Embed Size (px)
Citation preview

___________________________________________________________
Interuniversitaire opleiding
Master in de verzekeringsgeneeskunde en de medische expertise Eindverhandeling
__________________________________________________________________________
Return to work of patients treated with spinal cord stimulation for chronic pain:
a systematic review and meta-analysis
Maarten MOENS
Promotor: Prof. dr. Jan Verlooy
__________________________________________________________________________
Academiejaar 2017-2018
1

This thesis has been accepted for publication in Neuromodulation: Technology at the Neural Interface.
2

Return to work of patients treated with spinal cord stimulation for chronic pain: a systematic review and meta-analysis
Maarten Moens MD, PhD1,2,3,4; Lisa Goudman MSC1,4; Raf Brouns MD, PhD5,6; Alexis Valenzuela Espinoza7; Mats De Jaeger MSC1 ; Eva Huysmans MSC7,8; Koen Putman PhD7; Jan Verlooy MD, PhD9
1Department of Neurosurgery, UZ Brussel, Brussels, Belgium 2Department of Radiology, UZ Brussel, Brussels, Belgium 3Center for Neurosciences (C4N), Vrije Universiteit Brussel, Belgium 4Department of Manual Therapy (MANU), Vrije Universiteit Brussel, Brussels, Belgium 5Department of Neurology, ZorgSaam Hospital, Terneuzen, The Netherlands 6Faculty of Medicine and Pharmacy, Vrije Unversiteit Brussel, Belgium 7Department of Public Health (GEWE), Faculty of Medicine and Pharmacy, Vrije Universiteit Brussel, Brussels, Belgium8Department of Physiotherapy, Human Physiology and Anatomy, Faculty of Physical Education & Physiotherapy (KIMA), Vrije Universiteit Brussel, Brussels, Belgium
9Department of Epidemiology and Social Medicine (ESOC), Universiteit Antwerpen, Antwerpen, Belgium
Abstract Background Chronic pain has a substantial negative impact on work-related outcomes, which underscores the importance of interventions to reduce the burden. Spinal cord stimulation (SCS) efficiently causes pain relief in specific chronic pain syndromes. The aim of this review was to identify and summarize evidence on returning to work in patients with chronic pain treated with SCS.
Methods A systematic literature review was performed including studies from PubMed, EMBASE, SCOPUS, and Web of Science (up till October 2017). Risk of bias was assessed using a modified version of the Downs & Black checklist. Where possible, we pooled data using random-effects meta-analysis. The study protocol was registered prior to initiation of the review process (PROSPERO CRD42017077803).
Results Fifteen full-text articles (total articles screened: 2,835) were included. Risk of bias for these articles was scored low. Seven trials provided sufficient data and were judged similar enough to be pooled for meta-analysis on binary outcomes. SCS intervention results in a higher prevalence of patients at work compared with before treatment (OR 2,15; 95% CI, 1,44 to 3,21; I2 = 42%; p < 0,001). SCS treatment results also in high odds to return to work (OR 29,06; 95% CI, 9,73 to 86,75; I2 = 0%; p < 0,001).
Conclusions Based on available literature, SCS proved to be an effective approach to stimulate return to work in patients with specific chronic pain syndromes.
3

Background Spinal cord stimulation (SCS) is a well-known safe and effective treatment for many chronic
pain syndromes, including failed back surgery syndrome (FBSS), low back and lower
extremity pain, complex regional pain syndrome, and other neuropathic conditions(1-4).
Despite the extreme complexity of chronic pain, pain relief is the principal desired outcome
for SCS(1). The high socioeconomic burden and healthcare utilization associated with
chronic pain are therefore often reduced to secondary outcomes (5-7). When pain becomes
chronic, return to work (RTW) is negatively associated with a delay in referral to treatment,
socioeconomic status, attorney involvement, and worker’s compensation are(8). Several
studies have shown that unemployment and absenteeism are “negatively associated with
quality of life, depression and generally poor health outcomes”(9-11).
Currently, it is well accepted that SCS is an effective treatment for reducing pain and
improving quality of life, but little is known about the impact of SCS on occupational
outcome parameters such as RTW. Therefore, we conducted a systematic review and meta-
analysis to identify not only the prevalence of RTW by SCS in patients with chronic pain but
also the odds of working with SCS.
Methods Search strategy and selection criteria
This systematic review and meta-analysis were conducted in accordance with the PRISMA
(Preferred Reporting Items for Systematic Review and Meta-Analyses) guidance(12). The
electronic databases of PubMed, Embase, SCOPUS, and Web of Science were searched from
inception to October 20th, 2017 to identify potentially relevant studies.
The search strategy was, based on the PICO (evidence based search strategy focusing on
Patient/Population, Intervention, Comparison and Outcome) Framework (13). Our search
was not limited to randomized controlled trials (RCTs) but also included case series. A
4

language restriction of English, French, German, and Dutch was applied. We included
studies that met the following criteria: (1) population – adult (³18 years old) chronic pain
patients eligible for SCS; (2) intervention – SCS; (3) outcome – RTW, employment status and
sick leave. We excluded studies enrolling patients receiving other types of neuromodulation
and publications available only in abstract form or meeting reports.
Data extraction and quality assessment
After combining search results from different databases and removing duplicates by using
EndNote reference manager, two investigators (MM and LG) independently reviewed all the
retrieved abstracts and full texts to remove ineligible studies. In case of disagreement,
consensus was sought through consultation and discussion with a third party (RB). The two
reviewers (MM and LG) independently extracted data from included studies, using an a
priori determined data extraction form comprising the following items (1) first author (2)
year of publication, (3) country, (4) sample size in relation to RTW outcome, (5) study
design, (6) diagnosed population, (7) type of SCS and (8) all predefined outcomes. The
quality of the included studies was evaluated using the risk of bias Downs and Black
checklist (modified version) (14). We assigned a value of 0 or 1 to the different
subcategories of the following items: reporting, external validity and internal validity. A total
score < 10/16 was considered to be low quality, while scores ³ 10/16 were presumed to be
high quality. Discrepancies were identified and resolved through discussion.
Outcome and statistical analysis
The primary goal of this study was to identify the prevalence of work resumption after
implantation of SCS. Subgroup analyses were performed to evaluate the occupational status
at last follow-up point. The results from all relevant studies were merged to estimate the
pooled odds ratio (OR) and associated 95% confidence intervals (CI’s) for dichotomous
outcomes. The outcomes were pooled using a random effects model. All p< 0,05 were
considered statistically significant. Heterogeneity was tested with I2 statistics. This statistic
can be interpreted as the proportion of the total variation in the estimated treatment effect
due to the heterogeneity among studies(15). To explore the robustness and the potential
5

influence of various factors on our primary outcome, we performed a subgroup analysis
based on pathology (back and leg pain versus mixed). The Dixon’s Q test for the rejection of
extreme values (at the 5 and 1% levels) was performed to identify outliers(16). Publication
bias was evaluated by visual inspection of the funnel plot. All statistical analyses were
performed using RStudio (version 0.99.903, RStudio, Inc).
Results Study selection
A flowchart of the search strategy and the reasons for exclusion are shown in figure 1. The
initial search identified a total of 2,835 citations. After combining the results, removing
duplicates and selections based on the title and abstract, 54 full-text studies remained.
Thirty-nine studies were excluded after reviewing the full text: 10 because of inappropriate
outcome parameters (no RTW mentioned), 28 were excluded because of unsuitable study
design or conference meeting abstract and, one because no full text was available even
after communication with the first author. Thus, 15 full-text studies were read for further
evaluation. Of those 15 studies, 6 were excluded because they did not provide sufficient
information on the occupational status at last follow-up point(17-22), 1 was excluded
because the studied population was reported in another study(23, 24), and 1 study did not
pass the outlier test(25). This study from Harke et al. was considered an outlier at the level 5
and at the 1%(25). Finally, the remaining seven, which enrolled 824 patients, were included
in the meta-analysis(23, 26-31).
Study characteristics and quality
The main characteristics and predefined outcome data of the included studies for the
systematic review are described in table 1. These studies were published between 1978 and
2017, with sample sizes ranging from 20 to 410. One RCT was included, five retrospective
case series and one prospective cohort study. One study evaluated high-frequency SCS,
while the other studies reported on the use of conventional SCS (29). The mean follow-up
period varied from 1 year to 7.1 years. Three studies were included with a study population
6

suffering from back and/or leg pain (FBSS with axial back pain and unilateral limb pain),
while four other studies described a more heterogeneous study population (i.e., FBSS,
multiple sclerosis, spinal cord injury, vascular disease, cancer, occipital neuralgia, trauma,
and peripheral neuropathy). The risk of bias Downs and Black checklist score for each
citation varied across the studies, ranging from 10 to 16 out of 17.
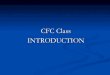
Primary Outcome
Occupational status
The number of patients working after SCS was mentioned in all seven studies. The pooled
analysis showed that SCS increases the odds to work after SCS (7 studies; n = 824, OR 2,15;
95% CI, 1,44 to 3,21; I2 = 42%; p = 0,0001). Given the moderate heterogeneity, a subgroup
based on the type of population was also evaluated. The type of population (chronic back
and/or leg pain versus mixed pain syndromes) was defined to be a factor influencing
heterogeneity (figure 2).
In general, both subgroups analyses confirmed similar OR of working status among groups.
The funnel plot shows no publication bias (available upon request).
Return to work %RTW, defined as the percentage of patients going back to work who were unemployed
before treatment, was reported or could be calculated in all seven studies. The %RTW
varied between 10 and 47 (mean 14). The pooled analysis showed that SCS increases the
odds to return to work after SCS in patients with absenteeism before treatment (7 studies;
n = 701, OR 29,06; 95% CI, 9,73 to 86,75; I2 = 0%; p < 0,0001). The funnel plot shows no
publication bias (available upon request).
Secondary outcomes
The types of employment after returning to work were not reported in all seven studies.
Three studies described the number of patients with part-time and full-time employment
after SCS implantation at the last follow-up(29, 30, 32). Two studies also mentioned the
numbers of patients who increased working time after SCS implantation(26, 30). One study
7

