordsvasculaires au bloc opeacuteratoire Voies veineuses et voies arteacuteriellespeacuteripheacuteriques Ann Fr Anesth Reacuteanim 1998 17 1250-125224 VEBER B Manipulation des agents anestheacutesiques et desseringues Recommandations et argumentations Ann Fr AnesthReacuteanim 1998 17 1253-125625 TAIT AR TUTTLE DB Preventing perioperative transmissionof infection a survey of anesthesiology practice Anesth Analg1995 80 764-769
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

besmettingen door aeumlrosolvorming te voorkomenbull Men dient de dagrecovery volgens dezelfde
procedures te onderhouden als de operatiezaalHet is echter niet aangewezen om het materieel tereinigen binnen de ruimte van de dagrecovery
Besluit
Het multifactorieel karakter van infecties bij degeopereerde patieumlnt stelt dat alle bewezenmaatregelen op het vlak van chirurgie en anesthesiemoet worden gevolgd (22-24) Wat deze laatstebetreft verklaart de moeilijkheid van een becijferderelatie tussen de ARI enerzijds en de gangbarepraktijken in de anesthesie anderzijds (25) demiskenning van het probleem door hetanesthesiepersoneelEen toepassing van de aanbevelingen gebeurt inverschillende stappen Deze houden in dat men eenpoging doet om kwalitatief betere zorgen toe tedienen Tijdens de opleiding van medisch enparamedisch personeel voor anesthesie wordt hetbesmettingsrisico binnen het operatiekwartierherkend en past men past preventieve maatregelentoe op basis van gevalideerde criteria volgensbeschreven procedures gevolgd door toezicht van deinfectiewaarden Daarna zal een audit vanberoepsmensen de toepassing van deze maatregelenevalueren Een optimale werkorganisatie binnen elkoperatiekwartier toepasselijk op vlak vanwerkbelasting en beschikbare middelen en geldendvoor zowel personeel als materieel is een onmisbaarelement voor het welslagen van deze betrachtingen
Bibliographie
1 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONLa pratique de lrsquoanestheacutesie en France en 1996 Ann Fr AnesthReacuteanim 1998 18 1299-13872 SOCIETE FRANCAISE DrsquoANESTHESIE ET DE REANIMATIONRecommandations concernant lrsquohygiegravene en anestheacutesie 1997 22pages3 CENTRE DE COORDINATION DE LA LUTTE CONTRE LESINFECTIONS NOSOCOMIALES DU SUD-EST Guide des bonnespratiques drsquohygiegravene en anestheacutesie Lyon 1996 64 pages4 AMERICAN SOCIETY OF ANESTHESIOLOGISTS Recommen-dations for infection control for the practice of anesthesiologyPark Ridge Illinois 1994 33 pages5 ASSOCIATION OF OPERATING ROOM NURSES Recommen-ded pratices Cleaning and processing anesthesia equipmentAORN J 1991 53 775-7776 OLDS JW KISCH AL EBERLE BJ WILSON JN Pseudomonasaeruginosa respiratory tract infection acquired from a contamina-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
7
ted anesthesia machine Am Rev Respir Dis 1972 105 628-6327 BENNET SN MCNEIL MM BLAND LA ARDUINO MJ VILLA-RINO ME PERROTTA DM Postoperative infections traced tocontamination of an intravenous anesthetic propofol N Engl JMed 1995 333 147-1548 HERWALDT LA POTTINGER J COFFIN SA Nosocomial infec-tions associated with anesthesia In Mayhall CG Ed Hospital epi-demiology and infection control Williams and Wilkins Balti-more 1996 655-6759 GORCE P De Abreu L PANNETIER C Evaluation du risqueinfectieux nosocomial lieacute agrave lrsquoanestheacutesie Abstract R240 37eCongregraves National de la Socieacuteteacute Franccedilaise drsquoAnestheacutesie et deReacuteanimation Paris 199510 HAJJAR J GIRARD R Surveillance des infections nosoco-miales lieacutees agrave lrsquoanestheacutesie Etude multicentrique Ann Fr AnesthReacuteanim 2000 1 47-5311 CHANT K KOCIUBA K MUNRO R CRONE S KEBRIDGE RQUIN J Investigation of possible patient-to-patient transmissionof hepatitis C in a hospital New South Wales Public Health Bul-letin 1994 5 47-5112 HAJJAR J HERNIGOU E GOUIN F Entretien et deacutesinfectiondu mateacuteriel neacutecessaire au controcircle des voies aeacuteriennes et agrave la ven-tilation meacutecanique Ann Fr Anesth Reacuteanim 1998 17 403-40713 MEFFRE C GIRARD R HAJJAR J Le risque de colonisationapregraves pose de catheacuteters veineux peacuteripheacuteriques est-il modifieacute selonlrsquoantiseptique utiliseacute lorsqursquoon applique un protocole en 4 temps HygiegraveneS 1995 9 4514 TREPANIER CA LESSARD MR BROCHU JG DENAULT PHRisk of cross-infection related to multiple use of disposablesyringes Can J Anaesth 1990 37 156-15915 ANONYME Changer drsquoaiguille et pas de seringue une pra-tique dangereuse BEH 1988 1 1-216 WEDEL DJ HERLOCKER TT Risks of regional anesthesia-infectious septic Reg Anesthes 1996 21(6) 57-6117 AUBOYER C Risque infectieux et anestheacutesie loco-reacutegionaleAnn Fr Anesth Reacuteanim 1998 17 1257-126018 MARSAUDON E BERTHIER F Meacuteningite agrave Staphylococcusaureus apregraves anestheacutesie peacuteridurale obsteacutetricale Ann Fr AnesthReacuteanim 1996 15 389-39019 HOLT HM ANDERSON SS ANDERSON O GARHN-HAN-SEN B SIBONI K Infection following epidural catheterization JHosp Infect 1995 30 253-26020 GARDEN JM OrsquoBANNION MK SHELNITZ LS ET AL Papil-loma virus in the vapor of carbon dioxide Laser-treated verrucaeJAMA 1988 8 1199-120221 LOT F DE BENOIST AC ABITEBOUL D Infections profes-sionnelles par le VIH en France chez le personnel de santeacute Lepoint au 30 juin 1998 BEH 1999 18 69-7022 BIMAR MC HAJJAR J POTTECHER B Risque infectieux noso-comial en anestheacutesie Recommandations geacuteneacuterales Ann fr AnesthReacuteanim 1998 17 392-40223 KORINEK AM Recommandations pour la pose des abordsvasculaires au bloc opeacuteratoire Voies veineuses et voies arteacuteriellespeacuteripheacuteriques Ann Fr Anesth Reacuteanim 1998 17 1250-125224 VEBER B Manipulation des agents anestheacutesiques et desseringues Recommandations et argumentations Ann Fr AnesthReacuteanim 1998 17 1253-125625 TAIT AR TUTTLE DB Preventing perioperative transmissionof infection a survey of anesthesiology practice Anesth Analg1995 80 764-769
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
N O S O - i n f o v o l V I n deg 1 2 0 0 2
8
2001 Veneuze Space OdysseyhellipHoever staan we in de praktijk Cooumlrdinatie BVZH afdeling verpleegkundigenWerkgroep uit Charleroi (Belgieuml)
F Cheron (CHU Charleroi) AM Chevalier (CHU Charleroi) J Daix (CHR Val de Sambre) N Laurent (Hocircpital de Braine lrsquoAlleud) VSchamroth (CHU Charleroi) A Spettante (Saint Joseph Gilly) G Vilain (CH Hornu)Biostatisici M Braeckman en C Kwitonda (CHU Charleroi)
ORIGINELE ARTIKEL
In het kader van een kwaliteitsproject dat in 1996werd voorgesteld door de verpleegkundigen van deBelgische Vereniging voor Ziekenhuishygieumlne (BVZH)leek het ons interessant de handelingen met perifereveneuze catheters binnen de muren van de Franstaligeinstellingen op te volgen Dit gebeurde na publicatievan de richtlijnen door de Hoge Raad voor Hygieumlnegebaseerd op de aanbevelingen van het CDCDeze studie vond plaats in 1999 EenentwintigFranstalige ziekenhuisinstellingen hebben aan dezemulticentrische studie meegewerkt
MaterieelDe studiegroep had voor het registreren van degegevens een rooster samengesteld met daarin 24vooraf gedefinieerde criteria Dit geheel werd uitgetestin 10 ziekenhuizen Na de nodige aanpassingen envalideringen werd er voor elke verpleegkundige-hygieumlnist door de BVZH een praktischeinitiatievergadering georganiseerd ombetrouwbaarheid en reproduceerbaarheid van deregistratie uit te testen De prevalentiestudie werd dusuitgevoerd door verpleegkundigen-hygieumlnisten uit dedeelnemende centra De gegevens werdengeregistreerd met EPI INFO 64 en verder verwerkt metACCESS door een cel bestaande uit biostatistici Elkeinstelling heeft naast haar eigen resultaten ook deglobale resultaten van de studie ontvangen
MethodeDe enquecircteurs evalueerden de voorzieningen (catheterverbanden leidingen en hoofdfles) en dus niet dezorgverstrekking als dusdanig (veneuze punctiecatheterverwisseling verschillende handelingen) Dedoelgroep bestond uit patieumlnten met eacuteeacuten of meerderecatheters tijdens de aanwezigheid van de enquecircteursDe diensten en verpleegeenheden begrepen in destudie waren de diensten voor heelkunde internegeriatrie de intensieve zorgen en de pediatrie
ResultatenDe gegevens afkomstig van de 21 Franstaligeziekenhuisinstellingen werden gerangschikt volgensgrootte en zijn weergegeven in de hiernavolgendetabel
We hebben 1425 gegevens ontvangen waarvan 1229geldig
De gemiddelde verblijfsduur van de opstelling wasonafhankelijk van de omvang van het ziekenhuis enwas vrij homogeen van 611 uur voor instellingen metmeer dan 500 bedden tot 632 uur (globaalgemiddelde 618 uur
Uit de bekomen resultaten blijkt de gemiddeldeverblijfsduur van catheters 618 uur te zijnIn verhouding tot de aanbevolen verblijfsduur van 72uur werd dit criterium in 245 van de gevallenoverschreden
In 426 van de gevallen werd gebruik gemaakt vaneen ondoorschijnend verband 481 opteerden vooreen doorzichtig type van verband en in 93 van degevallen werd het verband omwonden zodat menvisueel geen onderscheid kon maken
De verblijfsduur van een doorzichtig verband bedroeg405 uur en voor een ondoorschijnend verband 456uur
Wat de relatieve criteria betreft werd er bepaald datmen te maken had met een verband van goede kwaliteitindien het verband niet bevuild en niet losgekomen wasen correct aangebracht was Aan dit criterium werd in236 van de gevallen niet voldaan
Over het algemeen is het verband beter gefixeerd bijeen doorzichtig type (955 van de gevallen) dan bijeen ondoorschijnend type (826) Wat de volledigafdekkende eigenschap betreft is de situatie analoog
Kwaliteitsevaluatie van perifere veneuze catheters een multicentriche in franstalig Belgieuml
Omvang
lt250 bedden
250 tot 500 bedden
gt500 bedden
Aantal
5
11
5
Procenten
238
523
238
Tabel 1
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
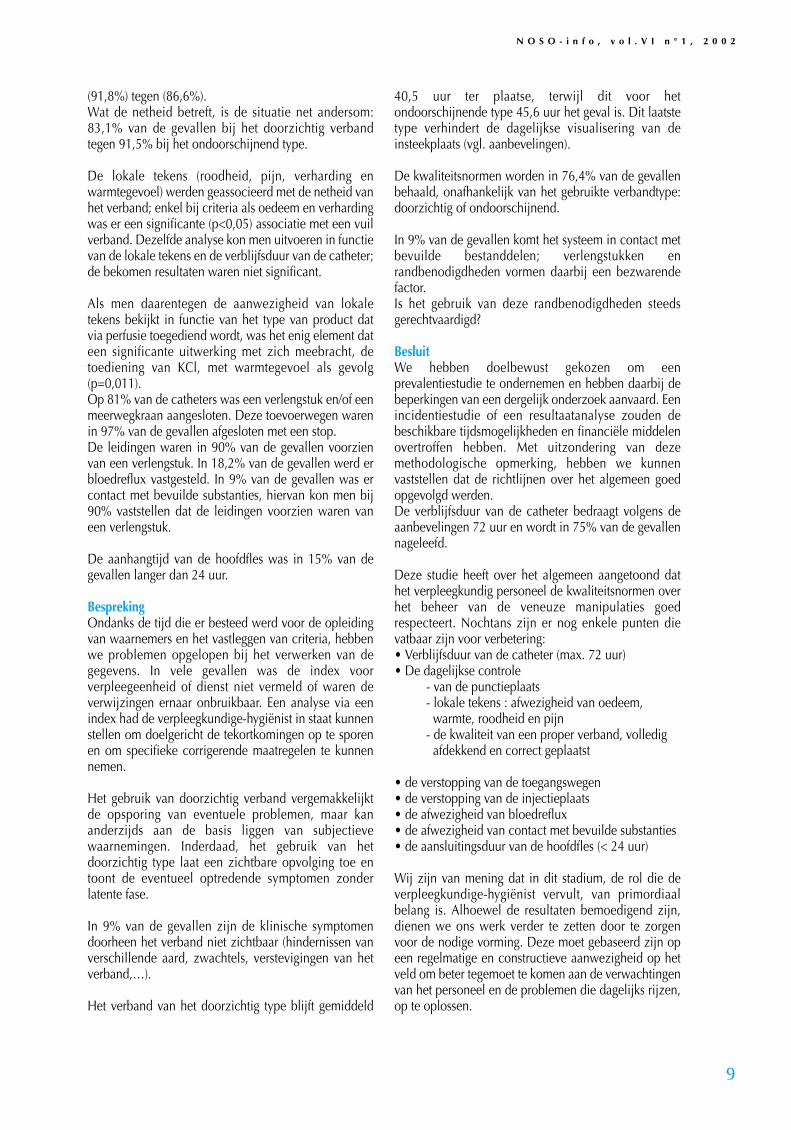
N O S O - i n f o v o l V I n deg 1 2 0 0 2
9
(918) tegen (866)Wat de netheid betreft is de situatie net andersom831 van de gevallen bij het doorzichtig verbandtegen 915 bij het ondoorschijnend type
De lokale tekens (roodheid pijn verharding enwarmtegevoel) werden geassocieerd met de netheid vanhet verband enkel bij criteria als oedeem en verhardingwas er een significante (plt005) associatie met een vuilverband Dezelfde analyse kon men uitvoeren in functievan de lokale tekens en de verblijfsduur van de catheterde bekomen resultaten waren niet significant
Als men daarentegen de aanwezigheid van lokaletekens bekijkt in functie van het type van product datvia perfusie toegediend wordt was het enig element dateen significante uitwerking met zich meebracht detoediening van KCl met warmtegevoel als gevolg(p=0011)Op 81 van de catheters was een verlengstuk enof eenmeerwegkraan aangesloten Deze toevoerwegen warenin 97 van de gevallen afgesloten met een stopDe leidingen waren in 90 van de gevallen voorzienvan een verlengstuk In 182 van de gevallen werd erbloedreflux vastgesteld In 9 van de gevallen was ercontact met bevuilde substanties hiervan kon men bij90 vaststellen dat de leidingen voorzien waren vaneen verlengstuk
