Embed Size (px)
Citation preview

[1]
O bG y n
ความสาคญทควรทราบ PPH ในโรงพยาบาลของทาน บงบอกถงระบบการดแลทางระบบ
สาธารณสข ของโรงพยาบาลทาน
ควรทบทวนอตราการเกด PPH ของโรงพยาบาลทอย พยายามปรบปรงระบบการดแล / มาตรฐานการดแลผปวยทม
ภาวะPPH
ประเดนทพจารณา
การประเมนปรมาณการสญเสยเลอด / ความแมนยำ
Early detection ภาวะเสยงตอ PPH จากปจจย
เสยงของแตละสาเหต
การคนหาสาเหตหรอการจำแนกชนดจากภาวะตกเลอด
การประเมนปรมาณของงการสญเสยเลอดและการแมนยำในการประเมน
PPH2
011
เอกสารประกอบการสอน ภาวะตกเลอดหลงคลอด PPH
ประการณ องอาจบญ วว.สตศาสตรนรเวชวทยา

[2]
PPHPrakarno2011
PostPartumHemorrhage
ภาวะตกเลอดหลงคลอด(PPH) ถอเปนหนงในสาเหตการตายของหญงตงครรภสงสด หาอนดบแรกทงในกลมประเทศท
พฒนาและยงไมพฒนา ( 1/100,000 - 1/1,000 ของการคลอด ) โดยมอบตการณประมาณ รอยละ 1 ถง 5 ขนอยกบหลกเกณฑในการวนจฉย ภาวะขาดแคลนบคลากรทมประสบการณในการทาคลอดและอปกรณทางการแพทย ไมมยาทจาเปนอยางพอเพยง ภาวะขาดแคลนเลอดหรอแมแตขนตอนการดแลรกษาทไมมประสทธภาพ
คาจากดความPostpartum hemorrhage ( PPH ) หมายถง การเสยเลอดจากอวยวะสบพนธสตรทมปรมาณอยางนอย 500 มลลลตรภายใน 24 ชวโมงแรก หลงคลอด ( World Health Organization , 1990 )การเสยเลอดอยางนอย 500 มลลลตรจากการคลอดปกตทางชองคลอด หรอ การเสยเลอดอยางนอย 750 มลลลตรจากการผาตดคลอด (ICD10-AM) หลงจากสนสดระยะทสามของการคลอด (ภายหลงรกคลอด )ปญหาของการใชเกณฑน คอการประเมนปรมาณเลอดทออกทางชองคลอดอยางถกตองเปนสงททาไดยากและสวนใหญมกประเมนตากวาความเปนจรงประมาณ รอยละ 50การประเมนปรมาณเลอดทสญเสยไปในระยะหลงคลอดดวยตาเปลานนมกจะไมแมนยาและประเมนไดนอยกวาทควรจะเปน ทาใหการวนจฉยภาวะตกเลอดภายหลงคลอดลาชาและไมทนทวงท นอกจากนมารดาแตละคนกมสภาพ
รางกายทแตกตางกน บางรายสามารถทนตอการสญเสยเลอดปรมาณ 500 มลลลตรไดเปนอยางด ขณะทบางราย
แมเสยเลอดเพยงเลกนอยกลบมการเปลยนแปลงของรางกายทแยลงและไมคงทดวยเหตนจงมปจจยอนๆทแพทยและบคลากรทางการแพทยควรใหความตระหนกและนามารวมในการประเมนผปวยเพอ
ใหการวนจฉยภาวะตกเลอดหลงคลอดไดอยางถกตองการใชลกษณะทางคลนกเพอประเมนการเสยเลอด ไดแก อาการวงเวยน หนามด เปนลม และ/หรอ มอาการแสดงของปรมาณเลอดในรางกายตาลง (hypovolemia) ไดแก ความดนโลหตลดลง ชพจรเตนเรว หรอปรมาณปสสาวะนอยลง

[3]
การประเมนการเสยสญเลอด
ตารางแสดงอาการทางคลนกทสมพนธกบการสญเสยเลอดในภาวะตกเลอดหลงคลอด ปรมาณเลอดทเสย รอยละ มลลลตร
ความดนโลหต (มลลลตรปรอท) อาการและอาการแสดง
10−15 500 - 1000
ปกต ใจสน มนงง ชพจรเรว
15−25 1000 - 1500
ตำเลกนอย 80 − 100
ออนแรง เหงอออก ชพจรเรว
25−35 1500 - 2000
70 – 80 กระสบกระสาย ซด ปสสาวะออกนอย
35−45 2000 - 3000
50 – 70 หมดสต ขาดอากาศ ไมมปสสาวะ
รวมทงการใชการตอบสนองของรางกายหรอมาตรวดสญญาณชพ
systolic blood pressure and mean arterialpressure. Thus, the failure to respond to theinitial administration of 3000 ml of crystalloidwould suggest a Class II hemorrhage with lossgreater than 20–30% of the total blood volumeor acute ongoing bleeding26,27. A systolic bloodpressure below 100 mmHg and a pulse rateabove 100 beats/min are late signs of depletedblood volume and indicate commencing failureof compensatory mechanisms28, whereas acuteblood loss might not be reflected by a decreasein hematocrit or hemoglobin level for 4 hor more26,27. The importance of diagnosis at aClass I stage cannot be too strongly emphasizedas women can progress into Class II rapidly.At level III, unless intervention is rapidand appropriate, women may progress toirreversible shock.
Quantitative methods
Visual assessment
The standard method of observation used forthe measurement of blood loss is relativelystraightforward and requires no expenditure8.Despite its inaccuracy and variation from onecare-giver to the next, birth attendants correlateit with clinical signs. A review of the records of32 799 deliveries at a large municipal hospitalduring the decade of 1963–1972 found an inci-dence of postpartum hemorrhage of 4.7/1000live births or 0.47%. This was extremely lowcompared to stated rates in the literature, andthe author concluded that many cases of post-partum hemorrhage were not recorded due tounderestimation of blood loss29.
The accuracy of this method can beimproved by standardization and training. Theobserver needs to be trained in determining theblood loss using a single collecting containerand fixed-sized gauze pads of size 10 ! 10 cm.Simulated scenarios with known measuredblood volume need to be created and calibratedvisually (see Figure 1).
Another method of calculation is by allowingblood to drain into a fixed collecting container(Figure 2) for estimation at the end of 1 h.Blood losses on the delivery table, garments andfloor should also be assessed. At the end of 1 h,the total amount of blood lost is estimated by
totaling up the blood in the container, in thesponges and secondary blood spillage on thedelivery table, garments and floor. How oftensuch calculation is utilized is unknown, butfailure to do so undoubtedly contributes tounderestimation.
Direct collection of blood into bedpan or plastic bags
This approach was used in the World HealthOrganization (WHO) multicenter, randomizedtrial of misoprostol in the management of thethird stage of labor30. In this trial, blood loss wasmeasured from the time of delivery until themother was transferred to postnatal care. Imme-diately after the cord was clamped and cut, theblood collection was started by passing a flatbedpan under the buttocks of a woman deliver-ing in a bed or putting in place an unsoiled sheetfor a woman delivering on a delivery table.
37
Assessment of blood loss and decision to transfer
Figure 1 Soakage characteristics of 10 ! 10 cmpads
Figure 2 Blood drained into a fixed collectingcontainer
59Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:19:18
Color profile: Generic CMYK printer profileComposite Default screen
systolic blood pressure and mean arterialpressure. Thus, the failure to respond to theinitial administration of 3000 ml of crystalloidwould suggest a Class II hemorrhage with lossgreater than 20–30% of the total blood volumeor acute ongoing bleeding26,27. A systolic bloodpressure below 100 mmHg and a pulse rateabove 100 beats/min are late signs of depletedblood volume and indicate commencing failureof compensatory mechanisms28, whereas acuteblood loss might not be reflected by a decreasein hematocrit or hemoglobin level for 4 hor more26,27. The importance of diagnosis at aClass I stage cannot be too strongly emphasizedas women can progress into Class II rapidly.At level III, unless intervention is rapidand appropriate, women may progress toirreversible shock.
Quantitative methods
Visual assessment
The standard method of observation used forthe measurement of blood loss is relativelystraightforward and requires no expenditure8.Despite its inaccuracy and variation from onecare-giver to the next, birth attendants correlateit with clinical signs. A review of the records of32 799 deliveries at a large municipal hospitalduring the decade of 1963–1972 found an inci-dence of postpartum hemorrhage of 4.7/1000live births or 0.47%. This was extremely lowcompared to stated rates in the literature, andthe author concluded that many cases of post-partum hemorrhage were not recorded due tounderestimation of blood loss29.
The accuracy of this method can beimproved by standardization and training. Theobserver needs to be trained in determining theblood loss using a single collecting containerand fixed-sized gauze pads of size 10 ! 10 cm.Simulated scenarios with known measuredblood volume need to be created and calibratedvisually (see Figure 1).
Another method of calculation is by allowingblood to drain into a fixed collecting container(Figure 2) for estimation at the end of 1 h.Blood losses on the delivery table, garments andfloor should also be assessed. At the end of 1 h,the total amount of blood lost is estimated by
totaling up the blood in the container, in thesponges and secondary blood spillage on thedelivery table, garments and floor. How oftensuch calculation is utilized is unknown, butfailure to do so undoubtedly contributes tounderestimation.
Direct collection of blood into bedpan or plastic bags
This approach was used in the World HealthOrganization (WHO) multicenter, randomizedtrial of misoprostol in the management of thethird stage of labor30. In this trial, blood loss wasmeasured from the time of delivery until themother was transferred to postnatal care. Imme-diately after the cord was clamped and cut, theblood collection was started by passing a flatbedpan under the buttocks of a woman deliver-ing in a bed or putting in place an unsoiled sheetfor a woman delivering on a delivery table.
37
Assessment of blood loss and decision to transfer
Figure 1 Soakage characteristics of 10 ! 10 cmpads
Figure 2 Blood drained into a fixed collectingcontainer
59Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:19:18
Color profile: Generic CMYK printer profileComposite Default screen
reduce the incidence of acute postpartumhemorrhage and hence maternal morbidity andmortality in women delivering in rural villages(away from major hospitals) within BelgaumDistrict, Karnataka, India. The interventionwas delivered by local health-care workers. Acritical component of this trial was the develop-ment of a specially designed low-cost ‘calibratedplastic blood collection drape’ that would objec-tively measure the amount of blood collectedin the immediate postpartum period. TheBRASSS-V drape was developed by theNICHD-funded Global Network UMKC/JNMC/UIC collaborative team to specificallyestimate postpartum blood loss45,46. (The name‘BRASSS-V’ was coined by adding the first let-ter of the names of the seven collaborators whodeveloped the drape.) The drape has a cali-brated and funneled collecting pouch, incorpo-rated within a plastic sheet that is placed underthe buttocks of the patient immediately after thedelivery of the baby. The upper end of the sheethas a belt, which is loosely tied around thewoman’s abdomen to optimize blood collection,particularly for deliveries performed on the flooror on a flat surface at homes or in rural primitivehealth posts. This simple tool not only hasthe potential for a more accurate detection ofpostpartum blood loss, but we hypothesize thatthis approach will lead to earlier interventions,with an ultimate goal of decreasing maternalmorbidity and mortality due to postpartumhemorrhage. Since most developing countriesuse some form of under-buttock sheet, either athome, in the health center or in hospitals, drapesubstitution is acceptable and relatively simple.The BRASSS-V calibrated drape used forobjective estimation of blood loss is shown inFigures 4 and 5.
Results of three studies conducted at JNMC,Belgaum, Karnataka, India4,7 strongly suggestthat the BRASSS-V drape is an accurate andpractical tool to measure blood loss occurring inthe third stage of labor. While, among womenwith little blood loss, the ranges of blood losswere similar in both visual and drape assess-ment, the actual visual assessment amount wasconsiderably less compared with the calibrateddrape values (Table 2 and Figure 6). Thisobservation further underscores the inaccuracyof the visual estimation method as described
in the literature, whereas differences betweenthe drape and spectrophotometry values werefound to be 37.15 ml, with the drape having thehigher value (an average error of 16.1%). Thedrape measured blood loss equally and as
40
POSTPARTUM HEMORRHAGE
Figure 4 BRASSS-V blood collection drape withcalibrated receptacle
Figure 5 Collection of blood using BRASSS-Vblood collection drape with calibrated receptacle
62Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:19:22
Color profile: Generic CMYK printer profileComposite Default screen
การประเมนการเสยเลอดในภาวะตกเลอดหลงคลอด
มความพยายามในการประเมนการเสยเลอดหลากหลายวธ ขนอยกบวตถประสงคในการทจะตองการวดประเมน โดยทวไปแลวมกทจะประเมนนอยกวาความเปนจรงเสมอ ดงนนการนาเอาอาการแสดงทางคลนกทสมพนธกบการสญเสยเลอดอาจจะชวยในการประเมนภาวะตกเลอดหลงคลอด นาจะชวยไดแตอยางไรกตามกตองอาศยการชานาญและการดแลผปวยไดอยางรวดเรวเพอทจะทนกบการประเมนเพอสามารถใหการรกษาไดอยางรวดเรวตามไปดวย

