Embed Size (px)
Citation preview

WIR SCHAFFEN WISSEN – HEUTE FÜR MORGEN
Radiotherapy for intracranial meningiomas
SAMO Interdisciplinary Workshop on Brain Tumors and Metastases 18.-19. November 2016
PD Dr Alessia Pica, Pr Damien Charles Weber: Paul Scherrer Institut
Introduction
Type of ‘radiotherapies’and RTQA
Management of Grade 1 Meningiomas
Management of non-grade 1 Meningiomas
NRG/EORTC prospective trials
Conclusions
Plan
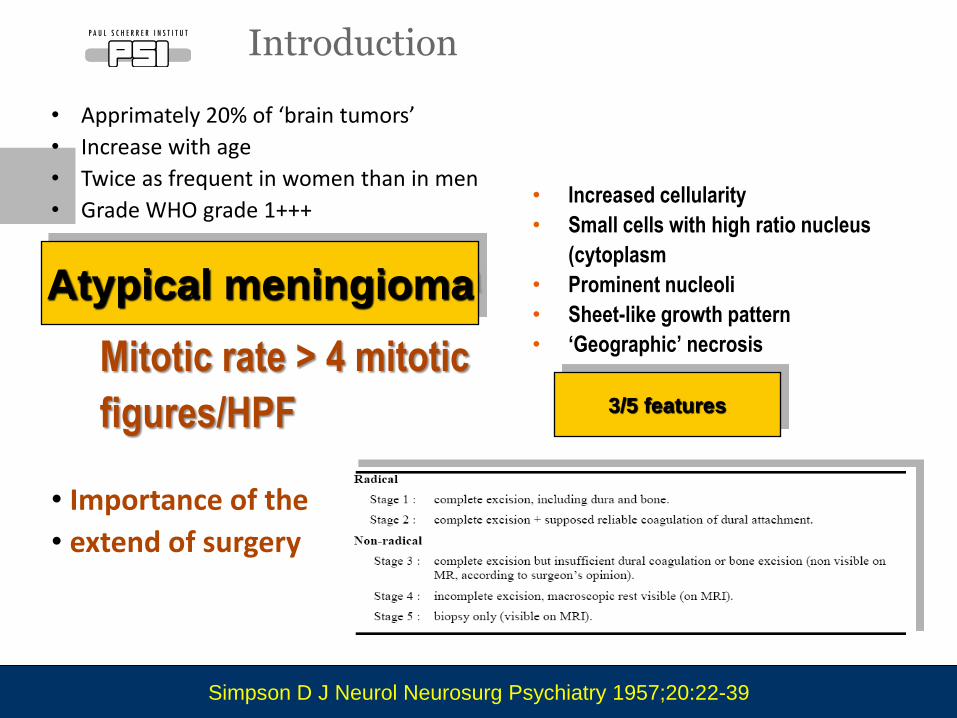
• Apprimately 20% of ‘brain tumors’
• Increase with age
• Twice as frequent in women than in men
• Grade WHO grade 1+++
• Importance of the
• extend of surgery
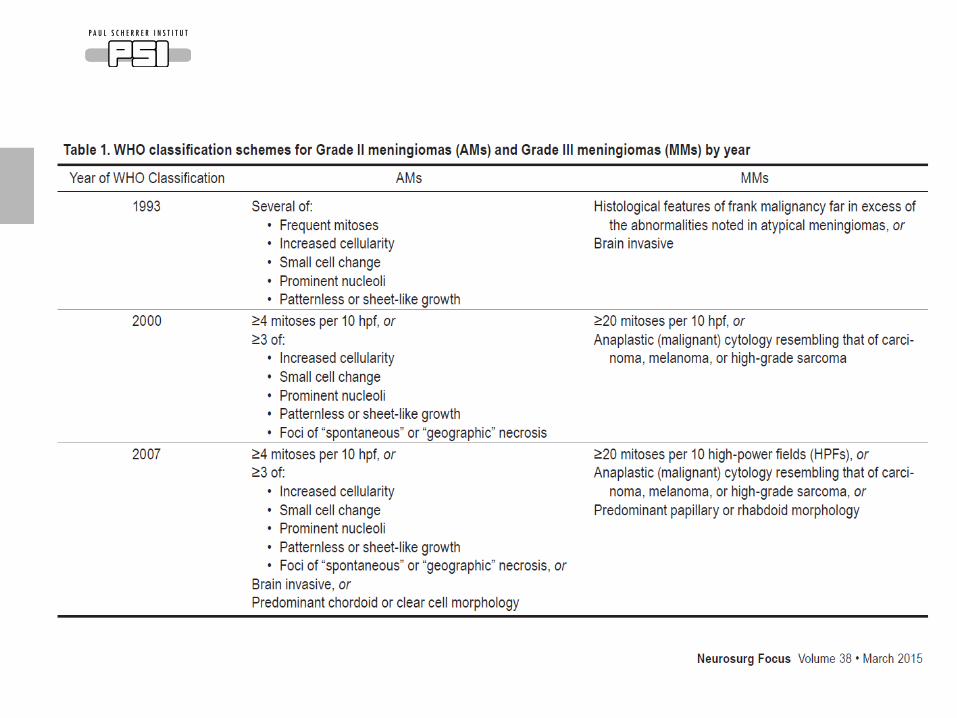
Introduction
Mitotic rate > 4 mitotic
figures/HPF
• Increased cellularity
• Small cells with high ratio nucleus
(cytoplasm
• Prominent nucleoli
• Sheet-like growth pattern
• ‘Geographic’ necrosis
3/5 features
Atypical meningioma
Simpson D J Neurol Neurosurg Psychiatry 1957;20:22-39
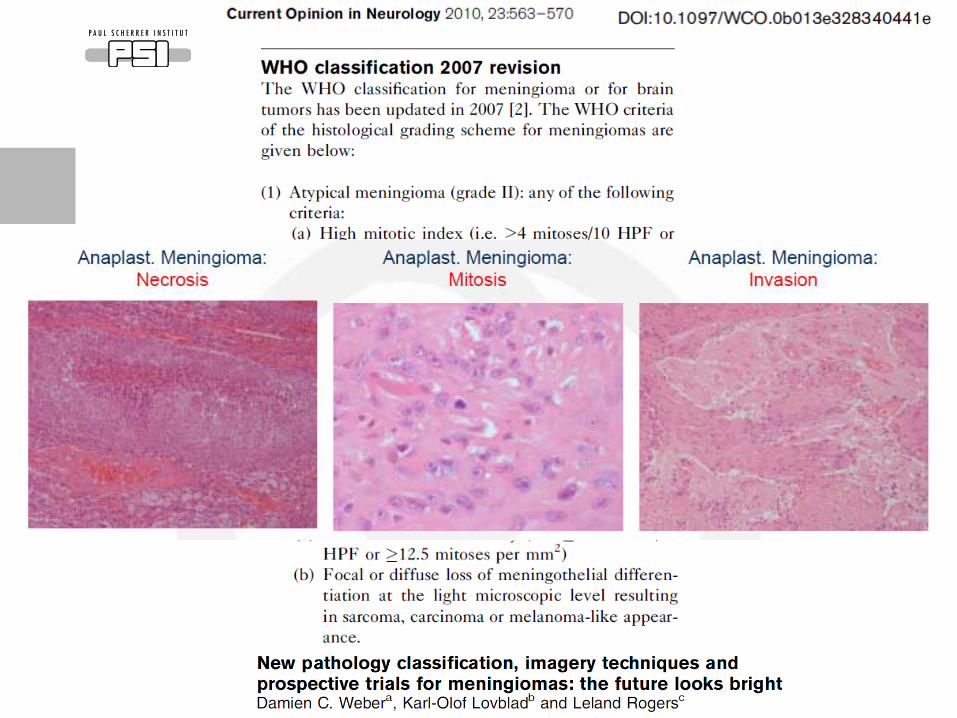
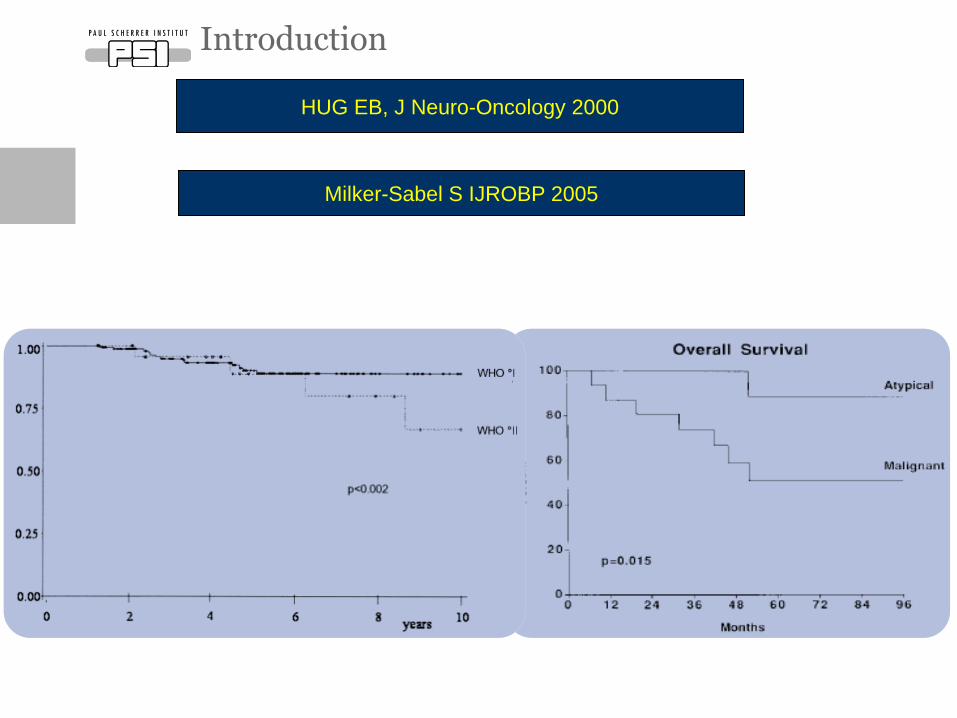
Introduction
HUG EB, J Neuro-Oncology 2000
Milker-Sabel S IJROBP 2005