De aanhangtijd van de hoofdfles was in 15 van degevallen langer dan 24 uur
BesprekingOndanks de tijd die er besteed werd voor de opleidingvan waarnemers en het vastleggen van criteria hebbenwe problemen opgelopen bij het verwerken van degegevens In vele gevallen was de index voorverpleegeenheid of dienst niet vermeld of waren deverwijzingen ernaar onbruikbaar Een analyse via eenindex had de verpleegkundige-hygieumlnist in staat kunnenstellen om doelgericht de tekortkomingen op te sporenen om specifieke corrigerende maatregelen te kunnennemen
Het gebruik van doorzichtig verband vergemakkelijktde opsporing van eventuele problemen maar kananderzijds aan de basis liggen van subjectievewaarnemingen Inderdaad het gebruik van hetdoorzichtig type laat een zichtbare opvolging toe entoont de eventueel optredende symptomen zonderlatente fase
In 9 van de gevallen zijn de klinische symptomendoorheen het verband niet zichtbaar (hindernissen vanverschillende aard zwachtels verstevigingen van hetverbandhellip)
Het verband van het doorzichtig type blijft gemiddeld
405 uur ter plaatse terwijl dit voor hetondoorschijnende type 456 uur het geval is Dit laatstetype verhindert de dagelijkse visualisering van deinsteekplaats (vgl aanbevelingen)
De kwaliteitsnormen worden in 764 van de gevallenbehaald onafhankelijk van het gebruikte verbandtypedoorzichtig of ondoorschijnend
In 9 van de gevallen komt het systeem in contact metbevuilde bestanddelen verlengstukken enrandbenodigdheden vormen daarbij een bezwarendefactorIs het gebruik van deze randbenodigdheden steedsgerechtvaardigd
BesluitWe hebben doelbewust gekozen om eenprevalentiestudie te ondernemen en hebben daarbij debeperkingen van een dergelijk onderzoek aanvaard Eenincidentiestudie of een resultaatanalyse zouden debeschikbare tijdsmogelijkheden en financieumlle middelenovertroffen hebben Met uitzondering van dezemethodologische opmerking hebben we kunnenvaststellen dat de richtlijnen over het algemeen goedopgevolgd werdenDe verblijfsduur van de catheter bedraagt volgens deaanbevelingen 72 uur en wordt in 75 van de gevallennageleefd
Deze studie heeft over het algemeen aangetoond dathet verpleegkundig personeel de kwaliteitsnormen overhet beheer van de veneuze manipulaties goedrespecteert Nochtans zijn er nog enkele punten dievatbaar zijn voor verbeteringbull Verblijfsduur van de catheter (max 72 uur)bull De dagelijkse controle
- van de punctieplaats - lokale tekens afwezigheid van oedeem warmte roodheid en pijn
- de kwaliteit van een proper verband volledig afdekkend en correct geplaatst
bull de verstopping van de toegangswegenbull de verstopping van de injectieplaatsbull de afwezigheid van bloedrefluxbull de afwezigheid van contact met bevuilde substantiesbull de aansluitingsduur van de hoofdfles (lt 24 uur)
Wij zijn van mening dat in dit stadium de rol die deverpleegkundige-hygieumlnist vervult van primordiaalbelang is Alhoewel de resultaten bemoedigend zijndienen we ons werk verder te zetten door te zorgenvoor de nodige vorming Deze moet gebaseerd zijn opeen regelmatige en constructieve aanwezigheid op hetveld om beter tegemoet te komen aan de verwachtingenvan het personeel en de problemen die dagelijks rijzenop te oplossen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
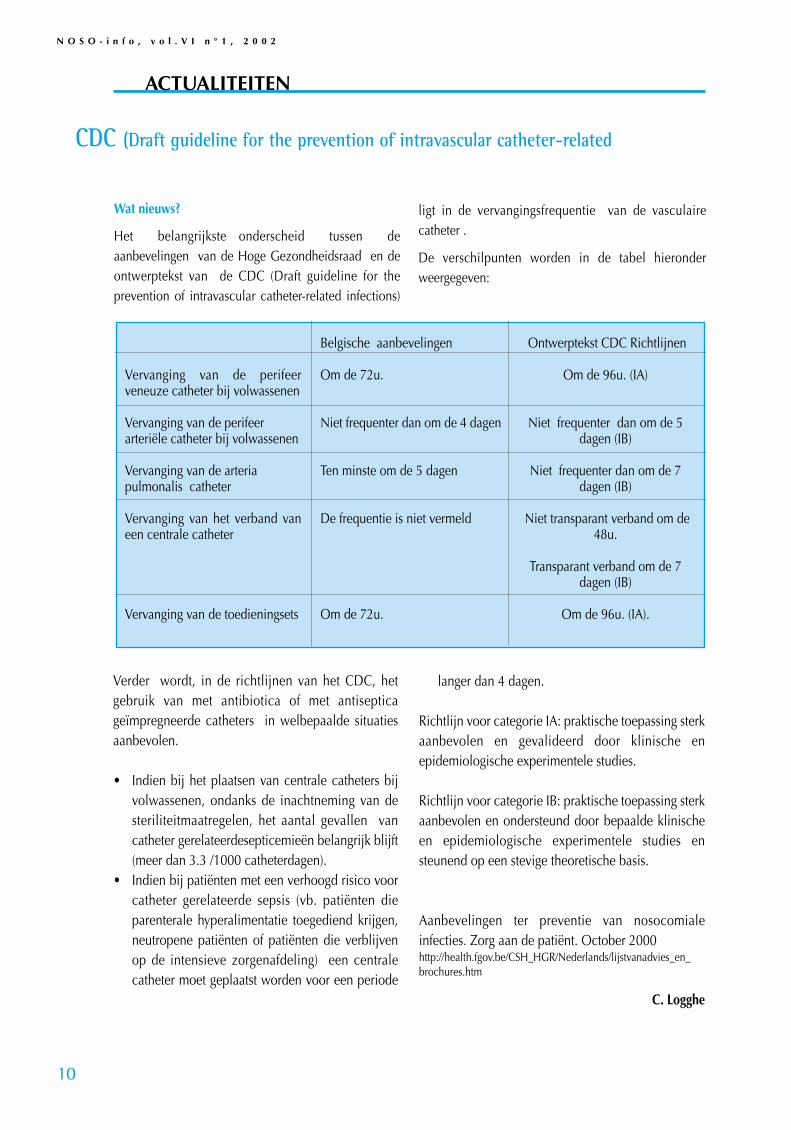
N O S O - i n f o v o l V I n deg 1 2 0 0 2
10
Wat nieuws
Het belangrijkste onderscheid tussen deaanbevelingen van de Hoge Gezondheidsraad en deontwerptekst van de CDC (Draft guideline for theprevention of intravascular catheter-related infections)
ligt in de vervangingsfrequentie van de vasculairecatheter
De verschilpunten worden in de tabel hieronderweergegeven
CDC (Draft guideline for the prevention of intravascular catheter-related
ACTUALITEITEN
Belgische aanbevelingen
Om de 72u
Niet frequenter dan om de 4 dagen
Ten minste om de 5 dagen
De frequentie is niet vermeld
Om de 72u
Ontwerptekst CDC Richtlijnen
Om de 96u (IA)
Niet frequenter dan om de 5dagen (IB)
Niet frequenter dan om de 7dagen (IB)
Niet transparant verband om de48u
Transparant verband om de 7dagen (IB)
Om de 96u (IA)
Vervanging van de perifeerveneuze catheter bij volwassenen
Vervanging van de perifeer arterieumlle catheter bij volwassenen
Vervanging van de arteria pulmonalis catheter
Vervanging van het verband vaneen centrale catheter
Vervanging van de toedieningsets
Verder wordt in de richtlijnen van het CDC hetgebruik van met antibiotica of met antisepticageiumlmpregneerde catheters in welbepaalde situatiesaanbevolen
bull Indien bij het plaatsen van centrale catheters bijvolwassenen ondanks de inachtneming van desteriliteitmaatregelen het aantal gevallen vancatheter gerelateerdesepticemieeumln belangrijk blijft(meer dan 33 1000 catheterdagen)
bull Indien bij patieumlnten met een verhoogd risico voorcatheter gerelateerde sepsis (vb patieumlnten dieparenterale hyperalimentatie toegediend krijgenneutropene patieumlnten of patieumlnten die verblijvenop de intensieve zorgenafdeling) een centralecatheter moet geplaatst worden voor een periode
langer dan 4 dagen
Richtlijn voor categorie IA praktische toepassing sterkaanbevolen en gevalideerd door klinische enepidemiologische experimentele studies
Richtlijn voor categorie IB praktische toepassing sterkaanbevolen en ondersteund door bepaalde klinischeen epidemiologische experimentele studies ensteunend op een stevige theoretische basis
Aanbevelingen ter preventie van nosocomialeinfecties Zorg aan de patieumlnt October 2000httphealthfgovbeCSH_HGRNederlandslijstvanadvies_en_brochureshtm
C Logghe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
11
Inleiding
Sinds januari 2000 verplicht het Kwaliteitsdecreet(KD) van de Vlaamse Gemeenschap de ziekenhuizen3 indicatoren te verzamelen onder het themaziekenhuisinfecties nosocomiale septicemieeumlnventilator-geassocieerde pneumonieeumln en post-operatieve wondinfecties De registratie van elkeindicator dient om de drie jaar gedurende 6 maandente worden uitgevoerd
Bij het uitwerken van de modaliteiten van het KDwerd er gestreefd naar een samenwerking met desinds 1992 lopende nationale surveillance vanziekenhuisinfecties (NSIH) van het WetenschappelijkInstituut Volksgezondheid Bij deelname aan NSIHontvangt het ziekenhuis oa een vertrouwelijkefeedback met de gegevens die vereist zijn in hetkader van het KD Daarbij wordt het ziekenhuisgepositioneerd tov de andere deelnemers(benchmarking) zonder dat de individuele gegevensevenwel door het WIV aan de Vlaamse overheidworden overgemaakt In dit artikel beschrijven we de invloed van de
wijzigingen - die het KD met zich meebracht - aan hetNSIH protocol en aan de algemene context van desurveillance op de incidentie van nosocomialesepticemieeumln
Methoden
De wijziging aan het protocol betreft voornamelijk dedefinitie van nosocomiale septicemieeumln waarbijhuidcontaminanten worden geiumlsoleerd In de NSIHdefinitie worden septicemieeumln met (uitsluitend)huidcontaminanten slechts opgenomen wanneer erbij een patieumlnt met klinische tekens 2 positievehemoculturen worden afgenomen bij 2 afzonderlijkebloednames binnen een periode van 72 uur Om dezedefinitie uit te breiden naar de CDC definitie - die ookdoor het KD gehanteerd wordt - moeten ooksepticemieeumln met slechts eacuteeacuten positieve hemocultuurbij een patieumlnt met een centrale catheter en bijdewelke er een aangepaste antibioticatherapie werdgestart worden geteld Daarnaast werd ook de lijstmet huidcontaminanten aangepast aan de CDC-lijst(zie tabel 1)
Hogere incidentie septicemieen met coagulase-negatievestafylokokken na introductie kwaliteitdecreet in VlaanderenCarl Suetens Eva Leens Ann Versporten Bea Jans Wetenschappelijk Instituut Volksgezondheid
ACTUALITEITEN
NSIH definitie (voacuteoacuter 2000)
-1 pos hemocultuur met erkend pathogeen OF
-2 pos hemoculturen met huidcontaminant (binnen72 uur) + klinische symptomen
(-huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp Streptococci viridansAcinetobacter sp Clostridium sp)
CDCKD definitie
- idem +
- 1 positieve hemocultuur met huidcontaminant bijpatieumlnt met centrale catheter en AB therapie
(- huidcontaminant = CNS Micrococcus spPropionibacterium acnes Bacillus spCorynebacterium sp)
- positieve antigeentest bloed (H influenzaeSpneumoniae Nmeningitidis of Streptococcusgroep B)
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
N O S O - i n f o v o l V I n deg 1 2 0 0 2
12
De gegevens die werden verzameld door hetpersoneel van de dienst ziekenhuishygiumlene werdenter plaatse ingevoerd in de software die daartoe doorhet WIV werd ontwikkeld en verdeeld De variabelen
Om de invloed van het kwaliteitsdecreet te evaluerenwerd een trendanalyse uitgevoerd voor deziekenhuizen die sinds het begin van desepticemiesurveillance (oktober 1992) minstensdriemaal deelnamen aan de perioden okt 1992-jun1994 jul 1994-jun 1996 okt 1998 - dec 1999 en jan2000 - jun 2001 In het totaal werden 73ziekenhuizen ingesloten die gemiddeld 136surveillance-trimesters hadden deelgenomen vanoktober 1992 tot juni 2001 Septicemieeumln waarbij enkel huidcontaminantenwerden geiumlsoleerd met slechts eacuteeacuten positievehemocultuur werden verwijderd uit de analyse Eensepticemie-episode werd als nosocomiaal beschouwdwanneer ze optrad na 2 dagen hospitalisatie of later(infectiedatum - opnamedatum +1 gt 2)
ResultatenVoacuteoacuter 2000 werden de gegevens geregistreerd met deWhocare software Van januari 2000 tot juni 2001werd er in 85 van de surveillance-trimesters gebruikgemaakt van NSIHwin Van de 6072 septicemie-episodes die met NSIHwin werden geregistreerd doorde 73 ziekenhuizen die in de trendanalyse werdenopgenomen werd 11 verwijderd omdat hetsepticemieeumln betrof met slechts eacuteeacuten positieve
hemocultuur van een huidcontaminant (Vlaanderen157 Brussel 18 Wallonieuml 10)
Coagulase-negatieve stafylokokken (CNS)vertegenwoordigden 97 van alle geiumlsoleerdehuidcontaminanten (na correctie) De evolutie van deincidentie nosocomiale septicemieeumln met coagulase-negatieve stafylokokken (aantal septicemie-episodesmet CNS per 10000 ligdagen) wordt weergegeven infiguur 2 De stijging verloopt parallel voor beidelandsdelen tijdens de perioden voacuteoacuter de introductievan het kwaliteitsdecreet en volgt de gelijktijdigestijging in de frequentie van hemocultuurname in dieperiode (aantal hemoculturen per 1000 ligdagen instippellijn) Vanaf 2000 daalt de incidentie inWallonieuml (parallel met een lichte daling in defrequentie van hemocultuurname) terwijl er (ondanksde correctie) een significante stijging optreedt inVlaanderen (en Brussel) Het percentage CNS van hettotaal aantal geiumlsoleerde micro-organismen bedroeg259 in Vlaanderen 190 in Brussel en 165 inWallonieuml In 48 betrof het catheter-geassocieumlerdesepticemieeumln 32 septicemieeumln waren vanongekende oorsprong en in 20 ging het omsepticemieeumln die optraden na een andere infectie ofeen invasieve procedure