[4]
การจาแนกชนดของภาวะการณตกเลอดหลงคลอด ( Classification of PPH ) ชนดของ PPH สามารถแยกไดหลายแบบ ดงน 1) จาแนกตามระยะเวลาเมอเทยบกบการคลอด เปนการจาแนกทงายและใชหนอยางแพรหลายไดแก Early หรอ Primary PPH หมายถง ภาวะตกเลอดทเกดขนภายใน 24 ชวโมงแรกหลงคลอดเปนสาเหตของภาวะตกเลอดหลงคลอดทพบไดมากและบอยทสดประมาณ 4-6% ของการตงครรภทงหมดโดยประมาณ 80% มสาเหตมาจาก uterine atony นอกจากนยงเปนสาเหตการเสยชวตของมารดาทพบไดบายทสด Late หรอ Secondary PPH หมายถง ภาวะตกเลอดทเกดขนภายหลง 24 ชวโมง แตไมเกน 12 สปดาหหลงคลอด พบไดนอย ประมาณ 1 – 3 % ของการคลอดทงหมด 2) จาแนกตามปรมาณจานวนเลอดทสญเสย การสญเสยเลอดเปนสดสวนใหญของสารนาทสญเสยไปจากรางกายเมอมภาวะตกเลอดหลงคลอด ดงนนการจาแนกปรมาณการสญเสยเลอดจงเปนตวสะทอนถงปรมาณสารนาทสญเสยไปจากรางกายดวย
3) จาแนกตามสาเหตของการเสยเลอดเราสามารถจาแนกสาเหตของ PPH ตามสาเหตไดโดยใช หลกการจา 4T ไดแก
Tone : หมายถง ความผดปกตของการหดรดตวของมดลก เปนสาเหตทพบไดบอยทสดประมาณ70% ของภาวะ การตกเลอดทงหมดTrauma : หมายถง การบาดเจบหรออนตรายทเกดขนกบชองทางคลอดและอวยวะสบพนธ พบเปนสาเหตไดประมาณ 20% ของภาวะตกเลอดหลงคลอดทงหมดTissue : หมายถงการเหลอคางของผลผลตจากการตงครรภ เชน รก , ทารกในครรภ เปนตน พบไดประมาณ 10% หลงคลอดทงหมดThrombin : หมายถงความผดปกตของเกรดเลอดและระบบการแขงตวของเลอด พบไดนอยมากประมาณ 1% ของภาวะตกเลอดหลงคลอดทงหมดบางคนแยก 4T + 1 โดย 1 สดทายคอ Traction จนเกด ut inversion4) จาแนกตามอาการและแสดงอาการตามคลนก การใชอาการและแสดงอาการทางคลนกรวมในการประเมนภาวะตกเลอดหลงคลอดมประโยชนชวยใหสามารถใหการวนจฉยและดแลผปวยไดรวดเรวยงขน เนองจากการเปลยนแปลงของรางกายแปรผนกบปรมาณเลอดทเสยไปโดยตรง
สาเหตPPH Causes of primary PPHTone ( uterine atony )Uterine overdistention : multiparity , polyhydramnios , macrosomiaUterine relaxants : nifedipine , magnesium , beta – mimetics , indomethacin , nitric oxide donorsRapid or prolonged laborOxytoxics to induce laborChorioamnioniticsFibroid uterusTissueImpediment to uterine contraction / retraction : multiple fibroids , retained placentaPlacental abnormality: placenta accrete , succenturiate lobeObstructed third stage of laborExcessive traction on the cordTraumaUterine ruptureUterine inversion Vulvovaginal injury Episiotomy / tearsMacrosomiaPrecipitous deliveryThrombin ( coagulopathy ) Acquired during pregnancy : thrombocytopenia of HELLP sysdrome , DIC (eclampsia , intrauterine fetal death,septicemia,placenta abruption,amniotic fluid embolism),pregnancy - induced hypertension,sepsisHereditary : Von Willebrand’s diseaseAnticoagulant therapy : valve replacement,patients on absolute bedrest
CAUSES OF SECONDARY PPH
Uterine infectionRetained placental fragmentsAbnormal involution of placental site