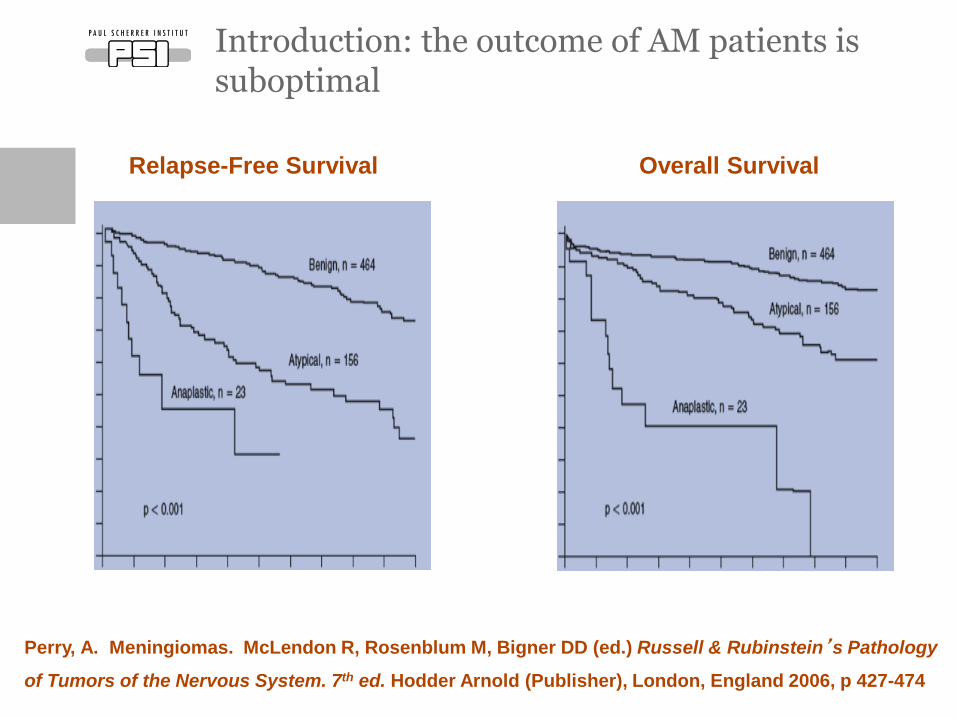
Perry, A. Meningiomas. McLendon R, Rosenblum M, Bigner DD (ed.) Russell & Rubinstein’s Pathology
of Tumors of the Nervous System. 7th ed. Hodder Arnold (Publisher), London, England 2006, p 427-474
Introduction: the outcome of AM patients is suboptimal
Relapse-Free Survival Overall Survival
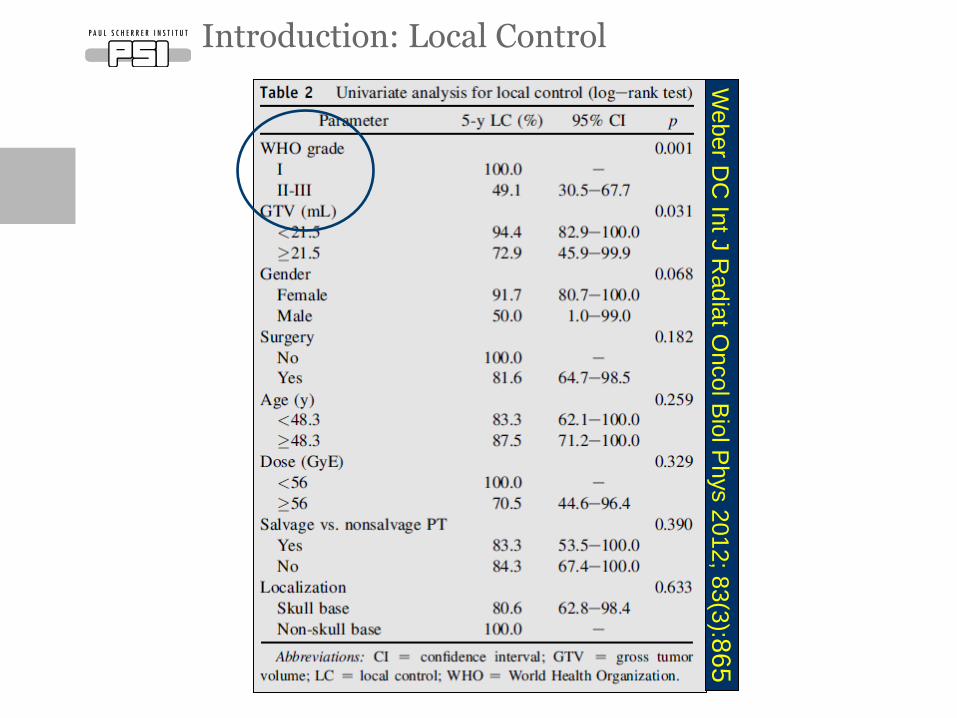
Introduction: Local Control
Weber D
C In
t J R
adia
t Oncol B
iol P
hys 2
012; 8
3(3
):86
5
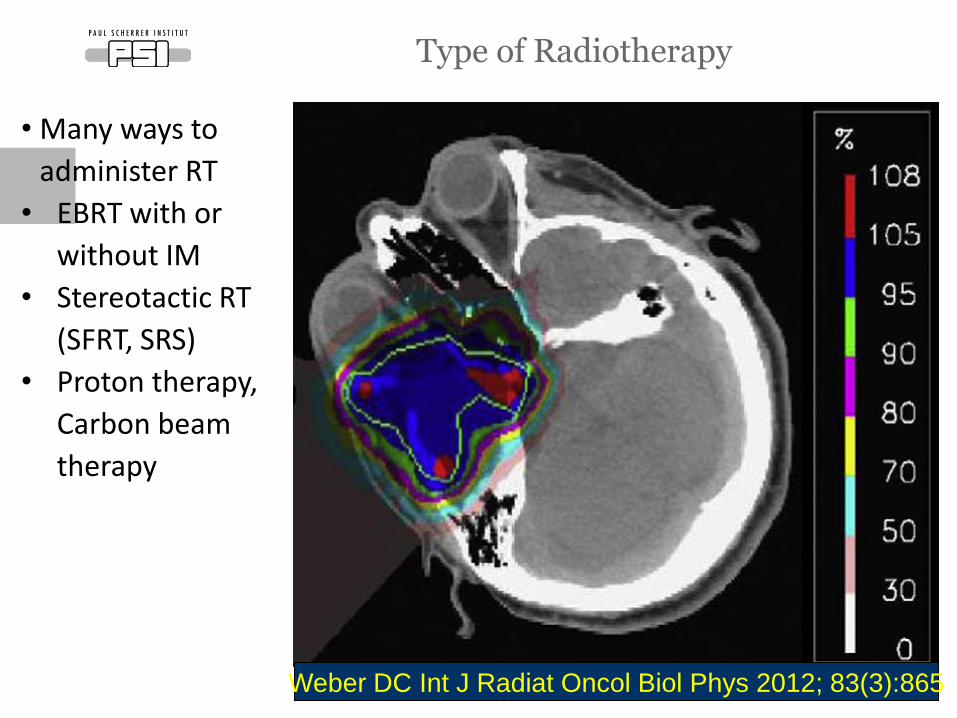
• Many ways to
administer RT
• EBRT with or
without IM
• Stereotactic RT
(SFRT, SRS)
• Proton therapy,
Carbon beam
therapy
Type of Radiotherapy
Weber DC Int J Radiat Oncol Biol Phys 2012; 83(3):865
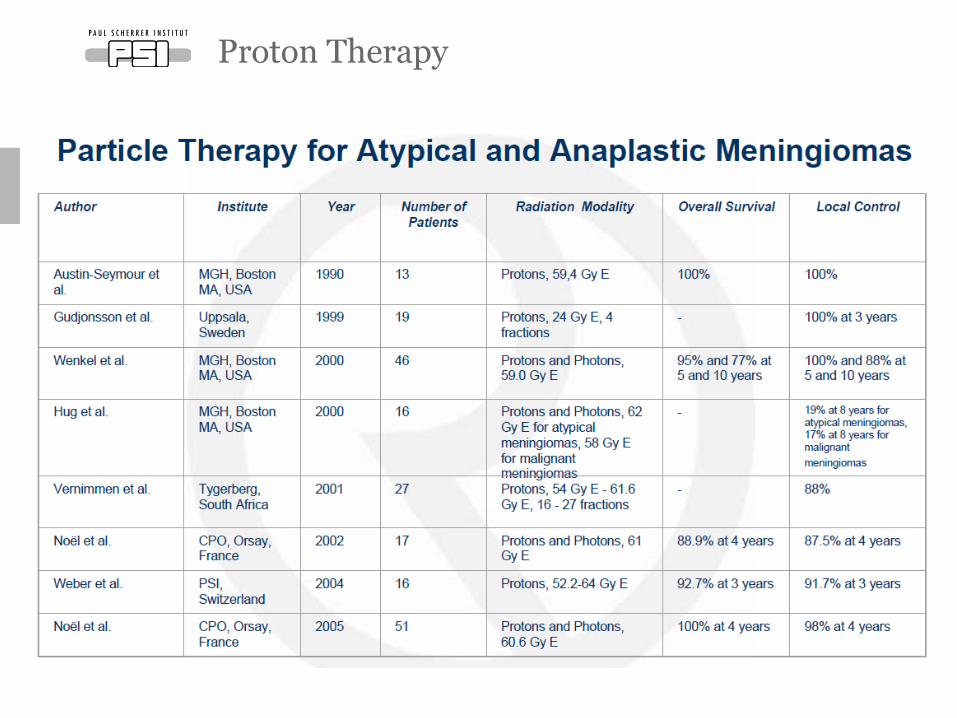
Proton Therapy
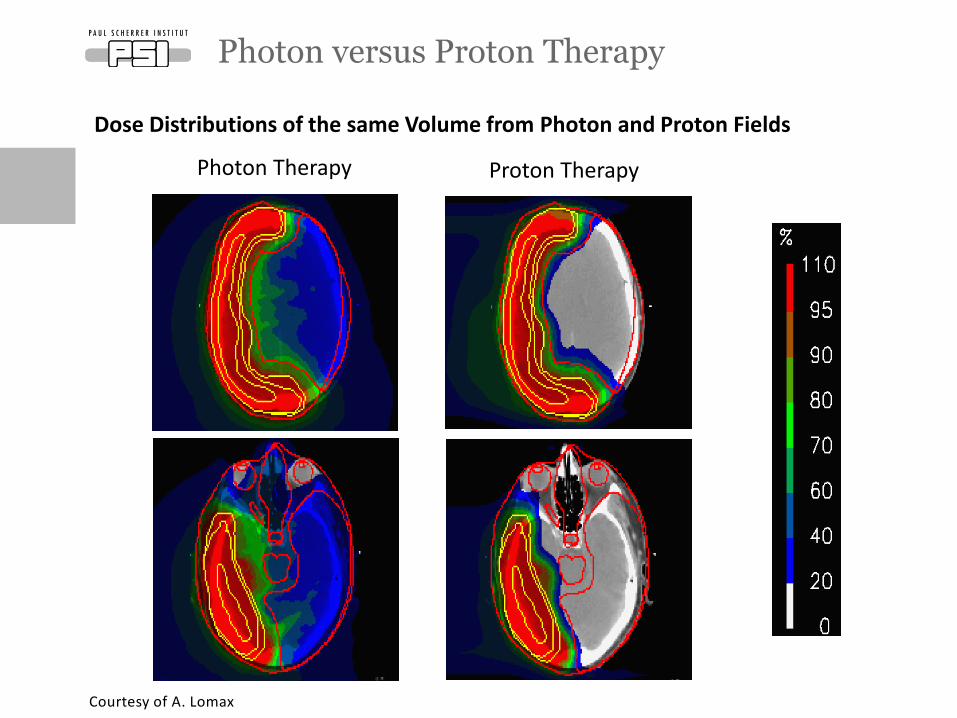
Photon versus Proton Therapy
Photon Therapy Proton Therapy
Dose Distributions of the same Volume from Photon and Proton Fields
Courtesy of A. Lomax
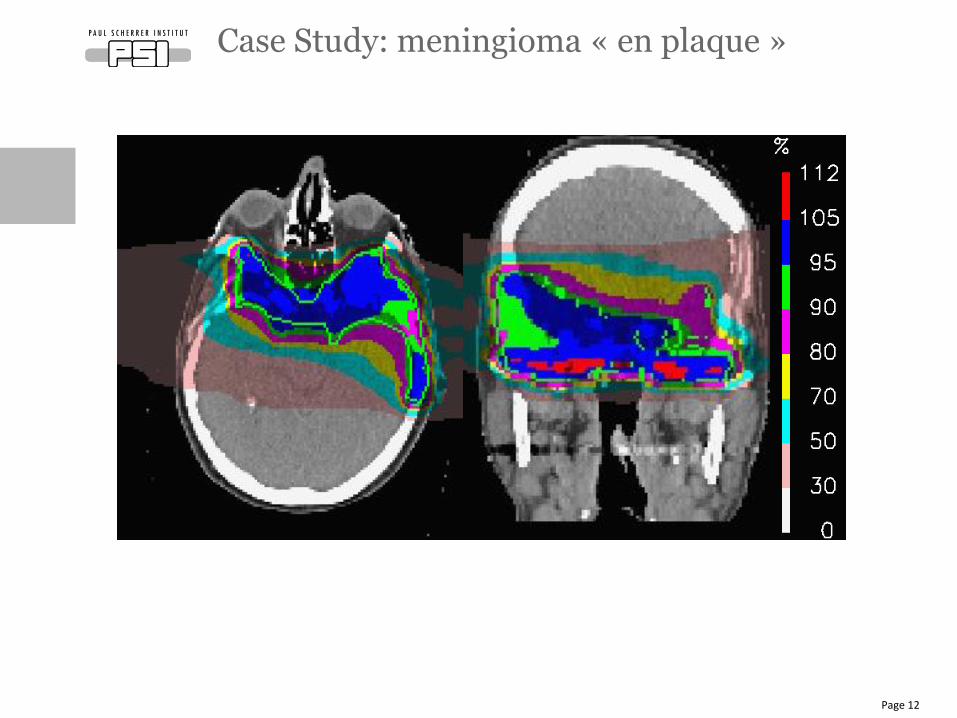
Case Study: meningioma « en plaque »
Page 12
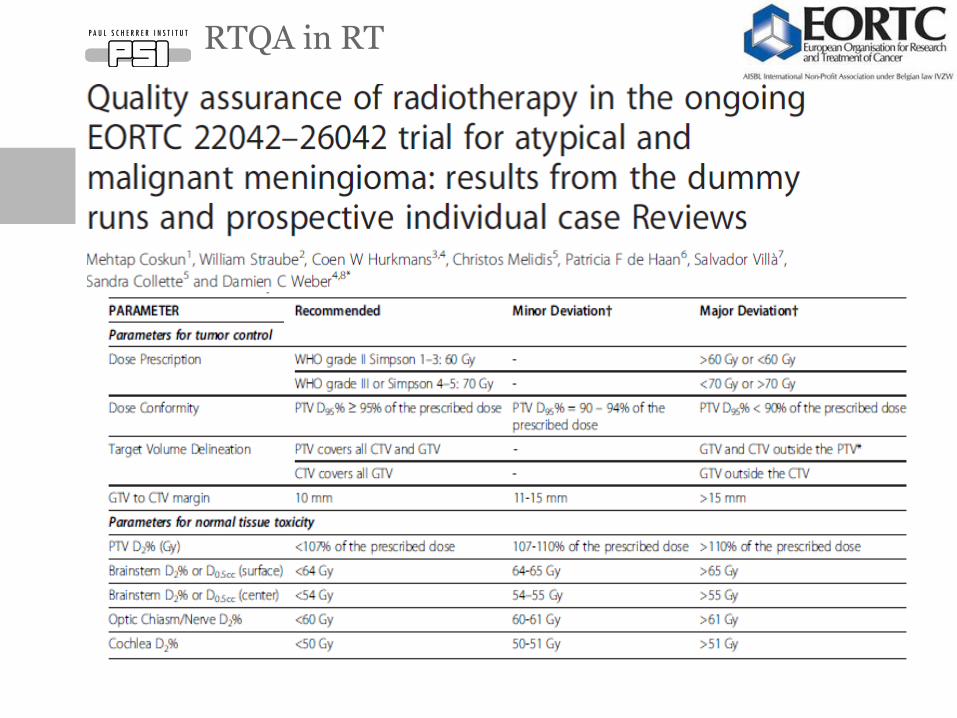
RTQA in RT
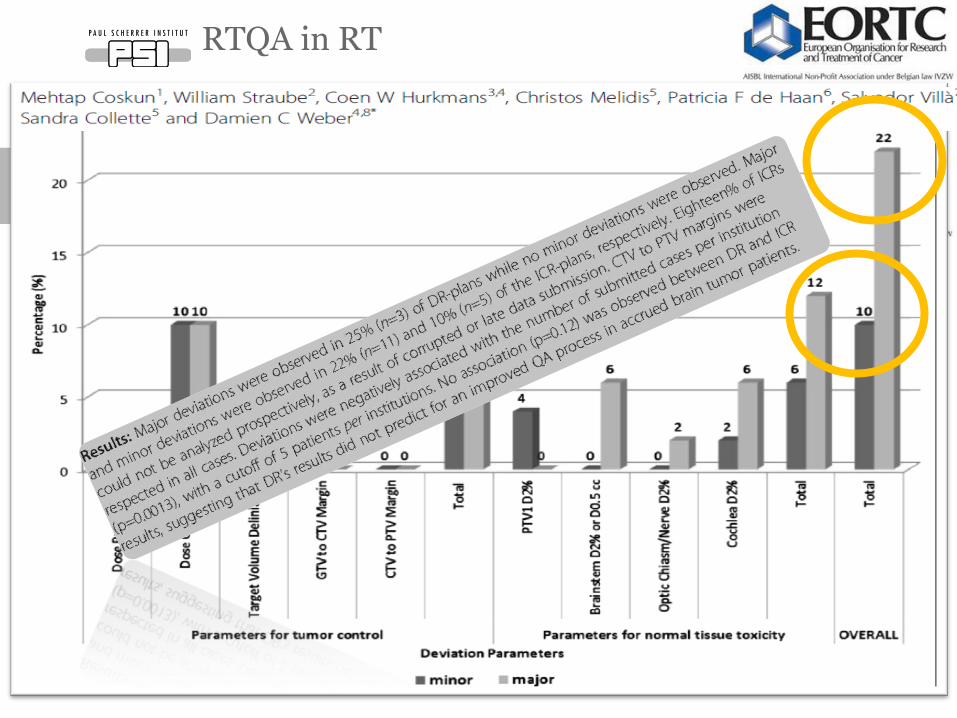
RTQA in RT