in de nieuwe software (NSIHwin vanaf 2000) dietoelaten de resultaten aan te passen aan de vroegeredefinitie zijn in figuur 1 aangeduid door pijltjes
Figuur 1 Scherm uit de NSIHwin software component surveillance nosocomiale septicemieeumln gegevens ivmmicro-organismen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
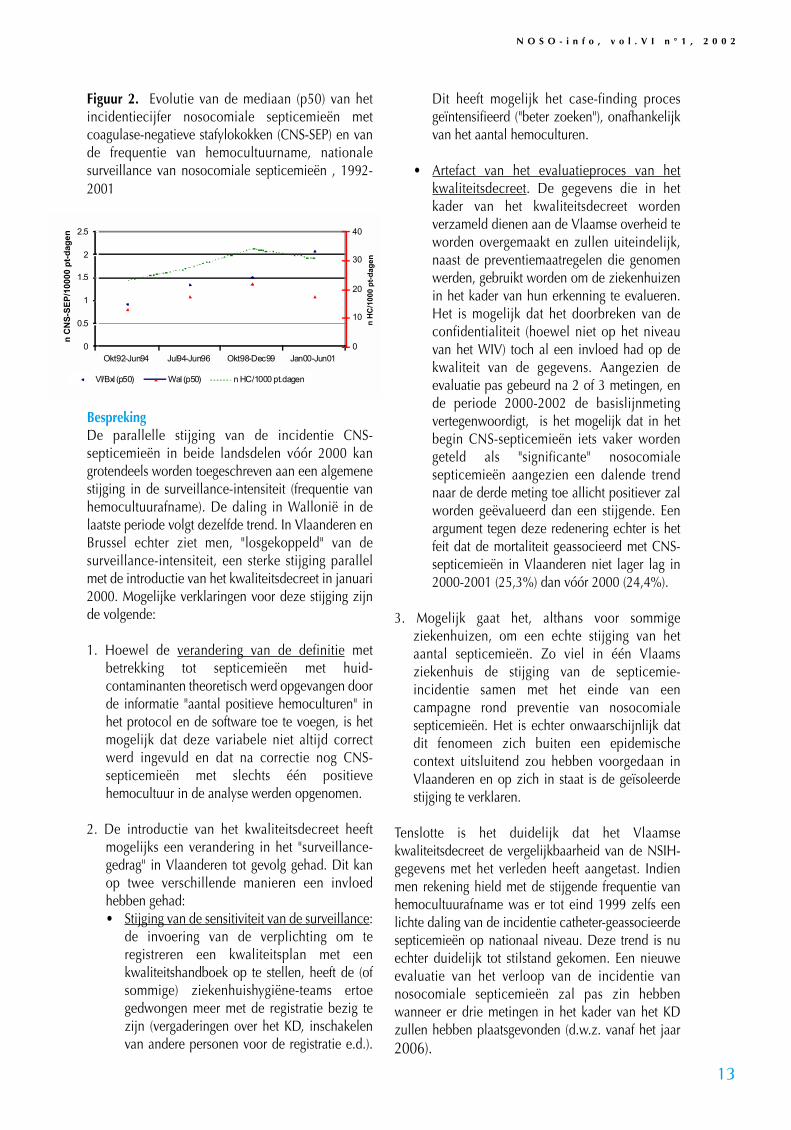
N O S O - i n f o v o l V I n deg 1 2 0 0 2
13
Figuur 2 Evolutie van de mediaan (p50) van hetincidentiecijfer nosocomiale septicemieeumln metcoagulase-negatieve stafylokokken (CNS-SEP) en vande frequentie van hemocultuurname nationalesurveillance van nosocomiale septicemieeumln 1992-2001
BesprekingDe parallelle stijging van de incidentie CNS-septicemieeumln in beide landsdelen voacuteoacuter 2000 kangrotendeels worden toegeschreven aan een algemenestijging in de surveillance-intensiteit (frequentie vanhemocultuurafname) De daling in Wallonieuml in delaatste periode volgt dezelfde trend In Vlaanderen enBrussel echter ziet men losgekoppeld van desurveillance-intensiteit een sterke stijging parallelmet de introductie van het kwaliteitsdecreet in januari2000 Mogelijke verklaringen voor deze stijging zijnde volgende
1 Hoewel de verandering van de definitie metbetrekking tot septicemieeumln met huid-contaminanten theoretisch werd opgevangen doorde informatie aantal positieve hemoculturen inhet protocol en de software toe te voegen is hetmogelijk dat deze variabele niet altijd correctwerd ingevuld en dat na correctie nog CNS-septicemieeumln met slechts eacuteeacuten positievehemocultuur in de analyse werden opgenomen
2 De introductie van het kwaliteitsdecreet heeftmogelijks een verandering in het surveillance-gedrag in Vlaanderen tot gevolg gehad Dit kanop twee verschillende manieren een invloedhebben gehadbull Stijging van de sensitiviteit van de surveillance
de invoering van de verplichting om teregistreren een kwaliteitsplan met eenkwaliteitshandboek op te stellen heeft de (ofsommige) ziekenhuishygieumlne-teams ertoegedwongen meer met de registratie bezig tezijn (vergaderingen over het KD inschakelenvan andere personen voor de registratie ed)
Dit heeft mogelijk het case-finding procesgeiumlntensifieerd (beter zoeken) onafhankelijkvan het aantal hemoculturen
bull Artefact van het evaluatieproces van hetkwaliteitsdecreet De gegevens die in hetkader van het kwaliteitsdecreet wordenverzameld dienen aan de Vlaamse overheid teworden overgemaakt en zullen uiteindelijknaast de preventiemaatregelen die genomenwerden gebruikt worden om de ziekenhuizenin het kader van hun erkenning te evaluerenHet is mogelijk dat het doorbreken van deconfidentialiteit (hoewel niet op het niveauvan het WIV) toch al een invloed had op dekwaliteit van de gegevens Aangezien deevaluatie pas gebeurd na 2 of 3 metingen ende periode 2000-2002 de basislijnmetingvertegenwoordigt is het mogelijk dat in hetbegin CNS-septicemieeumln iets vaker wordengeteld als significante nosocomialesepticemieeumln aangezien een dalende trendnaar de derde meting toe allicht positiever zalworden geeumlvalueerd dan een stijgende Eenargument tegen deze redenering echter is hetfeit dat de mortaliteit geassocieerd met CNS-septicemieeumln in Vlaanderen niet lager lag in2000-2001 (253) dan voacuteoacuter 2000 (244)
3 Mogelijk gaat het althans voor sommigeziekenhuizen om een echte stijging van hetaantal septicemieeumln Zo viel in eacuteeacuten Vlaamsziekenhuis de stijging van de septicemie-incidentie samen met het einde van eencampagne rond preventie van nosocomialesepticemieeumln Het is echter onwaarschijnlijk datdit fenomeen zich buiten een epidemischecontext uitsluitend zou hebben voorgedaan inVlaanderen en op zich in staat is de geiumlsoleerdestijging te verklaren
Tenslotte is het duidelijk dat het Vlaamsekwaliteitsdecreet de vergelijkbaarheid van de NSIH-gegevens met het verleden heeft aangetast Indienmen rekening hield met de stijgende frequentie vanhemocultuurafname was er tot eind 1999 zelfs eenlichte daling van de incidentie catheter-geassocieerdesepticemieeumln op nationaal niveau Deze trend is nuechter duidelijk tot stilstand gekomen Een nieuweevaluatie van het verloop van de incidentie vannosocomiale septicemieeumln zal pas zin hebbenwanneer er drie metingen in het kader van het KDzullen hebben plaatsgevonden (dwz vanaf het jaar2006)
0
05
1
15
2
25
Okt92-Jun94 Jul94-Jun96 Okt98-Dec99 Jan00-Jun01
n C
NS
-SE
P1
0000
pt-
dag
en
0
10
20
30
40
n H
C1
000
pt-
dag
enVlBxl (p50) Wal (p50) n HC1000 ptdagen
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
5PREVENTIE VAN INTRAVASCULAIRE INFECTIES
51 Probleemstelling
Bij ongeveer 30 agrave 50 van de gehospitaliseerde patieumlntenwordt via de intravasculaire weg vocht toegediend Hetintravasculair systeem biedt een directe toegangsweg tot debloedbaan van de patieumlnt voor hemodynamischemonitoring en voor de toedieningvan vocht voedingbloed medicatie of andere componenten waarvoor geenalternatieve toegangswegen mogelijk of effectief zijn
Door het doorbreken van de huidbarriegravere vormt dezebehandeling een belangrijke toegangsweg voor micro-organismen tot debloedbaan Deze micro-organismenkunnen binnendringen via de catheter punctieplaatsvloeistof producten of andere gebruikte materialen enaanleiding geven tot het ontstaan van sepsis die vooral bijeen patieumlnt met verminderde weerstand ernstige gevolgenkan hebben
Bloedbaaninfecties kunnen ook optreden uitgaande vanuiteen besmet orgaan of focus (secundaire infecties)
Deze aanbevelingen zijn gericht op de preventie vaninfecties die te wijten zijn aan de microbieumlle besmettingvan de catheter of de punctieplaats (catheterverwant) endeze te wijten aan de microbieumlle besmetting van detoegediende vloeistof (vloeistofverwant)
52 Algemene aanbevelingen voor het gebruik vanintravasculair materiaal
521 Indicaties Een intravasculaire catheter mag enkel geplaatst worden ofter plaatste gelaten worden op medisch voorschrift
Alternatieve toegangswegen oa enterale toedieningintramusculaire of subcutane injectie dienen overwogen teworden
De indicatie voor een invasieve drukmonitoring moet geletop het infectierisico strikt gesteld worden
522 Handhygieumlne Bij het plaatsen vervangen verzorgen palperenmanipuleren van elk onderdeel van het intravasculairsysteem wordt een correcte handhygieumlne toegepast
Voor het plaatsen van een perifere catheter volstaat hetwassen of het hygieumlnisch ontsmetten van de handen voorhet plaatsen van een centrale catheter is een chirurgischehandontsmetting noodzakelijk
N O S O - i n f o v o l V I n deg 1 2 0 0 2
14
523 Inspectie van de punctieplaats en bewakingElke dag wordt de punctieplaats nagekeken Het volstaatmeestal de punctieplaats doorheen het verband te palperenen de eventuele pijnreactie bij de patieumlnt na te gaan
Het verband wordt dagelijks vervangen indien pijnpalpatieof visuele inspectie onmogelijk is (dik verband comateuzepatieumlnt )
De data van plaatsing van de catheter en verbandwisselingworden steeds in het dossier en eventueel op het verbandgenoteerd
Bij het optreden van koorts van onduidelijke oorsprong ofindien de patieumlnt pijn of een verhoogde gevoeligheid thvde punctieplaats toont wordt het verband verwijderd depunctieplaats onderzocht en zonodig de catheterverwijderd
Indien de cathetertip gekweekt wordt wordt deinsteekplaats voacuteoacuter het verwijderen van de catheter ontsmetmet een alcoholisch ontsmettingsmiddel Na het opdrogenvan de alcohol wordt de tip van de catheter op aseptischewijze afgeknipt met een steriele schaar in een sterielrecipieumlnt gebracht en naar het laboratorium vervoerd om ervervolgens gekweekt te worden
Routinematig worden geen hemoculturen of culturen vanhet intravasculair materiaal genomen
524 Verzorging van de punctieplaats 5241 HuidontsmettingDe huid wordt voacuteoacuter en na de punctie alsook bij de verdereverzorging van de punctieplaats ontsmet met eenalcoholisch ontsmettingsmiddel (joodalcohol 1 of 2chloorhexidine 05 in alcohol 70deg alcohol 70deg of eenjodofoor in een alcoholische oplossing) Hetontsmettingsmiddel moet in voldoende mate aangebrachtworden waarna een contacttijd van minimum 15seconden noodzakelijk is vooraleer de punctie uitgevoerdwordt
Na ontsmetting wordt de punctieplaats niet opnieuwbesmet door palpatie met niet-ontsmette vingers of niet-steriele handschoenen
5242 Catheterzorg en verbandwisselingOm het bewegen van de catheter en bijgevolg de invoervan micro-organismen en irritatie van het bloedvat tevermijden moet de catheter goed gefixeerd wordenKleefpleister die gebruikt wordt ter hoogte van depunctieplaats moet steriel zijn Om tractie op de catheterte voorkomen wordt de infuusleiding buiten het verbandgefixeerd
AANBEVELINGEN
Aanbevelingen van de Hoge Gezondheidsraad httpwwwhealthfgovbeCSH_HGR
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
N O S O - i n f o v o l V I n deg 1 2 0 0 2
15
De punctieplaats wordt na ontsmetting afgedekt met eenvoldoende groot volledig afdekkend en steriel gaas oftransparant verband
Een verband dat inspectie toelaat (bijvoorbeeld transparantverband) kan ter plaatse blijven tot de catheter verwijderdof gewisseld wordt Het verband wordt vroeger vervangenindien het bevuild is vocht onder het verband aanwezig isof indien het onvoldoende bedekt
Bij het verwisselen van het verband wordt besmetting vande insteekpunt vermeden
Indien de catheter in de nabijheid van een besmette wondegelegen is wordt het insteekpunt met een occlusiefverband afgedekt
525 Keuze en vervanging van het intravasculair materiaal
Materiaal met het laagst mogelijk risico op zowelinfectieuze als niet-infectieuze verwikkelingen en aan delaagste kostprijs voor de vooropgestelde indicatie envermoedelijke duur verdient de voorkeur Risico envoordelen van het routinematig herplaatsen van de cathetermoeten afgewogen worden tegenover het risico opmechanische complicaties en de beschikbaarheid van eenalternatieve plaats De keuze van het materiaal en devervangingsfrequentie zijn aan elke patieumlnt aangepast
Het intravasculair materiaal wordt steeds verwijderd zodrade klinische indicatie daartoe vervalt
526 Vervanging van toedieningssets
Een toedieningsset is het geheel van een infuussysteemstartend vanaf de insteekpen van de infuuslijn die in devloeistoffles of zak wordt gebracht tot aan de koppeling metde catheter Een korte verlengleiding aan de catheter laateen gemakkelijke en aseptische wisseling van detoedieningsset toe Men vermijdt daardoor manipulatiesdicht bij de insteekplaats Deze verlengleiding wordtsamen met de catheter verwijderd
De intraveneuze toedieningsset met inbegrip van allezijleidingen en driewegkranen wordt niet eerder dan omde 72 uur vervangen tenzij het klinisch noodzakelijk is
De intraveneuze toedieningsset wordt onmiddellijk na detoediening van bloed bloedderivaten of vetemulsiesverwijderd eacuten ten laatste 24 uur na de start ervanvervangen