[5]
แนวทางการดแลรกษา ภาวะตกเลอดหลงคลอด PPH เมอมารดาไดรบการวนจฉยภาวะตกเลอดหลงคลอด ทมแพทยผดแลมความจาเปนอยางยงทจะตองใหการรกษาอยางทนทวงท ทงนเพอปองกนมใหมารดาเสยเลอดเพมมากขนจนเกดภาวะชอคซงจะนาไปสภาวะทพพลภาพและการเสยชวตของมารดาในทสด การรกษาภาวะตกเลอดหลงคลอดตองคานงถงหลก 3 ประการ ไดแก สาเหตททาใหเกดภาวะตกเลอดหลงคลอด,ทางเลอกของการรกษาทมอยในสถานพยาบาลนนๆและความตองการมบตรในอนาคตของมารดา อยางไรกตามการรกษาภาวะตกเลอดหลงคลอดเปนสถานการณทตองแขงกบเวลา ดงนน ความร,ความชานาญและประสบการณของทมแพทยผรกษาจงมความสาคญอยางยงในการดแลและตดสนใจใหการรกษาทเหมาะสมกบมารดาแตละราย
แนวทางการวนจฉยเพอหาสาเหตของภาวะตกเลอดหลงคลอดระยะแรก 1. ซกประวตอยางละเอยดเกยวกบการตงครรภ การคลอด โรคประจาตว เชน โลหตจางโรคทเกยวกบ
การแขงตวของเลอดผดปกตหาสาเหตและเหตชวนใหเกดการตกเลอดหลงคลอด การประเมนวาผปวยมปจจยเสยงทางคลนกตอการตกเลอดหรอไม 2. คะเนปรมาณเลอดทออกทางชองคลอดมากกวา 500 มลลลตรและเลอดทออกรนแรงเพยงใด 3. ตรวจรางกายดอาการแสดงของการเสยเลอดเชน สญญาณชพ ไดแก ชพจรเบาเรว ความดนโลหตตาหรอซดมากหรอไมเพอคะเนปรมาณเลอดทเสย เปดเสนเลอดดาดวยเขมขนาดใหญ ( เบอร 16 G ) 1-2 เสน เพอใหสารนา เลอดและยาไดอยางสะดวกและรวดเรว ใหสารcrystalloid ในปรมาณมากเพยงพอ เพอปองกนภาวะความดนโลหตตาสงเลอดตรวจทางหองปฏบตการ เชน complete blood count, จานวนเกลดเลอด , prothrombin time, active partial thromboplastine time, fibrinogen เพอเปนขอมลพนฐานในการตรวจตดตามการรกษาตอไป นอกจากนยงตองสงตรวจ type และ cross matching เพอจองเลอดจากธนาคารเลอดในคราวเดยวกน
แนวทางการรกษา
Royal College of Obstetricians and Gynaecologists (RCOG) และ American college of Obstetricians and Gynaecologists (ACOG)
ไดใหคาแนะนาเกยวกบการรกษาภาวะตกเลอดหลงคลอดสาหรบสถานพยาบาลระดบตตยภม โดย RCOG แบงภาวะตกเลอดออกเปน 2 ประเภท ไดแก Minor PPH : เสยเลอด 500 – 1,000 มลลเมตร และไมมอาการแสดงของภาวะชอค
Major PPH : เสยเลอดมากกวา 1,000 มลลลตร รวมกบยงมภาวะเลอดออกอยางตอเนองหรอมอาการแสดงของภาวะชอค

[6]
4. ตรวจการหดรดของมดลก ถายงหดรดตวไมดหลงจากสวนปสสาวะแลวแสดงวาการตกเลอดหลงคลอดเกดจากมดลกหดรดตวไมดใหนวดคลงหรอกดมดลกใหยากระตนการหดรดตวของมดลก ไดแก oxytocin ซงถอเปนยาหลกทเลอกใช โดยผสม oxytocin 10-40 ยนตในนาเกลอ 1,000 มล. หยดเขาทางเสนเลอดดาหรอฉดเขากลามเนอในปรมาณ 10 ยนต ในรายทจาเปนสามารถใชยาทมความเขมขนสง 80 ยนตตอนา 1,000 มล. ในระยะเวลาสนๆ ยา methergin ฉดเขากลามเนอใหขนาด 0.2 มก.ทก2-4 ชวโมง(สามารถฉดเขากลามเนอมดลกได) แตตองระวงในกรณทมภาวะความดนโลหตสง 15 – metlhy PGF2α (Hemabate) ฉดเขากลามเนอ 250 ไมโครกรม ทก 15 ถง 90 นาท (สามารถฉดเขากลามเนอมดลกได) ปรมาณสงสดไมเกน 2 มก.และหามใหในกรณทเปนหอบหด ยา misoprostol (Cytotec®) สามารถใหไดในรายทมความดนโลหตสงหรอเปนหอบหด วธการใหยามหลายรปแบบทงกน อมใตลน และเหนบทวารหนก หรอผสมกนสาหรบขนาดทใหกแตกตางกนไปตงแต 800 – 1000 ไมโครกรม
วธทนยมในปจจบนคอ เหนบทวารหนกในขนาด 600 ไมโครกรม เนองจากสะดวกในการบรหารยาผลขางเคยงทอาจพบคอทาใหอาการไข >40 องศาเซลเซยส แตถามดลกหดรดตวดแลวแตยงมเลอดออกอยแสดงวาเลอดออกจากสาเหตอน 5. ตรวจการฉกขาดของชองทางคลอดและปากมดลก จดผปวยในทา lithotomy เพอตรวจดการฉกขาดของชองคลอด ปากมดลกและเยบซอมจดทมเลอดออก โดยใชเครองมอถางขยายทเหมาะสม เชน Simpson หรอ Heaney retractors ในบางรายอาจพบกอนเลอด hematoma ขนาดใหญซงตองรกษาโดยการผาลมเลอดออก หรอวางทอระบายหรอใชผากอซบรรจใหแนนชองคลอด 6. ตรวจรกทคลอดออกมาอกครงวาครบหรอไมในกรณทรกลอกตวชาควรนกถงภาวะรกเกาะลกผดปกตเมอลวงรกและตรวจชนสวนของรกทคลอดออกมาวาไมหมดแสดงวานาจะมรกคางอยในโพลงมดลกรวมทงควรตรวจวารกมนอยหรอไมในกรณทสงสยวามเศษรกคาง ควรตรวจดวยคลนเสยงความถสงกอนทาหตถการใดๆบางรายอาจตอง
ใชมอลวงเขาไปในโพรงมดลกเพอเอาเศษรกและถงนาคราออก หากจาเปนอาจตองขดมดลกดวย curette ซงควรเลอกชนดทมขนาดใหญและปลายมน และสามารถใชคลนเสยงความถสงชวยในการทาหตถการได7. ถาตรวจทกอยางเบองตนแลวพบวาปกตใหตรวจสอบการแขงตวของมดลก8. ถามอาการชอกโดยเลอดทออกทางชองคลอดไมมากและไมไดสดสวนกบปรมาณเลอดทเสยไป แสดงวาอาจมเลอดออกในชองทอง ควรนกถงภาวะมดลกแตก
เปาหมายของการดแลภาวะตกเลอดหลงคลอดคอ การรกษาระดบของคาตางๆภายในเลอดดงตอไปน
- Hemoglobin > 8 g./dl- Platelet count > 7.5 x 109/l.- Prothrombin times < 1.5 x mean control
- Activated prothrombin times < 1.5 x mean control- Fibrinogen > 100 mg./dl.

[7]
ขณะทภาวะตกเลอดหลงคลอดทตยภม ( Secondary PPH ) มกพบมความสมพนธกบการตดเชอในโพรงมดลกมากกวาและการตกเลอดมกไมรนแรง สามารถใหการรกษาและตอบสนองเปนอยางด
กบ
การใหยาปฏชวนะ ในบทความนจะกลาวเนนถงการรกษา uterine atony ซงเปนสาเหตของภาวะตกเลอดหลงคลอดทพบมากและบอยทสดในเวชปฏบต การทดแทนเลอดทสญเสยไปและการรกษาระดบออกซเจนในกระแสเลอดเปนหลกการทสาคญทสดในการรกษาภาวะตกเลอดหลงคลอด อยางไรกตามสงทตองคดไวในใจเสมอคอ “ปรมาณเลอดทประเมนดวยตาเปลามกจะนอยกวาความเปนจรงเสมอ” ดงนนการใหเลอดเรวทสดเทาทจะทาไดเมอมภาวะตกเลอดหลงคลอดโดยไมจาเปนตองรอผลการตรวจทางหองปฏบตการจงเปนสงททมแพทยควรกระทามากทสดเมอพบและใหการวนจฉยภาวะตกเลอดหลงคลอดและชนดของเลอดทเหมาะสมทสดในภาวะนไดแก Packed red cell ขณะทการทดแทนสวนประกอบของเลอดอนๆหรอยาบางอยางควรปรกษาอายรแพทยโรคเลอดหรอแพทยเวชศาสตรธนาคารเลอดรวมดวย
! ตกเลอดหลงคลอดระยะแรก
รกคลอด
ครบ ไมครบ
ตรวจการหดรดตวของมดลก ชนสวนของรกคาง
ด ไมด
ตรวจชองทางคลอด
ฉกขาด ปกต
ตรวจชองทางคลอด ตรวจชองทางคลอด
มดลกไมหดรดตว

[8]
Uterine atony / Atonic Postpartum Hemorrhage 1. แนวทางการดแลเมอใหการวนจฉยวาเปน uterine atony Mechanical intervention Empty bladder (retained foley catheter) Bimanual uterine compression วธการทงายและทาไดรวดเรวทสดเมอเกด Uterine atony ไดแก การบบนวดมดลกเพอชวยเสรมการหดรดตวของมดลกโดยใชแรงจากมอทงสองขาง ( bimanual uterine compression ) และการสวนปสสาวะออกใหหมดพรอมกบการคาสายปสสาวะ แนะนาใหกระทาวธการนเปนอนดบแรกเมอวนจฉยวามารดามภาวะ uterine atony ขนตอนการทา bimanual uterine compression มดงน - ผกระทาสวมถงมอยาวปราศจากเชอใสมอหนงไปไวในชองคลอดและทาการลวงเอากอนเลอดทคางอยบรเวณ Lower uterine segment ออกทงหมด - กามอขางทอยในชองคลอดแลวดนเขาไปท anterior fornix จนรสกวาดนมดลกชนกบผนงหนาทอง - มออกขางหนงตานจากหนาทองผปวยจนถงดานหลงของมดลก - กดมอทงสองเขาหากนไวจนกระทงเลอดหยดและมดลกแขงตวด
UTERINE ATONY
2. Pharmacological intervention
ยาทใชรกษาในกรณ Uterine atony ชนดยา ขนาดทแนะนา ขอหาม/ขอควรระวง
Oxytocin ( Syntocinon® )*- 5 units by slow intravenous - แนะนาใหฉดเขาหลอดเลอดดาอยางชาๆ injection เพอไมใหเกด profound hypotension - 30 units ในสารนา NSS หรอ LRS - water intoxication 500 มลลลตรใหในอตรา125 ml./hr. - occasionally nausea and vomiting - 10 units intramyometrially (IMM)
Ergometrine, - Ergometrine 0.5 mg. by slow - หามใหในผปวย preeclampsia Methylergonovine maleate intravenous injection หรอมความดนโลหตสง(Methergin®) ** - Methylergonovine maleate 0.25 mg. - nausea and vomiting IM ซาไดทก 5 นาท แตไมเกน 1.25 mg.- Methylergonovine maleate 0.125 mg.
IV or IMM

