-
8/3/2019 perio microbioloy
1/22
PERIODONTAL MICROBIOLOGY:
Bacterial plaque is the primary cause of gingivitis and the
various forms of periodontitis.Although oral microbiota comprise of
over 300species, only about 30 of these are considered to be
periodontopathic.
Periodontal health results from a host-parasite equilibrium that
is characterized by minimal tissue
destruction and maximum repair of damaged structures.Alteration
of this equilibrium may result as a result of local or systemic
changes that decreases hostresistance or from quantitative and/or
qualitative alteration of the periodontal microbiota, especially
a
increase in virulence.
CRITERIA FOR PERIODONTOPATHOGENECITY OF A MICROORGANISM:
Socranskys theories of possible modes of progression of chronic
destructive periodontal disease:
a- Progressive loss of attachment some sites show progressive
loss of attachment over time
whereas other sites show no destruction. The time of onset and
extent of destruction vary from
site to site.
b- Random burst model activity occurs at random at any site.
Some sites show no activity,whereas other sites show one or several
bursts of activity. The cumulative effect of destruction
may vary from site to site.
c- Asynchronous multiple burst model several sites show bursts
of activity over a finite period
followed by prolonged periods of inactivity. Majority of disease
activity takes place within a
few years.
Kochs postulates (1870) = classic basis to establish a specific
micro-organism may be defined as the
causative agent for a human diseasei- always associatedwith the
disease
ii- be routinely isolatedfrom the diseased individual
iii- be able to be grown in vitro cultures
iv- produce a similar disease when inoculated in animal
studies
v- be recovered from lesions in diseased lab animals
vi- show specific immunologic changes in the human
Nature of periodontal diseases present difficulties in studying
the periodontal microbiota and an
inability to apply the Kochs postulates.
i. The chronic nature of periodontal disease shows an episodic
nature with alternating periods ofexacerbation and remission.
Therefore any microbial analysis must take into account the stage
of
disease activity at that location.
ii. The host resistance may be variable and difficult to
measure.
iii. Results noted in animal models may not be directly
transferable to a human model
iv. To access the changes of microbiota to treatment, it is
difficult to define the criteria for success
v. Difficulties in sampling, dispersion and cultivation of the
resident micro-organisms, becausebacteria from a diseased site may
be pooled with that of healthy site. Samples usually contained
more material from supra-gingival plaque.
-
8/3/2019 perio microbioloy
2/22
vi. Lack of a well developed technique for maintaining a
continuous anaerobic environment during
sampling harvesting and culture.
vii. Inadequate and ever evolving taxonomy.
Socransky suggested an alternative to Kochs postulates to label
periodontal micro-organisms as
possible periodontopathogens.
1. the number of etiologic organisms in the pathologic sites
must be increased and conversely the
number of organisms must be reduced or absent in healthy site or
sites with other forms of disease2. if the etiologic organism is
eliminated or suppressed, the disease should stop. If it doesnt
stopeither the wrong organism was eliminated or organisms that
remain in the site are sufficient by
themselves to enable destruction to continue.
3. an increase or decrease in cellular and/or humoral immune
response to a given species in a
specific form of periodontal disease suggests a role for that
organism in the disease process.
4. the micro-organism should be attempted to be isolated in pure
culture and replication of anim
pathogenicity should be shown5. bacterial virulence factors
responsible for enabling the micro-organism to cause destruction
o
the periodontal tissues must be demonstrated.
DENTAL PLAQUE:
Definition: Dental Plaque is a specific host associated biofilm
on tooth surface, restorations,orthodontic appliances and
prosthesis that consists primarily of proliferating
micro-organisms,
along with a scattering of epithelial cells, leukocytes, and
macrophages in an adherent intercellular
matrix.
It is different from other tooth associated aggregations like
pellicle, food debris, material alba and
calculus based upon its specificity, location, bacterial content
and matrix.
Materia alba is the tooth associated biofilm consisting of
bacterial aggregations, leukocytes anddesquamated oral epithelial
cells accumulating at the surface of the teeth, but lacking the
internal
structure observed in dental plaque.
Dental plaque lacks mineralization like calculus.