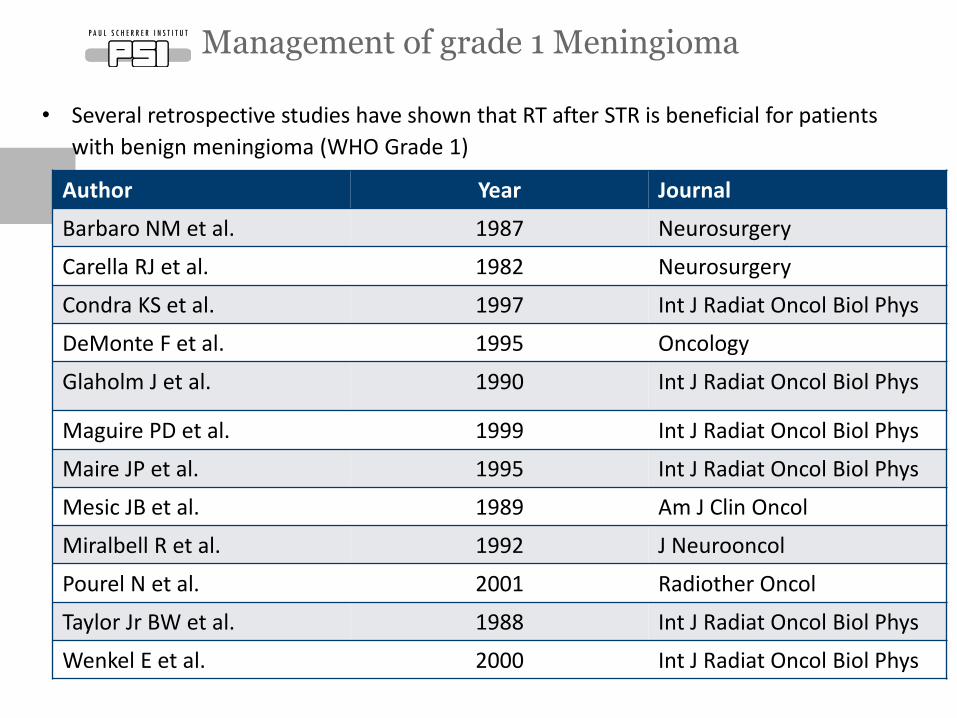
• Several retrospective studies have shown that RT after STR is beneficial for patients
with benign meningioma (WHO Grade 1)
Management of grade 1 Meningioma
Author Year Journal
Barbaro NM et al. 1987 Neurosurgery
Carella RJ et al. 1982 Neurosurgery
Condra KS et al. 1997 Int J Radiat Oncol Biol Phys
DeMonte F et al. 1995 Oncology
Glaholm J et al. 1990 Int J Radiat Oncol Biol Phys
Maguire PD et al. 1999 Int J Radiat Oncol Biol Phys
Maire JP et al. 1995 Int J Radiat Oncol Biol Phys
Mesic JB et al. 1989 Am J Clin Oncol
Miralbell R et al. 1992 J Neurooncol
Pourel N et al. 2001 Radiother Oncol
Taylor Jr BW et al. 1988 Int J Radiat Oncol Biol Phys
Wenkel E et al. 2000 Int J Radiat Oncol Biol Phys
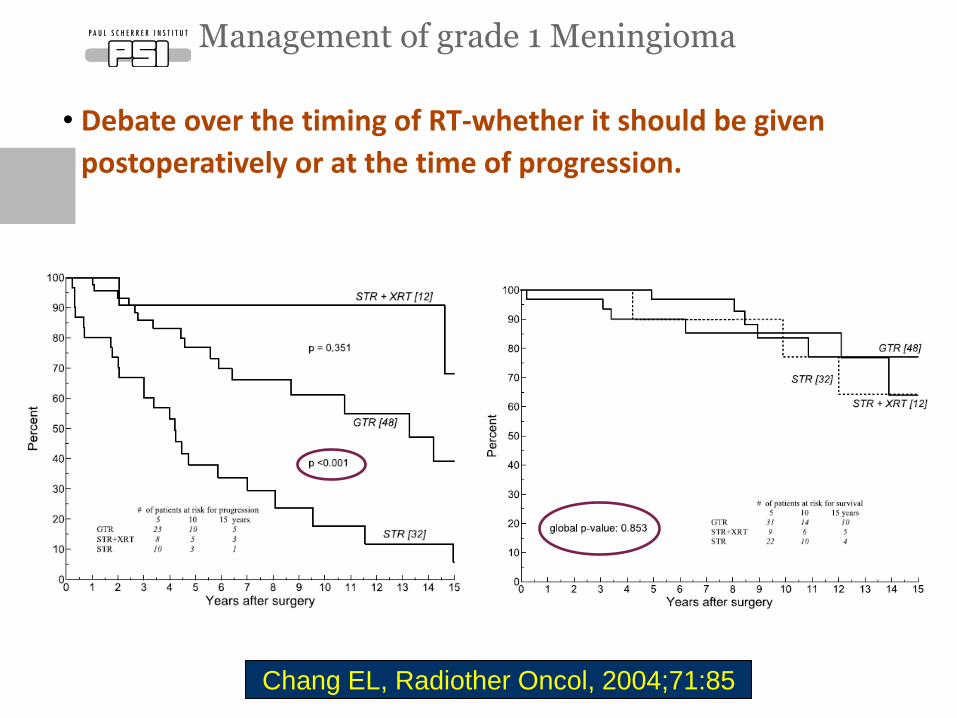
• Debate over the timing of RT-whether it should be given
postoperatively or at the time of progression.
Management of grade 1 Meningioma
Chang EL, Radiother Oncol, 2004;71:85
• Phase III trial assessing the impact of radiation therapy on tumor
control and QoL for patients with non-gross total resection
• (Simpson 3) as documented on MRI performed 1 month
