-
7/28/2019 RINITIS ATROFICA 4
1/12
doi: 10.1152/japplphysiol.01118.2006103:1082-1092, 2007. First
published 14 June 2007;J Appl Physiol
Guilherme J. M. Garcia, Neil Bailie, Drio A. Martins and Julia
S. Kimbellnasal cavityAtrophic rhinitis: a CFD study of air
conditioning in the
You might find this additional info useful...
46 articles, 7 of which you can access for free at:This article
citeshttp://jap.physiology.org/content/103/3/1082.full#ref-list-1
5 other HighWire-hosted articles:This article has been cited
byhttp://jap.physiology.org/content/103/3/1082#cited-by
including high resolution figures, can be found at:Updated
information and
serviceshttp://jap.physiology.org/content/103/3/1082.full
can be found at:Journal of Applied PhysiologyaboutAdditional
material and
informationhttp://www.the-aps.org/publications/jappl
This information is current as of July 3, 2013.
http://www.the-aps.org/.
2007 the American Physiological Society. ISSN: 8750-7587, ESSN:
1522-1601. Visit our website atyear (monthly) by the American
Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991.
Copyrightphysiology, especially those papers emphasizing adaptive
and integrative mechanisms. It is published 12 times a
publishes original papers that deal with diverse area of
research in appliedJournal of Applied Physiology
http://jap.physiology.org/content/103/3/1082#cited-byhttp://jap.physiology.org/content/103/3/1082#cited-byhttp://jap.physiology.org/content/103/3/1082#cited-byhttp://jap.physiology.org/content/103/3/1082#cited-byhttp://jap.physiology.org/content/103/3/1082#cited-by
-
7/28/2019 RINITIS ATROFICA 4
2/12
-
7/28/2019 RINITIS ATROFICA 4
3/12
A body of indirect evidence in the literature supports
thisargument. First, genuine AR has never been observed in anarrow
nose (49), which is consistent with abnormal flowpatterns playing a
role in the pathophysiology of the disease.Second, Girgis (18)
demonstrated that if a patient with ARblocks his nostrils with
pieces of cotton for 24 h, the nasalmucosa will present an entirely
different picture on removal of
the plugs; it becomes moist and less pale, and the crustsbecome
loosened. Third, crusts are never observed in theparanasal sinuses,
where the drying effect of airflow is lessvigorous than in the
nasal cavity (49). Finally, Dutt andKameswarans observation (11)
that primary AR seems to havea high prevalence in the arid regions
bordering the great desertsof Saudi Arabia suggests that low
absolute humidity of the airmay trigger AR in susceptible
populations.
Further evidence is provided by cases of unilateral ARrelated to
a septal deviation. It has been observed that theair-humidifying
capacity of the nose is time dependent becausewhen a continuous air
stream is drawn through the nose, airbecomes progressively cooler
and drier at the outlet (8). There-fore, we suggest that unilateral
AR associated with septaldeviation may be explained as follows: if
the cavity on theconcave side of the septum is too large, air will
flow mostlythrough this patent side, subjecting it to a permanent
water andtemperature gradient. If the water gradient is
sufficiently largeor the mucosa unhealthy, the mucous layer may dry
in regionsof high water flux, leading to crust formation and
predisposingto infection. Because of the lack of a cyclic closure
of theaffected side, the continuous airflow is a continuous burden
tothe mucosa, which will not heal unless artificial irrigation
isinstituted or airflow artificially obtunded. Clinical
observationssupport this idea: Bunnag and coworkers (5) noted that
in ARpatients with marked septal deviation, crust is found only in
thewider side of the nasal cavity; Gupta (20) reported improve-
ment in the symptoms of unilateral AR after the septal
devia-tion was corrected surgically. This improvement may be due
tothe more uniform division of the humidification task betweenthe
cavities after surgery. This reasoning suggests that the nasalcycle
may have an important role in allowing each cavity torecover after
it has been responsible for warming and humid-ifying the air for a
while. This duty of the nasal cycle inproviding a rest period for
recovery of the nasal epitheliumfrom any damage caused by the
airflow has also been proposedby others (4, 12).