Classification: based upon its relation to gingival margin
- supragingival plaque
coronal plaque that plaque in contact with only the tooth
surface
marginal plaque associated with tooth surface at the gingival
margin
- sub gingival plaque
Supragingival Plaque
Visibility: It can be detected clinically only when it reaches a
certain thickness. Small amounts are not
visible and can only be detected by using plaque disclosing
agents.
Colour: When it accumulates becomes a visible globular mass with
a nodular surface having a gray
to yellowish gray to yellow colour.Site: regularly at gingival
third, especially surface cracks, pits, fissures of occlusal
surfaces,
overhanging margins.
-
8/3/2019 perio microbioloy
3/22
That is sites protected from the normal mechanical cleansing
action of the tongue, the cheeks, and
the lips.
Other sites include restorations, artificial crowns, orthodontic
bands, dental implants, orthodonticappliances and prosthesis.
Quantity: measurable amounts within 1hour after the teeth are
thoroughly cleaned and maximum in
about 30days or less.
Rate of formation: varies among individuals, on different teeth
in same mouth, and different areas of
same toothInfluenced by - diet
- age
- salivary factors
- oral hygiene
- tooth alignment
- systemic disease
- host factors- mechanical retention factors
Composition: 70-80% = 200-400 different species bacteria in a
complex arrangement
1 cubic mm of dental plaque with weight 1mg has about 108
bacteria
Other micro-organisms are mycoplasma, yeasts, protozoa, virus in
different proportions
Non bacterial portion is interbacterial matrix = 20-30% plaque
volume.Organic portion polysaccharide protein complex
Extra cellular products of plaque bacteria,
Cytoplasmic and cell membrane remnants
Food debris
Derivatives of salivary glycoproteins
30% carbohydrate9.5% of total plaque = dextran (bacteria
produced polysaccharide)
Levan, galactose, rhamnose, and sometimes mutan30% protein
15% lipid
Remainder = note determined
Inorganic component very small quantity, and nil in early
plaqueGreatest quantity when plaque is being transformed into
calculus
Calcium and phosphorus are main
Small amounts of Magnesium, potassium and sodium
Fluoride when there is topical application
Formation and biochemistry:
First layer that is formed on tooth is called PELLICLEThis is
the organic structure formed prior to bacterial colonization
Significant difference in pellicle formed on natural teeth and
that on artificial surfaces
Therefore composition may vary as per the host site
Stage I adsorption of salivary proteins to apatite surfaces
By electrostatic ion interaction of calcium ions and phosphate
groups in the enamel
surface and oppositely charged groups in the salivary
molecules.Composed of glycoproteins
Immunoglobulins
Different carbohydrates
-
8/3/2019 perio microbioloy
4/22
Stage II transition from dental pellicle to dental plaque
Colonization of pellicle by bacteriaFirst colonizers cocci
Epithelial cells (few)
Polymorphonuclear leukocytes
Forms a monolayer of cells, either singly or in groups
Bacterial growth spreads laterallyCoalescing with neighboring
patchesGiving rise to different micro colonies in a complex
pattern
Bacterial adherence:
First bacteria must adhere too the pellicle surface
Become sufficiently attached to withstand the oral cleansing
forces
Second they must grow and adhere to each other
Electrostatic forces: negatively charged components of the
bacterial cell surface
and negatively charged surface glycoproteins in pellicle become
linked via
calcium cations
Hydrophobic interactions: based on close structural fit between
molecules
Organic solutes: salivary glycoproteins have specific receptors
called adhesions
which promote chemical bonding between some bacteria and
pellicle and inhibitother bacteria.
Bacterial Growth and Proliferation: leads to bacterial
accumulation
leads to increase in plaque mass
characterized by multiplication and cohesion of bacterial
cells
increase in bacterial byproducts and thus changes in
intercellular matrix
depends uponbacterial factors:
-bacteria like S. mutans produce extracellular glucans which are
sticky and causeentrapment of other bacteria.
- Some bacteria produce compounds that are essential nutrients
and growth
factors for other microorganisms.
- Some species produce bacteriocin which is inhibitory for
adhesion of othertypes
- The prevailing bacteria will utilize all available nutrients
and not leave any for
survival of other similar species
Environmental factors:
Low pH: fermentation of carbohydrate causes low pH, thus only
those bacteria
able to survive in this environment will predominate. (caries)O2
tension: streptococcus and lactobacillus consume the available
oxygen. As
their umber increases the oxygen tension decreases resulting in
a shift towards
obligatory anaerobes. Similarly changes in temperature can take
place facilitatin
or inhibiting future bacterial growth.