postoperatively.
• Targeted sample size of 478 patients was calculated
• and the protocol was activated in 2004.
Management of grade 1 Meningioma
Weber DC, Curr Opinion Neurol 2010;23:563-79
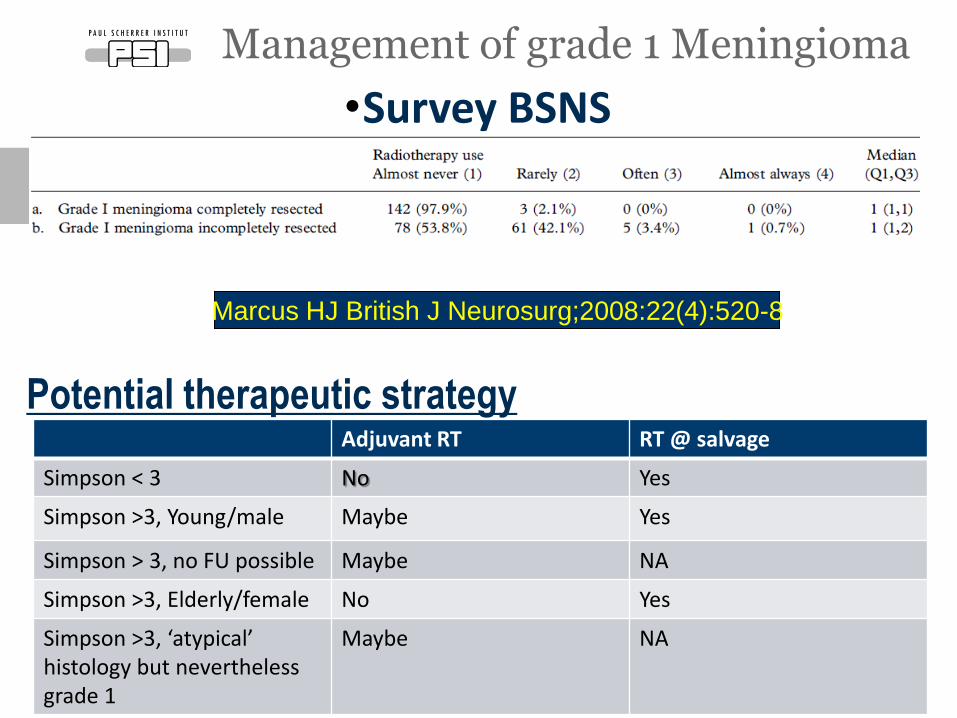
•Survey BSNS
Management of grade 1 Meningioma
Seite 18
Adjuvant RT RT @ salvage
Simpson < 3 No Yes
Simpson >3, Young/male Maybe Yes
Simpson > 3, no FU possible Maybe NA
Simpson >3, Elderly/female No Yes
Simpson >3, ‘atypical’ histology but nevertheless grade 1
Maybe NA
Marcus HJ British J Neurosurg;2008:22(4):520-8
Potential therapeutic strategy
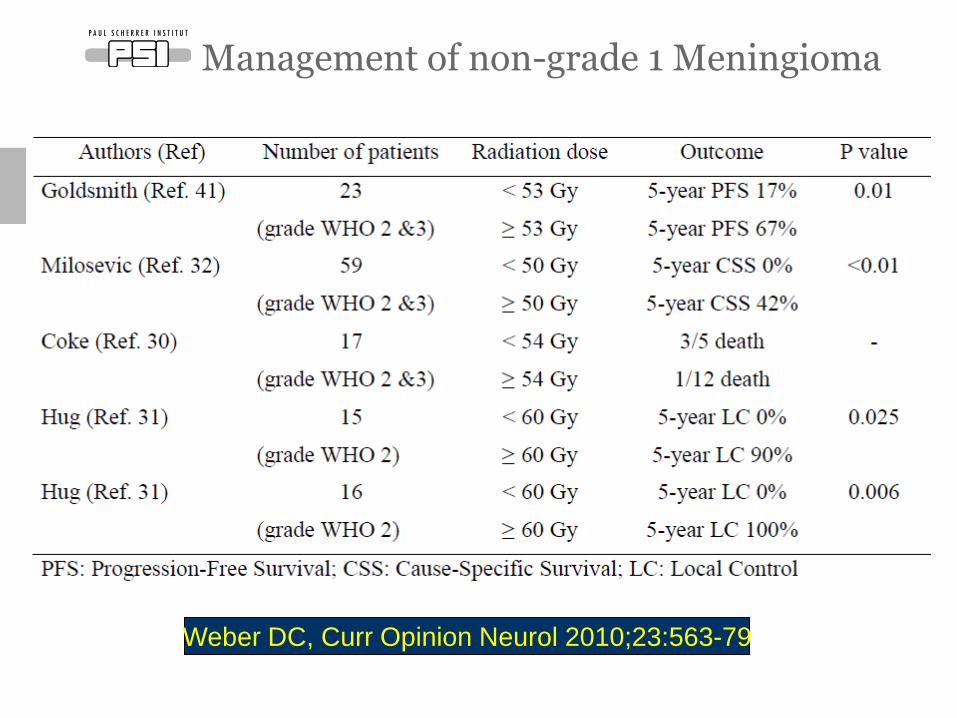
Management of non-grade 1 Meningioma
Weber DC, Curr Opinion Neurol 2010;23:563-79
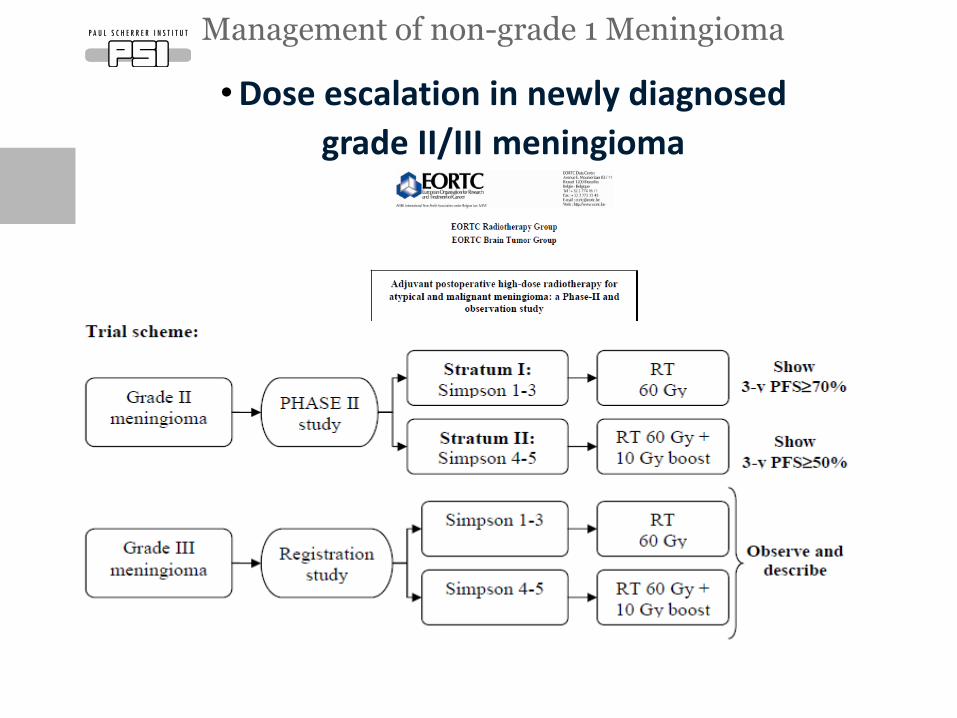
•Dose escalation in newly diagnosed
grade II/III meningioma
Management of non-grade 1 Meningioma
Management of non-grade 1 Meningioma
Management of non-grade 1 Meningioma
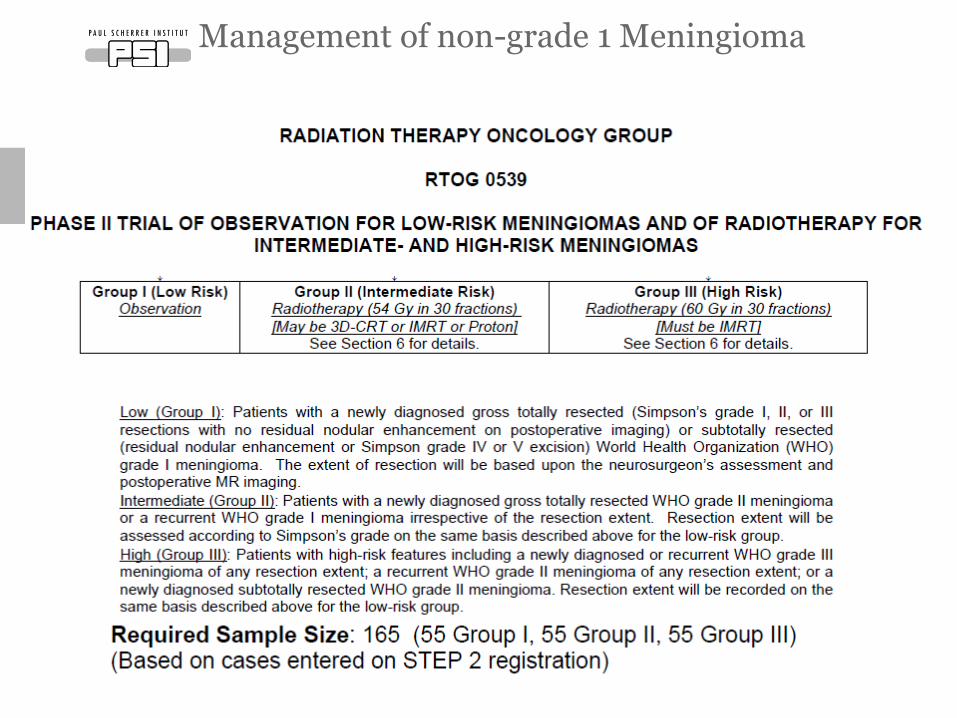
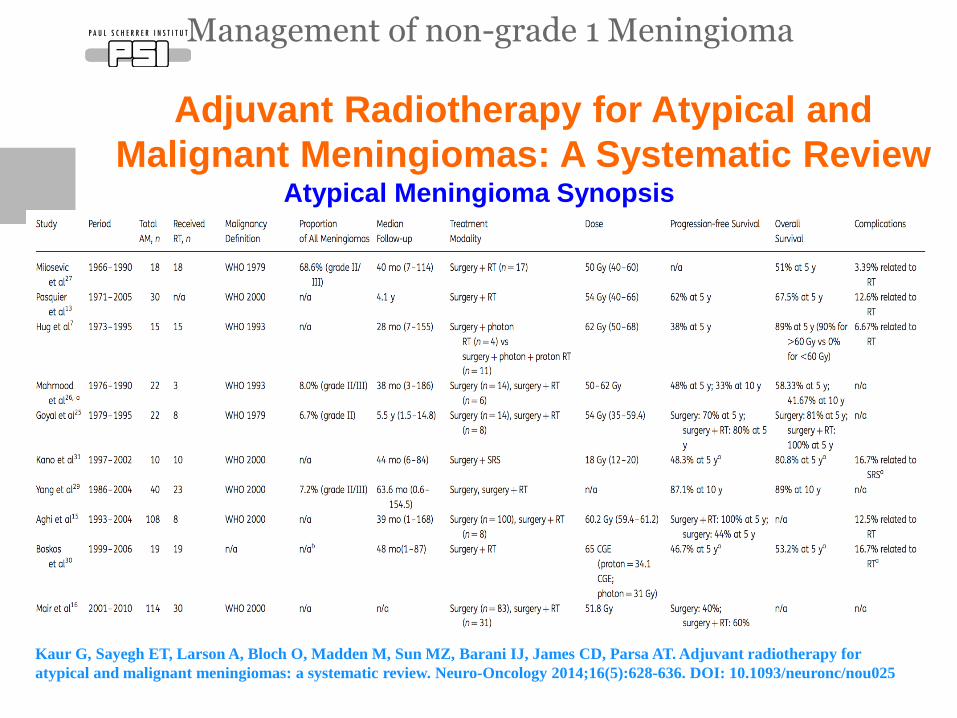
Adjuvant Radiotherapy for Atypical and
Malignant Meningiomas: A Systematic Review