presented the percentage of patients with SCS working at various follow-up points(31). Yet
another study reported the median time of unemployment(28).
Discussion In the past two decades, SCS for pain relief has evolved to include many new methods of
current delivery by neurostimulation devices(3). This resulted in several studies presenting
excellent results on pain reduction. Although the status of “remission,” or achieving almost
complete pain relief by SCS, for some patients has been reported, occupational outcomes,
such as RTW, are rarely an outcome parameter in neuromodulation studies(33). SCS has
shown superior efficacy to conventional medical management in an FBSS population and
SCS leads to long-term health care cost savings(28, 34). These data support the long-term
cost utility of SCS in the treatment of FBSS patients(34). However, in a chronic pain
population, it is well known that two thirds of the total health care costs are represented by
indirect costs (loss of productivity or working days lost)(35).
Our epidemiological meta-analysis included seven studies with 824 patients investigated
occupational outcomes. Despite the clinical heterogeneity of the subgroup “chronic back
and leg pain”, the results for this subgroup appeared to be statistically homogenous and this
in contrast to the subgroup with mixed diagnoses. This can be explained by the fact that the
mixed group consists of various diagnoses with variable evidence for SCS, while SCS for
chronic low back pain has proven to be effective and has reached a recommendation in the
recent European Academy of Neurology (EAN) guidelines(36).
This meta-analysis showed that, among chronic pain patients, SCS improves the odds of
returning to work and that SCS results in more patients at work, compared with the same
population before SCS.
In terms of %RTW, the percentage of patients going back to work who were unemployed
before treatment, SCS seems to allow chronic pain patients to work again. Since SCS
candidates are refractory to conventional pain therapy and therefore difficult to treat, a
mean of 14% of unemployed patients returning to work should be born in mind. However,
no information is available in these studies on the type of work the patients are returning
to. Although three studies reported the number of patients returning to work on a part-time
basis, the relevant number of hours worked daily was not mentioned(24, 26, 30). Young et
8

al. considered returning to household duties or to studying as returning to gainful
employment(31). It is generally accepted that patients at working age or defined as patients
under the age of 65 are more likely to return to work. This specific subdivision of patients
receiving SCS was reported only in a minority of the reviewed studies(28-30).
The number of patients found in this meta-analysis is similar to the findings of the
systematic review of Frey et al. in 2009(37). They summarized a 13% entry in gainful
employment and return to work in 16 to 31% of FBSS patients(37).
Researchers agree that both job loss and continuing “worklessness” impact adversely on
people’s health with increased levels of both mental and physical problems(38).
Notwithstanding the evidence of using classical pain relief, functionality, and quality of life
as outcome measurements in chronic pain studies, RTW as a central determinant of
(mental) health, should also be considered as an important clinical outcome measure.
Additionally, Elfering et al. reported that only measuring global work status and %RTW as
work-related outcome parameters, lack specificity(39). In-depth and detailed analyses, clear
definitions, disjunctive classes of categories and adequate time frames might upgrade this
specificity. Job description and educational level, type of employment (full time, part time or
casual), reasons for unemployment, work-related attitudes (e.g. job satisfaction, work-
related expectations, ...) and other risk factors for chronic disability may also be taken in
consideration(39, 40).
Strengths and limitations To diminish bias, the study selection, data extraction, and evaluation of study quality were
performed by two independent reviewers. We comprehensively analyzed the odds of
working and the odds of RTW after SCS treatment in studies with different designs.
There were also several potential limitations regarding our meta-analysis. First, some well-
designed studies were excluded because they lacked essential information about the work
status of all patients. Second, the sample size was small as only seven studies were included.
Third, the bias of the publications might have affected the validity of our conclusions, such
as lack of comparison (e.g. best medical treatment, other types of therapies, …). And finally,
the search method was limited to Medline, Embase, Web of Science and Scopus. We did not
search the “grey literature” (trial registries nor backward references).
9

Conclusion
In summary, based on available data, this meta-analysis demonstrates that SCS treatment
results in more patients at work and also more patients returning to work. More, large-scale
studies are warranted to analyze in detail the work status of the included patients (type of
job, full time, part-time, % patients at working age, etc).
References 1. Sitzman BT, Provenzano DA. Best Practices in Spinal Cord Stimulation. Spine (Phila Pa 1976) 2017;42 Suppl 14:S67-S71. 2. Deer TR, Mekhail N, Provenzano D, Pope J, Krames E, Leong M, et al. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the Neuromodulation Appropriateness Consensus Committee. Neuromodulation 2014;17:515-50; discussion 50. 3. Deer TR, Krames E, Mekhail N, Pope J, Leong M, Stanton-Hicks M, et al. The appropriate use of neurostimulation: new and evolving neurostimulation therapies and applicable treatment for chronic pain and selected disease states. Neuromodulation Appropriateness Consensus Committee. Neuromodulation 2014;17:599-615; discussion 4. Eldabe S, Buchser E, Duarte RV. Complications of Spinal Cord Stimulation and Peripheral Nerve Stimulation Techniques: A Review of the Literature. Pain Med 2016;17:325-36. 5. Mann EG, Johnson A, VanDenKerkhof EG. Frequency and characteristics of healthcare visits associated with chronic pain: results from a population-based Canadian study. Can J Anaesth 2016;63:411-41. 6. Breivik H, Eisenberg E, O'Brien T, Openminds. The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Health 2013;13:1229. 7. Duenas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res 2016;9:457-67. 8. Steenstra IA, Munhall C, Irvin E, Oranye N, Passmore S, Van Eerd D, et al. Systematic Review of Prognostic Factors for Return to Work in Workers with Sub Acute and Chronic Low Back Pain. J Occup Rehabil 2017;27:369-81. 9. Mathers CD, Schofield DJ. The health consequences of unemployment: the evidence. Med J Aust 1998;168:178-82. 10. Martella D. MA. Unemployment and life satisfaction: the moderating role of time structure and collectivism. J Appl Soc Psychology 2000;30:1095-108. 11. Gallie D. RH. Unemployment and life satisfaction: a cross cultural comparison. Eur J Sociology 1998;39:248-80. 12. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8:336-41. 13. O'Sullivan D, Wilk S, Michalowski W, Farion K. Using PICO to align medical evidence with MDs decision making models. Stud Health Technol Inform 2013;192:1057.
10

14. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health 1998;52:377-84. 15. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statistics in medicine 2002;21:1539-58. 16. Dixon WJ. Analysis of extreme values. Ann Math Stat 1950;21:488-506. 17. Devulder J, De Laat M, Van Bastelaere M, Rolly G. Spinal cord stimulation: a valuable treatment for chronic failed back surgery patients. J Pain Symptom Manage 1997;13:296-301. 18. Hamm-Faber TE, Aukes HA, de Loos F, Gultuna I. Subcutaneous stimulation as an additional therapy to spinal cord stimulation for the treatment of lower limb pain and/or back pain: a feasibility study. Neuromodulation 2012;15:108-16; discussion 16-7. 19. Kupers RC, Van den Oever R, Van Houdenhove B, Vanmechelen W, Hepp B, Nuttin B, et al. Spinal cord stimulation in Belgium: a nation-wide survey on the incidence, indications and therapeutic efficacy by the health insurer. Pain 1994;56:211-6. 20. Sundaraj SR, Johnstone C, Noore F, Wynn P, Castro M. Spinal cord stimulation: a seven-year audit. J Clin Neurosci 2005;12:264-70. 21. North RB, Kidd DH, Petrucci L, Dorsi MJ. Spinal cord stimulation electrode design: a prospective, randomized, controlled trial comparing percutaneous with laminectomy electrodes: part II-clinical outcomes. Neurosurgery 2005;57:990-6; discussion -6. 22. Kumar A, Felderhof C, Eljamel MS. Spinal cord stimulation for the treatment of refractory unilateral limb pain syndromes. Stereotact Funct Neurosurg 2003;81:70-4. 23. North RB, Ewend MG, Lawton MT, Kidd DH, Piantadosi S. Failed back surgery syndrome: 5-year follow-up after spinal cord stimulator implantation. Neurosurgery 1991;28:692-9. 24. North RB, Ewend MG, Lawton MT, Piantadosi S. Spinal cord stimulation for chronic, intractable pain: superiority of "multi-channel" devices. Pain 1991;44:119-30. 25. Harke H, Gretenkort P, Ladleif HU, Rahman S. Spinal cord stimulation in sympathetically maintained complex regional pain syndrome type I with severe disability. A prospective clinical study. Eur J Pain 2005;9:363-73. 26. Kumar K, Hunter G, Demeria D. Spinal cord stimulation in treatment of chronic benign pain: challenges in treatment planning and present status, a 22-year experience. Neurosurgery 2006;58:481-96; discussion -96. 27. Gopal H, Fitzgerald J, McCrory C. Spinal cord stimulation for FBSS and CRPS: A review of 80 cases with on-table trial of stimulation. J Back Musculoskelet Rehabil 2016;29:7-13. 28. Kumar K, Taylor RS, Jacques L, Eldabe S, Meglio M, Molet J, et al. The effects of spinal cord stimulation in neuropathic pain are sustained: a 24-month follow-up of the prospective randomized controlled multicenter trial of the effectiveness of spinal cord stimulation. Neurosurgery 2008;63:762-70; discussion 70. 29. Al-Kaisy A, Palmisani S, Smith TE, Pang D, Lam K, Burgoyne W, et al. 10 kHz High-Frequency Spinal Cord Stimulation for Chronic Axial Low Back Pain in Patients With No History of Spinal Surgery: A Preliminary, Prospective, Open Label and Proof-of-Concept Study. Neuromodulation 2017;20:63-70. 30. North RB, Kidd DH, Zahurak M, James CS, Long DM. Spinal cord stimulation for chronic, intractable pain: experience over two decades. Neurosurgery 1993;32:384-94; discussion 94-5.
11