Salivary nutrients which are present in the pellicle and the
surrounding saliva
will determine the changes in bacterial pattern.Host
factors:
Oral cleansing mechanism, like salivary flow, mastication and
movement of
tongue and cheek.
-
8/3/2019 perio microbioloy
5/22
Saliva contains bacterial inhibitory substances like
lactoperoxidase, lactoferrin,
and lysozyme which prevent accumulation of sensitive
bacteria.
Host response factors like antibodies, leukocytes and complement
in the GCF dnot allow bacterial adhesion and proliferation.
Clinical Significance: if the supragingival plaque is not
allowed to mature, then one can expect health
in gingival tissues
in case the plaque is allowed to mature, it results in
gingivitis and the subsequent formation o
subgingival plaque.
So in early periodontitis, the supragingival plaque strongly
influences the growth,
accumulation and pathologic potential of subgingival plaque
Once the pocket has formed and disease has progressed, the
influence of supragingival plaqu
on activity of subgingival plaque is limited to the most
coronally situated part only
SUB-GINGIVAL PLAQUE:
Definition: that dental plaque which is present in the gingival
sulcus or periodontal pocket
Structural Characteristics:Stagnant environment, less subject to
natural cleansing activities of the mouth
Thus even those micro organisms which do not readily attach to
hard surfaces are allowed to
colonize and proliferate.
These can adhere to the tooth surface or to pocket
epithelium.
More nutrient supply: those in relation to pocket epithelium
have more direct access to nutrients
especially the proteins of sulcular fluid
Lower oxidation-reduction potential: environment has lower
oxidation-reduction potential, thus
allowing anaerobic bacteria to establish more easily
-
8/3/2019 perio microbioloy
6/22
Bacterial invasion of connective tissue: bacteria from
epithelium associated plaque may penetrat
and colonize the gingival connective tissue, and may also
inhabit the alveolar crest as the
periodontitis
Types:
1. Tooth Associated(attached) Sub-Gingival Plaque
2. Epithelium Associated Sub-Gingival Plaque
3. Unattached Sub-Gingival Plaque
Tooth Attached Sub-Gingival Plaque:
Gram +ve bacteria predominate, densely packed and at right
angles to the root surface,
structure similar to supra-gingival plaque with granular like
surface
Rods and cocci like Streptococcus mitis, S sanguis, Eubacterium,
Bifido-bacterium,
Actinomyces viscosus, A naeslundi, Propionibacterium.
Few gram negative cocci and rods, especially in the more apical
portions.Does not extend to junctional epithelium, between the
junctional epithelium and apical
border of plaque there is accumulation of leukocytes.
May penetrate cementum
Associated with mineral deposition and calculus formation
besides root caries and root
resorption
Epithelium Associated Sub-Gingival Plaque:
Gram variable, gram negative rods and cocci, flagellated
bacteria and spirochetes, no
specific pattern.Bacteriodes, Fusobacterium, Capnocytophaga,
Selenomonas, Campylobacter,
Actinobacillus
Loosely adherent in direct association with epithelial wall of
pocket from gingival margin
extending upto junctional epithelium
May penetrate epithelium and connective tissue
Associated with gingivitis and periodontitis
Unattached Sub-Gingival Plaque:
-
8/3/2019 perio microbioloy
7/22
Gram variable
Extends upto junctional epithelium
Associated with gingivitis
Characteristics of Sub-Gingival plaque
Attached to Tooth Unattached Attached to Epithelium
Gram positive bacteria
predominate
Gram Variable Gram variable
Bacteria organized perpendicular
to tooth surface
Not organized Not organized
Does not extend upto junctional
epithelium
Extends upto junctional
epithelium
Extends upto junctional
epithelium
May penetrate cementum - May penetrate epithelium and
connective tissue
Associated with calculus
formation and root caries
Associated with gingivitis Associated with gingivitis and
periodontitis
Bacterial Invasion of Periodontium:There is evidence of
bacterial invasion into gingival in gingivitis and ANUG
Through lateral wall of periodontal pockets
Through the junctional epithelium in advanced periodontitis and
LJP
Penetration through ruptured intercellular spaces of stratum
spinosum. Basal lamina is sort
the barrier for such penetration. Such penetration through basal
lamina is through
perforations or interruptions in it or through ulcerations in
pocket wall or through
microholes through which leukocytes migrate across
Gram negative and positive cocci, rods, filaments and
spirochetes have been found in
connective tissue and also in contact with crest of alveolar
bone in advanced disease.