The objective of this research was to investigate airflow,water
transport, and heat transfer in the nose of an AR patientwho
underwent a surgical procedure to narrow his nasal cavity.We also
performed calculations of the air-conditioning process
in the noses of four healthy humans to establish a basis
forcomparison. Our aim was to test the hypothesis that
thepathophysiology of AR is associated with excessive evapora-tion
of the mucous layer, as well as to devise strategies toimprove the
outcome of cavity-narrowing procedures in thetreatment of AR.
MATERIALS AND METHODS
A 26-year old Caucasian male was diagnosed with primary AR inthe
Santa Casa hospital in Belo Horizonte, Brazil. His symptoms
wereaggressive fetor; nasal crusting; mucosal atrophy; rhinorrhea;
resorp-tion of the turbinates, resulting in a large nasal cavity;
and a paradox-ical sensation of nasal congestion. A marked atrophy
of the inferior
and middle turbinates yielded roomy nasal passages, especially
in theleft side. Both sides were affected by the disease, but the
right cavitywas not as wide as the left because of a septal
deviation. The patientreported having symptoms since he was 13
years old and that hissymptoms had not responded to repeated
courses of antibiotics.
The patient underwent a nasal cavity-narrowing procedure.
Ribcartilage was implanted under the mucosa along the floor of the
nose,and a septum spur was removed. At the time of surgery, it
wasreasoned that the septal deviation assisted in maintaining the
rightcavity narrow; therefore the deviation was not corrected.
Cartilagewas implanted mostly in the left side as an effort to
narrow the mostpatent side. Computerized tomography (CT) scans of
the nasal pas-sages were taken before and 6 wk after surgery. Axial
slices withthickness of 1.0 mm and an increment of 0.6 mm were
used, resultingin 109 cross sections.
The nasal geometry of the four healthy adult humans used in
thisstudy came from coronal cross sections of hexagonal meshes that
hadbeen created at The Hamner Institutes for Health Sciences
(ResearchTriangle Park, NC) from MRI scans of 3-mm spacing (43).
TheseMRI scans were carefully selected from a sample of 17 scans
ofhealthy volunteers to represent complete nasal passages and a
broadrange of surface area-to-volume ratios (19a). All subjects
participating
in this study signed a consent form. The research described in
thismanuscript was approved by our institution and by the
BiomedicalEngineering committee of Conselho Nacional de Pesquisa e
Desen-volvimento (CNPq), Brazil, through Postdoctoral Grant
201248/2004-2.
The nasal geometries were reconstructed in three dimensions
usingmedical imaging software (Mimics, Materialise, Ann Arbor, MI)
andmeshed with tetrahedral elements (ICEM-CFD, Ansys,
Canonsburg,PA). The quality of the tetrahedra was checked using
ICEM-CFD toensure that all cells had an aspect ratio larger than
0.3, a value neededto avoid distorted elements and optimize the
accuracy of the numer-ical simulations. The nasal cavity was
modeled as a rigid structure.
Steady-state inspiratory air, heat, and water transport were
simu-lated using Fluent (Fluent, Inc., Lebanon, NH). Pressure-inlet
andpressure-outlet boundary conditions were used to mimic the
pressure-
driven respiration occurring in real life. A constant pressure
drop wasimposed equally on both nostrils of each reconstructed nose
andchosen (using the target-mass-flow-rate feature of Fluent) such
thatthe total volumetric flow through the nostrils was 250 ml/s,
corre-sponding to resting breathing (2). A no-slip (zero velocity)
boundarycondition was assumed at the airway walls.
The experimental literature on nasal respiration suggests that
air-flow is primarily laminar in healthy adults during resting
breathing (7,21, 30). Likewise, most published CFD investigations
assume thatnasal airflow is laminar at rest (3, 31, 40, 48, 56).
However, there areno experimental data on the airflow patterns in
abnormally wide nasalcavities, such as noses affected by AR. Also,
the flow rate at whichturbulence effects become important in
healthy noses is still uncertainsince some researchers have
observed a partially turbulent flow evenat low air velocities (17,
45). For this seminal study, we assumed that
nasal airflow is laminar in normal and abnormal geometries.