31. Young RF. Evaluation of dorsal column stimulation in the treatment of chronic pain. Neurosurgery 1978;3:373-9. 32. North RB, Campbell JN, James CS, Conover-Walker MK, Wang H, Piantadosi S, et al. Failed back surgery syndrome: 5-year follow-up in 102 patients undergoing repeated operation. Neurosurgery 1991;28:685-90; discussion 90-1. 33. Khan H, Pilitsis JG, Prusik J, Smith H, McCallum SE. Pain Remission at One-Year Follow-Up With Spinal Cord Stimulation. Neuromodulation 2018;21:101-5. 34. Lad S, Petrella J, Xie J, Parente B, Pagadala P, Yang S, et al. Long-term Cost Utility of Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome. Pain Physician 2017;20:E797-E805. 35. Lardon A, Dubois JD, Cantin V, Piche M, Descarreaux M. Predictors of disability and absenteeism in workers with non-specific low back pain: A longitudinal 15-month study. Appl Ergon 2018;68:176-85. 36. Cruccu G, Garcia-Larrea L, Hansson P, Keindl M, Lefaucheur JP, Paulus W, et al. EAN guidelines on central neurostimulation therapy in chronic pain conditions. Eur J Neurol 2016;23:1489-99. 37. Frey ME, Manchikanti L, Benyamin RM, Schultz DM, Smith HS, Cohen SP. Spinal cord stimulation for patients with failed back surgery syndrome: a systematic review. Pain Physician 2009;12:379-97. 38. Litchfield P, Cooper C, Hancock C, Watt P. Work and Wellbeing in the 21st Century dagger. Int J Environ Res Public Health 2016;13. 39. Elfering A. Work-related outcome assessment instruments. Eur Spine J 2006;15 Suppl 1:S32-43. 40. Cancelliere C, Donovan J, Stochkendahl MJ, Biscardi M, Ammendolia C, Myburgh C, et al. Factors affecting return to work after injury or illness: best evidence synthesis of systematic reviews. Chiropr Man Therap 2016;24:32.
12

Figure legend Table 1 Characteristics of included studies.
Abbreviations: RTW: return to work; mo: months; y: year(s); CLBP: chronic low back pain; FBSS: failed back surgery syndrome; PT/FT: part time/full time; SCS: spinal cord stimulation Explanation: Country (C): presented in ISO3166-1 alpha-2 codes (US: United States of America; GB: Great Britain; CA: Canada; IE: Ireland) Study Type: RCT: randomized controlled trial; retro case series: retrospective case series; prosp cohort study: prospective cohort study N: total sample size for return to work analysis Population: type of population eligible to SCS: Mixed: a mixed group of patients with different diagnoses; CLBP: chronic low back pain patients; FBSS: patients with failed back surgery syndrome Mean postoperative sick leave duration: Presents the median time of unemployment before SCS treatment Follow-up points: either a fixed follow-up moment, or a mean of follow-up. %RTW (No of patients): X% of the patients has returned to work PT/FT: number of patients returned to work (part-time / full-time) Working at baseline: number of patients at work at baseline Working after SCS: number of patients at work after SCS at the latest follow-up point Figure 1: Flow chart of study selection in meta-analysis of occupational outcome after SCS treatment Figure 2: Forest plot of working status with SCS compared with before treatment
13

14

15

Pre-SCSSCSTotalTotal WorkingWorking
16

Appendix A: PICO Free terms MeSH-terms Population “Chronic pain patients”;
“chronic pain”; “persistent pain” “intractable pain”; AND "Causalgia"; "Reflex sympathetic dystrophy"; “failed back surgery syndrome”; “post laminectomy syndrome”; “postlaminectomy syndrome”; “failed neck surgery syndrome”; “CRPS”; “complex regional pain syndrome”; “complex regional pain syndromes”; “FBSS”; “FNSS”; “peripheral neuropathy”; “neuropathic pain”; “angina pectoris”; “peripheral vascular disease”; "peripheral vascular diseases"; "Peripheral nervous system diseases"
Chronic pain; Pain, Intractable; AND Failed back surgery syndrome; Causalgia; Complex regional pain syndromes; Reflex sympathetic dystrophy; peripheral nervous system diseases; neuropathic pain; angina pectoris; peripheral vascular diseases;
Intervention “Spinal cord stimulation”; "Neurostimulation"; "Neuromodulation"; “Dorsal column stimulation”; "Neurostimulator"; “Spinal cord stimulator”; “Dorsal column stimulator”; “electrical stimulation”; “pain stimulator”; “pain stimulation”;
spinal cord stimulation; Implantable neurostimulators; Electric stimulation therapy; Electric stimulation;
Control / / Outcome “occupation”;
“re-employment”; “professional situation”; “return-to-work”; “back to work”; “back-to-work”; “work activity”; “employment status”;
Return to work; Employment; Sick leave
17

Resume; Reintegration; Reinsertion; Incapacity AND Work; “labour market”; “labor market”; Professional; Occupation; occupational “disability leave”; “Sick day”; “sick days”; “illness day”; “illness days”; “disability pension”; “occupational disability”; “work disability”
18

Appendix B: Systematic literature search for PubMed
SEARCH 20/10/2017 PubMed
POPULATION
"Chronic pain patients" 2488
“chronic pain” 33327
“persistent pain” 4259
“intractable pain” 7309
“failed back surgery syndrome” 720
“post laminectomy syndrome” 30
“failed neck surgery syndrome” 4
“postlaminectomy syndrome” 32
“CRPS” 1886
“complex regional pain syndrome” 2415
“complex regional pain syndromes" 1245
“FBSS” 257
“FNSS” 23
“peripheral neuropathy” 15580
“neuropathic pain” 15952
“angina pectoris” 40590
“peripheral vascular disease” 8305
"Causalgia" 906
"Reflex sympathetic dystrophy" 3999
"peripheral vascular diseases" 12965
"Peripheral nervous system diseases" 21388
"Chronic Pain"[Mesh] 8555
"Pain, Intractable"[Mesh] 5987
"Failed back surgery syndrome"[Mesh] 233
"Causalgia"[Mesh] 666
"Complex regional pain syndromes"[Mesh] 5154
"Reflex sympathetic dystrophy"[Mesh] 3499
"peripheral nervous system diseases"[Mesh] 133020
19

"neuralgia"[Mesh] 27216
"angina pectoris"[Mesh] 41824
"peripheral vascular diseases"[Mesh] 49171
(((((((((((((((((((((((((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable pain”) OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "Causalgia") OR "Pain, Intractable"[Mesh]) OR "Failed back surgery syndrome"[Mesh]) OR "Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh]) OR neuralgia) OR "peripheral nervous system diseases"[Mesh]) OR "Peripheral nervous system diseases") OR "peripheral vascular diseases"
297580
(((((((((((((((((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable pain”) OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "Causalgia") OR "Reflex sympathetic dystrophy") OR "peripheral vascular diseases") OR "Peripheral nervous system diseases"
150948
((((((((("Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh]) OR "Failed back surgery syndrome"[Mesh]) OR "Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh]
245267
((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable pain”) OR "Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh]
42953
(((((((((((((((((((((((("Causalgia") OR "Reflex sympathetic dystrophy") OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "peripheral vascular diseases") OR "Peripheral nervous system diseases") OR "Failed back surgery syndrome"[Mesh]) OR "Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh]
260924
(((((((((((((((((((((((((("Causalgia") OR "Reflex sympathetic dystrophy") OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "peripheral vascular diseases") OR "Peripheral nervous system diseases") OR "Failed back surgery syndrome"[Mesh]) OR
6030
20

"Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh])) AND (((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable pain”) OR "Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh])
INTERVENTION
“Spinal cord stimulation” 2565
"Neurostimulation" 1985
"Neuromodulation" 7171
“Dorsal column stimulation” 195
"Neurostimulator" 385
“Spinal cord stimulator” 321
“Dorsal column stimulator” 18
“electrical stimulation” 41302
“pain stimulator” 12
“pain stimulation” 452
"spinal cord stimulation"[Mesh] 568
"implantable neurostimulators"[Mesh] 9204
"electric stimulation therapy"[Mesh] 68867
"electric stimulation"[Mesh]
122883
((((((((((((("electric stimulation"[Mesh]) OR "electric stimulation therapy"[Mesh]) OR "implantable neurostimulators"[Mesh]) OR "spinal cord stimulation"[Mesh]) OR “pain stimulation”) OR “pain stimulator”) OR “electrical stimulation”) OR “Dorsal column stimulator”) OR “Spinal cord stimulator”) OR "Neurostimulator") OR “Dorsal column stimulation”) OR "Neuromodulation") OR "Neurostimulation") OR “Spinal cord stimulation”)
216118
POPULATION AND INTERVENTION
(((((((((((((((((((((((((((("Causalgia") OR "Reflex sympathetic dystrophy") OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "peripheral vascular diseases") OR "Peripheral nervous system diseases") OR "Failed back surgery syndrome"[Mesh]) OR "Causalgia"[Mesh]) OR
830
21

"Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh])) AND (((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable pain”) OR "Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh]))) AND (((((((((((((("electric stimulation"[Mesh]) OR "electric stimulation therapy"[Mesh]) OR "implantable neurostimulators"[Mesh]) OR "spinal cord stimulation"[Mesh]) OR “pain stimulation”) OR “pain stimulator”) OR “electrical stimulation”) OR “Dorsal column stimulator”) OR “Spinal cord stimulator”) OR "Neurostimulator") OR “Dorsal column stimulation”) OR "Neuromodulation") OR "Neurostimulation") OR “Spinal cord stimulation”)
POPULATION OR INTERVENTION
((((((((((((((("electric stimulation"[Mesh]) OR "electric stimulation therapy"[Mesh]) OR "implantable neurostimulators"[Mesh]) OR "spinal cord stimulation"[Mesh]) OR “pain stimulation”) OR “pain stimulator”) OR “electrical stimulation”) OR “Dorsal column stimulator”) OR “Spinal cord stimulator”) OR "Neurostimulator") OR “Dorsal column stimulation”) OR "Neuromodulation") OR "Neurostimulation") OR “Spinal cord stimulation”)) OR ((((((((((((((((((((((((((("Causalgia") OR "Reflex sympathetic dystrophy") OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "peripheral vascular diseases") OR "Peripheral nervous system diseases") OR "Failed back surgery syndrome"[Mesh]) OR "Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh])) AND (((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable pain”) OR "Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh]))
221318
OUTCOME
“Return to work” 8113
Employment 109212
“Sick leave” 7334
“work activity” 666
“employment status” 7132
“Re-employment” 165
“professional situation” 89
“return-to-work” 8113
“back to work” 498
22

“back-to-work” 498
“disability leave” 41
“sick day” 102
“sick days” 335
“illness day” 40
“illness days” 57
“disability pension” 1121
“occupational disability” 268
“work disability” 1758
Incapacity 2764
Resume 6599
Reintegration 2641
Reinsertion 10339
professional 272333
“labour market” 1418
“labor market” 2082
Work 854476
Occupation 71922
Occupational 297058
(((((work) OR "labour market") OR “labor market”) OR occupation) OR occupational) OR professional)
1363359
(((reinsertion) OR reintegration) OR resume) OR incapacity 22247
((((((("labour market") OR work) OR occupational) OR occupation) OR professional) OR "labor market")) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity)
3246
(((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability") OR occupation
181732
(((((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability") OR occupation)) OR (((((((work) OR "labour market") OR occupation) OR
183898
23

occupational) OR professional)) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity))
((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability"
126726
((((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability")) OR (((((((work) OR "labour market") OR occupation) OR occupational) OR professional)) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity))
129050
((((((((("labour market") OR work) OR occupational) OR occupation) OR professional) OR "labor market")) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity))) OR ((((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability") OR occupation)
183900
((((((((("labour market") OR work) OR occupational) OR occupation) OR professional) OR "labor market")) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity))) OR (((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability")
129052
No “occupation” free
POPULATION OR INTERVENTION AND OUTCOME
((((((((((((((((("electric stimulation"[Mesh]) OR "electric stimulation therapy"[Mesh]) OR "implantable neurostimulators"[Mesh]) OR "spinal cord stimulation"[Mesh]) OR “pain stimulation”) OR “pain stimulator”) OR “electrical stimulation”) OR “Dorsal column stimulator”) OR “Spinal cord stimulator”) OR "Neurostimulator") OR “Dorsal column stimulation”) OR "Neuromodulation") OR "Neurostimulation") OR “Spinal cord stimulation”)) OR ((((((((((((((((((((((((((("Causalgia") OR "Reflex sympathetic dystrophy") OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "peripheral vascular diseases") OR "Peripheral nervous system diseases") OR "Failed back surgery syndrome"[Mesh]) OR "Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh])) AND (((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable
389
24

pain”) OR "Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh])))) AND (((((((((("labour market") OR work) OR occupational) OR occupation) OR professional) OR "labor market")) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity))) OR ((((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability") OR occupation))
POPULATION AND INTERVENTION AND OUTCOME
((((((((((((((((("electric stimulation"[Mesh]) OR "electric stimulation therapy"[Mesh]) OR "implantable neurostimulators"[Mesh]) OR "spinal cord stimulation"[Mesh]) OR “pain stimulation”) OR “pain stimulator”) OR “electrical stimulation”) OR “Dorsal column stimulator”) OR “Spinal cord stimulator”) OR "Neurostimulator") OR “Dorsal column stimulation”) OR "Neuromodulation") OR "Neurostimulation") OR “Spinal cord stimulation”)) AND ((((((((((((((((((((((((((("Causalgia") OR "Reflex sympathetic dystrophy") OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR “FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR “peripheral vascular disease”) OR "peripheral vascular diseases") OR "Peripheral nervous system diseases") OR "Failed back surgery syndrome"[Mesh]) OR "Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh])) AND (((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable pain”) OR "Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh])))) AND (((((((((("labour market") OR work) OR occupational) OR occupation) OR professional) OR "labor market")) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity))) OR ((((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR "employment status") OR "re-employment") OR "professional situation") OR "return-to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR "illness day") OR "illness days") OR "disability pension") OR "occupational disability") OR "work disability") OR occupation))
15
Bold: term used in the final systematic search with corresponding number of search results
25

Appendix C: Risk of bias assessment Reporting External validity Internal validity
Hyp
othe
sis
Mai
n ou
tcom
es
Patie
nt c
hara
cter
istic
s
Inte
rven
tions
Find
ings
Estim
ates
of
rand
om v
aria
bilit
y
Adve
rse
even
ts
Char
acte
ristic
s of
patie
nts L
TFU
Actu
al
prob
abili
ty v
alue
s
Repr
esen
tativ
enes
s of
pa
tient
s ask
ed
Repr
esen
tativ
enes
s of
in
clud
ed p
atie
nts
Repr
esen
tativ
enes
s of
tr
eatm
ent a
ccom
mod
atio
n
Data
dre
dgin
g
Appr
opria
tene
ss o
f st
atis
tics
Com
plia
nce
with
in
terv
entio
n
Out
com
e m
easu
res
va
lid/r
elia
ble
Loss
es o
f pat
ient
s
take
n in
to a
ccou
nt
Tota
l
North (1993) 1 1 1 1 1 0 1 1 1 0 0 0 1 1 1 1 1 13
Young (1978) 1 0 1 1 1 0 1 1 1 0 0 0 0 0 1 1 1 10
Kumar (2006) 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 14
Harke (2005) 1 1 1 1 1 1 1 1 1 1 0 0 0 1 1 1 1 14
Gopal (2016 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 14
Al-Kaisy (2017) 1 1 1 1 1 1 1 1 1 0 0 0 1 1 1 1 1 14
Kumar (2008) 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 16
North (1991) 1 1 1 1 1 1 1 1
1 1 0 0 1 1 1 1 1 15 Total 8 7 8 8 8 4 8 8 8 5 1 0 6 7 8 8 8 LTFU: loss to follow-up
26

North (1993)
Kumar (2008)
Gopal (2016)
North (1991)
Al-Kaisy (2017)Young (1978)
Kumar (2006)
Funnel plot: working status with SCS compared with before treatment
27

Funnel plot: return to work due to SCS compared with before treatment
Al-Kaisy (2017)Kumar (2008)
Young (1978)North (1991)
Gopal (2016)North (1993)
Kumar (2006)
28