Advancing Front: plaque adjacent to the sulcular and junctional
epithelia is the advancing
front of periodontitis disease. Active lesions in rapidly
progressive diseases contain gram
negative motile organisms
bursts of activity might be the result of periods of active
bacterial penetration and
subsequent tissue destruction.
Calculus has only an indirect role in periodontal disease. It
has on its surface the plaque an
allows it to be more in contact wit pocket walls. Causes
irritation and physical trauma to
thin inflamed pocket epithelium. Allows easier entry of plaque
bacteria
Pocket wall is constantly changing as per the disease activity.
There are microscopic areas
of (1)heavy bacterial accumulation, (2)host response,
(3)emergence of leukocytes,
(4)leukocyte-bacterial interaction, (5)evidence of tissue
destruction like hemorrhage &
ulceration (6)epithelial desquamationClinical implication: in
localized juvenile periodontitis mechanical periodontal therapy
do
not eliminate Actinobacillus actinomycetemcomitans from the
tissues, and therefore
systemic antibiotics along with surgical therapy is needed to
eliminate the bacteria
Concept of Microbial Specificity:
Before composition of plaque was thought to be similar from
patient to patient and from sit
to site.
-
8/3/2019 perio microbioloy
8/22
But in some cases a lot of plaque caused little destruction as
in case of chronic periodontitis
while in cases like localized juvenile periodontitis and
pre-pubertal periodontitis little
detectable plaque was present with dramatic loss of
periodontium.Loesche 1976 Specific plaque hypothesis
Specific forms of periodontal diseases have specific bacterial
causesThe concept of bacterial specificity suggests that
periodontal disease may be a group of diseases
with different causes and clinical courses but with similar
symptoms
Technical difficulties in studying Sub-Gingival flora:
1. Sampling: curette or scalar
Paper point
2. Dispersion: adherent micro organisms have to separated from
each other without losing
their viability
3. Cultivation: need different selective and non selective media
for growth of different
micro flora, especially the facultative and obligatory anaerobes
andmicroaerophillic
4. Identification of Microorganisms: need identification and
characterization of different
bacteria
5. Statistical Analysis: complex and voluminous data need
accurate analysis
Mechanism of Bacterial Mediated Destruction:
Health= Host-parasite equilibrium in favor of host
For disease to happen
Need bacterial colonization & proliferation
Need bacteria to maintain themselves
Need bacterial penetration and invasion into connective
tissue
Need toxicity effects of bacteria to occur through toxins,
enzymes, or metabolic produc
-
8/3/2019 perio microbioloy
9/22
Need to spread the organisms orproducts in the connective
tissue
Need bacteria to suppress/evade host immunity by inhibiting PMN
chemotaxis
Phagocytosis/bactericidal activit
interbacterial activity may give rise to favorable or inhibitory
bacterial succession
Direct Toxicity:
Toxins:Exotoxins: Released by bacteria in surrounding
environment
Protein type
Cause direct tissue injury
Epitheliotoxins
Leukotoxins
Endotoxins: structural components of Gm ve bacteria release
after bacterial lys
Lipo-polysaccharidesAmplify inflammatory process
Can produce localized leucopenia
Can activate Factor XII, causing intra vascular coagulation
Can activate complement system by alternative pathway
Can cause localized Shwartzman phenomenon and necrosis
Cytotoxic to fibroblastsMaybe induce bone resorption
Cell Constituents: bacterial surface components & capsular
components
peptidoglycan
Activates host tissue response like complement
Immunosuppression
Stimulates Reticulo Endothelial SystemIndirectly stimulates
collagenase production from macrophages
Causes tissue destruction and bone resorptionAllows bacteria to
evade host protective system
Enzymes: facilitate tissue penetration by bacteria
Proteases: collagenase, hyaluronidase, chondroitin
sulfataseOthers like Alkaline & acid phosphatase,
phospholipase, aminopeptidases
End products of bacterial metabolism: contribute to inflammatory
process
Volatile sulfur compounds, ammonia, indole, fatty acids,