Forhealthy nasal cavities, this hypothesis has been shown to
provideaccurate predictions (31, 48).
Lindemann and coworkers (34) measured mucosa temperatureduring
the respiratory cycle in 15 healthy volunteers at room condi-tions
of 25 1C and 30 4% relative humidity (RH). They reportedthat during
the course of inspiration, temperature decreased from32.5 1.1C to
30.2 1.7C in the nasal valve and from 34.4 1.1C to 33.2 2.3C in the
nasopharynx. During expiration, themucosal temperature increased
back to original values. Thus weadopted a mean value of 32.6C for
the mucosal temperature duringinspiration. Ambient air was set to
20C at the nostrils, and outflowboundary conditions were applied to
the outlet (see APPENDIX fordetails). To account for the cooling
effect of water evaporation, our
1083ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
4/12
heat flux calculation included a term of water flux times the
latent heatof evaporation, as proposed by Naftali et al. (40)
(APPENDIX).
The respiratory epithelium is coated with mucus, and thus air
wasassumed to be at 100% RH at the air-tissue boundary of the main
nasalcavity. However, the nasal vestibule is lined with squamous
epithe-lium, and therefore water flux was set to zero in this
region. To definethe vestibule, we created a curve on the nasal
surface by intersectingthe nasal geometry with a cylinder (diameter
20 mm) whose axis is
perpendicular to the septum. This curve was a good first
approxima-tion of the limen nasi, the anatomic ridge marking the
boundarybetween the nasal cavity proper and the vestibule (33). The
curve wasthen used to split the nasal surface, defining a region
covered withsquamous epithelium (nasal vestibule) and a region
covered withrespiratory epithelium (proper nasal cavity), where the
above-men-tioned boundary conditions were defined. Ambient air was
consideredto be at 50% RH, while outflow boundary conditions were
applied tothe outlet (see APPENDIX).
Nasal resistance (Rnose), defined as Rnose p/Q, where p is
thepressure drop in pascals (Pa) and Q is the flow rate in
milliliters persecond (ml/s), was computed from the simulation
results and com-pared with literature data obtained by
rhinomanometry (38). Meshdensity tests were conducted to ensure
grid independence of allresults, and the data reported here were
obtained in meshes of
900,0001,300,000 tetra cells. More details on the differential
equa-tions solved in Fluent, computational algorithms employed,
andboundary conditions and physical properties utilized can be
found inAPPENDIX.
RESULTS
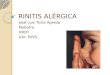
To characterize the geometry of the atrophic nose andcompare it
with healthy cavities, cross-sectional areas of coro-nal sections
from the nostrils to the beginning of the nasophar-ynx were
calculated (Fig. 1). The cross-sectional areas of thehealthy nasal
airways were at a minimum 15 mm posterior tothe nostrils. This
region, known as the nasal valve, correspondsto the level prior to
and including the anterior end of theinferior turbinate, and it is
responsible for most of the resis-tance to airflow (22, 25, 42).
Posterior to the valve, thecross-sectional area increased rapidly
to a plateau value thatwas maintained through most of the turbinate
region. Ap-proaching the choanae, the turbinates receded, the cross
sec-tions gradually became two oval empty spaces, and the
cross-sectional areas increased rapidly.
The before-surgery nasal geometry of the AR subject
wasremarkably different. The cross-sectional area increasedsteadily
from the nostrils to the end-turbinate region (except for
a small decline at the nasal valve), being at least twice
thenormal value throughout most of the turbinate region (Fig.