Kaur G, Sayegh ET, Larson A, Bloch O, Madden M, Sun MZ, Barani IJ, James CD, Parsa AT. Adjuvant radiotherapy for
atypical and malignant meningiomas: a systematic review. Neuro-Oncology 2014;16(5):628-636. DOI: 10.1093/neuronc/nou025
Atypical Meningioma Synopsis
Management of non-grade 1 Meningioma
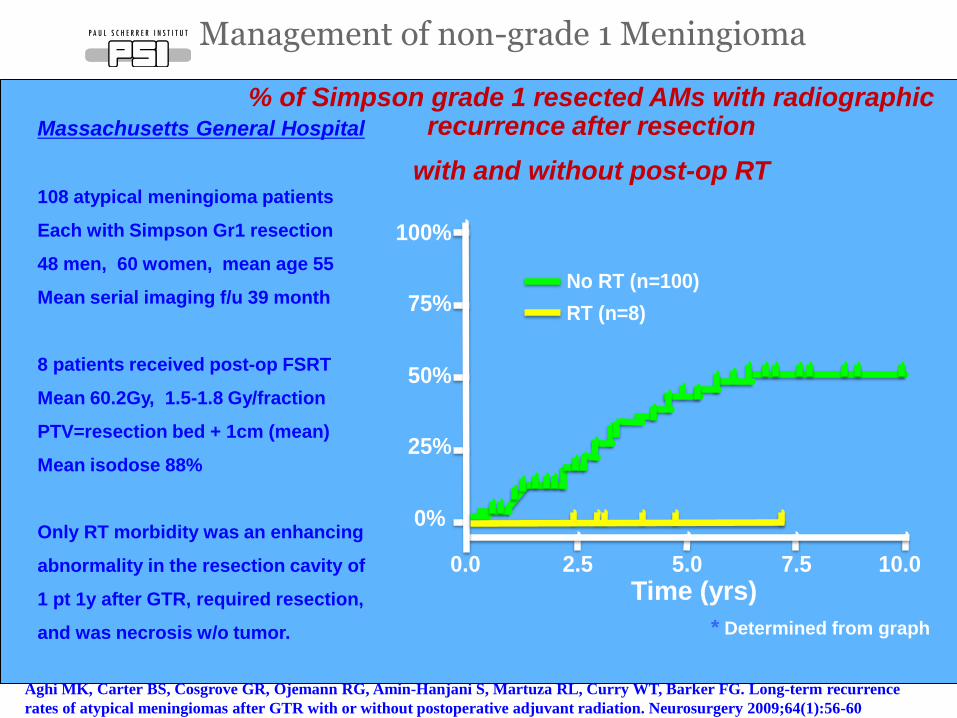
% of Simpson grade 1 resected AMs with radiographic recurrence after resection
with and without post-op RT
Aghi MK, Carter BS, Cosgrove GR, Ojemann RG, Amin-Hanjani S, Martuza RL, Curry WT, Barker FG. Long-term recurrence
rates of atypical meningiomas after GTR with or without postoperative adjuvant radiation. Neurosurgery 2009;64(1):56-60
Massachusetts General Hospital
108 atypical meningioma patients
Each with Simpson Gr1 resection
48 men, 60 women, mean age 55
Mean serial imaging f/u 39 month
8 patients received post-op FSRT
Mean 60.2Gy, 1.5-1.8 Gy/fraction
PTV=resection bed + 1cm (mean)
Mean isodose 88%
Only RT morbidity was an enhancing
abnormality in the resection cavity of
1 pt 1y after GTR, required resection,
and was necrosis w/o tumor.
Time (yrs)
! "#"$%&"
No RT (n=100)
RT (n=8)
100%
75%