polyamines
Indirect Toxicity:
Local immune reaction triggered by bacteria or their products
cause tissue destruction
Bacterial Factors In Evasion of Host Defenses:
Inhibition of PMN: Leukotoxin
Chemotaxis inhibitors
Decreased Phagocytosis and intracellular killing
Resistance to C-mediated killingLymphocyte alterations
Endotoxicity
IgA, IgG proteases
-
8/3/2019 perio microbioloy
10/22
Fibrinolysin
Superoxide dismutase
Catalase
Microbiological Flora in Health and Disease:
Oral Flora in normal mouths:Microorganisms from water, food,
air, etc gain ready accessIdeal temperature and pH and oxygen
tension
Abundant supply of nutrients
Oral cavity is sterile at birth
Simple facultative flora within 6-10 hours
Anaerobes within first 10 days to 5months and definitely when
incisors appearBesides bacteria there are Fungi like Candida,
Cryptococcus, Saccharomyces
Protozoa like Entamoeba gingivalis, Trichonomas tenax
Viruses
Mycoplasma
Only bacteria that are able to attach and resist detachment are
retained and colonize.Bacteria preferentially colonize specific
anatomic locations based on their adherence
characteristics, complex growth requirements. As the
micro-environmental conditions change
in favor of another species, the original species must either
adapt to new conditions of be
superseded by the next species which is better suited to
colonize and proliferate in the newer
conditions bacterial succession
Periodontal health = Gm +ve cocci and rods
Supragingival plaque initiated by Streptococcus sanguis &
other Gm +ve cocciActinomyces viscosus another one of important
initial colonizer
Secondary growth and proliferation
Bacterial succession or bacterial population shift occurs
(Streptococcus mitis, Staphylococcus epidermidis, Rothia
dentocariosa, A naeslundi and fewspecies of Neisseria &
Veilonella)
Very few Gm ve organisms like Capnocytophaga, Prevotella
loeschii, Campylobacter,
Fusobacterium and spirochetes like Treponema denticola
In healthy periodontium the non pathologic organisms predominate
and dont allow the
periodontopathogens to colonize, protective species(S sanguis, S
uberis, Veilonella parvula, R dentocariosa, Capnocytophaga
ochracea,
Propionobacterium acnes)
Gingivitis:
Increase in supragingival plaque
Change from gram +ve (mainly cocci) to a more complex flora
including substantial Gm veand spiral motile forms in a sequential
form of succession.
Gm +ve bacteria like Streptococcus sanguis, S mitis, S
intermedius, S oralis, Actinomyces
viscosus, A naeslundi, Peptococcus micros.
-
8/3/2019 perio microbioloy
11/22
Gm ve bacteria like Fusobacterium nucleatum, Prevotella
intermedia, Veilonella parvula, &
few Hemophillus, Capnocytophaga, Campylobacter species and few
Treponema denticola
Initially edematous changes in marginal gingivalAdvanced stages
may have bacterial penetration in gingival epithelium and
connective tissue.
Pregnancy Gingivitis:
Prevotella intermedia
Porphyromonas gingivalisCapnocytophagaIncrease in hormones like
estrogen and progesterone which act like nutrient source for
these
bacteria
ANUG:
pathophysiology of disease as being caused by a fusospirochetal
complex that requires
underlying tissue changes to facilitate the pathogenic activity
of the bacteria.Treponema microdentium,
Borrelia vincenti, intermediate size spirochetes, vibrios,
fusiform bacilli,
Prevotella intermedia
Actinomyces odontolyticus
Selenomas species
Chronic Periodontitis:
Increase in loss of attachment
High percentage of anaerobic (90%) species
Gm ve are more preponderant in plaque = 75%
Porphyromonas gingivalis, (elevated in active sites, associated
with disease progression
Prevotella intermedia, (elevated in active sites, associated
with disease progression)Bacteroides forsythus, (elevated in active
sites, associated with disease progression)
Campylobacter rectus, (elevated in active sites, associated with
disease progression)Actinobacillus actinomycetemcomitans,
(associated with disease progression)
Eikenella corrodens,
Fusobacterium nucleatum, (elevated in active sites)
Peptococcus micros,Treponema denticola and other species
Eubacterium species
Bacteria noted in connective tissue: P gingivalis, A
actinomycetemcomitans.