01-May-2018 Dear Professor Moens: It is a pleasure to accept your manuscript entitled "Return to work of patients treated with spinal cord stimulation for chronic pain: a systematic review and meta-analysis" in its current form for publication in the Neuromodulation: Technology at the Neural Interface. Your article cannot be published until the publisher has received the appropriate signed license agreement. Once your article has been received by Wiley for production the corresponding author will receive an email from Wiley’s Author Services system which will ask them to log in and will present them with the appropriate license for completion. In addition, WIKISTIM.org is a searchable, free, collaborative website supported by the neuromodulation community. WIKISTIM lists publications that present primary data and provides datasheets for extrapolating SCS, DRG, DBS, PNS, and SNS data. Citations and completed datasheets can be downloaded to create evidence tables, answer clinical questions, and aid in reimbursement and payment decisions. We congratulate you on the acceptance of your paper and invite you to submit a companion completed data sheet to WIKISTIM. Links to the datasheets are provided below. We thank you for your fine contribution. On behalf of the Editors of the Neuromodulation: Technology at the Neural Interface, we look forward to your continued contributions to the Journal. Many thanks, Dr Robert Levy Editor in Chief, Neuromodulation: Technology at the Neural Interface [email protected] WIKISTIM DATASHEET LINKS: SCS: http://www.wikistim.org/wp-content/uploads/2015/05/SCS-datasheet-with-examples.csv DRG: http://www.wikistim.org/wp-content/uploads/2015/05/DRG-datasheet-with-examples.csv DBS: http://www.wikistim.org/wp-content/uploads/2015/05/DBS-datasheet-with-examples.csv PNS: http://www.wikistim.org/wp-content/uploads/2015/05/PNS-datasheet-with-examples-.csv SNS: http://www.wikistim.org/wp-content/uploads/2015/05/SNS-datasheet-with-examples.csv GES: http://www.wikistim.org/wp-content/uploads/2015/09/GES-datasheet-with-examples-.csv
29

For Peer Review
Return to work of patients treated with spinal cord
stimulation for chronic pain:
a systematic review and meta-analysis
Journal: Neuromodulation: Technology at the Neural Interface
Manuscript ID NER-2413-03-2018.R2
Manuscript Type: Review Article
Date Submitted by the Author: n/a
Complete List of Authors: Moens, Maarten; Universitair Ziekenhuis Brussel, Neurosurgery
Goudman, Lisa; Universitair Ziekenhuis Brussel, Neurosurgery Brouns, Raf Valenzuela Espinoza, Alexis; Vrije Universiteit Brussel Faculteit Geneeskunde en Farmacie, Department of Public Health (GEWE) De Jaeger, Mats Huysmans, Eva Putman, Koen; Vrije Universiteit Brussel Faculteit Geneeskunde en Farmacie, Department of Public Health (GEWE) Verlooy, Jan; Universiteit Antwerpen Faculteit geneeskunde en gezondheidswetenschappen, Department of Epidemiology and Social Medicine (ESOC)
Keywords: Spinal Cord Stimulation, return to work, Review article, Meta-analysis,
Chronic Pain
Neuromodulation Proof
Neuromodulation Proof
30

For Peer Review
Return to work of patients treated with spinal cord stimulation for chronic pain:
a systematic review and meta-analysis
Maarten Moens MD, PhD1,2,3,4
; Lisa Goudman MSC1,4
; Raf Brouns MD, PhD5,6
; Alexis
Valenzuela Espinoza7; Mats De Jaeger MSC
1 ; Eva Huysmans MSC
7,8; Koen Putman PhD
7; Jan
Verlooy MD, PhD9
1Department of Neurosurgery, UZ Brussel, Brussels, Belgium
2Department of Radiology, UZ Brussel, Brussels, Belgium
3Center for Neurosciences (C4N), Vrije Universiteit Brussel, Belgium
4Department of Manual Therapy (MANU), Vrije Universiteit Brussel, Brussels, Belgium
5Department of Neurology, ZorgSaam Hospital, Terneuzen, The Netherlands
6Faculty of Medicine and Pharmacy, Vrije Unversiteit Brussel, Belgium
7Department of Public Health (GEWE), Faculty of Medicine and Pharmacy, Vrije Universiteit
Brussel, Brussels, Belgium
8Department of Physiotherapy, Human Physiology and Anatomy, Faculty of Physical
Education & Physiotherapy (KIMA), Vrije Universiteit Brussel, Brussels, Belgium
9Department of Epidemiology and Social Medicine (ESOC), Universiteit Antwerpen,
Antwerpen, Belgium
Abstract
Background
Chronic pain has a substantial negative impact on work-related outcomes, which
underscores the importance of interventions to reduce the burden. Spinal cord stimulation
(SCS) efficiently causes pain relief in specific chronic pain syndromes. The aim of this review
was to identify and summarize evidence on returning to work in patients with chronic pain
treated with SCS.
Methods
A systematic literature review was performed including studies from PubMed, EMBASE,
SCOPUS, and Web of Science (up till October 2017). Risk of bias was assessed using a
modified version of the Downs & Black checklist. Where possible, we pooled data using
random-effects meta-analysis. The study protocol was registered prior to initiation of the
review process (PROSPERO CRD42017077803).
Results
Fifteen full-text articles (total articles screened: 2,835) were included. Risk of bias for these
articles was scored low. Seven trials provided sufficient data and were judged similar
enough to be pooled for meta-analysis on binary outcomes. SCS intervention results in a
higher prevalence of patients at work compared with before treatment (OR 2,15; 95% CI,
1,44 to 3,21; I2
= 42%; p < 0,001). SCS treatment results also in high odds to return to work
(OR 29,06; 95% CI, 9,73 to 86,75; I2
= 0%; p < 0,001).
Conclusions
Based on available literature, SCS proved to be an effective approach to stimulate return to
work in patients with specific chronic pain syndromes.
Page 1 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 31

For Peer Review
Background
Spinal cord stimulation (SCS) is a well-known safe and effective treatment for many chronic
pain syndromes, including failed back surgery syndrome (FBSS), low back and lower
extremity pain, complex regional pain syndrome, and other neuropathic conditions(1-4).
Despite the extreme complexity of chronic pain, pain relief is the principal desired outcome
for SCS(1). The high socioeconomic burden and healthcare utilization associated with
chronic pain are therefore often reduced to secondary outcomes (5-7). When pain becomes
chronic, return to work (RTW) is negatively associated with a delay in referral to treatment,
socioeconomic status, attorney involvement, and worker’s compensation are(8). Several
studies have shown that unemployment and absenteeism are “negatively associated with
quality of life, depression and generally poor health outcomes”(9-11).
Currently, it is well accepted that SCS is an effective treatment for reducing pain and
improving quality of life, but little is known about the impact of SCS on occupational
outcome parameters such as RTW. Therefore, we conducted a systematic review and meta-
analysis to identify not only the prevalence of RTW by SCS in patients with chronic pain but
also the odds of working with SCS.
Methods
Search strategy and selection criteria
This systematic review and meta-analysis were conducted in accordance with the PRISMA
(Preferred Reporting Items for Systematic Review and Meta-Analyses) guidance(12). The
electronic databases of PubMed, Embase, SCOPUS, and Web of Science were searched from
inception to October 20th
, 2017 to identify potentially relevant studies.
The search strategy was, based on the PICO (evidence based search strategy focusing on
Patient/Population, Intervention, Comparison and Outcome) Framework (13). Our search
was not limited to randomized controlled trials (RCTs) but also included case series. A
Page 2 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 32

For Peer Review
language restriction of English, French, German, and Dutch was applied. We included
studies that met the following criteria: (1) population – adult (≥18 years old) chronic pain
patients eligible for SCS; (2) intervention – SCS; (3) outcome – RTW, employment status and
sick leave. We excluded studies enrolling patients receiving other types of neuromodulation
and publications available only in abstract form or meeting reports.
Data extraction and quality assessment
After combining search results from different databases and removing duplicates by using
EndNote reference manager, two investigators (MM and LG) independently reviewed all the
retrieved abstracts and full texts to remove ineligible studies. In case of disagreement,
consensus was sought through consultation and discussion with a third party (RB). The two
reviewers (MM and LG) independently extracted data from included studies, using an a
priori determined data extraction form comprising the following items (1) first author (2)
year of publication, (3) country, (4) sample size in relation to RTW outcome, (5) study
design, (6) diagnosed population, (7) type of SCS and (8) all predefined outcomes. The
quality of the included studies was evaluated using the risk of bias Downs and Black
checklist (modified version) (14). We assigned a value of 0 or 1 to the different
subcategories of the following items: reporting, external validity and internal validity. A total
score < 10/16 was considered to be low quality, while scores ≥ 10/16 were presumed to be
high quality. Discrepancies were identified and resolved through discussion.
Outcome and statistical analysis
The primary goal of this study was to identify the prevalence of work resumption after
implantation of SCS. Subgroup analyses were performed to evaluate the occupational status
at last follow-up point. The results from all relevant studies were merged to estimate the
pooled odds ratio (OR) and associated 95% confidence intervals (CI’s) for dichotomous
outcomes. The outcomes were pooled using a random effects model. All p< 0,05 were
considered statistically significant. Heterogeneity was tested with I2
statistics. This statistic
can be interpreted as the proportion of the total variation in the estimated treatment effect
due to the heterogeneity among studies(15). To explore the robustness and the potential
Page 3 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 33