[9]
ยาทรกษาในกรณ Uterine atony ชนดยา ขนาดทแนะนา ขอหาม/ขอควรระวง
15 methyl prostaglandin 0.25 mg. IM หรอ 0.5 mg. IMM ซาได - nausea, vomiting, diarrhea, headache ,F2α ( Carboprost ) ทก 15 นาท แตไมเกน 2 mg. hypertension, bronchospasm , flushing - diaphoresis and restlessness due to increased basal temperature - ไมแนะนาใหใชในผปวยโรคหดหอบ - relative contraindication ในผปวยโรคหวใจ , ตบและไตProstaglandin E1 1,000 mg. rectally or vaginally - ผลขางเคยงเชนเดยวกบ 15 misoprostol (Cytotec®) methyl prostaglandin F2α - แนะนาใหใชในกรณทไมม15 methyl prostaglandin F2α หรอผปวยทเปนโรคหอบหด - ไมแนะนาในขณะใหนมบตร
* แนะนาใหเลอกใชเปนอนดบแรก ** สามารถบรหารยารวมกบ Oxytocin ได
Surgical intervention Intrauterine balloon temponade Hemostatic brace suturing เชน B-lynch, modified compression suture Bilateral ligation of uterine arteries Bilateral ligation of internal iliac arteries Sengstaken-Blakemore tube Selective arterial embolization SOS Bakri tamponade ballon13 Hysterectomy(ในกรณทไมสามารถควบคมภาวะตกเลอดไดดวยวธขางตนและโดยเฉพาะในรายทเปน Placenta accrete หรอ uterine rupture )

[10]
Surgical interven.on
เมอการรกษาดวย bimanual uterine
compression และการใหยากระตนการหดรดตวของมดลกไมสามารถหยดภาวะตกเลอดหลงคลอดได การทาหตถการดงตอไปนเปนทางเลอกลาดบถดไปทควนพจารณาเพอควบคมการตกเลอดหลงคลอดกอนการตดสนใจตดมดลก โดยเฉพาะอยางยงในมารดาทยงตองการมบตรอยทงนการจะเลอกใชวธใดกอนหรอหลงขนอยกบการตดสนใจของทมแพทยผดแลเปนสาคญ
ในอดตการรกษาภาวะตกเลอดหลงคลอดดวยวธ
Uterine packing เปนวธการทยงยากและไมสามารถ
สงเกตและประมาณการเสยเลอด ไดอยางรวดเรวเนองจากผากอซทใชจะซบเลอดเอาไวในปรมาณมากจนเมอเหนเลอดออกจากชองคลอด มารดากไดเสยเลอดไปมากแลว Balloon tamponade จงไดถกคดคนขนมาเพอขจดปญหาดงกลาว โดยอาศยหลกการเดยวกนในการหยดเลอดคอ การใชแรงกด (pressure effect)
Balloon tamponade ทถกคดคนขนมามอยดวยกนหลายชนด แตกตางกนไปตามชนดของวสดทใชและการออกแบบ เชน Foley catheter,Bakri
balloon,Sengstaken-‐Blakemore oesophageal
catheter,Rusch hydrosta>c balloon catheter และ
Condom catheter เปนตน และการใชวธการนกสามารถ
ควบคมภาวะตกเลอดหลงคลอดไดเปนอยางด โดยมการศกษาพบวา Balloon tamponade สามารถลดการตด
มดลกในรายทมภาวะตกเลอดหลงคลอดรนแรงไดมากถง 78 %
วธการนอาจพจารณาเปนอนดบแรกเมอมภาวะตกเลอดหลงคลอดทควบคมไมได นอกจากนนยงใชเปนการทดสอบเพอพจารณาวาจาเปนตองทาการผาตดเพอหยดเลอดหรอไม เรยกวา “tamponade test” การทดสอบใหผลบวกหมายถง Balloon tamponade สามารถควบคม
หรอหยดเลอดทออกได และการทดสอบเปนลบเมอยงคงมภาวะตกเลอดหลงคลอดอยแมวาไดทา Balloon
tamponade แลว มารดากลมนจาเปนตองใหการรกษาดวยการผาตดวธอนตอไป
สาหรบระยะเวลาในการคา balloon นน สวนมากแนะนาวาระยะเวลาประมาณ 4-‐6 ชวโมงกเพยงพอทจะ
ทาใหเกดการแขงตวของเลอดและควบคมภาวะตกเลอดหลงคลอดได อยางไรกตามเมอจะเอา balloon ออกควรจะกระทาในชวงกลางวนและมแพทยผมประสบการณอยดวยเนองจากอาจเกดภาวะตกเลอดหลงคลอดซาซงจาเปนตองไดรบการรกษาดวยการผาตดตอไป
CONSERVATIVE SURGICAL MANAGEMENT
mass and plasma volume, which provides acompensative reserve for acute blood loss andhemostatic response following massive hemor-rhage14. Second, the arrangement of the uterinemuscle fibers, vis-à-vis the course of the uterinearteries, facilitates the use of compressiontechniques for effective control of postpartumhemorrhage and, finally, conservative treatmentsuch as bimanual compression of the uterusmay control blood loss (Figure 1), whilstintensive resuscitative measures are undertaken
according to established labor ward protocols,which involve the anesthetists, hematologists,the obstetric team and intensive care support(see Chapters 13 and 22).
NEW DEVELOPMENTS INTHERAPEUTIC OPTIONS
The type of surgical intervention dependsupon several factors, paramount of which is theexperience of the surgeon. Other factors includeparity and desire for future children, the extentof the hemorrhage, the general condition of thepatient and place of confinement. Women athigh risk of postpartum hemorrhage shouldnot be delivered in isolated units or unitsill-equipped to manage sudden, life-threateningemergencies. Immediate access to specialistconsultant care, blood products and intensivecare are essential.
The B-Lynch suture compressiontechnique
The procedure was first performed anddescribed by Mr Christopher B-Lynch, aconsultant obstetrician, gynecological surgeon,Fellow of the Royal College of Obstetriciansand Gynaecologists of the UK and Fellow of theRoyal College of Surgeons of Edinburgh, basedat Milton Keynes General Hospital NationalHealth Service (NHS) Trust (Oxford Deanery,UK), during the management of a patient with amassive postpartum hemorrhage in November1989. This patient refused consent to an emer-gency hysterectomy3! Table 2 provides an auditsummary of five case histories of other patientswith severe life-threatening postpartum hemor-rhage managed with this technique.
The principle
The suture aims to exert continuous verticalcompression on the vascular system. In thecase of postpartum hemorrhage from placentaprevia, a transverse lower segment compressionsuture is effective.
The technique2–4
See Figures 2a (i and ii), 2b and 2c.
288
POSTPARTUM HEMORRHAGE
Figure 1 Bimanual compression of the uterus,illustrating the first-line approach to mechanicalhemostasis. This in itself might control bleedingsignificantly by assisting the uterus to use itsanatomical and physiological properties such as thecross-over interlinked network of myometrial fibersfor vascular compression and bleeding control. Thepatient should be placed in stirrups or frog-leggedposition in the labor ward or in theater whilstintravenous fluid and/or appropriate blood productruns freely. In some cases and commonly so, theremay be failure to achieve satisfactory and lastinghemostasis by this method
310Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 15:00:04
Color profile: Generic CMYK printer profileComposite Default screen
304
POSTPARTUM HEMORRHAGE
Figure 1 Ligation of the anterior branch of the internal iliac artery with its associated vein.(a) Demonstrable vulnerability of internal iliac vein and obturator nerve in close proximity; (b) A ‘skeletal’anatomy, showing proximity of external iliac artery, ureter and anterior branches of sciatic nerve
(a)
(b)
326Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 15:03:24
Color profile: Generic CMYK printer profileComposite Default screen
Surgeon’s position In outlining the stepsinvolved, we assume that the surgeon is right-handed and standing on the right-hand side ofthe patient. A laparotomy is always necessary toexteriorize the uterus. A lower segment trans-verse incision is made or the recent lowersegment Cesarean section suture (LSCS)removed to check the cavity for retainedplacental fragments and to swab it out.
Test for the potential efficacy of the B-Lynch suturebefore performing the procedure The patient isplaced in the Lloyd Davies or semi-lithotomyposition (frog leg). An assistant stands betweenthe patient’s legs and intermittently swabs thevagina to determine the presence and extent ofthe bleeding. The uterus is then exteriorized
and bimanual compression performed. To dothis, the bladder peritoneum is reflected inferi-orly to a level below the cervix (if it has beentaken down for a prior LSCS, it is pushed downagain). The whole uterus is then compressed byplacing one hand posteriorly with the ends ofthe fingers at the level of the cervix and the otherhand anteriorly just below the bladder reflec-tion. If the bleeding stops on applying suchcompression, there is a good chance thatapplication of the B-Lynch suture will workand stop the bleeding.
Even in the presence of coagulopathy,bimanual compression will control diffusebleeding points. If this test is successful, theapplication of the suture will also succeed.
289
Conservative surgical management
Figure 2a–c Summary of the application of the B-Lynch procedure
(a(i)) (b)
(a(ii))(c)
311Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 15:00:52
Color profile: Generic CMYK printer profileComposite Default screen