50%
25%
0%
0.0 2.5 5.0 7.5 10.0
* Determined from graph
Management of non-grade 1 Meningioma
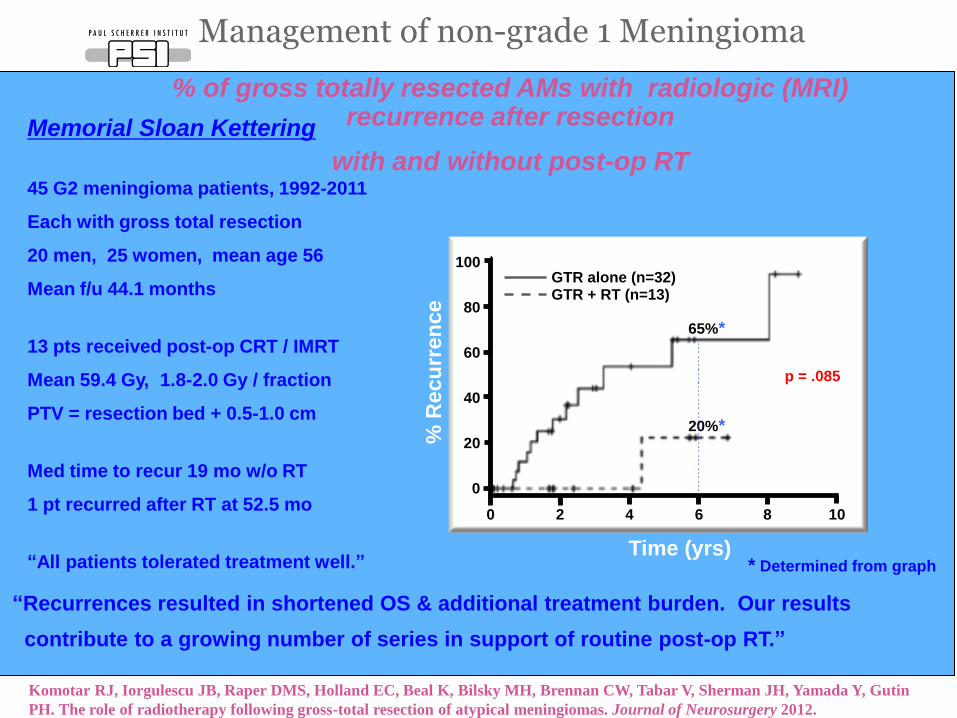
% of gross totally resected AMs with radiologic (MRI) recurrence after resection
with and without post-op RT
Komotar RJ, Iorgulescu JB, Raper DMS, Holland EC, Beal K, Bilsky MH, Brennan CW, Tabar V, Sherman JH, Yamada Y, Gutin
PH. The role of radiotherapy following gross-total resection of atypical meningiomas. Journal of Neurosurgery 2012.
* Determined from graph
Memorial Sloan Kettering
45 G2 meningioma patients, 1992-2011
Each with gross total resection
20 men, 25 women, mean age 56
Mean f/u 44.1 months
13 pts received post-op CRT / IMRT
Mean 59.4 Gy, 1.8-2.0 Gy / fraction
PTV = resection bed + 0.5-1.0 cm
Med time to recur 19 mo w/o RT
1 pt recurred after RT at 52.5 mo
“All patients tolerated treatment well.” Time (yrs)
% R
ecu
rren
ce
100
80
60
40
20
0
0 2 4 6 8 10
20%*
65%*
p = .085
GTR alone (n=32) GTR + RT (n=13)
“Recurrences resulted in shortened OS & additional treatment burden. Our results
contribute to a growing number of series in support of routine post-op RT.”
