-
ΗΗ ΑΔΕΝΟΫΠΟΦΥΣΗΑΔΕΝΟΫΠΟΦΥΣΗ:: OI OI ΓΟΝΑΔΟΤΡΟΠΙΝΕΣΓΟΝΑΔΟΤΡΟΠΙΝΕΣ
((FSH, FSH, LHLH) ) ΚΑΙΚΑΙ ΗΗ ΠΡΟΛΑΚΤΙΝΗΠΡΟΛΑΚΤΙΝΗ ((PRLPRL))
ΚωνσταντίνοςΚωνσταντίνος
ΚαλλαράςΚαλλαράςΙατρόςΙατρός
ΠαθολόγοςΠαθολόγος
ΚαθηγητήςΚαθηγητής
ΦυσιολογίαςΦυσιολογίαςΕργαστήριοΕργαστήριο
ΠειραματικήςΠειραματικής
ΦυσιολογίαςΦυσιολογίας
ΙατρικήςΙατρικής
ΣχολήςΣχολής ΑΑ..ΠΠ..ΘΘ..
-
FSH:ΜΒ
∼33000, περιεκτικότητα
σε σιαλικό
οξύ
αρκετή
LH
(ICSH): ΜΒ
∼
28000, περιεκτικότητα
σε
σιαλικό
οξύ
περιορισμένη
α-υπομονάδα
και
των
δύο: Μ.Β.14900
β-υπομονάδα
FSH:110 αμινοξέα
β-υπομονάδα
LH:
121 αμινοξέα
Η σύνθεση των β-υπομονάδων καθοριστικό
όριο
(rate limiting)
για
την
ποσότητα
των
γοναδοτροπινών
«Ειδικότητα
στο
είδος»
Μετρήσεις: βιομετρήσεις, RIA, RRA
Σύνδεση
με
υποδοχείς
με
την
α- υπομονάδα
μόνο
επί
παρουσία
της
β
→ Gs
αδενυλκυκλάση
-
Περιεκτικότητα
υποφύσεως
σε γοναδοτροπίνες
ποικίλλει
σημαντικά:
↑↑μετά
εμμηνόπαυση
σε
γυναίκες
και μετά
τα
50 στους
άνδρες
Στο
αίμα: ↑↑μετά
εμμηνόπαυση
σε γυναίκες
και
στο
μέσον
του
κύκλου
(φασική
έκκριση)
LΗ: στους
άνδρες
8-10 εκκριτικές αιχμές
στο
24ώρο
με
υψηλότερες
τιμές
την
6.00 πρωινή
(τονική έκκριση)
T1/2
FSH = 3 h, T1/2
LH = ∼60 min
Ρυθμός
νεφρικής
κάθαρσης: FSH/LH 7:1.Έτσι
στα
ούρα
πολύ
μεγαλύτερες
ποσότητες
FSH παρά
LH
-
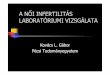
Figure
23-34.
Episodic
secretion
of LH (s) and
FSH (d) during
the
follicular
stage
(top)
and
the
luteal stage
(bottom)
of
the
menstrual
cycle. The
numbers
above
each graph
indicate
the
numbers
of
LH
pulses
per
12 hours
and
the
plasma estradiol
(E2) and
progesterone (P)
concentrations
at
these
two
times
of the
cycle. (Reproduced, with
permission, from
Marshall
JC, Kelch RO: Gonadotropin-releasing
hormone: role
of
pulsatile
secretion
in the
regulation
of
reproduction. N Engl
J Med
1986;315:1459.)
-
Η
ρύθμιση
της εκκρίσεως
των
γοναδοτροπινών
-
Η προλακτίνη (PRL)
M.B. = 26364, 198 αμινοξέα
-
Τιμές
: : 6,2 ± 0,6 μg/l, : 9,0 ± 0,6 μg/l
Αύξηση
: 2ο
ήμισυ
κυήσεως, αρχικές
φάσεις γαλουχίας. Μεγαλύτερες
τιμές
στον
τοκετό,
προοδευτική
πτώση
από
την
8η
ημέρα
-
Η
ρύθμιση
της
έκκρισης
της
PRL
-
Sleep-associated changes in prolactin (PRL) and growth hormone
(GH) secretion in humans. Peak levels of GH occur during sleep
stages 3 or 4; the increase in PRL is observed 1–2 hours after
sleep begins and is not associated with a specific sleep phase.
(Reproduced, with permission, from Sassin JF et al: Human
prolactin: 24- hour pattern with increased release during sleep.