[11]
Hemosta.c suturing
หมายถงวธการเยบมดลกเพอหยดเลอด ปจจบนมหลายวธการทไดรบการเผยแพรและคนพบวามประโยชนในการควบคมภาวะตกเลอดหลงคลอด โดย B-‐lynch suturing
เปนวธการแรกทถกคดคนขนมาตงแตป พ.ศ. 2540 และมรายงานการเยบมดลปแบบ B-‐lynch จานวนมากกวา
1,000 ราย ขณะทมเพยง 7 รายเทานนทลมเหลวในการหยดภาวะตกเลอดหลงคลอด ตอมาไดมผคดคนวธการเยบมดลกอกหลายแบบ เชน วธของ Hayman ทไมจาเปนตองผาตดเขาโพรงมดลก และวธของ Cho et al
ทแนะนาในรายทมภาวะ Placenta
previa หรอ Placenta
พบวาการใหการรกษาดวยวธ
การนมประสทธภาพในการควบคมภาวะการตกเลอดหลงคลอดไดดและสามารถลดการตดมดลกในรายทมภาวะตกเลอดหลงคลอดรนแรงไดมากถง 81% อยางไรกตามยงไมมขอสรปทจะบอกไดวาวธการใดทดกวากน ดงนนหากตดสนใจทจะใช Hemosta>c
suturing ในการรกษาภาวะตกเลอดหลงคลอด แพทยผดและควรฝกฝนวธการเยบดวยวธใดวธหนงจนชานาญและอยภายใตการควบคมของผมประสบการณ อยางไรกตามมรายงานถงผลแทรกซอนจากวธนไดเชน pyometra,par>al uterine necrosis
เปนตน
Internal iliac artery liga.on
การผก Internal iliac artery
เปนอกวธการหนงทนยมใชเพอหยดภาวะตกเลอดหลงคลอดทงนเพราะ Internal iliac artery เปนเสนเลอดหลกทหลอเลยงอวยวะในชองเชงกรานและการผกเสนเลอดดงกลาวไมพบวาทาใหเกดภาวะแทรกซอน
เชน ประจาเดอนผดปกตหรอมผลตอการมบตรในอนาคตแตอยางใด
นอกจากการผก Internal iliac artery
แลว แพทยสามารถเลอกผกเสนเลอดอนๆ ทเขาเลยงตวมดลกโดยตรงกได เชน bilateral uterine artery liga>on
หรอ bilateral uteroovarian vessels
liga>on เปนตน อยางไรกตามการ
รกษาดวยวธการนแนะนาใหทาในมารดาทมสญญาณชพอยในเกณฑคงทและยงคงมการตกเลอดอยในอตราทไมมาก
วธการนมประสทธภาพสงในการหยดเลอด โดยพบวาสามารถหยดเลอดไดมากถง 97% ในภาวะตกเลอด
ทางสตกรรม สาหรบภาวะตกเลอดหลงคลอดพบวา arterial
emboliza>on สามารถหยดภาวะตกเลอดหลงคลอดและลดการตดมดลกไดมากถง 71%
CONSERVATIVE SURGERY
304
POSTPARTUM HEMORRHAGE
Figure 1 Ligation of the anterior branch of the internal iliac artery with its associated vein.(a) Demonstrable vulnerability of internal iliac vein and obturator nerve in close proximity; (b) A ‘skeletal’anatomy, showing proximity of external iliac artery, ureter and anterior branches of sciatic nerve
(a)
(b)
326Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 15:03:24
Color profile: Generic CMYK printer profileComposite Default screen

ขอจากดเพยงอยางเดยวของการรกษาวธการนกคอจาเปนตองมเครองมอและรงสแพทยทมความชานาญซงอาจไมสามารถจดหาไดในหองคลอด อยางไรกตามวธการนสามารถทจะมบทบาทไดในราย
placenta previa with accrete ซงสามารถเตรยมการใสสายสวนไวตงแตกอนการผาตดและทาหตถการนเพอควบคมหรอลดการเสยเลอดในขณะผาตด สาหรบผลกระทบในระยะยาวนนพบวาวธการนไมมผลตอประจาเดอนหรอการมบตรในอนาคตแตอยางใด
Hysterectomy
การตดสนใจตดมดลกในภาวะตกเลอดหลงคลอดควรรบกระทาทนทโดยไมรรอหากไมสามารถควบคมการเสยเลอดได โดยเฉพาะอยางยงในมารดาทตรวจพบวาภาวะตกเลอดนนเปนผลมาจาก placenta accrete หรอ
uterine rupture นอกจากนนยง
แนะนาใหรบทาในมารดาทอยในภาวะวกฤตหรอแพทยผดแลไมมประสบการณในการผาตดหยดเลอดดวยวธอน โดยการผาตดอาจทาเพยง subtotal hysterectomy หาก
ตาแหนงทเลอดออกไมไดอยท lower
uterine segment หรอทปากมดลก
4T +1 TONETISSUETRAUMATHROMBINTRACTION
ภาวะนพบไดประมาณรอยละ 0.5-‐2 (24) โดยมสาเหตมาจากมดลกหดรดตวไมด ซงอาจเปนผลมาจากมเศษรกคาง การตดเชอ แตสาเหตทแทจรงนนยงไมทราบแนชด
ในรายทมดลกหดรดตวไมดสามารถรกษาดวยยากระตนการหดรดตวของมดลกเชนเดยวกบภาวะตกเลอดหลงคลอดทนท แตถาผปวยมเลอดออกไมมากแตมไขรวมกบอาการกดเจบบรเวณมดลก หรอนาคาวปลามกลนเหมน ควรนกถงภาวะ endometri>s และใหการรกษาดวย
ยาปฏชวนะทครอบคลมเชอ ไดแก gentamicin และ clindamycin แสดงยาปฏชวนะตวอนทสามารถใชรกษาได ในรายทสงสยเศษรกหรอเยอ
หมทารกคางการตรวจดวยคลนเสยง
ความถสงจะชวยในการวนจฉยไดโดยเหนลกษณะเปน
echogenic mass ในโพรงมดลกทมขนาดใหญ มรายงานเศษรกคางในโพรงมดลกภายหลงการผาตดคลอด
ซงผปวยควรไดรบการรกษาตอดวยการขดมดลก ภาวะนสามารถปองกนไดดวยการตรวจรกหลงคลอดอยางละเอยด และสงเกตดวามสวนของเนอรกหลดหายไปหรอไม ในรายทมดลกหดรดตวปกตการตรวจดวยคลนเสยงความถสงอาจเหนนาหนกเศษเนอคงอย ภายในโพรงมดลกได อยางไรกตามผปวยทมเลอดออกมากกวา 500 มล. และ
รกษาดวยยาไมไดผลควรใหการรกษาดวยวธ suc>on cureSage แต
ตองระวงภาวะแทรกซอนทอาจเกดตามมาไดแก ภาวะมดลกทะล หรอ
uterine synechiae นอกจากนยงม
รายงานการเกด late PPH จาก
pseudoanuerysm ของ uterine
artery ซงเปนสาเหตทพบไดนอยมากอาจเกดภายหลงคลอดทางชองคลอดหรอผาคลอดกได ภาวะดงกลาวสามารถวนจฉยดวยการตรวจคลนเสยงดอพพเลอรชนดส (Color
Doppler) สวนการรกษาทาไดดวยการเยบผกเสนเลอดทไปเลยงบรเวณดงกลาวหรอผาตดมดลก นอกจากนยงรกษาดวยการทา selec>ve
arterial emboliza>on
ภาวะตกเลอดหลงคลอดหลง 24 ชวโมง (LATE PPH)
จะเหนไดวาภาวะตกเลอดหลงคลอดเปนภาวะทปองกนได แตหากเกดขนแลวการดแลรกษาตองอาศยทมงานผมประสบการณผานการฝกฝนและปฏบตตามขนตอนอยางถกตอง แพทยผดแลตองตดสนใจสงการรกษาไดอยางรวดเรวและสอดคลองกบสถานการณ โดยไมควรปลอยใหเกดความลาชา เนองจากในชวงเวลาดงกลาวแมเพยงเสยววนาทกมคณคาเปนอยางมาก และชวยปองกนภาวะแทรกซอนทอาจถงชวตได อยางไรกตามสงหนงททมแพทยผดแลมกจะมองขามความสาคญไป ไดแก การแจงอาการและความรนแรง รวมถงผลการรกษาใหญาตของผปวยทราบเปนระยะๆอยางตอเนอง ซงจะชวยลดปญหาทจะตามมา และในบางครงญาตอาจจะชวยทมผดแลในการตดสนใจถงประเดนทสาคญบางเรอง นอกจากนการสอสารทดยงชวยใหเกดความเขาใจถงขนตอนการดแลรกษาและสรางความสมพนธอนด ซงจะชวยลดปญหาความเขาใจผดอนอาจนาไปสการฟองรองในภายหลงไดอกดวย
Late PostPartum Hemorrhage
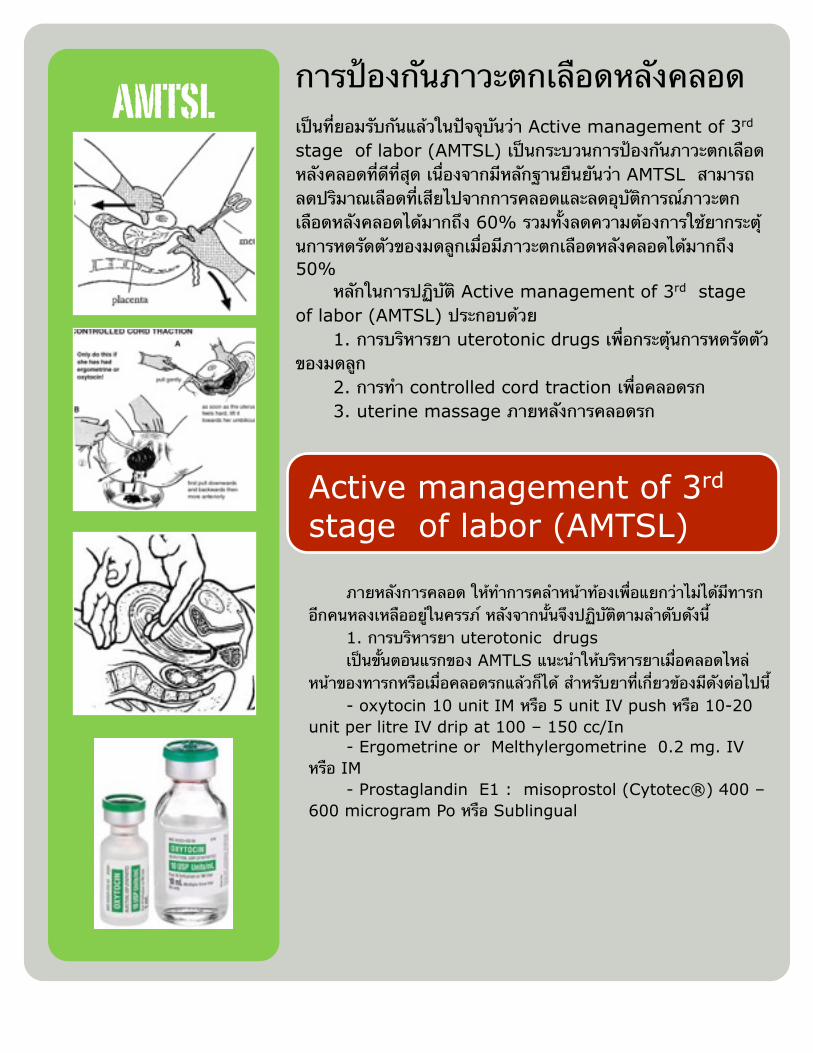
การปองกนภาวะตกเลอดหลงคลอดเปนทยอมรบกนแลวในปจจบนวา Active management of 3rd stage of labor (AMTSL) เปนกระบวนการปองกนภาวะตกเลอดหลงคลอดทดทสด เนองจากมหลกฐานยนยนวา AMTSL สามารถลดปรมาณเลอดทเสยไปจากการคลอดและลดอบตการณภาวะตกเลอดหลงคลอดไดมากถง 60% รวมทงลดความตองการใชยากระตนการหดรดตวของมดลกเมอมภาวะตกเลอดหลงคลอดไดมากถง 50% หลกในการปฏบต Active management of 3rd stage of labor (AMTSL) ประกอบดวย 1. การบรหารยา uterotonic drugs เพอกระตนการหดรดตวของมดลก 2. การทา controlled cord traction เพอคลอดรก 3. uterine massage ภายหลงการคลอดรก
AMTSL
Active management of 3rd stage of labor (AMTSL)
ภายหลงการคลอด ใหทาการคลาหนาทองเพอแยกวาไมไดมทารกอกคนหลงเหลออยในครรภ หลงจากนนจงปฏบตตามลาดบดงน 1. การบรหารยา uterotonic drugs เปนขนตอนแรกของ AMTLS แนะนาใหบรหารยาเมอคลอดไหลหนาของทารกหรอเมอคลอดรกแลวกได สาหรบยาทเกยวของมดงตอไปน - oxytocin 10 unit IM หรอ 5 unit IV push หรอ 10-20 unit per litre IV drip at 100 – 150 cc/In - Ergometrine or Melthylergometrine 0.2 mg. IV หรอ IM - Prostaglandin E1 : misoprostol (Cytotec®) 400 – 600 microgram Po หรอ Sublingual