Verbindingen tussen de verschillende onderdelen van hetinfuussysteem zijn beveiligd door een luer-lock sluiting
527 Zorg aan de intravasculaire vloeistoffen 5271 Vethoudende vloeistoffenVethoudende parenterale voedingsoplossingen(bijvoorbeeld 3-in-1-oplossing) moeten binnen de 24 uurna ingebruikname toegediend zijn of verwijderd worden
Voor zuivere vetoplossingen gebeurt dit 12 uur na de start
5272 Bloed en bloedderivatenIngeval van bewaring van bloed- of bloedderivaten moet dekoude keten behouden blijven Tussenstadia tussen hetafleveren door het transfusiecentrum of de bloedbank enhet gebruik bij de patieumlnt dienen beperkt te worden
52721 Afname bereiding bewaring en deterhandstelling van bloed en bloedderivatenDe afname bereiding bewaring en de terhandstelling vanbloed en bloedderivaten van menselijke oorsprong werdbepaald in het KB van 04041996 ( BS van 16101997)
52722 Toediening van bloed en bloedderivatenEen eenheid volledig of geconcentreerd bloed die lauw ofwarm aanvoelt of gehemolyseerd is (bruine verkleuring)mag niet worden toegediend maar moet onmiddellijk aande bloedbank worden terugbezorgd Een SOPP-oplossingdie niet helder is mag niet toegediend worden
De toediening van een eenheid bloed moet binnen het uurna het doorbreken van de koude keten aanvatten
Bloedplaatjesconcentraat en bloedplaatjesrijk plasmamoeten bij ontvangst zonder uitstel toegediend worden
Een eenheid bloed mag onmiddellijk na het verwijderen uitde koelkast in 30 minuten toegediend worden Indientransfusie van koele producten heel snel of in grotehoeveelheden moet gebeuren is het gebruik van een(droge) bloedverwarmer onontbeerlijk
De toedieningstijd per eenheid mag de 4 uur nietoverschrijden Wanneer de transfusie tijdelijk onderbrokenwordt (meer dan 2 uur) en hierdoor deze tijdslimietoverschreden wordt moet het bloed verwijderd worden
In geval van een koortsopstoot bij de patieumlnt of een incidentbij de toediening van bloed of bloedderivaten wordt detransfusie onmiddellijk onderbroken Er wordt eenhemocultuur afgenomen op een andere plaats en hetgetransfundeerde bloed wordt voor kweek naar hetlaboratorium voor microbiologie gebracht
528 Intraveneuze injectiepoorten driewegkranen enmanipulaties
Bij elke manipulatie waarbij het gesloten systeem geopendwordt worden beide uiteinden (catheter infuusleidingdriewegkranen) ontsmet met een alcoholischontsmettingsmiddel
Rechtstreekse inspuitingen via de infuusleiding gebeuren inhet daartoe voorzien membraan ter hoogte van deinjectieplaats op de leiding of op de afsluitdop van eendriewegkraan hetzij door punctie met een subcutane naaldhetzij met een naaldvrij systeem
Vooraleer toegang te nemen tot het systeem worden de
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
injectiepoorten met een alcoholisch ontsmettingsmiddelontsmet
Het gebruik van driewegkranen wordt vermeden
De afsluitdop van de driewegkraan wordt enkel verwijderdvoor het aansluiten van een infuusleiding
Bij het niet verder gebruik van de driewegkraan is hetnoodzakelijk een steriele afsluitdop te plaatsen op dedriewegkraan
529 Bereiding en kwaliteitscontrole van intravasculaireoplossingen toevoegingen en materiaalParenterale vloeistoffen (oa TPN) worden in de apotheekbereid in een laminair airflowkast onder aseptischeomstandigheden De bereiding en het bewaren van dezevloeistoffen vallen onder de verantwoordelijkheid van deapotheker
Indien parenterale vloeistoffen niet in idealeomstandigheden bereid worden of indien er nogtoevoegingen aan het infuus gebeuren dan wordt detoediening binnen de 6 uur of na koeling op 4degC binnen de24 uur gestart
Indien mogelijk wordt steeds gebruik gemaakt vaneenheidsdosisverpakkingen voor toevoegingen aanparenterale vloeistoffen of het toedienen van medicatie
Bij gebruik van een multidosisflacon worden volgendevoorzorgsmaatregelen getroffen na het openen van eenmultidosisflacon worden de temperatuur (bewaring bijkamertemperatuur of in de koelkast) en de maximale duurvan de bewaring (bijvoorbeeld 1 week) bepaald in functievan de samenstelling (al dan niet aanwezigheid van eenbewaarmiddel) de datum van het eerste gebruik wordtaangebracht op de flacon de dop van de flacon wordt meteen alcoholische oplossing ontsmet vooraleer deze aan teprikken voor het aanprikken van de flacon wordt sterielmateriaal gebruikt en wordt aseptisch gewerkt eenmultidosisflacon wordt verwijderd bij verdacht of zichtbaarvuil of bij het verstrijken van de vervaldatum
De persoon die een infuus bereidt of toevoegingen doetplaatst een label op het infuus met volgende gegevens deaard en de dosis van toevoeging de datum en het uur devervaldatum en zijn identiteit
Parenterale vloeistoffen en hun recipieumlnten (zak of fles)worden voacuteoacuter gebruik op troebel lekken barsten partikelsen vervaldatum nagezien
Al het materiaal wordt voacuteoacuter gebruik nagezien op deintegriteit van de verpakking en de vervaldatum
De dop van de infuusfles wordt met een alcoholischeoplossing ontsmet
5210 Gebruik van een bacteriefilter
N O S O - i n f o v o l V I n deg 1 2 0 0 2
16
Het systematisch gebruik van een bacteriefilter op hettoedieningssysteem draagt niet bij tot de preventie vaninfecties Indien een filter gebruikt wordt moet hij zo dichtmogelijk bij de catheter geplaatst worden
5211 Antimicrobieumlle profylaxisVoacuteoacuter het plaatsen van een catheter of gedurende deintravasculaire therapie wordt het routinematig toedienenvan antimicrobieumlle middelen ter profylaxis van kolonisatievan de catheter of bloedstroominfectie niet geadviseerd
53 Specifieke aanbevelingen bij het gebruik van perifeerveneuze catheters
531 CatheterkeuzeDe indicatie en de vermoedelijke duur van de therapiebepalen de keuze van de catheter Er wordt een teflon ofpolyurethaan catheter of een naald gebruikt Het gebruikvan catheters in polyethyleen of polyvinylchloride wordtafgeraden
Voor de toediening van vochten of medicatie die in gevalvan extravasatie weefselnecrose veroorzaken wordt hetgebruik van een naald vermeden
Het gebruik van een middenlange catheter (75 tot 20 cm)wordt overwogen als de vermoedelijke duur van deintraveneuze therapie de 6 dagen overschrijdt
532 Keuze van de punctieplaatsBij volwassenen wordt de catheter bij voorkeur in debovenste ledematen (van het distaal naar het proximaaldeel van de arm) geplaatst Van zodra mogelijk wordt eencatheter van de onderste ledematen naar een beschikbaarbloedvat in de bovenste ledematen verplaatst om het risicoop tromboflebitis te verlagen
Bij pediatrische patieumlnten gaat de voorkeur van plaatsingvan de catheter naar de schedel hand of voet Mindergunstige plaatsen zijn de benen armen of deelleboogplooi
Het aanprikken van venen in de nabijheid van gewrichtenwordt vermeden
533 Voorzorgsmaatregelen bij de plaatsing van decatheterBij het plaatsen van een perifere catheter worden (niet-steriele) handschoenen gedragen als algemenevoorzorgsmaatregel
534 Vervanging van de catheterEen perifeer veneuze catheter wordt verwijderd van zodrade patieumlnt tekenen van tromboflebitis of lokale infectie aande insteekplaats vertoont zoals warmte verhoogdegevoeligheid erytheem of een voelbare veneuze streng
Een catheter die in minder gunstige omstandighedengeplaatst is (bijvoorbeeld in urgentie met vermoeden vanfouten in de asepsis) wordt zo snel mogelijk vervangen
N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
17
door een nieuwe catheter op een andere plaats
Een korte perifeer veneuze catheter wordt bij volwassenengewoonlijk na 72 uur verwijderd om het risico vantromboflebitis en infectie te minimaliseren Indien geenandere toegangsweg voorhanden is kan een perifereveneuze catheter langer dan 3 dagen ter plaatse gelatenworden Indien noodzakelijk wordt een nieuwe catheterop een andere perifeer veneuze plaats aangebracht
Bij volwassenen wordt een catheter met heparien slot omde 96 uur vervangen
54 Specifieke aanbevelingen bij gebruik van centraalveneuze en centraal arterieumlle catheter
541 CatheterkeuzeEen centraal veneuze catheter met een enkel lumenverdient de voorkeur tenzij meer lumina nodig zijn voorde behandeling vande patieumlnt
Een parenterale-voedingscatheter met een enkel lumenwordt uitsluitend gebruikt voor het toedienen vanhyperalimentatie
Indien een meerlumencatheter gebuikt wordt voor hettoedienen van parenterale voeding wordt eacuteeacutentoegangsweg gereserveerd voor hyperalimentatie Dezetoegangsweg wordt nooit voor andere doeleinden (oatoedienen van vocht bloed of bloedderivaten) gebruikt
Voor patieumlnten waarbij verwacht wordt dat zij gedurendeeen lange tijd (meer dan 30 dagen) een vasculaire toegangnodig hebben wordt een perifeer geplaatste centraalveneuze catheter een getunneliseerde catheter(bijvoorbeeld Hickman Broviac) of een geiumlmplanteerdevasculaire toegangspoort (bijvoorbeeld Port-a-Cath)gebruikt
542 Keuze van de punctieplaatsDe keuze van de punctieplaats wordt bepaald door hetafwegen van het risico op zowel infectieuze alsmechanische complicaties (bijvoorbeeld pneumothoraxhemothorax het doorprikken van de arteria subclaviabeschadiging van de vena subclavia tromboseluchtembool het verkeerd plaatsten van de catheter)
Bij de plaatsing van een centraal veneuze catheter geeftmen de voorkeur aan de vena subclavia boven de venajugularis of vena femoralis tenzij bij medischetegenindicatie (bijvoorbeeld stollingsstoornissenanatomische afwijkingen)
543 Voorzorgsmaatregelen bij de plaatsing van decatheterBij de plaatsing wordt onder chirurgische omstandighedengewerkt de punctieplaats wordt breed ontsmet met eenalcoholisch ontsmettingsmiddel
De persoon die de punctie uitvoert draagt een steriele
schort steriele handschoenen en een masker hij plaatstgrote steriele velden
Deze voorzorgsmaatregelen worden toegepast bij hetplaatsen van de catheter zowel op het operatiekwartier alsdaarbuiten
544 Vervanging van de catheterBij vermoeden van catheterverwante bacterieumlmie wordt decatheter vervangen en de cathetertip wordt voor kweeknaar het laboratorium gezonden
De centraal veneuze catheter wordt niet routinematigvervangen
Een arteria pulmonalis catheter wordt ten minste om de 5dagen vervangen De catheterinvoerder van de arterieumllecatheter wordt indien mogelijk om de 5 dagen vervangenzelfs indien de catheter verwijderd werd
545 BloednameBloedname via het perfusiesysteem gebeurt slechts indringende gevallen of juist voacuteoacuter de verwijdering van decatheter
55 Specifieke aanbevelingen bij het gebruik van perifeerarterieumlle catheters en drukmonitoringsystemen
551 Keuze van drukmonitoringsysteemHet drukmonitoringsysteem is steriel bij voorkeur vooreenmalig gebruik en in zijn totaliteit samengesteld Indienhet toch uit afzonderlijke bestanddelen samengesteld moetworden dient dit te gebeuren zo kort mogelijk voacuteoacuter deingebruikname
552 Vervanging van de catheter en hetdrukmonitoringsysteemDe arterieumlle catheter en het volledigdrukmonitoringsysteem worden vervangen bij vermoedenvan catheterverwante bacterieumlmie
