Embed Size (px)
Citation preview

HotSpots
Novel cilia-dependent pathwayactivates rapid cyst growthin autosomal dominant polycystickidney disease
References1. Steinman TI. Polycystic kidney disease: a 2011 update. Curr Opin
Nephrol Hypertens 2012: 2: 189–194.2. Hopp K, Ward CJ, Hommerding CJ et al. Functional polycystin-1 dosage
governs autosomal dominant polycystic kidney disease severity. J ClinInvest 2012: 11: 4257–4273.
Loss of cilia suppresses cyst growth in genetic modelsof autosomal dominant polycystic kidney disease.Ma et al. (2013)Nature Genetics 45(9):1004–1012
Autosomal dominant polycystic kidney disease(ADPKD) (MIM# 173900) is characterized by pro-gressive loss of renal glomerular filtration caused bythe formation of fluid filled cysts in the glomerularepithelium. The age of onset varies vastly, which mayinvolve hypertension, cyst formation in other organs,especially liver and subarachnoid haemorrhage from
230

HotSpots
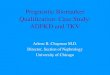
Fig. 2. Ciliary processes leading to cyst formation. Wild type mice repress the cilia-dependent activation pathway via PC1 & PC2. ADPKDmice lack functional PC and hence overactivate cilia-dependent cyst growth. cAMP is a putative downstream intermediate of the pathway (Redlines = inhibition; Dotted lines = multiple steps; ? = mediator unknown).
intracranial aneurysms and finally end-stage renaldisease (1). Underlying mutations in either of thetwo polycystin genes Pkd1 and Pkd2 are the mostcommon cause of ADPKD. The polycystin proteinsPC1 and PC2 are components of the primary cilium ofepithelial cells undergoing cyst formation. The primarycilium is composed of the intra-flagellar transport (IFT)machinery disruption of which leads to cyst formationin mice. However, it is not known whether it is the lossof polycystins or the persistence of intact cilia devoidof PCs which leads to changes in signalling implicatedin the ensuing cyst growth.
Ma et al. use an elegant genetic approach to dissectthe pathways that depend on intact cilium devoid ofpolycystins leading to rapid cyst growth. Using tissue-specific constitutive and inducible knockout mousemodels of Pkd1 and Pkd2 in combination withknockouts of Kif3a and Ift20 (integral components ofciliary IFT), the authors show that disruption of ciliaretards cyst growth caused by the loss of polycystins.Concomitant loss of Pkd1 and Pkd2 along with Kif3aand Ift20 , respectively, caused a phenotype that wasintermediate to the loss of polycystins alone. Lossof polycystins led to rapid cyst growth but did notaffect cilia formation. Cilia were completely absent in
mice lacking either Kif3a or Ift20 proteins. Polycystinexpression still persisted in cells devoid of cilia and waslocalized at cellular sites outside of cilia.
The mild severity of cyst formation caused by dis-ruption of cilia alone hinted at possible suppressiverole of persistent polycystin expression. It was recentlyreported that the gene dosage of Pkd1 governs the sever-ity of ADPKD (2). The authors tested this hypothesisby using kidney epithelium-specific heterozygous Pkd1mice to reduce gene dosage or mice expressing a threecopy BAC transgenic variant to increase gene dosage.Neither of the two models showed differences in cystformation induced by disrupting cilia, implying thatciliary localization of polycystins is indispensible fortheir suppressive action. This indicated that the loss ofpolycystins caused cyst formation in a cilia-dependentmanner, but loss of cilia caused cyst formation inde-pendent of polycystin function.
Next, the authors tested whether disease severity wasaffected by a time-dependent persistence of cilia follow-ing polycystin loss. Age-matched double knockouts forhomozygous Pkd1; single copy Kif3a had a lower cystindex compared to double knockouts of homozygousPkd1 and Kif3a. As the single copy Kif3a mice had arelatively rapid disappearance of cilia, the period of ciliapersistence after polycystin loss was less than Kif3a
231

HotSpots
homozygous mice. Hence, the authors concluded thatcyst index and severity are directly affected by theperiod for which polycystin-free cilia persisted.
Next using the TetO-cre inducible mice, the authorsreplicated these findings in adult mice where con-comitant lack of both polycystin and disruption ofcilia reduced disease severity. The TetO-Cre induciblesystem allowed the authors to identify downstreamcomponents of the newly identified cilia-dependentcyst-activating pathway. They examined the activitiesof the MAPK/ERK, mTOR and cAMP pathways all ofwhich have been implicated in mouse models of cysticdisease and are targets of pre-clinical and clinical inter-vention in humans. No significant correlation was foundbetween ERK and mTOR activities and cyst index.Lastly, activation of cAMP response element binding
protein (CREB) was significantly enhanced at both 8-and 14-week post-induction in Pkd1 knockouts. Levelsof nuclear active CREB were comparable betweendouble knockouts and controls. However, there was noCREB activation in the proximal tubule irrespectiveof genotype or cyst burden. Taken together these dataindicate the presence of a new cilia-dependent cystpromoting pathway, which is suppressed by functionalpolycystins as depicted in Fig. 2. The identification ofdownstream components of the pathway will definesuperior targets for ADPKD intervention.
J.V. PatankarCentre for Molecular Medicine and Therapeutics, Department of
Medical Genetics, University of British Columbia, 950 West 28thAvenue, Vancouver, BC V5Z4H4, Canada
e-mail: [email protected]
232