1).After implantation of rib cartilage under the mucosa on thefloor
of the nose, the cross-sectional areas of the anteriorportion
became similar to normal. The posterior part, however,was not
modified during surgery and, therefore, remainedwide. An expansion
of both inferior turbinates was observed
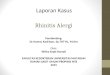
throughout the nasal cavity after surgery (Fig. 2).Volumes and
surface areas of the models were calculated for
each nasal cavity from the nostrils to the end of the
septum(Table 1). The atrophic nose had a smaller surface area and
alarger volume than the normal subjects. Surgery decreased
thevolume but did not increase the surface area. A useful
mea-surement to determine whether a nasal cavity is narrow or
wideis the surface area-to-volume ratio (SAVR). The narrower
thecavity is, the larger is the SAVR, and vice versa. Our sampleof
four healthy humans had a mean SAVR of 0.97 0.14mm1 for the left
and right cavities combined. This value is ingood agreement with a
recent study by Yokley (53), who usedCT scans to calculate SAVRs in
a much larger sample (40
European Americans and 9 African Americans) of
healthyvolunteers. He found SAVR 1.05 0.23 mm1 in
Europeandescendents and SAVR 1.03 0.29 mm1 in African ones.In
contrast, before surgery the atrophic nose had a SAVR of0.39 mm1,
which increased to 0.50 mm1 after surgery.
Several investigators have reported that in a normal nose,
airflows mainly near the septum, especially along the floor of
thenose and between the septum and the middle meatus (30, 42,48,
52). A small percentage of air flows through the meatusesand the
olfactory slit. The turbinates have been reported tohave a
streamlining effect, directing the flow to the nasophar-ynx,
leaving the airflow distribution almost unchanged as flowrate
increases (21, 31, 42, 48). In contrast, our simulationsdisplayed a
very different pattern in the atrophic nasal cavity.We predicted
that in an empty nose, the air flows mainlythrough the upper half
of the cavity, while a low-velocity eddywas observed in the
inferior portion (Fig. 2).
Our simulations predicted that the atrophic nose did notwarm or
humidify the air as effectively as the healthy nasalairways studied
(Table 2). Simulated air temperature wasalready within 1.5C of the
mucosal temperature at the mid-turbinate region for the normal
subjects (4050 mm after thenostrils; Fig. 3A). Meanwhile, at the
same location, the tem-
Fig. 1. Cross-sectional areas of coronal sections of the
humannose (left and right cavities combined). The distance along
thenose is measured from the first coronal section after the
nostrils.The curve representing a normal nose is an average of the
4healthy subjects included in this study; the bars show the rangeof
variation in these data. Atrophic pre-op and atrophic post-oprefer,
respectively, to the atrophic nose before and after surgery.
1084 ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
5/12
perature was still 2728C in the before-surgery atrophic
nose,which is 4.65.6C below the mucosal temperature. Aftersurgery,
the airflow simulations predicted the nose had par-tially recovered
its capacity to warm the inspired air (Fig. 3A;
Table 2). A similar behavior was predicted for air
humidifica-tion (Fig. 3B; Table 2).
To provide a partial test of our hypothesis that AR is relatedto
exaggerated evaporation of the mucous layer, we computedwater
fluxes per unit area throughout the nasal mucosa(Figs. 46; Table
3). In the normal noses studied, inspired airwas warmed and
humidified mainly in the anterior-inferiorportion of the cavity
(Fig. 3), in agreement with previousreports (28, 40), and thus this
was the region with the largestheat and water fluxes (Figs. 5 and
6). In contrast, the disturbedflow pattern and smaller surface area
of the atrophic nosepredicted a very different scenario. Here,
large water fluxeswere spread throughout most of the nasal cavity
(Figs. 5 and 6),with hot spots along the superior part of the
cavity and on themiddle turbinate (Fig. 4). Past the nasal valve,
heat and waterfluxes were higher in the atrophic geometries than in
thenormal subjects (Fig. 5). In particular, the AR nose had
muchhigher heat and water fluxes in the nasopharynx compared
withthe normal noses (Table 3).
After surgery the atrophic nose had a significant imbalancein
the partitioning of airflow (Table 4). While 64% of the airflowed
through the left cavity before surgery, this fractionincreased to
91% postoperatively. Consequently, the left cavitycarried out most
of the air conditioning, leading to much higherheat and water
fluxes in this side than in the right side andpreventing a desired
reduction in water flux levels on the leftside postoperatively
(Table 3). This imbalance in airflow dis-tribution was partially
due to a postsurgery constriction in theright side caused by excess
implantation of cartilage at thenasal valve area (more details
below).
Postoperative CT scans depicted the atrophic nose 6 wk afterthe
procedure. At this stage, the patient reported nasal obstruc-
Fig. 2. Airflow patterns in the atrophic nose compared with
ahealthy nasal cavity colored by air speed magnitudes.