2.Controlled cord traction มขนตอนการปฏบตดงตอไปน - ภายหลงการคลอดทารกแลว ทาการ clamp สายสะดอ ตาแหนงทใกลตอปากชองคลอด แลวใชมอหนงจบไว - วางอกมอหนงไวบรเวณเหนอตอกระดกหวเหนา แลว stabilized มดลกเอาไว เพอทจะออกแรง counter pressure กบแรงดงของอกมอหนงขณะทา controlled cord traction - ขงมอทตรงสายสะดอเอาไว แลวรอใหเกดการหดตวของมดลก - เมอมการหดตวของมดลก กระตนใหมารดาเบง พรอมกบดงสายสะดอลงในแนว downward อยางนมนวล ในจงหวะเดยวกบทอกมอหนงทา counter pressure - หลงจากทา controlled cord traction แลว 30 – 40 วนาท หากไมมการเคลอนตาลงของรกใหหยดทาหตถการแลวตรงสายสะดอเอาไว รอจนกวามการหดตวของมดลกในครงถดไป - เมอการหดตวของมดลกเกดขนใหม ใหกระทาหตถการเหมอนเชนเดมอกครง - ขณะทมการหดตวของมดลก หามทาการดงสายสะดอโดยไมม counter traction โดยเดดขาด - เมอรกคลอด ใหประคองดวยสองมอ แลวหมนจนเยอหมเดกเปนเกลยว พรอมกบดงรกเพอใหคลอดออกมาอยางนมนวล - หากมการขาดของเยอหมเดกขณะคลอดรก ใหทาการตรวจภายในชองคลอดและปากมดลกดวยวธปลอดเชอ หากมองเหนเศษเยอหมเดกใหใช sponge forceps คบออก - ทาการตรวจรกอยางละเอยด เพอใหแนใจวารกคลอดออกมาครบ หากตรวจพบวามสวนหนงสวนใดของรกขาดหายไป ใหสงสยวามภาวะรกคาง ใหปฏบตตามกรณรกคางตอไป
3. Uterine massage after delivery of placenta, as appropriate - ทาการนวดคลงมดลกบรเวณยอดมดลกผานทางหนาทองทนทจนมดลกมการหดรดตวด - ตรวจสอบการหดรดตวของมดลกทกๆ 15 นาท และทาการนวดคลงมดลกซาหากตรวจพบวามการหดรดตวทไมด โดยเฉพาะอยางยงในชวง 2 ชวโมงแรกหลงคลอด - หากจะหยดนวดคลงมดลก ตองมนใจวาการหดรดตวของมดลกอยในเกณฑดแลว
Active management of 3rd stage of labor

ขอแนะนาในการใหเลอดและองคประกอบของเลอดและผลลพธทได
ชนด องคประกอบ ผลลพธ Whole blood (1 ยนต = 500 มลลลตร)
ครบ ใชนอยมาก อาจใชในกรณทเสยเลอดปรมาณมากและให
packed red cell มากกวา 5−7 ยนตขนไป
Packed red cell (1 ยนต = 200 −250 มลลลตร)
เมดเลอดแดง 1 ยนตจะเพม hematocrit รอยละ 3
Fresh frozen plasma (1 ยนต = 500 มลลลตร)
Clotting factor ครบ ใชในการแกไขการแขงตวของเลอดผดปกต
เชน DIC , โรคตบ , ไดรบยา warfarin มากเกนไป 1 ยนตจะเพม fibrinogen ในเลอด 7−10 มลลกรมตอเดซลตร ขนาดทวไปทใชเทากบ 15 มลลลตรตอนำหนกตว 1 กโลกรม
Cryoprecipitate (1 ถง = 10 – 15
มลลลตร)
Fibrinogen factor V , VIII , XIII, von Willebrand factor
10 ถงจะเพม Fibrinogen ในเลอด 70 มลลกรมตอเดซลตร ในผปวยทมนำหนก 70 กโลกรม
Platelets (1 ถง = 50 มลลลตร)
เกลดเลอด 6 ยนตจะเพมเกรดเลอดประมาณ 30,000 ตอไมโครลตรในผใหญทมพนผวรางกาย 2.0 ตารางเมตร
เปาหมายของการดแลภาวะตกเลอดหลงคลอด คอ การรกษาระดบของคาตางๆภายในเลอดดงตอไปน
Hemoglobin > 8 g./dl Platelet count > 7.5 x 109/l. Prothrombin times < 1.5 x
mean control Activated prothrombin times
< 1.5 x mean control Fibrinogen > 100 mg./dl.