For Peer Review
influence of various factors on our primary outcome, we performed a subgroup analysis
based on pathology (back and leg pain versus mixed). The Dixon’s Q test for the rejection of
extreme values (at the 5 and 1% levels) was performed to identify outliers(16). Publication
bias was evaluated by visual inspection of the funnel plot. All statistical analyses were
performed using RStudio (version 0.99.903, RStudio, Inc).
Results
Study selection
A flowchart of the search strategy and the reasons for exclusion are shown in figure 1. The
initial search identified a total of 2,835 citations. After combining the results, removing
duplicates and selections based on the title and abstract, 54 full-text studies remained.
Thirty-nine studies were excluded after reviewing the full text: 10 because of inappropriate
outcome parameters (no RTW mentioned), 28 were excluded because of unsuitable study
design or conference meeting abstract and, one because no full text was available even
after communication with the first author. Thus, 15 full-text studies were read for further
evaluation. Of those 15 studies, 6 were excluded because they did not provide sufficient
information on the occupational status at last follow-up point(17-22), 1 was excluded
because the studied population was reported in another study(23, 24), and 1 study did not
pass the outlier test(25). This study from Harke et al. was considered an outlier at the level 5
and at the 1%(25). Finally, the remaining seven, which enrolled 824 patients, were included
in the meta-analysis(23, 26-31).
Study characteristics and quality
The main characteristics and predefined outcome data of the included studies for the
systematic review are described in table 1. These studies were published between 1978 and
2017, with sample sizes ranging from 20 to 410. One RCT was included, five retrospective
case series and one prospective cohort study. One study evaluated high-frequency SCS,
while the other studies reported on the use of conventional SCS (29). The mean follow-up
period varied from 1 year to 7.1 years. Three studies were included with a study population
Page 4 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 34

For Peer Review
suffering from back and/or leg pain (FBSS with axial back pain and unilateral limb pain),
while four other studies described a more heterogeneous study population (i.e., FBSS,
multiple sclerosis, spinal cord injury, vascular disease, cancer, occipital neuralgia, trauma,
and peripheral neuropathy). The risk of bias Downs and Black checklist score for each
citation varied across the studies, ranging from 10 to 16 out of 17.
Primary Outcome
Occupational status
The number of patients working after SCS was mentioned in all seven studies. The pooled
analysis showed that SCS increases the odds to work after SCS (7 studies; n = 824, OR 2,15;
95% CI, 1,44 to 3,21; I2
= 42%; p = 0,0001). Given the moderate heterogeneity, a subgroup
based on the type of population was also evaluated. The type of population (chronic back
and/or leg pain versus mixed pain syndromes) was defined to be a factor influencing
heterogeneity (figure 2).
In general, both subgroups analyses confirmed similar OR of working status among groups.
The funnel plot shows no publication bias (available upon request).
Return to work
%RTW, defined as the percentage of patients going back to work who were unemployed
before treatment, was reported or could be calculated in all seven studies. The %RTW
varied between 10 and 47 (mean 14). The pooled analysis showed that SCS increases the
odds to return to work after SCS in patients with absenteeism before treatment (7 studies;
n = 701, OR 29,06; 95% CI, 9,73 to 86,75; I2
= 0%; p < 0,0001). The funnel plot shows no
publication bias (available upon request).
Secondary outcomes
The types of employment after returning to work were not reported in all seven studies.
Three studies described the number of patients with part-time and full-time employment
after SCS implantation at the last follow-up(29, 30, 32). Two studies also mentioned the
numbers of patients who increased working time after SCS implantation(26, 30). One study
Page 5 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 35

For Peer Review
presented the percentage of patients with SCS working at various follow-up points(31). Yet
another study reported the median time of unemployment(28).
Discussion
In the past two decades, SCS for pain relief has evolved to include many new methods of
current delivery by neurostimulation devices(3). This resulted in several studies presenting
excellent results on pain reduction. Although the status of “remission,” or achieving almost
complete pain relief by SCS, for some patients has been reported, occupational outcomes,
such as RTW, are rarely an outcome parameter in neuromodulation studies(33). SCS has
shown superior efficacy to conventional medical management in an FBSS population and
SCS leads to long-term health care cost savings(28, 34). These data support the long-term
cost utility of SCS in the treatment of FBSS patients(34). However, in a chronic pain
population, it is well known that two thirds of the total health care costs are represented by
indirect costs (loss of productivity or working days lost)(35).
Our epidemiological meta-analysis included seven studies with 824 patients investigated
occupational outcomes. Despite the clinical heterogeneity of the subgroup “chronic back
and leg pain”, the results for this subgroup appeared to be statistically homogenous and this
in contrast to the subgroup with mixed diagnoses. This can be explained by the fact that the
mixed group consists of various diagnoses with variable evidence for SCS, while SCS for
chronic low back pain has proven to be effective and has reached a recommendation in the
recent European Academy of Neurology (EAN) guidelines(36).
This meta-analysis showed that, among chronic pain patients, SCS improves the odds of
returning to work and that SCS results in more patients at work, compared with the same
population before SCS.
In terms of %RTW, the percentage of patients going back to work who were unemployed
before treatment, SCS seems to allow chronic pain patients to work again. Since SCS
candidates are refractory to conventional pain therapy and therefore difficult to treat, a
mean of 14% of unemployed patients returning to work should be born in mind. However,
no information is available in these studies on the type of work the patients are returning
to. Although three studies reported the number of patients returning to work on a part-time
basis, the relevant number of hours worked daily was not mentioned(24, 26, 30). Young et
al. considered returning to household duties or to studying as returning to gainful
Page 6 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 36

For Peer Review
employment(31). It is generally accepted that patients at working age or defined as patients
under the age of 65 are more likely to return to work. This specific subdivision of patients
receiving SCS was reported only in a minority of the reviewed studies(28-30).
The number of patients found in this meta-analysis is similar to the findings of the
systematic review of Frey et al. in 2009(37). They summarized a 13% entry in gainful
employment and return to work in 16 to 31% of FBSS patients(37).
Researchers agree that both job loss and continuing “worklessness” impact adversely on
people’s health with increased levels of both mental and physical problems(38).
Notwithstanding the evidence of using classical pain relief, functionality, and quality of life
as outcome measurements in chronic pain studies, RTW as a central determinant of
(mental) health, should also be considered as an important clinical outcome measure.
Additionally, Elfering et al. reported that only measuring global work status and %RTW as
work-related outcome parameters, lack specificity(39). In-depth and detailed analyses, clear
definitions, disjunctive classes of categories and adequate time frames might upgrade this
specificity. Job description and educational level, type of employment (full time, part time or
casual), reasons for unemployment, work-related attitudes (e.g. job satisfaction, work-
related expectations, ...) and other risk factors for chronic disability may also be taken in
consideration(39, 40).
Strengths and limitations
To diminish bias, the study selection, data extraction, and evaluation of study quality were
performed by two independent reviewers. We comprehensively analyzed the odds of
working and the odds of RTW after SCS treatment in studies with different designs.
There were also several potential limitations regarding our meta-analysis. First, some well-
designed studies were excluded because they lacked essential information about the work
status of all patients. Second, the sample size was small as only seven studies were included.
Third, the bias of the publications might have affected the validity of our conclusions, such
as lack of comparison (e.g. best medical treatment, other types of therapies, …). And finally,
the search method was limited to Medline, Embase, Web of Science and Scopus. We did not
search the “grey literature” (trial registries nor backward references).
Page 7 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 37

For Peer Review
Conclusion
In summary, based on available data, this meta-analysis demonstrates that SCS treatment
results in more patients at work and also more patients returning to work. More, large-scale
studies are warranted to analyze in detail the work status of the included patients (type of
job, full time, part-time, % patients at working age, etc).
References
1. Sitzman BT, Provenzano DA. Best Practices in Spinal Cord Stimulation. Spine (Phila Pa
1976) 2017;42 Suppl 14:S67-S71.
2. Deer TR, Mekhail N, Provenzano D, Pope J, Krames E, Leong M, et al. The appropriate
use of neurostimulation of the spinal cord and peripheral nervous system for the treatment
of chronic pain and ischemic diseases: the Neuromodulation Appropriateness Consensus
Committee. Neuromodulation 2014;17:515-50; discussion 50.
3. Deer TR, Krames E, Mekhail N, Pope J, Leong M, Stanton-Hicks M, et al. The
appropriate use of neurostimulation: new and evolving neurostimulation therapies and
applicable treatment for chronic pain and selected disease states. Neuromodulation
Appropriateness Consensus Committee. Neuromodulation 2014;17:599-615; discussion
4. Eldabe S, Buchser E, Duarte RV. Complications of Spinal Cord Stimulation and
Peripheral Nerve Stimulation Techniques: A Review of the Literature. Pain Med
2016;17:325-36.
5. Mann EG, Johnson A, VanDenKerkhof EG. Frequency and characteristics of
healthcare visits associated with chronic pain: results from a population-based Canadian
study. Can J Anaesth 2016;63:411-41.
6. Breivik H, Eisenberg E, O'Brien T, Openminds. The individual and societal burden of
chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge
and availability of appropriate care. BMC Public Health 2013;13:1229.
7. Duenas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on
patients, their social environment and the health care system. J Pain Res 2016;9:457-67.
8. Steenstra IA, Munhall C, Irvin E, Oranye N, Passmore S, Van Eerd D, et al. Systematic
Review of Prognostic Factors for Return to Work in Workers with Sub Acute and Chronic
Low Back Pain. J Occup Rehabil 2017;27:369-81.
9. Mathers CD, Schofield DJ. The health consequences of unemployment: the evidence.
Med J Aust 1998;168:178-82.
10. Martella D. MA. Unemployment and life satisfaction: the moderating role of time
structure and collectivism. J Appl Soc Psychology 2000;30:1095-108.
11. Gallie D. RH. Unemployment and life satisfaction: a cross cultural comparison. Eur J
Sociology 1998;39:248-80.
12. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for
systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8:336-41.
13. O'Sullivan D, Wilk S, Michalowski W, Farion K. Using PICO to align medical evidence
with MDs decision making models. Stud Health Technol Inform 2013;192:1057.
Page 8 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 38

