Embed Size (px)
Citation preview
10/7/2013
1
The 2013 Nurse Practitioner Update
October 12th, 2013
Columbia, MD
Aruoriwo Oboh-Weilke, MD
“RED EYE”
Need to determine: If the red eye requires the prompt attention
of an Ophthalmologist
“RED EYE”Disorders associated with a red eye The big three:
Conjunctivitis Uveitis (iritis or
iridocyclitis) Acute angle closure
glaucoma
Other: Herpes simplex keratitis Sub-conjunctival
hemorrhage Episcleritis Scleritis Pterygium Abrasions and foreign
bodies Adnexal disease Secondary to abnormal
lid function
“RED EYE”Symptoms of: Major and Minor
Blurred vision
Severe pain
Photophobia
Colored halos
Exudation
Itching
“RED EYE”
“RED EYE”Nine diagnostic steps1. What is the vision?2. What is pattern of redness?3. The presence and type of discharge?4. Are corneal opacities present?5. Are corneal defects present?6. Depth of anterior chamber?7. Status of pupils?8. Intraocular pressure?9. Proptosis? Limitation of eye movement or
lid?
10/7/2013
2
“RED EYE”Signs of: Major and Minor Reduced visual acuity
Suggests serious ocular disease Never present with simple conjunctivitis
Ciliary flush Injection of deep conjunctival and episcleral vessels Present with uveitis, acute glaucoma, cornea
inflammations Usually not present in conjunctivitis
Corneal opacification Keratic precipitates (KP) - endothelial cellular deposits Diffuse haze - usually due to corneal edema Localized opacities – usually due to ulcer or keratitis
“RED EYE”Signs of: Major and Minor Corneal epithelial disruption
Fluorescein – will stain the areas bright green
Pupillary abnormalities Smaller with uveitis
○ Posterior synechiae – inflammatory adhesions between iris and lens – may cause the pupil to irregular
Acute glaucoma – fixed mid-dilation Conjunctivitis does not affect the pupil
Shallow anterior chamber depth acute angle-closure glaucoma
“RED EYE”Signs of: Major and Minor Corneal epithelial disruption
Fluorescein – will stain the areas bright green
Pupillary abnormalities Smaller with uveitis
○ Posterior synechiae – inflammatory adhesions between iris and lens – may cause the pupil to irregular
Acute glaucoma – fixed mid-dilation Conjunctivitis does not affect the pupil
Shallow anterior chamber depth acute angle-closure glaucoma
“RED EYE”Signs of: Major and Minor
Elevated intra-ocular pressure Seen with glaucoma and sometimes with uveitis
Proptosis Forward displacement of the globe
Acute – suspect cavernous sinus disease or orbital infection
Chronic –○ Most common cause – thyroid disease
○ Tumor or other orbital disease
“RED EYE”Signs of: Major and Minor Conjunctival hyperemia
Seen with almost all conditions which cause red eye