Science 1972;177:1205.)
-
Figure
8-22
Effect
of hyperprolactinemia
on
suppressing
follicle-stimulating hormone
(FSH) and
luteinizing
hormone
(LH) secretory patterns
leading
to
hypogonadotrophism
in
a female
patient. PRL,
prolactin. (Adapted from Tolis G. Prolactin: physiology and
pathology. Hosp Pract 1980;15:85-95.)
Kronenberg: Williams
Textbook
of
Endocrinology, 11th ed.
-
Figure 23-39. Hormonal control of breast development and
lactation in rats. Estrogens (E) plus someprogesterone (P) and some
prolactin in the presence of glucocorticoids (C), insulin (I), and
growth hormone(GH) cause duct proliferation and growth at puberty
(right). During pregnancy, all of these hormones bringabout full
alveolar development and some milk secretion (below). After
delivery, increased secretion ofprolactin and a decline in estrogen
and progesterone levels bring about copious milk secretion and, in
thepresence of oxytocin, ejection of milk (left). Chorionic
mammotropin is the lactogenic hormone presumablysecreted by the
placenta in rats and is analogous to hCS. It supplements the action
of prolactin.
-
Η νευροϋπόφυση: οι ορμόνες Βαζοπρεσσίνη και Οξυτοκίνη
-
Δραστικότητα
Lys-Βαζοπρεσσίνης
: 65-70% της αντιδιουρητικής
δράσης
της
Arg-Βαζοπρεσσσίνης
-
Figure
14-11.
Structure
of
bovine
prepropressophysin (left)
and
prepro-oxyphysin
(right).
Gly
in
the
10 position
of
both
peptides
is
necessary
for
amidation
of
the
Gly
residue in
position
9. aa, amino
acid
residues. (Reproduced, with
permission, from
Richter
D: Molecular
events
in
expression of
vasopressin
and
oxytocin
and
their
cognate
receptors.
Am
J Physiol
1988;255:F207.)
-
ΠεριεκτικότηταΠεριεκτικότητα πλάσματοςπλάσματος σεσε ΑΑDH DH
:1:1 pmol/lpmol/lΧρόνοςΧρόνος υποδιπλασιασμούυποδιπλασιασμού ADH
ADH :: 88--2020minminΧρόνοςΧρόνος υποδιπλασιασμούυποδιπλασιασμού
OT: 5 minOT: 5 minMMεταβολισμόςεταβολισμός ADH ADH σεσε ήπαρήπαρ
καικαι νεφρούςνεφρούςADHADH + + ΟΤΟΤ ευρίσκεταιευρίσκεται
επίσηςεπίσης σεσε υπερχιασματικόυπερχιασματικόπυρήναπυρήνα, ,
γενννητικούςγενννητικούς αδένεςαδένες, , φλοιόφλοιό
επινεφριδίωνεπινεφριδίωνΑΑDH DH →→VV1A1A
((αγγειοδιαταλτικήαγγειοδιαταλτική δράσηδράση), ), VV1B 1B
((δράσηδράση σταστακορτικοτρόπακορτικοτρόπα)) →→ PLC & CaPLC
& Ca2+2+
ΑΑDH DH →→ VV22 ((αντιδιουρητικήαντιδιουρητική δράσηδράση) ) →→
αδενυλκυκλάσηαδενυλκυκλάση
-
Key
Aspects
of
Posterior Pituitary
Hormones
Oxytocin Arginine
vasopressinReceptor Gq/11
protein-coupled G protein
-
coupled
(V1
R, Gq/11
, V2
R, Gs
)
Second messenger
Phospholipase C [Ca2+]i
(V1
R) Phospholipase C [Ca2+]i
(V2
R) Adenylate
cyclase
cAMPTarget
organ
or
cellsUterusMammary
myoepithelial
cells
V2
R; kidney
collecting
ductsV1
R; smooth
muscle
cells
Physiologic effectsUterine
contraction
Milk
ejectionIncreased
H2
O permeabilityVasoconstriction
-
JOSE´
ANTUNES-RODRIGUES, MARGARET DE CASTRO, LUCILA L. K. ELIAS,
MARCELO M. VALENC¸
A, AND SAMUEL M. McCANN. Neuroendocrine
Control
of
Body
Fluid
Metabolism. Physiol Rev 2004 84:169-208
-
Figure 14-8. Diagrammaticrepresentation of the way in
whichchanges in plasma osmolality andchanges in ECF volume affect
thirst byseparate pathways.