For Peer Review
14. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the
methodological quality both of randomised and non-randomised studies of health care
interventions. J Epidemiol Community Health 1998;52:377-84.
15. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statistics in
medicine 2002;21:1539-58.
16. Dixon WJ. Analysis of extreme values. Ann Math Stat 1950;21:488-506.
17. Devulder J, De Laat M, Van Bastelaere M, Rolly G. Spinal cord stimulation: a valuable
treatment for chronic failed back surgery patients. J Pain Symptom Manage 1997;13:296-
301.
18. Hamm-Faber TE, Aukes HA, de Loos F, Gultuna I. Subcutaneous stimulation as an
additional therapy to spinal cord stimulation for the treatment of lower limb pain and/or
back pain: a feasibility study. Neuromodulation 2012;15:108-16; discussion 16-7.
19. Kupers RC, Van den Oever R, Van Houdenhove B, Vanmechelen W, Hepp B, Nuttin B,
et al. Spinal cord stimulation in Belgium: a nation-wide survey on the incidence, indications
and therapeutic efficacy by the health insurer. Pain 1994;56:211-6.
20. Sundaraj SR, Johnstone C, Noore F, Wynn P, Castro M. Spinal cord stimulation: a
seven-year audit. J Clin Neurosci 2005;12:264-70.
21. North RB, Kidd DH, Petrucci L, Dorsi MJ. Spinal cord stimulation electrode design: a
prospective, randomized, controlled trial comparing percutaneous with laminectomy
electrodes: part II-clinical outcomes. Neurosurgery 2005;57:990-6; discussion -6.
22. Kumar A, Felderhof C, Eljamel MS. Spinal cord stimulation for the treatment of
refractory unilateral limb pain syndromes. Stereotact Funct Neurosurg 2003;81:70-4.
23. North RB, Ewend MG, Lawton MT, Kidd DH, Piantadosi S. Failed back surgery
syndrome: 5-year follow-up after spinal cord stimulator implantation. Neurosurgery
1991;28:692-9.
24. North RB, Ewend MG, Lawton MT, Piantadosi S. Spinal cord stimulation for chronic,
intractable pain: superiority of "multi-channel" devices. Pain 1991;44:119-30.
25. Harke H, Gretenkort P, Ladleif HU, Rahman S. Spinal cord stimulation in
sympathetically maintained complex regional pain syndrome type I with severe disability. A
prospective clinical study. Eur J Pain 2005;9:363-73.
26. Kumar K, Hunter G, Demeria D. Spinal cord stimulation in treatment of chronic
benign pain: challenges in treatment planning and present status, a 22-year experience.
Neurosurgery 2006;58:481-96; discussion -96.
27. Gopal H, Fitzgerald J, McCrory C. Spinal cord stimulation for FBSS and CRPS: A review
of 80 cases with on-table trial of stimulation. J Back Musculoskelet Rehabil 2016;29:7-13.
28. Kumar K, Taylor RS, Jacques L, Eldabe S, Meglio M, Molet J, et al. The effects of spinal
cord stimulation in neuropathic pain are sustained: a 24-month follow-up of the prospective
randomized controlled multicenter trial of the effectiveness of spinal cord stimulation.
Neurosurgery 2008;63:762-70; discussion 70.
29. Al-Kaisy A, Palmisani S, Smith TE, Pang D, Lam K, Burgoyne W, et al. 10 kHz High-
Frequency Spinal Cord Stimulation for Chronic Axial Low Back Pain in Patients With No
History of Spinal Surgery: A Preliminary, Prospective, Open Label and Proof-of-Concept
Study. Neuromodulation 2017;20:63-70.
30. North RB, Kidd DH, Zahurak M, James CS, Long DM. Spinal cord stimulation for
chronic, intractable pain: experience over two decades. Neurosurgery 1993;32:384-94;
discussion 94-5.
Page 9 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 39

For Peer Review
31. Young RF. Evaluation of dorsal column stimulation in the treatment of chronic pain.
Neurosurgery 1978;3:373-9.
32. North RB, Campbell JN, James CS, Conover-Walker MK, Wang H, Piantadosi S, et al.
Failed back surgery syndrome: 5-year follow-up in 102 patients undergoing repeated
operation. Neurosurgery 1991;28:685-90; discussion 90-1.
33. Khan H, Pilitsis JG, Prusik J, Smith H, McCallum SE. Pain Remission at One-Year
Follow-Up With Spinal Cord Stimulation. Neuromodulation 2018;21:101-5.
34. Lad S, Petrella J, Xie J, Parente B, Pagadala P, Yang S, et al. Long-term Cost Utility of
Spinal Cord Stimulation in Patients with Failed Back Surgery Syndrome. Pain Physician
2017;20:E797-E805.
35. Lardon A, Dubois JD, Cantin V, Piche M, Descarreaux M. Predictors of disability and
absenteeism in workers with non-specific low back pain: A longitudinal 15-month study.
Appl Ergon 2018;68:176-85.
36. Cruccu G, Garcia-Larrea L, Hansson P, Keindl M, Lefaucheur JP, Paulus W, et al. EAN
guidelines on central neurostimulation therapy in chronic pain conditions. Eur J Neurol
2016;23:1489-99.
37. Frey ME, Manchikanti L, Benyamin RM, Schultz DM, Smith HS, Cohen SP. Spinal cord
stimulation for patients with failed back surgery syndrome: a systematic review. Pain
Physician 2009;12:379-97.
38. Litchfield P, Cooper C, Hancock C, Watt P. Work and Wellbeing in the 21st Century
dagger. Int J Environ Res Public Health 2016;13.
39. Elfering A. Work-related outcome assessment instruments. Eur Spine J 2006;15 Suppl
1:S32-43.
40. Cancelliere C, Donovan J, Stochkendahl MJ, Biscardi M, Ammendolia C, Myburgh C,
et al. Factors affecting return to work after injury or illness: best evidence synthesis of
systematic reviews. Chiropr Man Therap 2016;24:32.
Page 10 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 40

For Peer Review
North (1993) US RCS 171 92 Mixed C - mean 7,1 y
Young (1978) US RCS 51 19 Mixed C - 3 m, 6 m, 1 y, 2 y, 3 y, 4y, 5y
Kumar (2006) CA RCS 410 158 Mixed C - mean 97,6 m
Gopal (2016) IE RCS 80 33 Mixed C - 1 m, 12m
Al-Kaisy (2017) GB PCS 20 9 CLBP HF10 - 1y
Kumar (2008) CA RCT 42 17 FBSS C median unemployment: 2,76 y1 m, 3 m, 6 m, 9 m, 12 m, 18 m, 24 m
North (1991) US RCS 50 23 FBSS C - 5y
Study (Year) Study DesignC N Female P Type SCS Mean postop sick leave duration Follow-up intervals
Page 11 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
41

For Peer Review
% RTW (No of patients) PT/FT Working at baseline Working after SCS
15% (24/157) 5/19 64 74
17% (8/48) - 3 11
10% (39/391) - 19 58
47% (8/17) - 63 71
27% (4/15) 2/2 11 15
15% (5/33) - 9 11
25% (10/40) 4/6 10 20
outcome
Page 12 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
42

For Peer Review
Figure 1: Flow chart of study selection in meta-analysis of occupational outcome after SCS treatment
179x213mm (300 x 300 DPI)
Page 13 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 43

For Peer Review
Pre-SCSSCSTotalTotal WorkingWorking
Page 14 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
44

For Peer Review
Figure legend
Table 1
Characteristics of included studies.
Abbreviations:
RTW: return to work; mo: months; y: year(s); CLBP: chronic low back pain; FBSS: failed back
surgery syndrome; PT/FT: part time/full time; SCS: spinal cord stimulation
Explanation:
Country (C): presented in ISO3166-1 alpha-2 codes (US: United States of America; GB: Great
Britain; CA: Canada; IE: Ireland)
Study Type: RCT: randomized controlled trial; retro case series: retrospective case series;
prosp cohort study: prospective cohort study
N: total sample size for return to work analysis
Population: type of population eligible to SCS: Mixed: a mixed group of patients with
different diagnoses; CLBP: chronic low back pain patients; FBSS: patients with failed back
surgery syndrome
Mean postoperative sick leave duration: Presents the median time of unemployment before
SCS treatment
Follow-up points: either a fixed follow-up moment, or a mean of follow-up.
%RTW (No of patients): X% of the patients has returned to work
PT/FT: number of patients returned to work (part-time / full-time)
Working at baseline: number of patients at work at baseline
Working after SCS: number of patients at work after SCS at the latest follow-up point
Figure 1: Flow chart of study selection in meta-analysis of occupational outcome after SCS
treatment
Figure 2: Forest plot of working status with SCS compared with before treatment
Page 15 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 45