Left:streamlines of massless particles released from the left
nostril.
Right: airflow distribution at coronal cross-sections at 15
mm(a), 35 mm (b), and 55 mm (c) after the nostrils.
Table 1. Geometrical features of our 6 human meshes
Subject/Region Surface Area, mm2 Volume, ml SAVR, mm1
Healthy nose 1Left cavity 9,900 9.2 1.07Right cavity 10,190 8.7
1.17Both cavities 20,090 18.0 1.12
Healthy nose 2Left cavity 8,300 7.9 1.06Right cavity 8,330 7.8
1.07Both cavities 16,630 15.6 1.06
Healthy nose 3Left cavity 11,620 11.6 1.00Right cavity 11,510
15.5 0.74Both cavities 23,130 27.1 0.86
Healthy nose 4Left cavity 10,240 13.2 0.78Right cavity 10,380
11.0 0.94Both cavities 20,620 24.2 0.85
Atrophic preopLeft cavity 7,130 24.0 0.30Right cavity 6,220 10.5
0.59Both cavities 13,350 34.5 0.39
Atrophic postopLeft cavity 6,270 13.7 0.46Right cavity 5,860
10.6 0.55Both cavities 12,130 24.3 0.50
Atrophic preop and atrophic postop refer, respectively, to the
pre- andpostoperative geometries of the atrophic nose. SAVR is the
surface area-to-volume ratio of the nasal cavity from the nostrils
to the end of the septum.
1085ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
6/12
tion and anosmia, but no crusting, rhinorrhea, or fetor.
Sixmonths after surgery, partial resorption of the implant
wasnoted. The patient was satisfied with the absence of stench,
butendoscopy revealed crust formation on the posterior portion
ofthe septum, between the septum and the superior turbinate,
andalong the medial aspect of the middle and inferior turbinates
onthe left side. There were fewer crusts in the right cavity,
andthese were located on the proximal aspect of the middleturbinate
and in the upper posterior region. The larger amountof crusts on
the left side correlated with the higher left-sideflow rate and
water flux levels (Tables 3 and 4). The postop-erative total amount
of crusts seemed to be smaller than the
preoperative, which might be related to the improvement of
thefetor 6 mo after the operation. Anosmia and nasal
obstructionwere persistent symptoms.
Despite the patients preoperative complaint of nasal
con-gestion, the calculated nasal resistance of the AR nose
wassmaller than the values predicted for the four healthy
nosesbefore surgery (Table 2; Fig. 7). On the other hand,
thepostoperative nasal resistance was predicted to be twice aslarge
as the average for our four healthy noses. This higherpostoperative
resistance was partially due to the cavity-narrow-ing procedure and
partially due to the different positions of thesoft palate in the
before and after CT scans, which led to a
Table 2. Air temperature, relative humidity, and water content
at the nasopharynx, and nasal resistance for inspiratoryairflow of
250 ml/s through left and right cavities combined
Subject Temperature, oC RH, % Water Content, kg/m3 Rnose,
Pa/(ml/s)
Healthy nose 1 32.4 100.0 0.0366 0.070Healthy nose 2 32.3 100.0
0.0362 0.082Healthy nose 3 32.3 100.0 0.0363 0.039
Healthy nose 4 32.0 99.8 0.0356 0.046Atrophic preop 29.7 95.7
0.0297 0.028Atrophic postop 30.9 98.2 0.0330 0.119
Atrophic preop and atrophic postop refer, respectively, to the
pre- and postoperative geometries of the atrophic nose. Mucosal
temperature and relativehumidity (RH) were assumed to be 32.6C and
100%, respectively. Rnose, nasal resistance.
Fig. 3. Temperature (A) and water content (B) of the air
streamaveraged over coronal cross sections along the human nose.
SeeFig. 1 legend for more information on symbols.