CONCLUSIONภาวะตกเลอดหลงคลอดถอวาเปนสาเหตสำคญของการเจบปวยและเสยชวตของมารดา การปองกนตามแผนกลยทธ และการวนจฉยไดเรวรวมทงใหการรกษาอยางเรงดวนจงจะลดความรนแรงของภาวะ
แทรกซอนได การรกษาอาจไมเพยงพอถาไมสามารถประเมนการสญเสยเลอดไดถกตองและแปลผลการตอบสนองของมารดาตอภาวะฉกเฉนทผด ทมงานในหองคลอดตองทราบวธการบรหารจดการกบภาวะเลอดออกใหทนเวลา รวมทงการประสานงานกบคลงเลอดและเจาหนาทหองปฏบตการ การประสานงานทดของทมงานทงสตแพทย วสญญแพทย กมารแพทย แพทยทางโลหตวทยา
และแพทยเวชบำบดวกฤต รวมทงทมงานในหองคลอด การปฏบตตามแนวทางทถกตองอยางมประสทธภาพ จงจะสามารถชวยทารกและมารดาทเกดปญหาได
Prakarn OngArtboon OB-GYN Department Phrae Hospital PhraeMEC


Statewide Maternity and Neonatal Clinical Guideline: Primary postpartum haemorrhage
Refer to online version, destroy printed copies after use Page 3 of 17
Flowchart: Primary postpartum haemorrhage

References
1. El-Refaey H, Rodeck C. Post partum haemor-rhage: definitions, medical and surgical manage-ment. A time for change. Br Med Bull 2003;67:205–17
2. World Health Organization. The Prevention andManagement of Postpartum Haemorrhage. Reportof a Technical Working Group, Geneva, 3–6July, 1989. Unpublished document. WHO/MCH/90.7. Geneva: World Health Organiza-tion, 1990
3. Pritchard JA, Baldwin RM, Dickey JC, WigginsKM. Blood volume changes in pregnancy andthe puerperium. Am J Obstet Gynecol 1962;84:1271–82
4. Newton M. Postpartum hemorrhage. Am JObstet Gynecol 1966;94:711–17
5. De Leeuw NK, Lowenstein L, Tucker EC,Dayal S. Correlation of red cell loss at deliverywith changes in red cell mass. Am J ObstetGynecol 1968;100:1092–101
6. Letsky E. The haematological system. In HyttenF, Chamberlain G, eds. Clinical Physiology inObstetrics, 2nd edn. Oxford: Blackwell, 1991:2–75
7. Baskett TF, ed. Complications of the third stageof labour. In Essential Management of ObstetricalEmergencies, 3rd edn. Bristol, UK: Clinical Press,1999:196–201
8. Alexander J, Thomas P, Sanghera J. Treatmentsfor secondary postpartum haemorrhage.Cochrane Database of Systematic Reviews,2005, Issue 3
9. Gahres EE, Albert SN, Dodek SM. Intrapartumblood loss measured with Cr 51-tagged erythro-cytes. Obstet Gynecol 1962;19:455–62
10. Newton M, Mosey LM, Egli GE, Gifford WB,Hull CT. Blood loss during and immediatelyafter delivery. Obstet Gynecol 1961;17:9–18
11. Prata N, Mbaruku G, Campbell M. Using thekanga to measure post partum blood loss. Int JGynaecol Obstet 2005;89:49–50
12. National Centre for Classification in Health.Australian Coding Standards. The InternationalStatistical Classification of Diseases and RelatedHealth Problems, Tenth Revision, AustralianModification (ICD-10-AM). Sydney, Australia,2002
13. American College of Gynecologists and Obstetri-cians. Quality Assurance in Obstetrics and Gynecol-ogy. Washington DC: American College ofObstetricians and Gynecologists, 1989
14. Sobieszczyk S, Breborowicz GH. Managementrecommendations for postpartum hemorrhage.Arch Perinatal Med 2004;10:1
15. Benedetti T. Obstetric haemorrhage. In GabbeSG, Niebyl JR, Simpson JL, eds. A PocketCompanion to Obstetrics, 4th edn. New York:Churchill Livingstone, 2002:Ch 17
15
Definitions and classifications
Hemorrhage class Estimated blood loss (ml) Blood volume loss (%) Clinical signs and symptoms
0 (normal loss) < 500 < 10 noneALERT LINE
1 500–1000 < 15 minimalACTION LINE
2 1200–1500 20–25 ! urine output" pulse rate" respiratory ratepostural hypotensionnarrow pulse pressure
3 1800–2100 30–35 hypotensiontachycardiacold clammytachypnea
4 > 2400 > 40 profound shock
Need observation ± replacement therapyReplacement therapy and oxytocicsUrgent active managementCritical active management (50% mortality if not managed actively)
Table 4 Proposed classification. Adapted from Benedetti15
37Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:19:08
Color profile: Generic CMYK printer profileComposite Default screen
6
Supplies and logistics
The sufficient availability of high-quality uterotonic drugs, needles, and syringes at national and local levels is essential for routine use of AMTSL. Effective use of AMTSL also implies appropriate conditions during transport and storage to ensure the use of chemically active drugs and safe, sterile needles and syringes.
Figure 1. Determinants of the routine use of AMTSL.
Womanreceives AMTSL
Policy
Provider
Logistics
Historicalprecedent, influence ofleader,WHO,in-servicetraining
Nationalguidelines
Presence inpre-service training
AMTSL protocolin hospital
Expectedbehaviorin hospital
Knowledge,skills inAMTSL
Motivationto use
Implementation
Uterotonicsincluded onEssentialDrug List(oxytocin=drug of choice)
Sufficientamount procured
Transportissues
Procure-mentat hospitallevel
Availabilityof sufficientoxytocics,needles,syringe on site
Properstorage
“Champions” foruse of AMTSL
The aim of this study is to provide ministries of health (MOHs) and their international partners with the descriptive information necessary to assess AMTSL practices and identify major barriers to its use. The findings will inform interventions that improve adoption and implementation of AMTSL and provide policymakers with the information they need to promote skilled attendance at birth. A third aim of this study is to produce tools and a method that others could employ to document the current practice of AMTSL. The study’s specific research questions are as follows:
1. For what proportion of deliveries is AMTSL used at a national level? Which components of AMTSL (e.g., prophylactic use of oxytocic agents, controlled cord traction, fundal massage) are practiced, and how consistently are they practiced?
2. Is AMTSL formally promoted in the Standard Treatment Guidelines (STGs) in each country at national and/or facility levels? If so, since when? How is AMTSL defined in the standards?
3. How is the need for AMTSL drugs quantified at national and facility levels?
4. Which uterotonic drug (e.g., oxytocin, ergometrine, or a prostaglandin) is used? How is it stored?
5. At the facility level, is enough oxytocin available to allow for routine use of AMTSL?

Normal delivery results in predictable lossesof 300–500 ml blood volume for vaginal deliver-ies and 750–1000 ml for Cesarean section births(see Chapter 4). However, in addition to bloodlost from the body, a substantial amount ofblood is also redirected into the systemic circu-lation, often referred to as the autotransfusioneffect. This results in an increase in cardiac out-put by as much as 80%. The effect persists inuncomplicated patients, gradually returning tonon-pregnant levels at 2–3 weeks5.
ASSESSMENT OF CIRCULATINGBLOOD VOLUME
Young healthy adults can compensate for theloss of large volumes from the circulation withfew obvious external signs. Accurate assessmentof blood loss can be difficult for the experiencedas well as the inexperienced examiner, asdescribed in Chapter 4.
In cases of hemorrhage symptoms often pre-cede signs. These include unexplained anxietyand restlessness, the feeling of breathlessness(with or without an increased respiratory rate),and a sensation of being cold or generallyunwell. For healthy, non-pregnant adults, hypo-volemia and associated signs can be divided intofour stages (Table 1). These range from thelargely undetectable stage 1 with less than 15%loss of volume, to the severe life-threateningstage when more than 40% has been lost.Unfortunately, comparable tables for early andlate pregnancy and the immediate postpartum
period have not been compiled, but the signsfollow a similar pattern.
The most important principle in the treat-ment of postpartum hemorrhage is early recog-nition and prompt correction of lost circulatingvolume, together with simultaneous medicaland/or surgical intervention to prevent furtherloss. Early recognition of life-threatening physi-ological derangements can be improved by theuse of early-warning scoring systems.
Recording physiological observations atregular intervals has long been routine practicein hospitals. Early-warning scores derived fromsimple routine physiological recordings canidentify patients with greater risk of criticalillness and mortality. Such scores can be usedto flag the early but sometimes subtle signs ofconcealed but largely compensated hemorrhagein the early postpartum patient and have beenrecently recommended for use by the Confiden-tial Enquiry into Maternal and Child Healthreport of 20047. These scores use the physiolog-ical parameters most likely to detect impendinglife-threatening compromise. These usuallycomprise respiratory rate, heart rate, systolicblood pressure, temperature and mental aware-ness. Each variable is assigned a weighted scoreand the total score is the sum of these. Thisallows a trigger value for ward staff to call forassistance from intensive care or other seniorstaff. Such systems have been shown to bereproducible and effective at predicting thelikelihood of progressing on to critical illness.They are well suited to the early detection of the
46
POSTPARTUM HEMORRHAGE
Classification Class 1 Class 2 Class 3 Class 4
Blood loss(% volume lost)
Conscious state
Respiratory rateComplexionExtremitiesCapillary refillPulse rateSystolic blood pressureUrine output
10–15%
Alert, mildthirst
normalnormalnormalnormalnormalnormalnormal
15–30%
anxious andrestless
mildly elevatedpalecool
slow (> 2 s)normalnormalreduced
30–40%
agitated orconfused
raisedpale
pale and coolslow (> 2 s)
elevatednormal or slightly low
reduced
> 40%
drowsy, confused orunconscious
raisedmarked pallor or gray
coldminimal or absentfast but thready
hypotensiveoligoanuric
Modified from Baskett PJF. ABC of major trauma. Management of hypovolaemic shock. BMJ 1990;300:1453–7
Table 1 Stages of shock
68Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:19:24
Color profile: Generic CMYK printer profileComposite Default screen
normal as the volume in the venous capacitancebecomes replete (line C to D). Thus, volumeadministration should be rapid but infused indiscrete volume challenges, with the effect onthe right atrial filling pressure, systemic bloodpressure and other hemodynamic variablesbeing monitored. Commonly, 250–500 ml ofeither a crystalloid or a colloid is administeredover a period of 10–20 min as the urgencydictates (a patient with life-threatening class 4shock will receive 2–3 liters more quickly,but, even then, the principles of monitoring thehemodynamic variables during the infusion offluid remain). Simple measures of tissue under-perfusion, which may persist after apparentrestoration of global hemodynamics, include thebase deficit and serum lactate. Efforts to mea-sure and enhance tissue perfusion should con-tinue until all such parameters return to normal.More specific measures to monitor tissue perfu-sion, including tissue oxygen tension devices19
and gastric tonometry20, are not widely used.The best fluid to use for volume expansion in
hemorrhagic shock remains a matter of debate.Both crystalloid and colloid are effective, buteach has advantages and disadvantages21 (Table3). One recent large study showed no difference
in mortality in intensive care patients requiringvolume expansion whether this expansion wasmade with saline or albumin22. Colloids expandthe intravascular space preferentially, whereascrystalloids quickly become distributed through-out the extracellular space. Saline has the disad-vantage of hyperchloremia, which causes adilutional or hyperchloremic acidosis23,24. Theuse of crystalloids is not associated with anaphy-laxis, whereas colloids such as the gelatins canproduce severe life-threatening reactions,although this is less common with hydroxyethylstarch25. Crystalloids have minimal effect on co-agulation other than a dilutional effect, althoughsaline infusions may have a procoagulant effect26.Overall, crystalloids have a lower cost and lowerincidence of side-effects, but the colloids haveseveral theoretical advantages regarding tissueedema and oxygen delivery to the tissues.Despite intense debate and research interest,neither crystalloids nor colloids have beenshown to be superior to one another regardingsurvival outcome from hemorrhagic shock.
It is essential that a protocol be availablefor the use of blood products in instances ofmassive bleeding. In the UK, the responsibilityfor maintaining such a protocol lies with the
51
Assessing and replenishing lost volume
Type of fluid Advantages Disadvantages
CrystalloidsSaline cheap; easily available; long history of use produces a hyperchloremic acidosis;
small procoagulant effectHartmann’s no risk of anaphylaxis; minimal direct effect on
the base deficit; easily availablemildly hypotonic
5% dextrose no place in acute expansion of the intravascularspace
hypotonic; no significant expansion ofthe vascular space; rapid distribution tointracellular and extracellular spaces
Hypertonicsaline
rapid expansion of the intravascular space inexcess of the volume infused; possible beneficialeffects on red cell and endothelial edema andcapillary blood flow
insufficient data; uncertainty regardingpossible adverse effects such as on theimmune system
ColloidsGelatins largely remains in the intravascular space for
2–4 hrisk of anaphylaxis; no clear survivaladvantage over crystalloids
4% humanalbumin
more physiological than gelatins; remainspredominantly in the intravascular space for 12 h
expensive; no clear survival advantageover crystalloids
Hydroxyethylstarch
remains in the intravascular space for 12–24 h risk of coagulopathy, renal injury andreticulo-endothelial accumulation
Table 3 Intravenous fluids
73Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:19:25
Color profile: Generic CMYK printer profileComposite Default screen