For Peer Review
Appendix A: PICO
Free terms MeSH-terms
Population “Chronic pain patients”;
“chronic pain”;
“persistent pain”
“intractable pain”;
AND
"Causalgia";
"Reflex sympathetic dystrophy";
“failed back surgery syndrome”;
“post laminectomy syndrome”;
“postlaminectomy syndrome”;
“failed neck surgery syndrome”;
“CRPS”;
“complex regional pain syndrome”;
“complex regional pain syndromes”;
“FBSS”;
“FNSS”;
“peripheral neuropathy”;
“neuropathic pain”;
“angina pectoris”;
“peripheral vascular disease”;
"peripheral vascular diseases";
"Peripheral nervous system diseases"
Chronic pain;
Pain, Intractable;
AND
Failed back surgery
syndrome;
Causalgia;
Complex regional pain
syndromes;
Reflex sympathetic
dystrophy;
peripheral nervous
system diseases;
neuropathic pain;
angina pectoris;
peripheral vascular
diseases;
Intervention “Spinal cord stimulation”;
"Neurostimulation";
"Neuromodulation";
“Dorsal column stimulation”;
"Neurostimulator";
“Spinal cord stimulator”;
“Dorsal column stimulator”;
“electrical stimulation”;
“pain stimulator”;
“pain stimulation”;
spinal cord stimulation;
Implantable
neurostimulators;
Electric stimulation
therapy;
Electric stimulation;
Control / /
Outcome “occupation”;
“re-employment”;
“professional situation”;
“return-to-work”;
“back to work”;
“back-to-work”;
“work activity”;
“employment status”;
Return to work;
Employment;
Sick leave
Page 16 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 46

For Peer Review
Resume;
Reintegration;
Reinsertion;
Incapacity
AND
Work;
“labour market”;
“labor market”;
Professional;
Occupation;
occupational
“disability leave”;
“Sick day”;
“sick days”;
“illness day”;
“illness days”;
“disability pension”;
“occupational disability”;
“work disability”
Page 17 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 47

For Peer Review
Appendix B: Final systematic literature search for PubMed
SEARCH 20/10/2017 PubMed
((((((((((((((((("electric stimulation"[Mesh]) OR "electric stimulation therapy"[Mesh]) OR
"implantable neurostimulators"[Mesh]) OR "spinal cord stimulation"[Mesh]) OR “pain
stimulation”) OR “pain stimulator”) OR “electrical stimulation”) OR “Dorsal column
stimulator”) OR “Spinal cord stimulator”) OR "Neurostimulator") OR “Dorsal column
stimulation”) OR "Neuromodulation") OR "Neurostimulation") OR “Spinal cord
stimulation”)) OR ((((((((((((((((((((((((((("Causalgia") OR "Reflex sympathetic dystrophy")
OR “failed back surgery syndrome”) OR “post laminectomy syndrome”) OR “failed neck
surgery syndrome”) OR “postlaminectomy syndrome”) OR “CRPS”) OR “complex
regional pain syndrome”) OR “complex regional pain syndromes") OR “FBSS”) OR
“FNSS”) OR “peripheral neuropathy”) OR “neuropathic pain”) OR “angina pectoris”) OR
“peripheral vascular disease”) OR "peripheral vascular diseases") OR "Peripheral
nervous system diseases") OR "Failed back surgery syndrome"[Mesh]) OR
"Causalgia"[Mesh]) OR "Complex regional pain syndromes"[Mesh]) OR "Reflex
sympathetic dystrophy"[Mesh]) OR "peripheral nervous system diseases"[Mesh]) OR
neuralgia) OR "angina pectoris"[Mesh]) OR "peripheral vascular diseases"[Mesh])) AND
(((((("Chronic pain patients") OR “chronic pain”) OR “persistent pain”) OR “intractable
pain”) OR "Chronic Pain"[Mesh]) OR "Pain, Intractable"[Mesh])))) AND (((((((((("labour
market") OR work) OR occupational) OR occupation) OR professional) OR "labor
market")) AND ((((reinsertion) OR reintegration) OR resume) OR incapacity))) OR
((((((((((((((((((return to work) OR employment) OR sick leave) OR "work activity") OR
"employment status") OR "re-employment") OR "professional situation") OR "return-
to-work") OR "back to work") OR "disability leave") OR "sick day") OR "sick days") OR
"illness day") OR "illness days") OR "disability pension") OR "occupational disability")
OR "work disability") OR occupation))
389
Page 18 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 48

For Peer Review
Appendix C: Risk of bias assessment
Reporting External validity Internal validity
Hy
po
the
sis
Ma
in o
utc
om
es
Pa
tie
nt
cha
ract
eri
stic
s
Inte
rve
nti
on
s
Fin
din
gs
Est
ima
tes
of
ran
do
m v
ari
ab
ility
Ad
vers
e e
ven
ts
Ch
ara
cte
rist
ics
of
pa
tie
nts
LT
FU
Act
ua
l
pro
ba
bili
ty v
alu
es
Re
pre
sen
tati
ven
ess
of
pa
tie
nts
ask
ed
Re
pre
sen
tati
ven
ess
of
incl
ud
ed
pa
tie
nts
Re
pre
sen
tati
ven
ess
of
tre
atm
en
t a
cco
mm
od
ati
on
Da
ta d
red
gin
g
Ap
pro
pri
ate
ne
ss o
f
sta
tist
ics
Co
mp
lian
ce w
ith
inte
rve
nti
on
Ou
tco
me
me
asu
res
valid
/re
liab
le
Los s
es
of
pa
tie
nts
tak
en
into
acc
ou
nt
To
tal
North (1993) 1 1 1 1 1 0 1 1 1 0 0 0 1 1 1 1 1 13
Young (1978) 1 0 1 1 1 0 1 1 1 0 0 0 0 0 1 1 1 10
Kumar (2006) 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 14
Harke (2005) 1 1 1 1 1 1 1 1 1 1 0 0 0 1 1 1 1 14
Gopal (2016 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 14
Al-Kaisy (2017) 1 1 1 1 1 1 1 1 1 0 0 0 1 1 1 1 1 14
Kumar (2008) 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 16
North (1991) 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 15
Total 8 7 8 8 8 4 8 8 8 5 1 0 6 7 8 8 8
LTFU: loss to follow-
up
Page 19 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 49

For Peer Review
Hy
po
the
sis
Ma
in o
utc
om
es
Pa
tie
nt
cha
ract
eri
stic
s
Inte
rve
nti
on
s
Fin
din
gs
Est
ima
tes
of
ran
do
m v
ari
ab
ility
Ad
vers
e e
ven
ts
Ch
ara
cte
rist
ics
of
pa
tie
nts
LT
FU
Act
ua
l
pro
ba
bili
ty v
alu
es
Re
pre
sen
tati
ven
ess
of
pa
tie
nts
ask
ed
Re
pre
sen
tati
ven
ess
of
incl
ud
ed
pa
tie
nts
Re
pre
sen
tati
ven
ess
of
tre
atm
en
t a
cco
mm
od
ati
on
Da
ta d
red
gin
g
Ap
pro
pri
ate
ne
ss o
f
sta
tist
ics
Co
mp
lia
nce
wit
h
inte
rve
nti
on
Ou
tco
me
me
asu
res
valid
/re
lia
ble
Loss
es
of
pa
tie
nts
tak
en
into
acc
ou
nt
To
tal
Devulder (1997) 1 1 1 1 1 0 1 0 1 0 0 0 1 1 1 1 1 12
Hamm-Faber (2012) 1 1 1 1 1 1 1 1 1 0 0 0 1 0 1 1 1 13
Kumar (2003) 1 1 0 1 1 0 1 0 0 0 0 0 0 0 1 1 0 7
Kupers (1994) 1 0 1 1 0 0 1 0 0 0 0 0 0 0 1 0 0 5/6
North (1991) fbss 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 15
North (1993) 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 14
Young (1978) 1 0 1 1 1 0 1 1 1 0 0 0 0 0 1 1 1 10
North (2005) 1 1 1 1 1 1 1 1 0 1 0 0 0 1 1 1 1 13
Kumar (2006) 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 14
Harke (2005) 1 1 1 1 1 1 1 1 1 0 0 0 1 1 1 1 1 14
Gopal (2016 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 14
Al-Kaisy (2016) 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 15
Kumar (2008) 1 1 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 15
Sundaraj (2005)
0 1 1 1 1 0 1 1 0 1 0 0 1 1 1 1 1 12
North (1991) scs 1 1 0 1 0 0 1 1 1 1 0 0 1 1 1 1 1 12
Total 14 13 15 15 14 6 15 12 11 7 1 0 11 12 13 13 13
* 9: 1 if correct reported + if not reported due to no testing (shoud be indicated as NA).
Page 20 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960 50

For Peer Review
North (1993)
Kumar (2008)
Gopal (2016)
North (1991)
Al-Kaisy (2017)Young (1978)
Kumar (2006)
Funnel plot: working status with SCS compared with before treatmentPage 21 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
51

For Peer Review
Funnel plot: return to work due to SCS compared with before treatment
Al-Kaisy (2017)Kumar (2008)
Young (1978)North (1991)
Gopal (2016)North (1993)
Kumar (2006)
Page 22 of 22
Neuromodulation Proof
Neuromodulation Proof
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
52