1086 ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
7/12
narrower nasopharynx in the postsurgery geometry. The rise
innasal resistance a month and a half postoperatively was
ex-pected: the surgeon had anticipated that partial resorption
ofthe implants would occur and implanted excess cartilage.Because
of the implant resorption, nasal resistance most likelydiminished
since the CT scans were taken, but no quantitativeassessment could
be made because of the lack of a rhinoma-nometer in our Brazilian
clinic. Thus our data suggest that thepreoperative complaint of
nasal congestion was due to loss ofsensory receptors, in agreement
with rhinomanometry datacollected by Moore and Kern (38) for 135 AR
patients, whilethe postoperative nasal congestion may be associated
with theincreased nasal resistance.
DISCUSSION
The human nose is responsible for warming, humidifying,and
cleaning inspired air. To accomplish this task, the nasalmucosa is
coated with a thin layer of mucus, which trapsair-borne particles
as well as moistens the air by evaporation.AR is a chronic disease
of the nasal mucosa, and its etiology isstill unknown. The disease
is characterized by progressiveatrophy, nasal crusting, dryness,
fetor, enlargement of the nasal
space, and a paradoxical sensation of nasal congestion.
Twocomprehensive reviews of AR have recently been published,and the
readers are referred to them as detailed descriptions ofthis
disease (11, 38).
Fig. 4. Regions of the nasal mucosa were thewater flux per unit
area exceeds 2 104
kg/(s m2). Only the left cavity and the naso-pharynx are shown.
(Nostrils are to the left;nasopharynx to the right.) Note that the
wa-ter flux was set to be zero at the nasalvestibule. Atrophic
pre-op and atrophicpost-op refer, respectively, to the pre-
andpostoperative geometries of the atrophicnose.
Fig. 5. Circumferential averages of heat flux (A) and water
flux(B) through the nasal wall as a function of the distance from
thenostrils. For each subject, the data represent the nasal
cavitywith the higher air flow rate (Table 4). See Fig. 1 legend
formore information on symbols.
1087ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
8/12
We simulated the airflow and transport processes that occurin
the nasal cavities of four healthy humans and one ARpatient. We
found that, while air humidification occurredmainly in the
anterior-inferior portion of the cavity in thehealthy noses studied
(Figs. 5 and 6), high water fluxes weremore spread out in the AR
nose, with hot spots at the superiornasal cavity and on the
proximal aspect of the middle turbinate(Fig. 4). These hot spots
correlated with the regions wherecrusting is more frequently
observed in AR patients in ourBrazilian clinic. Other investigators
have also reported that themiddle turbinate is more frequently
affected than the inferiorturbinate (23, 47). Ssali (47) stated
that in the early stage of thedisease crusts may be confined to the
middle and superior
turbinates, but one hardly ever finds crusts confined to
theinferior turbinate without involvement of the middle one.These
findings suggest that the superior air current that waspredicted in
our simulations (Fig. 2) may be a prevailingfeature of AR, leading
to crust formation mainly in the upperhalf of the cavity. Our
simulations also predicted an above-normal mucus evaporation past
the nasal valve in the AR nose(Fig. 5). In particular, water fluxes
were substantially higher atthe nasopharynx of the atrophic nose
compared with thenormal noses (Table 3). This may explain why AR is
oftenaccompanied by pharyngitis sicca, a disease characterized
byatrophy of the mucous glands and absence of their secretion(11,
44).
Fig. 6. Circumferential averages of heat flux (A) and water
flux(B) through the nasal wall as a function of the height from
thenasal floor. For each subject, the data represent the nasal
cavitywith the higher air flow rate (Table 4). See Fig. 1 legend
formore information on symbols.
Table 3. Total heat and water fluxes per unit area in each
region of the nasal cavity
Subject
Heat Flux, 103 W/m2 Water Flux, 104 kg/(s m2)
Leftcavity
Rightcavity Nasopharynx
Leftcavity
Rightcavity Nasopharynx
Healthy nose 1 1.12 0.93 0.03 3.99 3.30 0.11Healthy nose 2 1.17
1.24 0.05 4.17 4.43 0.17Healthy nose 3 0.66 1.05 0.11 2.35 3.72
0.37Healthy nose 4 1.01 0.80 0.28 3.61 2.88 0.98Atrophic preop 1.17
0.78 0.86 4.12 2.80 3.02Atrophic postop 2.18 0.26 0.72 7.92 0.99
2.58
Atrophic preop and atrophic postop refer, respectively, to the
pre- and postoperative geometries of the atrophic nose.