-
Figure 14-7. Relation of plasmaosmolality to thirst in healthy
adulthumans during infusion of hypertonicsaline. The intensity of
thirst ismeasured on a special analog scale. (Reproduced, with
permission, fromThompson CJ et al: The osmoticthresholds for thirst
and vasopressinrelease are similar in healthyhumans. Clin Sci Lond
1986;71:651.)
-
Figure
14-12.
Responses
of magnocellular
neurons
to
stimulation.
The
tracings
show
individual extracellularly
recorded
action
potentials, discharge
rates, and intramammary
duct
pressure. A:
Response
of
an
oxytocin-secreting neuron. HFD, high-frequency
discharge;
ME, milk
ejection. Stimulation
of
nipples started
before
the
onset
of
recording. B:
Responses
of
a vasopressin-secreting neuron, showing
no
change
in
the
slow
firing
rate
in
response
to
stimulation
of nipples
and
a prompt
increase
in
the
firing
rate
when
5 mL
of
blood
was drawn, followed
by
typical
phasic
discharge. (Tracings
from
Wakerly
JB: Hypothalamic
neurosecretory
function:
Insights
from
electrophysiological studies
of
the
magnocellular
nuclei.
IBRO News
1985;4:15.)
-
Figure
14-13.
Relation between
plasma
osmolality
and
plasma
vasopressin
in healthy
adult
humans
during
infusion
of hypertonic
saline. LD, limit
of
detection. (Reproduced, with
permission, from
Thompson
CJ et
al: The osmotic
thresholds
for
thirst
and
vasopressin
are similar
in
healthy
humans.
Clin
Sci
[Colch] 1986;71:651.)
-
Figure
14-14.
Relation
of mean
arterial
blood
pressure
to
plasma
vasopressin
in healthy
adult
humans
in
whom
a progressive
decline in
blood
pressure
was
induced
by
infusion
of graded
doses
of
the
ganglionic
blocking
drug trimethaphan. The
relation
is
exponential
rather
than linear. (Drawn
from
data
in
Baylis
PH: Osmoregulation and
control
of
vasopressin
secretion
in
healthy
humans. Am
J Physiol
1987;253:R671.)
-
Figure
14-15.
Effect
of
hypovolemia and
hyper-volemia
on
the
relation
between
plasma
vasopressin
(pAVP) and
plasma
osmolality
(posm). Seven
blood
samples
were
drawn
at
various times
from
ten
normal
men
when
hypovolemia
was
induced
by
water deprivation
(colored
circles, dashed
line) and
again
when
hypervolemia was
induced
by
infusion
of
hypertonic
saline
(black circles, solid
line). Linear
regression
analysis
defined
the
relationship
pAVP
= 0.52 (posm
- 283.5) for
water
deprivation
and
pAVP
= 0.38 (posm
-
285.6) for hypertonic
saline. LD, limit
of
detection. Note
the
steeper
curve
as well
as
the
shift
of
the
intercept
to
the
left
during
hypovolemia. (Courtesy
of CJ Thompson.)
-
Figure 32-7.Circumventricular organs. Theneurohypophysis (NH),
organum vasculosum of thelamina terminalis (OVLT, supraoptic
crest), subfornicalorgan (SFO), and areapostrema (AP) are
shownprojected on a sagittal sectionof the human brain. SCO,
subcommissural organ; PI, pineal.
Η ΑΔΕΝΟΫΠΟΦΥΣΗ:� OI ΓΟΝΑΔΟΤΡΟΠΙΝΕΣ (FSH, LH) ΚΑΙ Η ΠΡΟΛΑΚΤΙΝΗ
(PRL)Slide Number 2Slide Number 3Slide Number 4Slide Number 5Slide
Number 6Slide Number 7Slide Number 8Slide Number 9Slide Number
10Slide Number 11Slide Number 12Slide Number 13Slide Number 14Slide
Number 15Slide Number 16Slide Number 17Slide Number 18Slide Number
19Slide Number 20Slide Number 21Slide Number 22Slide Number 23Slide
Number 24Slide Number 25Slide Number 26Slide Number 27Slide Number
28Slide Number 29Slide Number 30Slide Number 31Slide Number 32



![1. Mô tả nồng độ LH, tỉ số LH/FSH ở bệnh nhân vô …nồng độ tăng LH cao khoảng 60% ở bệnh nhân buồng trứng đa nang [2] và được nhìn nhận](https://img.pdfslide.tips/doc/110x75/5e5d815c79b84b61d027612c/1-m-t-nng-lh-t-s-lhfsh-bnh-nhn-v-nng-.jpg)