Discharge Purulent or muco-purulent – suggests bacterial
conjunctivitis○ Gonococcal – copious discharge
Serious potentially blinding disease Culture and refer
Serous – suggest viral conjunctivitis White, stringy – suggests allergic conjunctivitis
Pre-auricular lymph node enlargement Usually suggest viral conjunctivitis
“RED EYE”Big threeR
ed
Eye
Con
unc
v
s
o
nea
opac
esNo
ma
OPNodesNo
ma
pup
No
ma
AC
No
ea
y
e
e
a
Excep
o
GC
Uve
s
eCo
nea
KPNo
nodesMaybe
e
eva
ed
OPPup
sma
e
synech
aeCe
s
n
AC
e
e
a
Acu
e
ang
e
g
aucoma
Decreased VAMinimal/moderate pain
Ciliary flushNo discharge
Corneal edemaIncreased IOP
No nodesPupil mid-dilation, fixed
Shallow ACreferral
10/7/2013
3
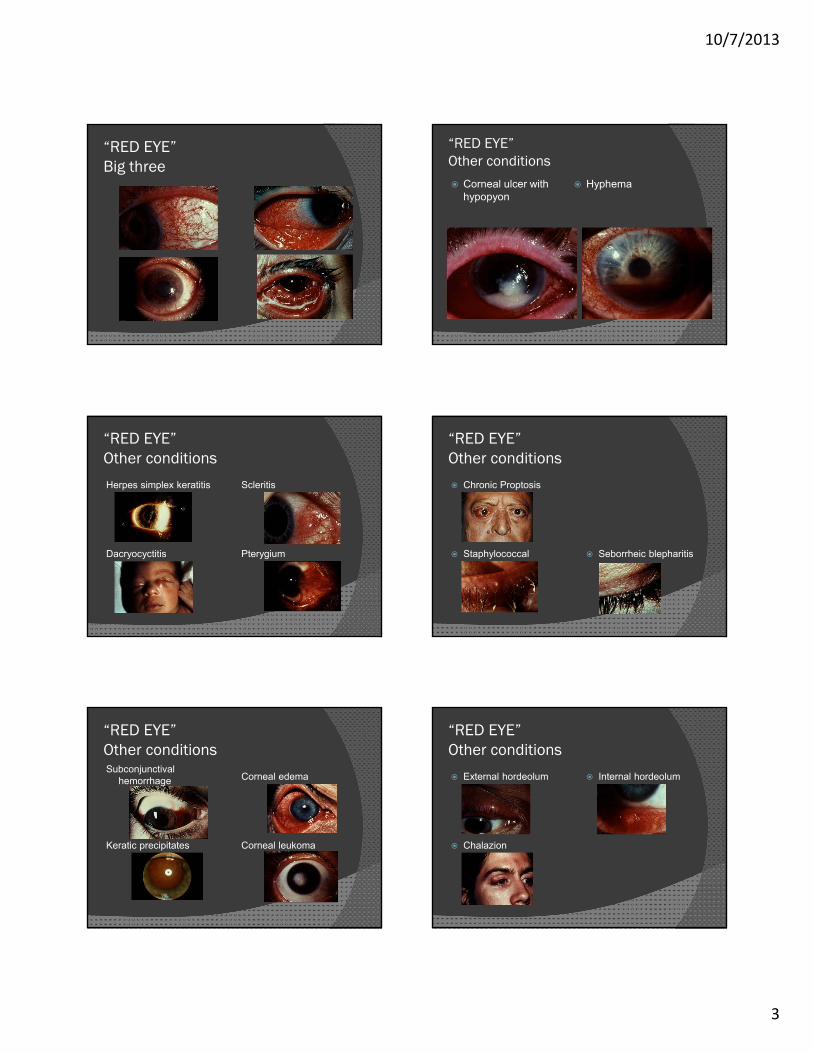
“RED EYE”Big three
“RED EYE”Other conditions
Herpes simplex keratitis Scleritis
Dacryocyctitis Pterygium
“RED EYE”Other conditionsSubconjunctival
hemorrhage Corneal edema
Keratic precipitates Corneal leukoma
“RED EYE”Other conditions
Corneal ulcer with hypopyon
Hyphema
“RED EYE”Other conditions
Chronic Proptosis
Staphylococcal blepharitis
Seborrheic blepharitis
“RED EYE”Other conditions
External hordeolum Internal hordeolum
Chalazion
10/7/2013
4

10/7/2013
5
“RED EYE”Points to remember
If the VA is acutely reduced, a Dx of conjunctivitis is highly unlikely
Unequal pupils are a sign of serious ocular disease
Use Fluorescein to test for corneal epithelial integrity
Topical anesthetics - Use for Dx exam only Inhibit growth and healing of corneal
epithelium Eliminates the protective blink reflex
Topical steroids Keratitis Cataract Elevated IOP
“RED EYE”Therapeutic warnings
CASE REPORT
A 31 year old caucasian female was referred for an ophthalmology consultation by her internist. The patient stated she had noticed redness of her left eye for one week. This was accompanied by boring left ocular pain. The patient had seen an optometrist who started her on topical steroids. She reported worsening of the symptoms on this regimen. She then saw her internist who started her on systemic steroids and promptly referred her to the eye clinic.
CASE REPORT On review of systems, the patient admitted to blurry
vision, pain on eye motion and blood in her urine. On further questioning about her medical problems, she stated that she had been diagnosed and treated for IgA nephropathy for 4 years. She previously had proteinuria and microscopic hematuria as manifestations of her renal condition and had been followed by her nephrologist. Her diagnosis of IgA nephropathy had been confirmed by a renal biopsy. Her last follow-up with her nephrologist was 1 year prior to this presentation and she was noted to have a stable renal status at that time.