Bij volwassenen moet de perifeer arterieumlle catheter nietfrequenter dan om de 4 dagen vervangen worden
De transducer wordt om de 4 dagen vervangen Hettoedieningssysteem en de vloeistof worden op hetzelfdeogenblik vervangen
553 Zorg aan het drukmonitoringsysteem5531 Algemene aanbevelingenDe ruimte tussen dome en transducer wordt indien nodiggevuld met steriel water
Het aantal manipulaties en toegangen tot hetdrukmonitoringsysteem worden beperkt
5532 BloednameHet routinematig afnemen van bloed via hetdrukmonitoringsysteem wordt afgeraden tenzij arterieelbloed vereist is
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
N O S O - i n f o v o l V I n deg 1 2 0 0 2
18
ACTUALITEITEN
MINISTERIE VANSOCIALE ZAKEN
VOLKSGEZONDHEID ENLEEFMILIEU
Brussel 12 december 2001
Nota voor Mevrouw Magda AelvoetMinister van ConsumentenzakenVolksgezondheid en Leefmilieu
HOGE GEZONDHEIDSRAAD
Betreft Mondeling verzoek om advies van 15112001 uitgaande van de heer Dr SnackenNr HGR 7626
ADVIES VAN DE HOGE GEZONDHEIDSRAAD BETREFFENDE DE TE VOLGEN HANDELSWIJZE BIJ HOSPITALISATIE VAN EEN VERDACHT
OF BEWEZEN GEVAL VAN POKKEN
Tijdens de buitengewone vergadering van 29 november 2001 waarvan het verslag op 12 december 2001schriftelijk werd goedgekeurd heeft de Hoge Gezondheidsraad (afdeling Hygieumlne in de Gezondheid-szorg Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties) het volgende adviesuitgebracht betreffende de te volgen handelswijze bij hospitalisatie van een verdacht of bewezen gevalvan pokken
Vraag Advies wordt gevraagd met betrekking tot de te volgen handelwijze bij hospitalisatie van een ver-dacht of bewezen geval van pokken
Vraagsteller Deze vraag om advies werd gesteld ter gelegenheid van een buitengewone vergadering van deAfdeling HGR Vaccinaties op 15 november 2001 in de aanwezigheid van een vertegenwoordiger van het kabi-net van de Minister van ConsumentenzakenVolksgezondheid en Leefmilieu
Voorafgaande vaststelling
1 Een geval van pokken wijst vrijwel zeker op een kwaadaardig opzet en zal gevolgd worden door andere primaire ensecundaire gevallen in de nabije omgeving of op andere plaatsen in Belgieuml2 Pokken zijn slechts besmettelijk vanaf het ogenblik dat de huiduitslag zich manifesteert De verspreiding gebeurt face toface dit wil zeggen via de ademhaling of via contact met de huidletsels naar personen in de onmiddellijke omgeving3 Een patieumlnt in het prodromale stadium of bij het begin van de aandoening voelt zich ernstig ziek en zal daardoor ver-moedelijk snel wensen gehospitaliseerd te worden meest waarschijnlijk via de spoedopnamen waar patieumlnt zal toeko-men zonder of slechts met een tentatieve diagnose4 Hospitalisatie is ook medisch noodzakelijk gezien de slechte algemene toestand waarnaar geeumlvolueerd wordt deslechte prognose en de onmogelijkheid om thuis adequaat te isoleren en te verzorgen5 Ringvaccinate dient uitgevoerd te worden binnen de 4 dagen na mogelijke besmetting
N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
19
Advies aan de Minister
1 Bij vermoeden van pokken dient de patieumlnt gehospitaliseerd te worden in een isolatiekamer met sas voorzien van onder-druk Het personeel dient alle voorzorgen in acht te nemen die gangbaar zijn bij de behandeling van een sterk infectieuzepatieumlnt en het gebruikte materiaal dient lege artis behandeld te worden of vernietigd2 Indien dergelijke kamer niet aanwezig is dient een noodsas ingericht te worden De lucht in de kamer mag zich niet vers-preiden in het hospitaal maar dient naar buiten afgevoerd te worden waar verspreiding en verdunning in het milieu moge-lijk wordt Het hospitaal dient zich te realiseren dat een dergelijke opname een belangrijke impact zal hebben om de afde-ling waarin deze kamer ligt3 Bij vermoeden van pokken dient de Provinciale Gezondheidsinspecteur onmiddellijk verwittigd te worden Deze zal eronder meer voor zorgen dat biologische stalen ter bevestiging van de diagnose via de overheid snel terechtkomen in hetaangewezen laboratorium (CDC Atlanta VS) Op deze wijze is ook de overheid verwittigd die bijkomende acties pas-sende in het crisisplan kan ondernemen4 Een snelle bevestiging laat toe om bij verkeerde diagnose snel deze zware isolatiemaatregelen op te heffen Bij bevesti-ging van de diagnose dient ringvaccinatie uitgevoerd te worden De arbeidsgeneeskundige dienst van het hospitaal zal hier-bij betrokken worden Deze vaccinatie zal waarschijnlijk de volgende personen omvatten huisgenoten en huisarts van depatieumlnt ambulance personeel personeelsleden en omstanders aanwezig in de spoedopname bij opname van de patieumlnt enal het personeel van het ziekenhuis dat verder met de patieumlnt of met materiaal afkomstig van de patieumlnt in aanraking zalkomen5 Wat het verzorgingspersoneel betreft wordt de voorkeur gegeven aan vrijwilligers die in hun jeugd reeds een primovac-cinatie tegen pokken hebben gekregen bij hen zullen eventuele nadelige reacties op een hervaccinatie goedaardiger ver-lopen dan bij primovaccinaties bij volwassenen6 Het is aangewezen om bij de eerste gevallen van pokken de patieumlnten op te nemen in een regionaal hospitaal dat overde aangepaste infrastructuur beschikt Het is aan de overheid om deze hospitalen in een lijst op te nemen en met hen meerconcrete afspraken te maken Gezien de besmettelijkheid van pokken zal dit echter naar alle waarschijnlijkheid niet vol-staan en dient bijgevolg elk hospitaal zich voor te bereiden op de mogelijkheid van dergelijke opname
Namens Namens
G Reybrouck J WillemsAfdeling hygiene Werkgroep biologisch enin de gezondheidszorg chemisch terrorisme
De Secretaris Van de Hoge Gezondheidsraad
G Devleeschouwer
Bijlage Totstandkoming advies
Op mondelinge vraag van de heer Dr Snacken Vertegenwoordiger van het Kabinet van Mevrouw de Minister van Consu-mentenzaken Volksgezondheid en Leefmilieu tijdens de vergadering van de Werkgroep Vaccinaties van 15112001 werdop 29112001 een buitengewone vergadering samengeroepen bestaande uit experten van de afdeling Hygieumlne in deGezondheidszorg de Werkgroep Biologisch en Chemisch Terrorisme en de Werkgroep Vaccinaties zodanig dat de opvol-ging van dit dossier volledig werd afgedekt zonder nutteloze overlappingen
RAC ndash Esplanadegebouw 718 Pachecolaan 19 Bus 5 B-1010 BRUSSELTel 022104835Fax 022104655
E-mail guydevleeschouwerhealthfgovbe
N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
20
ABSTRACTS VAN 1STE AUGUSTUS TOT 31 OKTOBER 2001
De samenvattingen van artikels uit de literatuur sedert 1994 met driemaandelijkse actualisatie mogelijkheidtot het opzoeken dank zij sleutelwoorden en laquo downloading raquo zijn ook beschikbaar op het Internet-URL
httpwwwmduclacbedidacintrohtml
Alberti C Bouakline A Ribaud P Lacroix C Rousselot PLeblanc T Derouin F Relationship between environmen-tal fungal contamination and the incidence of invasiveaspergillosis in haematology patients Journal of Hospi-tal Infection 48 198-206 (2001)
NOTES Invasive aspergillosis (IA) is a major opportunis-tic infection in haematology patients Spore inhalation isthe usual route of Aspergillus infection suggesting adetermining role of environmental contamination byspores in the epidemiology of IA We prospectively exa-mined the relationship between environmental contami-nation by Aspergillus and other fungal species and theincidence of invasive nosocomial aspergillosis (INA) in abone marrow transplantation unit and two haematologywards During a four-year period levels of air and surfacefungal contamination were determined bi-monthly inpatients rooms (some equipped with HEPA filters andLAF systems) and various common sites in each ward(corridors nursing stations etc) Results were comparedto the incidence of INA A total of 3100 air and 9800 sur-face samples were collected and 79 cases of IA were dia-gnosed of which 64 were probably or possibly INA Pat-terns of fungal contamination were comparable in thethree wards with a gradient ranging from high levels incommon sites to a virtual absence in rooms equippedwith HEPA filters and LAF systems Using a regressionmodel a significant relationship was found between theincidence of INA and the degree of fungal contaminationof air and surfaces in conventional patient rooms (notequipped with HEPA) and common sites This studyshows that in a non-epidemic setting there is a signifi-cant relationship between environmental fungal contami-nation in haematology wards and the incidence of INAOur findings underline the importance of environmentalsurveillance and strict application of preventive mea-sures
Appelgren P Hellstrom I Weitzberg E Soderlund VBindslev L Ransjo U Risk factors for nosocomial inten-sive care infection a long-term prospective analysisActa anaesthesiologica Scandinavia 45 710-719(2001)
NOTES Background To identify risk factors for nosoco-mial infection in intensive care and to provide a basis forallocation of resources METHODS Long-term prospec-tive incidence study of risk factors for nosocomial infec-tion in the surgical-medical intensive care unit of a uni-versity hospitalResults A total of 2671 patients wereadmitted during four years and 562 of 574 patientsstaying gt 48 h were observed during 4921 patient days(median length of stay 5 days range 2-114) Of these196 (34) patients had 364 nosocomial infections aftermedian 8-10 days an infection rate of 14100 admis-sions infection prolonged length of stay 8-9 days anddoubled the risk of death The infections were 17 bloodstream 26 pneumonias 34 wound 10 urinarytract and 13 other infections The incidence of blood-stream infection declined significantly during the studyyears from 12 to 50 In multiple regression analysis
the important variables for infection were central venouscatheter mechanical ventilation pleural drainage andtrauma with open fractures High age immunosuppres-sion and infection on admission did not influence the riskof acquiring infection Trauma patients constituted 24of the study Population Trauma with open fracturesincreased the risk of infection more than twice (P =0003) mainly due to wound infectionsCONCLUSION Trauma cases with open fractures were the Patients mostat risk of infection despite low disease severity scoresResources to prevent nosocomial infection should beallocated to these patients
Astagneau P Desplaces N Vincent V Chicheportiche VBotherel AH Maugat S Lebascle K Leonard P Desen-clos JC Grosset J Ziza JM Brucker G Mycobacteriumxenopi spinal infections after discovertebral surgeryinvestigation and screening of a large outbreak Lancet358 747-751( 2001)