Management of non-grade 1 Meningioma
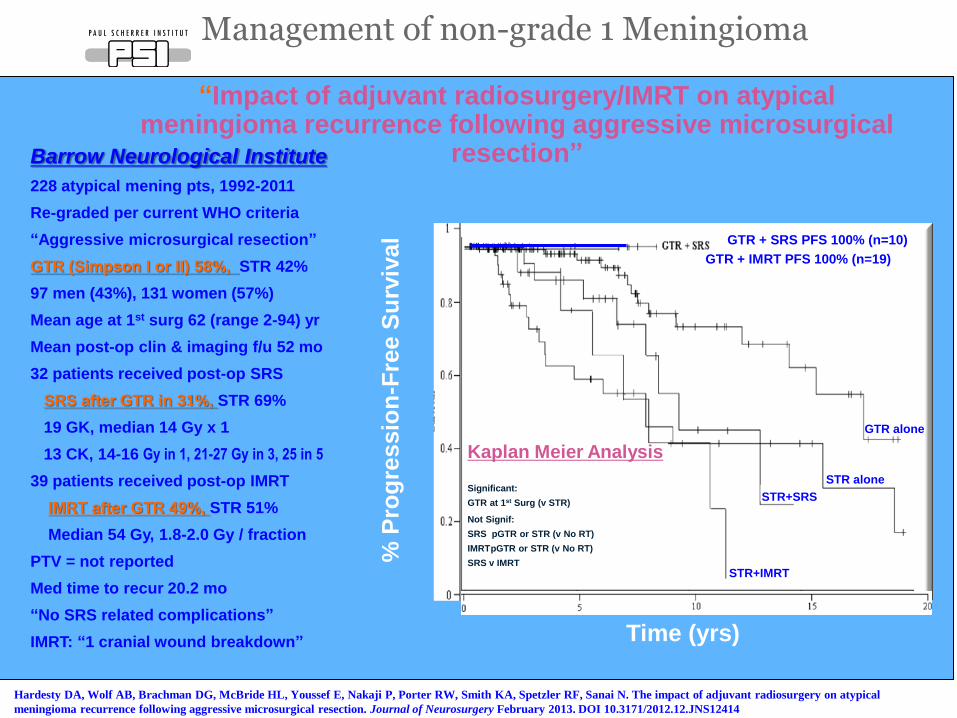
“Impact of adjuvant radiosurgery/IMRT on atypical meningioma recurrence following aggressive microsurgical
resection” Barrow Neurological Institute
228 atypical mening pts, 1992-2011
Re-graded per current WHO criteria
“Aggressive microsurgical resection”
GTR (Simpson I or II) 58%, STR 42%
97 men (43%), 131 women (57%)
Mean age at 1st surg 62 (range 2-94) yr
Mean post-op clin & imaging f/u 52 mo
32 patients received post-op SRS
SRS after GTR in 31%, STR 69%
19 GK, median 14 Gy x 1
13 CK, 14-16 Gy in 1, 21-27 Gy in 3, 25 in 5
39 patients received post-op IMRT
IMRT after GTR 49%, STR 51%
Median 54 Gy, 1.8-2.0 Gy / fraction
PTV = not reported
Med time to recur 20.2 mo
“No SRS related complications”
IMRT: “1 cranial wound breakdown”
Hardesty DA, Wolf AB, Brachman DG, McBride HL, Youssef E, Nakaji P, Porter RW, Smith KA, Spetzler RF, Sanai N. The impact of adjuvant radiosurgery on atypical
meningioma recurrence following aggressive microsurgical resection. Journal of Neurosurgery February 2013. DOI 10.3171/2012.12.JNS12414
Time (yrs)
STR+IMRT
STR+SRS
STR alone
GTR alone
Kaplan Meier Analysis
Significant:
GTR at 1st Surg (v STR)
Not Signif:
SRS pGTR or STR (v No RT)
IMRT pGTR or STR (v No RT)
SRS v IMRT
GTR + SRS PFS 100% (n=10)
GTR + IMRT PFS 100% (n=19)
% P
rog
ressio
n-F
ree S
urv
ival
Management of non-grade 1 Meningioma
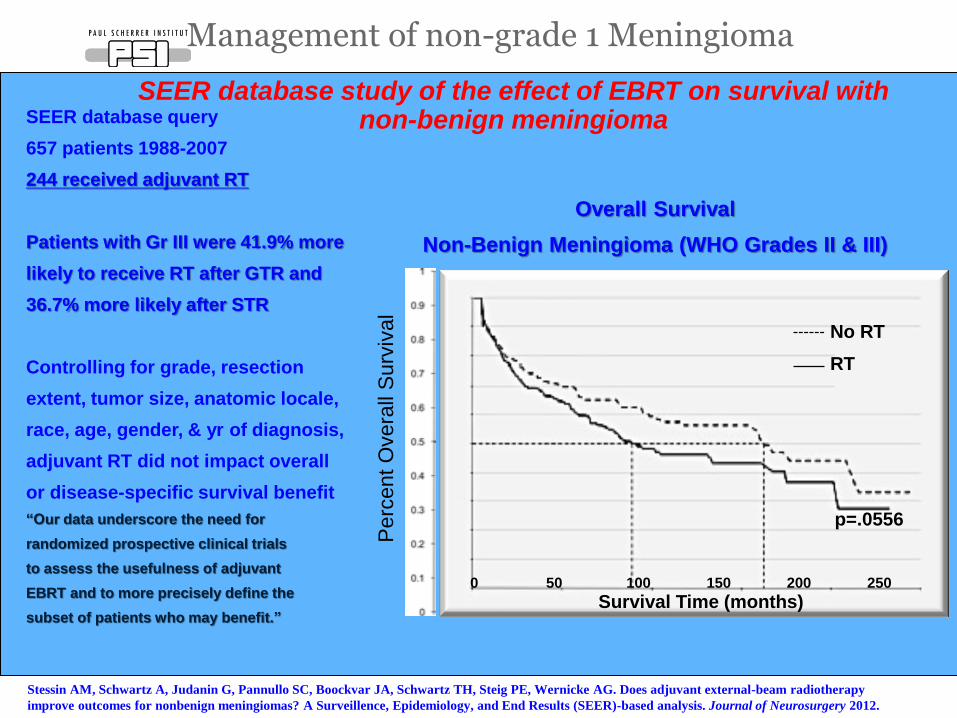
SEER database study of the effect of EBRT on survival with non-benign meningioma SEER database query
657 patients 1988-2007
244 received adjuvant RT
Patients with Gr III were 41.9% more
likely to receive RT after GTR and
36.7% more likely after STR
Controlling for grade, resection
extent, tumor size, anatomic locale,
race, age, gender, & yr of diagnosis,
adjuvant RT did not impact overall
or disease-specific survival benefit
“Our data underscore the need for
randomized prospective clinical trials
to assess the usefulness of adjuvant
EBRT and to more precisely define the
subset of patients who may benefit.”
Overall Survival
Non-Benign Meningioma (WHO Grades II & III)
Stessin AM, Schwartz A, Judanin G, Pannullo SC, Boockvar JA, Schwartz TH, Steig PE, Wernicke AG. Does adjuvant external-beam radiotherapy
improve outcomes for nonbenign meningiomas? A Surveillence, Epidemiology, and End Results (SEER)-based analysis. Journal of Neurosurgery 2012.
Survival Time (months)
Perc
ent
Overa
ll S
urv
ival
p=.0556
RT
No RT