Rapidly Progressive Periodontitis:
Young adults 20-35years of ageGeneralized, severe and rapid bone
loss
Small amounts of plaque
Porphyromonas gingivalis, Prevotella intermedia, Bacteroides
capillus
Actinobacillus actinomycetemcomitans, Eikenella corrodens,
Wolinella recta
Localized Aggressive Periodontitis:
Rapid and severe loss of attachment in individuals during or
after puberty
Complicated by some diminished host response functionPrePubertal
Periodontitis:
-
8/3/2019 perio microbioloy
12/22
Rare form
Immediately after eruption of primary teeth
Patients have severe defects in neutrophils and
macrophagesActinobacillus actinomycetemcomitans is predominant
Capnocytophaga sputigena, Prevotella intermedia, Eikenella
corrodensLocalized Juvenile Periodontitis:
Adolescents
Rapid destruction of periodontium around incisors and molars
(arc shaped)90% bacteria in Localized Juvenile Periodontitis is A
actinomycetemcomitansOther: P gingivalis, E corrodens, C rectus, F
nucleatum, Bacteroides capillus,
Eubacterium brachy, Capnocytophaga species, and spirochetes
A actinomycetemcomitans produces a neutrophil inhibiting toxin =
leukotoxin
Refractory periodontitis:
Does not respond to conventional treatmentPorphyromonas
gingivalis
A. actinomycetemcomitans, Peptococcus micros, Wolinella recta,
Bacteroides forsythus,
Prevotella intermedia, Eikenella corrodens
Periodontal Abscess
Acute lesionWith or without concomitant periodontitis
Fusobacterium nucleatum, Prevotella intermedia, Porphyromonas
gingivalis,
Peptococcus micros, Bacteroides forsythus
Immunology of Periodontal Disease:
Bacteria and Host Defense interactionMay be beneficial by
protecting against the spread and effects of bacteria
May be detrimental by contributing to tissue damage
Host defense variables try to influence bacteria at every
step
- bacterial colonization
- bacterial invasion- tissue destruction
- healing and repairBacterial colonization:
IgG and complement present in GCF to fight against subgingival
plaque bacteria
Inhibits adherence and co-aggregation
Maybe reduce number by lysisExplosion of bacteria increases
antigen load
immune system may get overwhelmedBacterial Invasion:
Only few bacteria traverse across epithelium into connective
tissue
Tissue are having plenty of antibodies and complement
Chemotaxis of PMN and monocyte infiltrationLeading to
phagocytosis and lysis of bacteria
Patients having defects of neutrophil and macrophage function
and chemotaxis have diseaseTissue Destruction:
-
8/3/2019 perio microbioloy
13/22
Antibody mediated hypersensitivity type release of histamine
Cytotoxic reactions by IgG and IgM and complement
Immune microcomplex reactions by IgG & IgM activates
complement leading to hormonal,vascular and cytotoxic events and
lysozyme release
Cell mediated reactions by sensitized T lymphocytes resulting in
release of lymphokines,
interleukins (IL-1) and osteoclast activating factor,
Activation of tissue factors like collagenase
Healing and fibroblasts:Lymphocyte and macrophage produced
chemotactic factors for fibroblastsRelease of lymphokines like
fibroblast activating factors
Some Bacteriodes produce proteases which inactivate antibodies,
or stimulate OAF production
or activate T suppressor cells
Immunologic Changes in health and periodontal disease:
Health: presence of chronic inflammatory cells and low titres of
antibodies
Chronic disease: increase in Gm ve, filamentous and
spirochetes
Increase in B cells, Mast cells, Complement, Inflammatory cells,
Prostaglandins,
Enzymatic action, and tissue destruction
Increase antibodies to P gingivalis and other
periodontopathogens
Increase in immune complexes in tissuesImmediate
hypersensitivity to gingival bacteria
Cell mediated immunity to gingival bacteria
ANUG: PMN chemotactic defect
Increase antibodies to Prevotella intermedia and intermediate
spirochetes
Localized Juvenile Periodontitis: PMN chemotactic defect
Decrease in ability for PhagocytosisPMN cellular abnormality
Increase immunoglobulins to A actinomycetemcomitans serotype B
and little serotypeA
Increase in leukotoxin production by the bacteria
Generalized Juvenile Periodontitis: PMN chemotactic defect
Decreased phagocytosis but normal migration
Increase IgG to Porphyromonas gingivalis, with increase in
protease activity
Increase antibodies to A actinomycetemcomitans serotype C
PrePubertal Periodontitis: increased WBC countDecreased PMN and
monocyte chemotaxis
Decreased adherence
Increased functional defects
Periodontitis in Juvenile Diabetes:Neutrophil chemotactic
defect.