173
Resuscitation
Immediate actions Key points Other considerations
! Arrest bleeding ! Early surgical or obstetric intervention! Upper G/I tract procedures! Interventional radiology
! Contact key personnel ! Most appropriate surgical team! Duty anesthetist! Blood bank
! Restore circulating volumeN.B. In patients with majorvessel or cardiac injury,it may be appropriate torestrict volume replacementafter discussion with surgicalteam
! Insert wide-bore peripheral cannulae! Give adequate volumes of
crystalloid/blood! Aim to maintain normal blood
pressure and urine output > 30 ml/hin adults (or 0.5 ml/kg/h)
! Blood loss is oftenunderestimated
! Refer to local guidelines for theresuscitation of trauma patientsand for red cell transfusion
! Monitor CVP ifhemodynamically unstable
! Request laboratoryinvestigations
! FBC, PT, APTT, fibrinogen; bloodbank sample, biochemical profile,blood gases
! Repeat FBC, PT, APTT, fibrinogenevery 4 h, or after one-third bloodvolume replacement, or after infusionof FFP
! Take samples at earliestopportunity as results may beaffected by colloid infusion
! Misidentification is mostcommon transfusion risk
! May need to give FFP &platelets before the FBC andcoagulation results available
! Request suitable red cellsN.B. All red cells are nowleukocyte-depleted. Thevolume is provided on eachpack, and is in the range of190–360 ml
! Blood needed immediately – use‘Emergency stock’ group O Rh(D)-negative
! Blood needed in 5–10 min – type-specificwill be made available to maintainO Rh (D)-negative stocks
! Blood needed in 30 min or longer – fullycross-matched blood will be provided
! Contact blood transfusionlaboratory or oncall BMS andprovide relevant details
! Collect sample for group andcross-match before usingemergency stock
! Blood warmer indicated if largevolumes are transfused rapidly
! Consider the use ofplatelets
! Anticipate platelet count < 50 ! 109/lafter > 2 liters blood loss with continuedbleeding
! Dose: 10 ml/kg body weight for aneonate or small child, otherwise one‘adult therapeutic dose’ (one pack)
! Target platelet count:-> 100 ! 109/l for multiple/CNStrauma> 50 ! 109/l for other situations
! Consider early use of plateletsif clinical situation indicatescontinued excessive blood lossdespite the count
! Consider the use of FFP ! Anticipate coagulation factor deficiencyafter > 2 liters blood loss with continuedbleeding
! Aim for PT & APTT < 1.5 ! meancontrol
! Allow for 20-min thawing time! Dose: 12–15 ml/kg body wt = 1 liter
or 4 units for an adult
! PT/APTT > 1.5 ! meancontrol correlates withincreased surgical bleeding
! May need to use FFP beforelaboratory results available:take sample for PT, APTT,fibrinogen before FFPtransfused
continued
Table 2 Acute massive blood loss: a template guideline
195Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:20:38
Color profile: Generic CMYK printer profileComposite Default screen
an adult, and the objective should be to aim fora PT and APTT less than 1.5 control level. FFPrequires a thawing time of 20 min, and henceearly anticipation of a potential requirement ishelpful.
Cryoprecipitate
It is appropriate to administer cryoprecipitatewhich contains fibrinogen and factor VIIIwhen there is evidence of a consumptivecoagulopathy with a fibrinogen level lessthan 0.5 g/l. The normal dose is 10 units. Aswith FFP, cryoprecipitate needs thawing time.The aim is to restore the fibrinogen level to> 1.0 g/l.
Coagulopathy
Coagulopathy can develop rapidly in an obstet-ric patient. Confirmatory laboratory tests arerequired for precise diagnosis, but in the clinicalsetting of postpartum hemorrhage the presenceof microvascular bleeding is a good clinical indi-cator18,19. Absence of clotting with continuedbleeding strongly suggest a coagulopathy.Hemostasis is normally adequate when clottingfactors are greater than 30% of normal18–21. Ifbleeding continues in the presence of clottingfactors > 30% normal and a PT and APTT lessthan 1.5 times control level, it is unlikely thatlow coagulation levels are responsible18,19.
Disseminated intravascular coagulopathy
Disseminated intravascular coagulopathy(DIC) represents the most deadly form of
coagulopathy wherein a vicious cycle consumesclotting factors and platelets rapidly. DIC candevelop dramatically in obstetric patients, espe-cially in association with placental abruptionand amniotic fluid embolism. It also occurssuddenly after massive bleeding with shock,acidosis and hypothermia. This latter riskemphasizes the importance of warming allinfused fluids whenever possible. DIC carriesa high mortality and, once established, canbe difficult to reverse. Patients with prolongedhypovolemia are particularly at risk. The diag-nosis can be made by frequent estimation ofplatelets, fibrinogen, PT and APTT. Treatmentconsists of administering platelets, FFP andcryoprecipitate sooner rather than later.
Complications of blood transfusion
Increasing awareness of the risks of transfusionhas led to diminished use of blood and bloodproducts in recent years. Complications canoccur because of incompatibility, storage prob-lems, and transmission of infection.
The most common cause of a transfusion-related death is incompatibility leading to ahemolytic reaction22. Most of such deaths aredue to misidentification and are entirely pre-ventable, emphasizing the importance of safesystems for cross-checking all blood products.
Storage problems include hyperkalemia, aspotassium levels rise in stored blood which, ifgiven rapidly and repeatedly, can give rise tohyperkalemia, especially in an acidotic, hypo-thermic patient. Similarly, hypothermia canincrease if large volumes of cold stored bloodare given rapidly without a blood warmer.
174
POSTPARTUM HEMORRHAGE
Immediate actions Key points Other considerations
! Consider the use ofcryoprecipitate
! To replace fibrinogen & FVIII! Aim for fibrinogen > 1.0 g/l! Allow for 20-min thawing time! Dose: 10 packs or 1 pack/10 kg in
children
! Fibrinogen < 0.5 stronglyassociated with microvascularbleeding
! Suspect DIC ! Treat underlying cause if possible ! Shock, hypothermia, acidosis,risk of DIC
! Mortality if DIC is high
For abbreviations, see text
Table 2 Continued
196Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:20:38
Color profile: Generic CMYK printer profileComposite Default screen




