NOTES Background Mycobacterium xenopi spinalinfections were diagnosed in 1993 in patients who hadundergone surgical microdiscectomy for disc hernia bynucleotomy or microsurgery in a private hospital Conta-minated tap water used for rinsing surgical devices afterdisinfection was identified as the source of the outbreakSeveral cases were recorded in the 4 years after imple-mentation of effective control measures because of thelong time between discectomy and case detection Thenational health authorities decided to launch a retrospec-tive investigation in patients who were exposed to Mxenopi contamination in that hospital METHODS Mai-ling and media campaigns were undertaken concurrentlyto trace exposed patients for spinal infections Patients were screened by magnetic resonance imaging (MRI) andthe scans were reviewed by a radiologist who was una-ware of the diagnosis Suspected cases had discovertebralbiopsy for histopathological and bacteriological exami-nationFindings Of 3244 exposed patients 2971 (92)were informed about the risk of infection and 2454 (76)had MRI Overall 58 cases of M xenopi spinal infectionwere identified (overall cumulative frequency 18)including 26 by the campaign (mean delay in detection52 years SD 24 range 1-10 years) Multivariate analysisshowed that the risk of M xenopi spinal infection wasrelated to nucleotomy and high number of patients peroperating sessionInterpretation Failures in hygiene prac-tices could result in an uncontrolled outbreak of nosoco-mial infection Patients who have been exposed to aniatrogenic infectious hazard should be screened promptlyand receive effective information
Astagneau P Rioux C Golliot F Brucker G Morbi-dity and mortality associated with surgical site infec-tions results from the 1997-1999 INCISO surveillanceJournal of Hospital Infection 48 267-274 (2001)
NOTES Since 1997 a surgical-site infections (SSI) sur-veillance network (INCISO) has been implemented involunteer general surgical units in Northern France Forthree months each year all patients who undergo a surgi-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
21
cal procedure are consecutively reviewed for their peri-operative condition and traced for outcome with a 30-dayfollow-up Of the 38 973 surgical patients included overa three-year period 1344 (34) developed SSI and 568died (15) including 78 with an SSI Organ-space anddeep incisional SSI were associated with a higher morta-lity and required re-operation more frequently than didsuperficial incisional SSI SSI incidence and mortalityvaried according to the surgical procedure SSI was asignificant predictor of mortality independently of NNISrisk index and other survival predictors Thirty-eight percent of deaths in SSI patients were attributable to infec-tion Hence the significant impact of SSI on mortality andmorbidity in surgical patients is now an additional reasonto reinforce compliance of surgical staff with preventivemeasures and hygiene practices
Bar W de Bar GM Naumann A Rusch Gerdes SContamination of bronchoscopes with Mycobacteriumtuberculosis and successful sterilization by low-tempera-ture hydrogen peroxide plasma sterilization AmericanJournal of Infection Control 29 306-311 (2001)
NOTES Background The transmission of mycobacteriaby bronchoscopes has been reported several times in thelast years To explore methods to prevent transmission oftuberculosis in this way we sterilized contaminated bron-choscopes with tow-temperature hydrogen peroxide gasplasma sterilization METHODS Bronchoscopes werecontaminated with Mycobacterium tuberculosis anddecontaminated with a washerdisinfector (normalwashing) Some were additionally disinfected with gluta-raldehyde (intensive washing) Afterward the broncho-scopes were sterilized by low-temperature hydrogen per-oxide plasma sterilization RESULTS After normalwashing 817 samples had positive results by cultureand 717 had positive results by nucleic acid amplifica-tion technique After intensive washing all samples hadnegative results by culture and 1025 had positive resultsby nucleic acid amplification technique after sterilizationwith low-temperature hydrogen peroxide plasma sterili-zation all samples had negative results by culture andnucleic acid amplification techniqueCONCLUSION Washing of bronchoscopes as performed normally is notsufficient for decontamination of bronchoscopes Addi-tional disinfection is recommended If the nucleic acidamplification technique is used for diagnostic proce-dures sterilization by low-temperature hydrogen per-oxide plasma sterilization is recommended to avoid false-positive results
Barbut F Petit JC Epidemiology of Clostridium diffi-cile-associated infections Clinical Microbiology andInfection 7 405-410 (2001)
NOTES Clostridium difficile is responsible for 15-25 ofcases of antibiotic-associated diarrhea (AAD) and for vir-tually all cases of antibiotic-associated pseudomembra-nous colitis (PMC) This anaerobic bacterium has beenidentified as the leading cause of nosocomial infectiousdiarrhea in adults and can be responsible for large out-breaks Nosocomial C difficile infection results in anincreased length of stay in hospital ranging from 8 to 21days Risk factors for C difficile-associated diarrheainclude antimicrobial therapy older-age (gt65 years) anti-neoplastic chemotherapy and length of hospital stayOther interventions with high risk associations are ene-mas nasogastric tubes gastrointestinal surgery and anti-peristaltic drugs Prospective studies have shown that
nosocomial transmission of C difficile is frequent butoften remains asymptomatic Patients can be contamina-ted from environmental surfaces shared instrumentationhospital personnel hands and infected roommates Oncean outbreak starts C difficile may be spread rapidlythroughout the hospital environment where spores maypersist for months Measures that are effective in reducingincidence of C difficile infections and cross-infectioninclude (i) an accurate and rapid diagnosis (ii) appro-priate treatment (iii) implementation of enteric precau-tions for symptomatic patients (iv) reinforcement ofhand-washing (v) daily environmental disinfection and(vi) a restrictive antibiotic policy C difficile is a commoncause of infectious diarrhea and should be therefore sys-tematically investigated in patients with nosocomial diar-rhea
Bergmans DCJJ Bonten MJM Gaillard CAPaling JC van der Geest S van Tiel FH BeysensAJ de Leeuw PW Stobberingh EE Prevention ofventilator-associated pneumonia by oral decontamina-tion - A prospective randomized double-blind placebo-controlled study American Journal of Respiratory andCritical Care Medicine 164 382-388 (2001)
NOTES Colonization of the intestinal tract has beenassumed to be important in the pathogenesis of ventilator-associated pneumonia (VAP) but relative Impacts of oro-pharyngeal gastric or intestinal colonization have notbeen elucidated Our aim was to prevent VAP by modu-lation of oropharyngeal colonization without influencinggastric and Intestinal colonization and without systemicprophylaxis In a prospective randomized placebo-controlled double-blind study 87 patients received topi-cal antimicrobial prophylaxis (gentamicin colistinvanco-mycin 2 in Orabase every 6 h) in the oropharynx and139 patients divided over two control groups receivedplacebo (78 patients were studied in the presence ofpatients receiving topical prophylaxis [control group A]and 61 patients were studied In an intensive care unitwhere no topical prophylaxis was used [control groupB]) Baseline characteristics were comparable in all threegroups Topical prophylaxis eradicated colonization pre-sent on admission in oropharynx (75 in study groupversus 0 in control group A [p lt 000001] and 9 incontrol group B patients [p lt 000001]) and In trachea(52 versus 22 in A [p = 003] and 7 in 8 [p =0004]) Moreover topical prophylaxis prevented acqui-red oropharyngeal colonization (10 versus 59 in A [plt 000001] and 63 in B [p lt 000001]) Colonizationrates In stomach and intestine were not affected Inci-dences of VAP were 10 in study patients 31 in GroupA and 23 in Group B patients (p = 0001 and p = 004respectively) This was not associated with shorter dura-tions of ventilation or ICU stay or better survival Oropha-ryngeal colonization is of paramount importance in thepathogenesis of VAP and a targeted approach to preventcolonization at this site is a very effective method ofinfection prevention
Blunt MC Young PJ Patil A Haddock A Gel lubri-cation of the tracheal tube cuff reduces pulmonary aspi-ration Anesthesiology 95 377-381 (2001)
NOTES BACKGROUND Leakage of fluid occurs alongthe longitudinal folds within the wall of an inflated high-volume low-pressure cuff Theoretically lubrication ofthe cuff with a water-soluble gel might prevent aspirationby plugging the channels in the cuff wall Pulmonary
N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
22
aspiration during anesthesia has been linked with post-operative pneumonia and during critical illness causesventilator-associated pneumonia METHODS Lubricatedcuffs were compared with nonlubricated cuffs for leakageof dye placed in the subglottic space to the tracheobron-chial tree in a benchtop model (n = 5) and in a prospec-tive double-blinded randomized controlled trial of anes-thetized patients (n = 36) The duration of the efficacy ofthe lubricant was determined in a prospective openobservational study of critically ill patients with tracheo-stomies (n = 9) Dye was detected clinically by dye colo-ration of secretions during tracheal suctioning RESULTS In the benchtop model the incidence of leakage was 0in the lubrication group and 100 in the nonlubricationgroup (P lt 001) Dye leakage in anesthetized patientswas 11 in the lubrication group and 83 in the nonlu-brication group (P lt 00001) In the critically ill patientswith lubricated cuffed tracheostomy tubes leakage firstoccurred after a median period of 48 h (range 24-120 h)CONCLUSIONS Cuff lubrication with a water-solublegel reduces pulmonary aspiration in anesthetizedpatients In the critically ill patient with a tracheostomythe protective effect is lost after 24-120 h
Borer A Gilad J Meydan N Riesenberg K Schlaef-fer F Alkan M Schlaeffer P Impact of active monito-ring of infection control practices on deep sternal infec-tion after open-heart surgery Annals of thoracic Surgery 72 515-520 (2001)
Notes Background Deep-sternal infection is a devasta-ting complication after open-heart surgery However theassociation between infection control practices anddeep-sternal infection rates is unclear METHODS Toidentify contributors to increased deep-sternal infectionrates in our institution consecutive open-heart surgerypatients were prospectively studied during two periods(75 and 40 days) including 66 and 40 patients respecti-vely Active monitoring including 149 infection controlpractices was performed in the operating room and inten-sive care unit End-points were deep-sternal infectionrates and their relation to infection control practicesRESULTS Mean age was 62 +- 11 years and 68 weremales Coronary bypass was performed in 82 Clinicaland surgical features were comparable except thatpatients in period 2 were more likely to have heart failure(15 vs 15 p = 001) and had a longer mean durationof surgery (277 vs 217 minutes p lt 0005) Only 57 prac-tices (38) were adequately performed The main cate-gories showing inadequate practices were disinfectiontraffic hand-washing and surgical attire of non-scrubbedpersonnel anesthesiologists and pump techniciansMany categories showed a statistically significant impro-vement between periods Deep-sternal infection rates inprestudy and poststudy periods were 10 and 28 res-pectively (p = 0007) CONCLUSIONS Active monito-ring among personnel involved in open-heart surgeryresulted in a significant and sustained decrease in deep-sternal infection rates through modification of humanbehavior and improvement of performance standardsprobably mediated by the Hawthorne effect Periodicactive monitoring may be a valuable tool to achieve andeven sustain such a decrease with tremendous implica-tions on morbidity costs and quality of care