Rapidly Progressive Periodontitis: suppressed or enhanced PMN or
monocyte chemotaxis
Increased antibody levels to several Gm ve bacteria
-
8/3/2019 perio microbioloy
14/22
Refractory periodontitis: decreased PMN chemotaxis
Periodontal Abscess: same as adult periodontitis
Desquamative Gingivitis: diagnostic or
characteristicimmunopathologic changes
Autoimmune etiopathogenesis in pemphigus and pemphigoid
cases
AIDS and ANUP: altered T4: T8 ratio
Neutrophil Related Periodontal Disease:
Periodontal Disease with Neutrophil Disorder:
1. ANUG
2. Localized Juvenile Periodontitis
3. PrePubertal Periodontitis4. Rapidly Progressive
Periodontitis
5. Refractory Periodontitis
Neutrophil disorders associated with Periodontal Disease
Primary:
1. Cyclic Neutropenia2. Chediak Higashi syndrome
3. Leukocyte Adhesion Deficiency (LAD-1)
4. Agranulocytosis or Chronic Granulamatous Disease (CGD)
Secondary:
1. Diabetes Mellitus
2. Papillon Lefevre Syndrome3. Down syndrome
4. AIDS5. Pre Leukemic syndrome
6. Acute Myeloid Leukemia
7. HyperImmunoglobenemia E (Jobs syndrome)
Future Advances in Study of Periodontal Microbiology:
Plaque Assays:
ii) phase and darkfield microscopy
iii) culture and isolation
iv) identification of bacterial enzymes and products
v) immunofluorescencevi) latex agglutination
vii) ELISA
viii) immunoblotting
ix) DNA probes :DNA based methodology to identify and detect
specific bacteria and
viruses
- no need for cultivation- more samples can be examined
- more amount of data
- detect even those organisms that are sensitive to dispersion,
sampling, culture.
-
8/3/2019 perio microbioloy
15/22
Indirect Assays on Sera:
i) Immunofluorescence
ii) ELISA
Corn-cob formation: rods like Bacterionema matruchotii &
Fusobacterium nucleatum
Cocci like streptococci and Porphyromonas gingivalis
Interbacterial interaction
Fimbriae
Coaggregation
Van der Wahls forces
-
8/3/2019 perio microbioloy
16/22
-
8/3/2019 perio microbioloy
17/22
-
8/3/2019 perio microbioloy
18/22
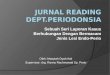
Summary of Events
1
Initial colonization by pioneer species
2
Outgrowth, microcolonies are formed which spread outwards and
upwards
Secondary colonisation and multiplication. Species diversity
increases. Theproportion of streptococci decreases as the plaque is
invaded by bacteria from
other genera. The overall cell density decreases and the space
between cells isoccupied by polymers.
Climax Community
This transmission electron micrograph of a section through
mature dental plaque illustrates
some important features . Note the densely packed palisades of
cells at the base of theplaque. These are almost always seen to
have thick cell walls characteristic of cells which
are slow growing due to starvation conditions. Above these the
plaque is less denselypacked with cells and there is an increase in
species diversity illustrated by the presence of
rod-shaped organisms. Electron-dense material between cells are
high molecular weight
polymers such as extracellular polysaccharides synthesised from
sucrose. Within the body ofplaque microcolonies are often featured.
The one labelled above is more visible than others
-
8/3/2019 perio microbioloy
19/22
because it has a very different morphology.
-
8/3/2019 perio microbioloy
20/22
-
8/3/2019 perio microbioloy
21/22
-
8/3/2019 perio microbioloy
22/22