CASE REPORT On physical examination, the patient’s VA was
OD 20/25 and OS 20/40 EOM were full, however, there was pain on
motion. Pupils and IOPs were normal. Slit Lamp Exam revealed diffusely inflammed
temporal conjunctival and underlying scleral vessels with scleral and episcleral edema. There was minimal blanching with the application of topical phenylephrine.
Dilated fundus exam was normal and did not reveal any choroidal folds
RESULTS The patient was continued on the oral steroids
and tapered according to her symptoms. Her symptoms resolved after 2 weeks.
A work-up for more common causes of scleritis was undertaken.
CBC, ESR, RF, ANA, c-ANCA, p-ANCA, uric acid and ACE levels were all negative.
A 24 hour urine collection revealed proteinuria. An appointment was made for the patient to see her nephrologist, to evaluate whether there was any worsening of her renal status.
10/7/2013
6
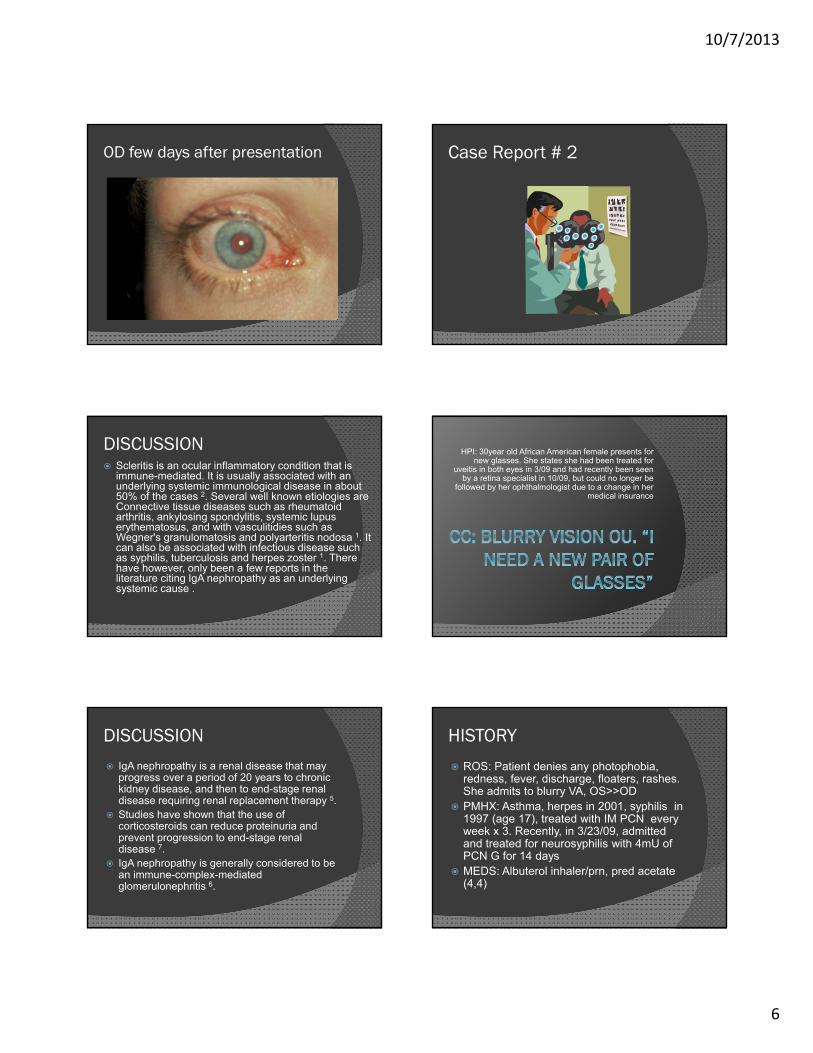
OD few days after presentation
DISCUSSION Scleritis is an ocular inflammatory condition that is
immune-mediated. It is usually associated with an underlying systemic immunological disease in about 50% of the cases 2. Several well known etiologies are Connective tissue diseases such as rheumatoid arthritis, ankylosing spondylitis, systemic lupus erythematosus, and with vasculitidies such as Wegner's granulomatosis and polyarteritis nodosa 1. It can also be associated with infectious disease such as syphilis, tuberculosis and herpes zoster 1. There have however, only been a few reports in the literature citing IgA nephropathy as an underlying systemic cause .