0 50 100 150 200 250
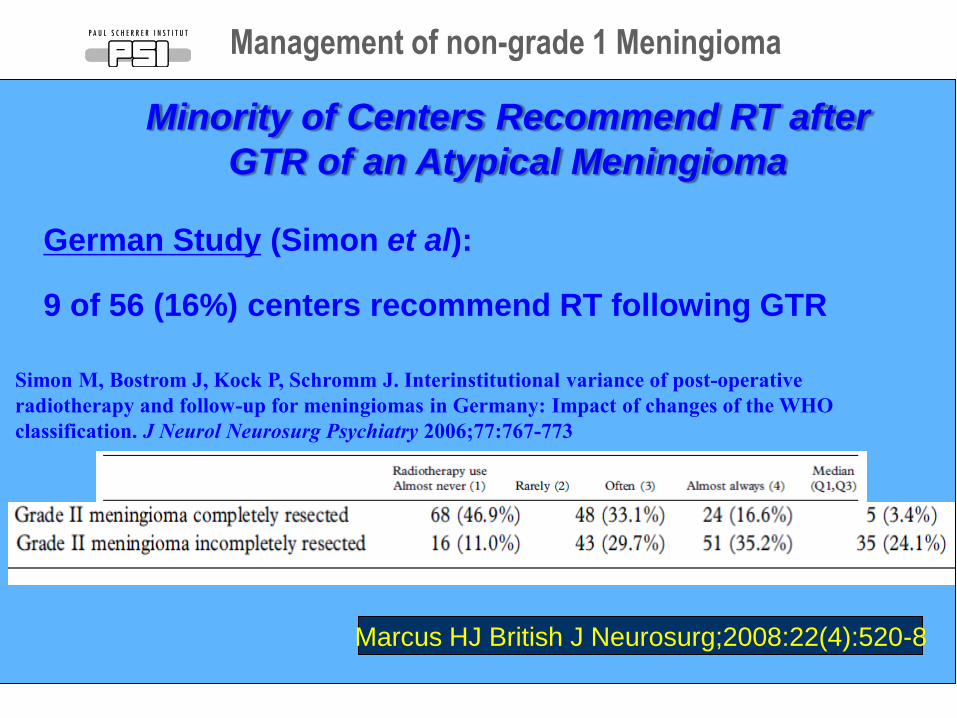
Minority of Centers Recommend RT after
GTR of an Atypical Meningioma
Simon M, Bostrom J, Kock P, Schromm J. Interinstitutional variance of post-operative
radiotherapy and follow-up for meningiomas in Germany: Impact of changes of the WHO
classification. J Neurol Neurosurg Psychiatry 2006;77:767-773
German Study (Simon et al):
9 of 56 (16%) centers recommend RT following GTR
Marcus HJ British J Neurosurg;2008:22(4):520-8
Management of non-grade 1 Meningioma
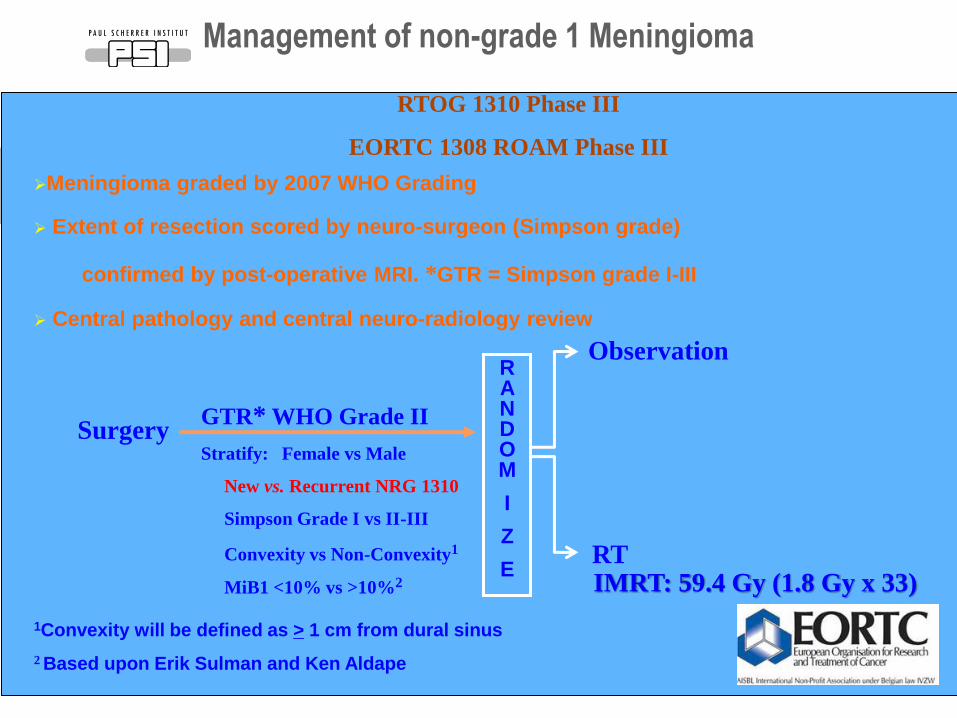
RTOG 1310 Phase III
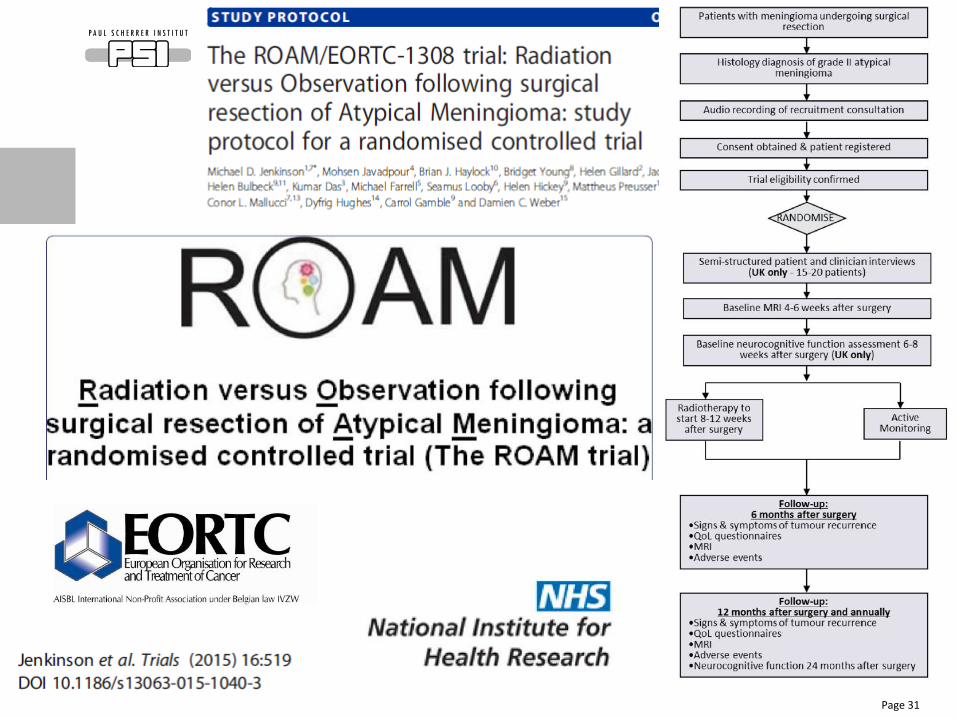
EORTC 1308 ROAM Phase III
Meningioma graded by 2007 WHO Grading
Extent of resection scored by neuro-surgeon (Simpson grade)
confirmed by post-operative MRI. *GTR = Simpson grade I-III
Central pathology and central neuro-radiology review
Surgery GTR* WHO Grade II
Stratify: Female vs Male
New vs. Recurrent NRG 1310
Simpson Grade I vs II-III
Convexity vs Non-Convexity1
MiB1 <10% vs >10%2
IMRT: 59.4 Gy (1.8 Gy x 33)
RANDOM
I
Z
E RT
Observation
1Convexity will be defined as > 1 cm from dural sinus
2 Based upon Erik Sulman and Ken Aldape
Management of non-grade 1 Meningioma
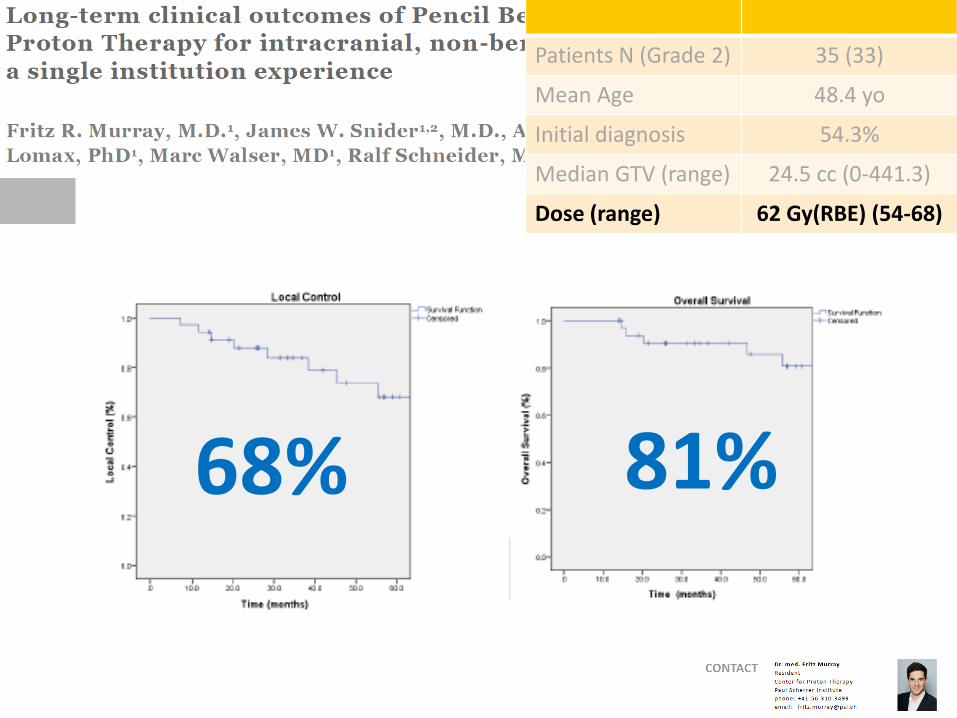
Patients N (Grade 2) 35 (33)
Mean Age 48.4 yo
Initial diagnosis 54.3%
Median GTV (range) 24.5 cc (0-441.3)
Dose (range) 62 Gy(RBE) (54-68)
68% 81%
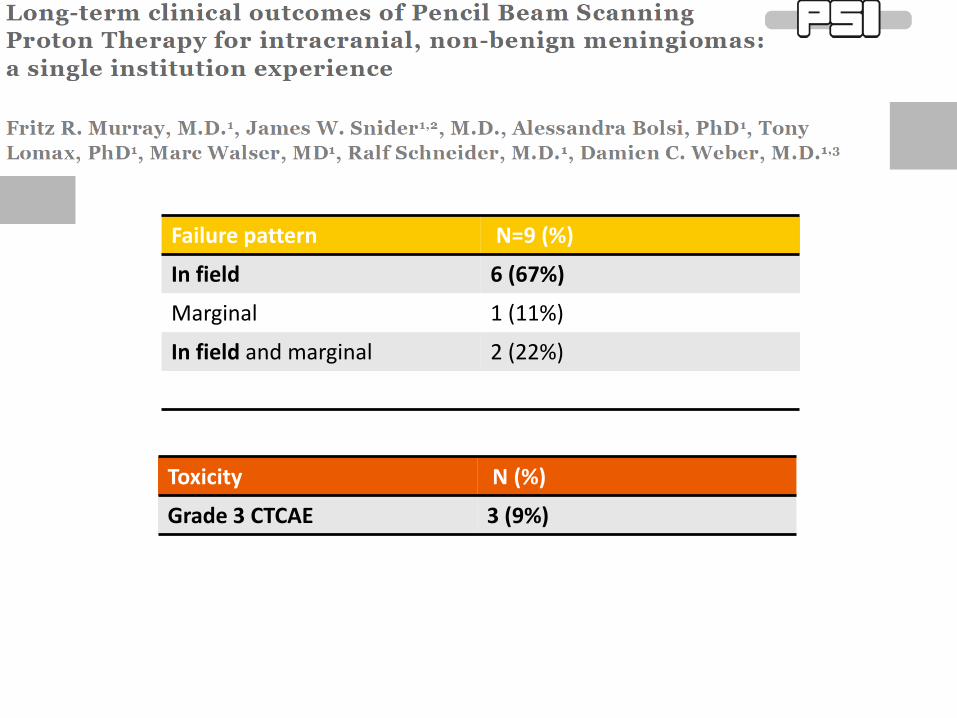
Failure pattern N=9 (%)
In field 6 (67%)
Marginal 1 (11%)
In field and marginal 2 (22%)
Toxicity N (%)
Grade 3 CTCAE 3 (9%)
Page 31
Conclusions
• Several retrospective studies have shown that RT after
STR is beneficial for patients with WHO 1 grade
meningioma
• Debate over the timing of RT-whether it should be
given postoperatively or at the time of progression
(WHO grade 1 meningioma )
• Modification of the WHO classification
• Suboptimal outcome of grade 2-3 meningioma
patients
Conclusions
•Dose-response of non-benign meningiomas
• FSRT, SRS, Protons, Carbons
• Failure pattern: IN FIELD
•Results of phase II (RTOG-EORTC) trials awaited for
Q2-3 2017
•On going phase III trial for Simpson 1-3 Grade 2
meningiomas









![protestas, derechos y violencias privatizaciones. Rol del ... · Godio, La Semana Trágica de enero de 1919, Buenos Aires, Hyspamérica, 1986 [Primera Edición de 1972]; Edgardo Bilsky,](https://img.pdfslide.tips/doc/110x75/5e1783a50219216ca06cecc6/protestas-derechos-y-violencias-privatizaciones-rol-del-godio-la-semana-trgica.jpg)