Boyce JM MRSA patients proven methods to treatcolonization and infection Journal of Hospital Infection48 Suppl A S9-S14 (2001)
NOTES Methicillin-resistant Staphylococcus aureus
(MRSA) infections continue to cause serious nosocomialinfections in many hospitals Measures used to controlthe spread of these infections include ongoing laboratory-based surveillance placing colonized and infectedpatients in isolation use of barrier precautions and hand-washing and hand antisepsis Culturing hospitalizedpatients at high risk of acquiring MRSA can facilitatedetection and isolation of colonized patients EradicatingMRSA nasal colonization among affected patients andhealthcare personnel has also been as a control measurewith variable success Eradicating MRSA nasal carriagefrom epidemiologically-implicated healthcare workershas been used on a number of occasions to control out-breaks Attempts to eradicate MRSA colonization amongaffected patients has proven difficult Of more than 40different decolonization regimens that have been testedduring the last 60 years topical intranasal application ofmupirocin ointment has proven to be the most effectiveHowever intranasal application of mupirocin has limitedeffectiveness in eradicating colonization in patients whocarry the organism at multiple body sites Furthermorebecause decolonization of patients has virtually alwaysbeen used in combination with other control measuresits efficacy has been difficult to determine BecauseMRSA is transmitted primarily on the hands of healthcareworkers greater emphasis should be given to improvinghand hygiene practices among health personnel Forpatients infected with MRSA vancomycin remains a drugof choice
Cadwallader HL Toohey M Linton S Dyson ARiley TV A comparison of two methods for identifyingsurgical site infections following orthopaedic surgeryJournal of Hospital Infection 48 261-266 (2001)
NOTES Many infection control practitioners (ICPs) dedi-cate a significant amount of time and resources to Sur-veillance of surgical site infections (SSIs) Alternative Sur-veillance methods need to be explored to reflect thechanges to the healthcare system and the increasing eco-nomic constraints placed on infection control units Thisstudy was undertaken to compare two methods of identi-fying SSIs in orthopaedic Surgery Surveillance data col-lected routinely by ICPs was compared with data obtai-ned from the International Classification of Disease 9thRevision Clinical Modification (ICD-9-CM) coding in themedical record Concordant results between the twomethods were obtained The use of ICD-9-CM coding asstored in hospital patient administration system data-bases has the ability to enhance routine surgical Site Sur-veillance programmes These systems can be used as thebasis for screening large data sets for SSIs and identifyingwhere SSIs resulted in patient re-admission A reductionin the duplication of data and time spent by the ICP onthe collection of information for Surveillance purposescan be achieved
Eckmanns T Rath A Brauer H Daschner F RudenH Gastmeier P Compliance with hand hygiene inintensive care units Deutsche Medizinische Wochen-schrift 126 745-749 (2001)
NOTES INTRODUCTION Nosocomial infections arean important problem in modern hospitals The preva-lence in German intensive care units is 153 Handwashing or hand disinfection is believed to be the mostimportant means of preventing nosocomial infectionsWe wished to answer the following questions 1 Howgood is the compliance of hand hygiene on intensive careunits 2 Is compliance associated with the patientnurse-
N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
23
ratio METHOD In a study of 8 intensive care units thecompliance of hand hygiene was observed on two occa-sions once in May 1996 and again in November 1997The prime necessity for hand disinfection occurred whenhandling ventilation devices intravascular catheters uri-nary catheters and dressings In addition thepatientnurse-ratio was calculatedResults A total of1879 infection-relevant handlings were observed Thecompliance of hand hygiene ranged from 257 to 832(mean 552) The most commonly observed handlingswere the manipulation of venous catheters (527) thehighest compliance was observed with the manipulationof ventilation equipment (918) With a better patientnurse ratio the compliance did not improve but remainedthe same or was even reduced DISCUSSION The com-pliance of hand disinfection is similar to other studyresults but on some intensive care units there was consi-derable room for improvement In this study the com-pliance of hand hygiene is more of a constant factor inindividual intensive care units than associated with thepatientnurse-ratio
Franzin L Scolfaro C Cabodi D Valera M TovoPA Legionella pneumophila pneumonia in a newbornafter water birth A new mode of transmission ClinicalInfectious Diseases 33 E103-E104 (2001)
NOTES We report a case of Legionella pneumophilapneumonia in a 7-day old neonate Because the hospitalwater and particularly the pool water for water birthingwas contaminated by L pneumophila serogroup 1 thenewborn was infected following prolonged delivery incontaminated water perhaps by aspiration This is thefirst case of nosocomial Legionella pneumonia in neonateafter water birth
Fraud S Maillard JY Russell AD Comparison of themycobactericidal activity of ortho-phthalaldehyde glu-taraldehyde and other dialdehydes by a quantitative sus-pension test Journal of Hospital Infection 48 214-221(2001)
NOTES The mycobactericidal activity of various dialde-hydes has been assessed by a quantitative suspension testin both clean and dirty conditions Test organismsconsisted of glutaraldehyde (GTA)-sensitive strains ofMycobacterium chelonae NCTC 946 M abscessusNCTC 10882 two GTA-resistant M chelonae strains andM terrae NCTC 10856 (a proposed M tuberculosis surro-gate) The aldehydes tested were a new high-level disin-fectant ortho-phthalaldehyde (OPA) at 05 (vv) unad-justed pH 65 and pH 8 GTA at 05 (vv) pH 8 glyoxalat 05 (vv) pH 8 and 10 (vv) unadjusted pn 28malonaldehyde sodium salt (NaMDA) at 05 (wv) pH 8and 10 (wv) unadjusted pH 75 and succinaldehyde at05 (vv) pH 8 Results showed that 05 acidic andalkaline OPA were rapidly mycobactericidal under bothclean and dirty conditions and more importantly wereactive against GTA-resistant strains The washer disinfec-tor isolates of M chelonae were as expected extremelyresistant to 05 GTA which was slowly mycobacterici-dal against the other strains Glyoxal NaMDA and succi-naldehyde were ineffective against all the strains investi-gated However a high concentration of glyoxalexhibited a slow mycobactericidal activity except withM terrae NCTC 10856 but this was not observed withNaMDA This evaluation using a quantitative suspensiontest based on a European standard supported the claimthat OPA is an effective choice as a high-level disinfectantfor medical devices
Hanberger H Diekema D Fluit A Jones R Strue-lens M Spencer R Wolff M Surveillance of antibio-tic resistance in European ICUs Journal of HospitalInfection 48 161-176 (2001)
NOTES Antibiotic resistance among bacteria causinghospital-acquired infections poses a threat particularly topatients in intensive care units (ICUs) In order to controlthe spread of resistant bacteria local regional and natio-nal resistance surveillance data must be used to developefficient intervention strategies In an attempt to identifynational differences and the dynamics of antibiotic resis-tance in European ICUs data have been merged fromseveral networks of resistance surveillance performedduring the 1990s It should be stressed however thatcomparisons of results from different studies using diffe-rent methods and different population samples must bemade with caution Antibiotic resistance across all spe-cies and drugs Tn-as with some exceptions highest insouthern European countries and Russia and lowest inScandinavia More effective strategies are needed tocontrol the selection and spread of resistant organismsAntibiotic intervention policies efficient infection controlmeasures and an overall awareness of the serious impli-cations at public health level will contribute to the mana-gement of antibiotic resistance
Heeg P Does hand care ruin hand disinfection Journalof Hospital Infection 48 Suppl A S37-S39 (2001)
NOTES Hand washing and hand disinfection put consi-derable stress on the skin thus requiring specific handcare It is important however that the care products donot impair the effect of hand disinfectants We thereforeinvestigated the interaction of two hand care products(oil-in-water and water-in-oil emulsions) on the microbi-cidal efficacy of different alcoholic hand-rubs using thecontamination model described in EN 1500 The meanlog(10)-reduction factors for three hand-rubs varied bet-ween 403 and 422 compared with 376 and 443 for sixpossible combinations of hand-rubs and hand care pro-ducts applied immediately prior to disinfect ion Diffe-rences between reduction factors achieved with hand-rubs alone and in combination with hand care were notsignificant Repeated application of care products withsubsequent hand disinfection also did not result in signifi-cantly lower reduction factors than achieved with handdisinfection alone Our data suggest that administrationof selected products for hand care does not necessarilyimpair hand disinfection and is therefore recommendedfor occupational health as well as for infection controlreasons
Jaisson Hot I Haond C Reverdy ME Bui Xuan BVedrinne JM Duperret S Mohammedi I BobineauI Petit P Bouletreau P Guerraz FT Incidence ofnosocomial infections in an intensive care unit a three-year prospective study including 815 patients Meacutedecineet Maladies infectieuses 30 520-527 (2001)
NOTES We report the results of a prospective study onthe incidence of nosocomial infections including 815patients admitted in an intensive care unit in the LyonEdouard Herriot Hospital from 1995 to 1997 We notedan incidence rate of 292 nosocomial infections per1000 patient days 145 respiratory tract infections1000ventilator days 116 urinary tract infections1 000 ind-welling urinary catheter days 48 bacteremia1000patient days 22 colonization of central venous or arterial