DISCUSSION
IgA nephropathy is a renal disease that may progress over a period of 20 years to chronic kidney disease, and then to end-stage renal disease requiring renal replacement therapy 5.
Studies have shown that the use of corticosteroids can reduce proteinuria and prevent progression to end-stage renal disease 7.
IgA nephropathy is generally considered to be an immune-complex-mediated glomerulonephritis 6.
Case Report # 2
HPI: 30year old African American female presents for new glasses. She states she had been treated for
uveitis in both eyes in 3/09 and had recently been seen by a retina specialist in 10/09, but could no longer be
followed by her ophthalmologist due to a change in her medical insurance
HISTORY
ROS: Patient denies any photophobia, redness, fever, discharge, floaters, rashes. She admits to blurry VA, OS>>OD
PMHX: Asthma, herpes in 2001, syphilis in 1997 (age 17), treated with IM PCN every week x 3. Recently, in 3/23/09, admitted and treated for neurosyphilis with 4mU of PCN G for 14 days
MEDS: Albuterol inhaler/prn, pred acetate (4,4)
10/7/2013
7
PHYSICAL EXAM VASC 20/20 OD, 20/40-2 OS Pupils: 4-3mm OD, 3-2mm, No RAPD Tap, 10mmHg OU EOM: Full SLE: 2+ injection OD, trace OS 2-3+ fine KPs OD, 4+ mutton fat KP OS 2+ c/f OD, 1-2+ c/f OS 360 Posterior synechia OS, iris nodule @ 7 o’
clock Clear lens DFE: Slightly hazy medium C:D 0.3 healthy nerves, flat fovea
PHYSICAL EXAM
DIFFERENTIONAL DIAGNOSIS
Bilateral, granulomatous uveitis ant/post involvement
Syphilis
Sarcoidosis
Tuberculosis
Lyme disease
Herpes
HLA -B27 associated
TESTS/WHAT TO DO NEXTIncreased her topical steroids, started scopalamine. Requested for old records. Follow-up 1 week3/23/10 tests done: LP, HIV, HLA B27, RPR, ESR, CRP, ANA, ANCA, ACE levels were done2/10: RPR,CBC,ESR, HLA-B27,ACE,RF,ANA, Lyme Titres, PPD, CXRCTScan of chest performed. Transbronchialbiopsy
TREATMENT
Received systemic steroids, intravitreal kenalog Developed dense PSC, underwent
Phaco/Ant/posterior synechialysis/PCIOL ( now that was one of the longer hours of my life)
Underwent pars-plana vitrectomy with epiretinalmembrane peeling for significant posterior involvement.
Doing well systemically. Off her oral predisone. Vision is 20/20 OD, 20/40 OS and is controlled on very low dose topical NSAIDS and steroids
DISCUSSION Sarcoidosis is a multisystem disease. Typically
affects pulmonary function, can also affect liver function and the CNS
In US, occurs 10x more in AA, than in caucasians. Age range typically 20 – 50yrs. ¼ to ½ of patients with systemic dz will have ocular dz. Uveitis being the most common
All structures of the eye could be affected. If there’s clinical suspicion, but tests are
negative, limited gallium scan of head/neck can be done. Also, biopsy of skin, conjunctiva or lacrimal gland lesions, or transbronchial can be performed.
10/7/2013
8
CASE REPORT # 3
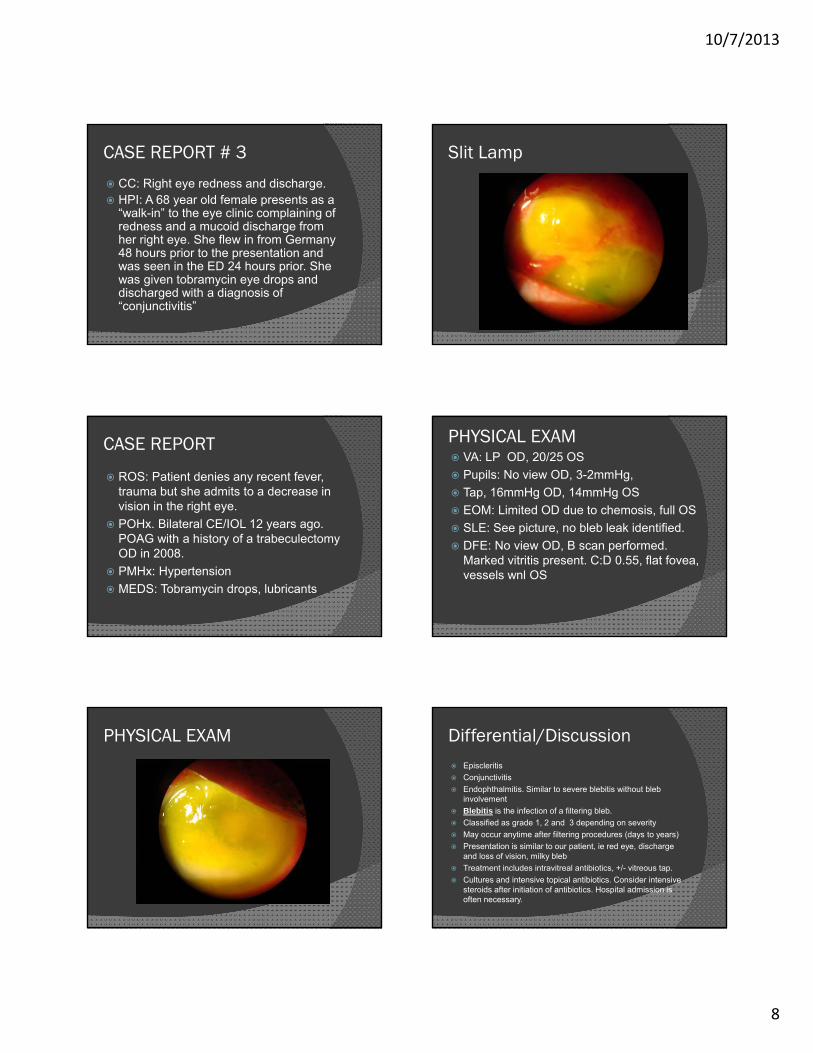
CC: Right eye redness and discharge. HPI: A 68 year old female presents as a
“walk-in” to the eye clinic complaining of redness and a mucoid discharge from her right eye. She flew in from Germany 48 hours prior to the presentation and was seen in the ED 24 hours prior. She was given tobramycin eye drops and discharged with a diagnosis of “conjunctivitis”
CASE REPORT
ROS: Patient denies any recent fever, trauma but she admits to a decrease in vision in the right eye.
POHx. Bilateral CE/IOL 12 years ago. POAG with a history of a trabeculectomyOD in 2008.
PMHx: Hypertension
MEDS: Tobramycin drops, lubricants
PHYSICAL EXAM
Slit Lamp
PHYSICAL EXAM VA: LP OD, 20/25 OS
Pupils: No view OD, 3-2mmHg,
Tap, 16mmHg OD, 14mmHg OS
EOM: Limited OD due to chemosis, full OS
SLE: See picture, no bleb leak identified.
DFE: No view OD, B scan performed. Marked vitritis present. C:D 0.55, flat fovea, vessels wnl OS
Differential/Discussion Episcleritis
Conjunctivitis
Endophthalmitis. Similar to severe blebitis without bleb involvement
Blebitis is the infection of a filtering bleb.
Classified as grade 1, 2 and 3 depending on severity
May occur anytime after filtering procedures (days to years)
Presentation is similar to our patient, ie red eye, discharge and loss of vision, milky bleb
Treatment includes intravitreal antibiotics, +/- vitreous tap.
Cultures and intensive topical antibiotics. Consider intensive steroids after initiation of antibiotics. Hospital admission is often necessary.



























![HLA-B27 [Human Leukocite Antigen] B27.pdf · HLA-B27 [Human Leukocite Antigen] Questo test è utile per determinare la presenza o l’assenza dell’antigene HLA-B27 sulla superficie](https://img.pdfslide.tips/doc/110x75/5ebb1ebaa0a9221249652263/hla-b27-human-leukocite-antigen-b27pdf-hla-b27-human-leukocite-antigen-questo.jpg)