N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
24
catheters1000 catheter days The most important resultwas the lower incidence of UTI during these 3 years Thisepidemiological survey should be continued in order toreduce the rates of other nosocomial infections and toobtain quality markers
Lacey S Flaxman D Scales J Wilson A The useful-ness of masks in preventing transient carriage of epide-mic methicillin-resistant Staphylococcus aureus by heal-thcare workers Journal of hospital infections 48 308-311 (2001)
NOTES We assessed the usefulness of waring masks inpreventing epidemic methicillin-resistant Staphylococcusaureus (EMRSA) carriage in nursing and physiotherapystaff on two dedicated EMRSA units In the first phase ofthe study members of staff were screened for EMRSA car-riage immediately before and after periods of duty usingnose throat and hand swabs During the second phase ofthe study masks were worn by staff carrying out proce-dures associated with significant EMRSA exposure andexamined for EMRSA as described for the first phaseBoth phases were conducted over a period of twomonths Forty-eight percent of nursing staff were coloni-zed with EMRSA at some time during the first phase of thestudy Wearing masks significantly reduced nasal throatand hand carriage of EMRSA (P lt 005) We concludethat the wearing of masks by healthcare workers perfor-ming certain activities for EMRSA positive patients mayprevent transient colonization and hence may be a usefulintervention in the control of EMRSA in the hospital envi-ronment
McGuckin M Waterman R Storr J Bowler ICJWAshby M Topley K Porten L Evaluation of a patient-empowering hand hygiene programme in the UK Jour-nal of Hospital Infection 48 222-227 (2001)
NOTES Partners in Your Care(R) a patient educationbehavioral model for increasing handwashing com-pliance and empowering the patient with responsibilityfor their care was evaluated in an acute care hospital inOxford UK A controlled prospective intervention studycomparing medical and surgical patients was performedNinety-eight patients were eligible for the study Thirty-nine patients (40) agreed to participate in the pro-gramme Partners in Your Care by asking all healthcareworkers who were going to have direct contact with themDid you wash your hands Compliance with the pro-gramme was measured through soapalcohol usage andhandwashings per bed day before and after its introduc-tion Partners in Your Care increased handwashing onaverage 50 Healthcare workers washed hands moreoften with surgical patients than with medical (Plt005)Alcohol gel was used on less than 1 of occasions Sixty-two percent of patients in study felt at ease when askinghealthcare workers Did you wash your hands Seventy-eight percent received a positive response (washedhands) All patients asked nurses but only 35 askedphysicians Partners in Your Care increased handwashingcompliance in the UK This programme empowerspatients with responsibility for their care provides infec-tion control staff with a continuing means for providinghandwashing education without additional staff and cansave costs for a hospital
Melling AC Ali B Scott EM Leaper DJ Effects ofpreoperative warming on the incidence of wound infec-tion after clean surgery a randomised controlled trialLance 358 876-880 (2001)
NOTES BACKGROUND Wound infection after cleansurgery is an expensive and often underestimated causeof patient morbidity and the benefits of using prophylac-tic antibiotics have not been proven Warming patientsduring colorectal surgery has been shown to reduceinfection rates We aimed to assess whether warmingpatients before short duration clean surgery would havethe same effectMethods 421 patients having clean(breast varicose vein or hernia) surgery were randomlyassigned to either a non-warmed (standard) group or oneof two warmed groups (local and systemic) We appliedwarming for at least 30 min before surgery Patients werefollowed up and masked outcome assessments made at 2and 6 weeksFindings Analysis was done on an intention-to-treat basis We identified 19 wound infections in 139non-warmed patients (14) but only 13 in 277 whoreceived warming (5 p=0001) Wound scores werealso significantly lower (p=0007) in warmed patientsThere was no significant difference in the development ofhaematomas or seromas after surgery but the non-war-med group were prescribed significantly more postopera-tive antibiotics (p=0002)Interpretation Warming patientsbefore clean surgery seems to aid the prevention of post-operative wound infection If applied according to themanufacturers guidelines these therapies have no knownside-effects and might with the support of further studiesprovide an alternative to prophylactic antibiotics in thistype of surgery
Morris W Simon L Pineiro A Pelle Lancien ELaplace C Hamza J Assessment of antibacterial fil-ters for epidural catheters in obstetrics Annales franccedilaises drsquoAestheacutesie et de reacuteanimation 20 600-603 (2001)
NOTES OBJECTIVES To assess the antibacterial effi-ciency of filters used in obstetrics when epidural top-upsare performedStudy design Observational prospectivestudyPatients and methods We aseptically collected 201anti-bacterial filters that had been used for top-ups withropivacaine +- sufentanil for epidural analgesia duringtabour We flushed them first with 2 mL of saline and thenwith 2 mL of a solution containing 15 x 10(6) Staphylo-coccus epidermidismL The filtrates were incubated at 37degreesC for 72 h Number of top-ups and duration ofepidural analgesia are expressed as median(extremes)Results 3 (1-10) top-ups were performed fortabour analgesia over a period of 65 h (18-18) After fil-tering all the solutions were found to be sterile Espe-cially when using Staphylococcus epidermidis solutionsbacteria were not found beyond any filter These resultssuggest the integrity of the filter membrane after severalboluses No infection related to epidural analgesia wasreportedConclusion Antibacterial filters provide a goodprotection against a potentially contaminated procedureduring epidural top-ups
N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt

N O S O - i n f o v o l V I n deg 1 2 0 0 2
25
WETENSCHAPPELIJK AGENDA
Gelieve ons de verschillende manifestaties die U organiseert mee te delen
10 11 24 APRIL et 15 29 MEI 2002NSPH Cursus Capita Selecta van de infectieziektebestrijdingPlaats Utrecht (The Netherlands)Inlichtingen wwwnsphnl - E-mail mvleerlaagnsphnl
4 - 7 MEI 20024th European Congress of Chemotherapy and InfectionPlaats Paris (France)Inlichtingen Congrex Sweden AB Stockholm SwedenTel 4684596600 ndash Fax 4686619125 ndash E-mail ecc4congrexsehttpwwwcongrexcomecc4
15 MEI 2002Seminaires des Maladies infectieuses (groupe Anvers)Candida-sepsis E Vlieghe M Van de VijverePlaats ACZA campus Stuivenberg ndash Auditorium Sano AnversUur 12h30-13h30Inlichtingen httpgso-wwwuiaacbegsoIZGhtmTel 038202502 ndash Fax 038202501 ndash E-mail mvbareluiauaacbe
16 MEI 2002La Microbiologie Clinique Pratique Rencontres interhospitaliegraveres de la Province de Hainautlaquo Meacuteningites agrave enterovirus bilan de lrsquoeacutepideacutemie 2000raquo Drs C Liesnard Virologie Hocircpital Erasme et D Famereacutee Microbiologie CHU CharleroiPlaats Salle de seacuteminaire (niveau 0) CHU A Veacutesale Montigny-le-TilleulInlichtingen Dr C Potvliege MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
15-16-17 MEI 20028egraveme Rencontre Internationale des Infirmier(egravere)s Francophones en Hygiegravene HospitaliegraverePlaats Martigny (Suisse)Inlichtingen Patricia Taminiau preacutesidente de lrsquoABHH - E-mail ABHHcaramailcom
16-23 MEI 2002APIC 2002 ndash USAPlaats Nashville (Tennessee) Convention CenterInlichtingen APIC Nat Office 1275K street NW suite 1000 Washington DC 20036Tel (202)7891890 ndash Fax (202)7891899 ndash E-mail apicinfoapicsorghttpwwwapicorg
29-30 MEI 2002VHIG Congres 2002Plaats Doorwerth Parkhotel de BrandingInlichtingen Secretaris Congrescie M Louwers Teacutel 073-6404587
12 JUNI 2002Seacuteminaris van de Volksgezondheid Instituutlaquo European surveillance of nosocomial infections in ICU the HELICS-ICU project IMorales C SuetensEpidemiology ISP)Plaats ISP J Wytsmanstraat 14 1050 Brussel zaal NELISSteeds 12u30-13u30Ilichtingen Secretariaat van epidemiologie 026425037
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt
N O S O - i n f o v o l V I n deg 1 2 0 0 2
26
13 - 14 JUNI 2002XIIIIste Nationaal Congres van de laquo Socieacuteteacute Franccedilaise drsquoHygiegravene Hospitaliegravere raquoPlaats Toulouse (Frankrijk)Inlichtingen Europa Organisation St Pantaleacuteon 5 BP844 31015 Toulouse cedex 6Tel (33)534452645 - Fax (33)534452546 ndash E-mail europaeuropa-organisationcom
20 JUNI 2002Klinische Microbiologie in de praktijk laquo Rencontres interhospitaliegraveres de la Province de Hainaut raquolaquo Automatisering van de microscopische ontleding van de urines bespreking en toekomst raquoDrs Allemeersch Microbiologie Clin Elisabeth et G Mascart Biol Clinique CHU BrugmannPlaats Seariezaal (op 11ste verdieping) CHU Tivoli La LouviegravereInlichtingen Dr C Potvliege Dienst MicrobiologieCHU Tivoli Teacutel 064276406Dr D Govaerts Dienst Microbiologie CHU A Veacutesale Montigny-le-Tilleul ndash Teacutel 071295530
27 JULI ndash 1ste AUGUSTUS 2002Joint Meeting of the three divisions of the International Union of Microbiological SocietiesPlaats Paris (Frankrijk)Inlichtingen httpwwwiums-paris-2002com
25 AU 28 AUGUSTUS 2002SHEACDCESGNITraining course in hospital epidemiologyPlaats Stein am Rhein (Suissi)Inlichtingen http WWW hosp-epi-coursechspitalhygienedimuszch
15 - 18 SEPTEMBER 20025th International Conference of the Hospital Infection SocietyPlaats Edinburgh (UK)Inlichtingen HIS 2002 Concorde Services Ltd Glasgow UKTel 441413310123 ndash Fax 441413310234 ndash E-mail hisconcorde-ukcom
15-16 OCTOBER 2002Opleiding in Centra CEFHlaquo Hygieumlne Beheersmogelijkheid in de klinische omgeving raquoPlaats Strasbourg (Frankrijk)Inlichtingen Centre drsquoeacutetudes et de formation hospitaliegraveres BP 98 Cahors cedex 9Tel 0565230600 ndash Fax 0565230609 wwwcefh-cepscom
Te onthouden adressen
CDC HICPAC httpwwwcdcgovncidodhipDEFAULTHTMCSH httpwwwhealthfgovbeCSH_HGRFrancaissommairehtmInfect Control amp Hosp Epidemiol ICHE httpwwwslackinccomgeneralicheichetochtmJournal of Hospital Infection JHI httpwwwharcourt-internationalcomjournalsjhinNosobase httpwwwuniv-lyon1frLyonSudnosobaseNoso-info httpwwwmduclacbenosoinfointrohtmSite UCL httpwwwmduclacbedidachospintrohtm
SITES WEBNieuwigheden
CClin Paris ndashNord httpwwwccrjussieufrcclinwelcomebishtmHandhygieumlneActualisatie bij het plaatsen van een veneuze catheter
CclinSud-ouest httpwwwcclin-sudouestcomAanbevelingen ter vermindering van het risico vaninfectie in relatie met de ruimte waar implanteerbarecatheters geplaatst wordenAanbevelinge voor de preoperatieve ontsmetting vande patieumlnt





