1088 ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
9/12
These results are consistent with the hypothesis that abnor-mal
patterns of mucus evaporation may play a key role in
thepathophysiology of AR. The wide nasal cavity of the ARpatient
(demonstrated by below-normal surface area-to-volumeratio)
generated an abnormal flow pattern. This abnormaldistribution of
airflow, in turn, led to an increase in the water
fluxes in regions that normally would not be subject to
highlevels of mucus evaporation, namely the upper half of the
nasalcavity (Fig. 6B). The drying effect of the airflow would
beexpected to increase the viscosity of the mucus, fostering
theformation of crusts. These crusts may in turn impair thedelicate
ciliary apparatus, causing stasis of the secretion, per-haps
leading to more crust formation. The lack of nasalclearance
facilitates infection by opportunistic pathogens; andthe fetor that
characterizes the disease may come from thesehighly infected
crusts. This reasoning was also proposed byWachsberger (49).
Mygind et al. (39) explain how the normal nasal
epitheliumgradually changes from squamous epithelium to
pseudostrati-fied columnar epithelium with abundant ciliated cells
moving
from the vestibule toward the turbinates. The ciliated cells
donot appear suddenly, but rather their density increases
gradu-ally going deeper into the nose. The prediction of high
waterflux in the anterior portion of the healthy nose (Figs. 4 and
5)suggests that ciliated cells are more predominant in regions
oflow water flux. Since in the atrophic nose large water fluxeswere
not restricted to the anterior portion of the cavity, wepropose
that the abnormal patterns of water fluxes in the
atrophic nose may lead to replacement of ciliated cells by
someother type in the respiratory epithelium. The
characteristicfinding of patches of squamous epithelium in the
respiratorymucosa of AR patients is in agreement with this
reasoning (1,5, 11, 19). It is recognized that exposure to
irritants in generalcan cause squamous metaplasia. Thus squamous
metaplasiamay occur in AR patients because of the drying effects
of
airflow, rather than being the root cause for the lack of
mucouslayer. Once the epithelium has been replaced, the patches
ofsquamous epithelium may be expected to contribute to theshortage
of mucus, stasis, and progress of the disease. Morestudies are
needed, however, to establish a causal associationbetween regions
of high mucus evaporation and squamousmetaplasia.
AR is not permanently cured by antibiotics (38). One way
tocontrol the disease is to irrigate the nose artificially, but
thesymptoms return whenever the irrigation is ceased. Our
hy-pothesis may explain this relentless nature of the
diseasebecause the disease would not be expected to recede
whileexcessive evaporation of the mucus continued. The
hypothesisalso suggests that closure of the nostrils (Youngs
procedure)stops the disease because suturing the nostrils releases
the nosefrom its humidification task.
The anosmia in AR patients has been proven to be a
sensoryproblem, since electron microscopic studies have shown
thatthese patients have atrophy of the olfactory epithelium
recep-tors (38). Our simulations suggest that loss of these
receptorsmay be due to the high water flux predicted at the
olfactoryregion (Figs. 4 and 6B). In a healthy nose, air flows
mainlyalong the floor and between the septum and the middle
meatus(16, 48, 52). Only 1015% of the air passes through
theolfactory slit. In contrast, in the atrophic nose, most of the
airflowed along the upper half of the nose (Fig. 2). Comparedwith
the healthy nose, this abnormal airflow distribution sub-
jects the olfactory epithelium to increased water and heat
fluxesthat may damage the olfactory cells by drying the
epithelium.
The sensation of nasal congestion in AR has been proposedto be
due to the loss of receptors for pain and temperature (38).However,
this hypothesis is still unproven (38). The calculatednasal
resistance for the before-surgery atrophic nose, 0.028Pa/(ml/s), is
below the range of resistances we computed forthe four normal
cavities, namely 0.0390.082 Pa/(ml/s). This
Table 4. Flow partitioning between left and right nasalpassages
in the 6 human nasal geometries studied
Subject
Flow Partitioning
Left Cavity Right Cavity
Healthy nose 1 54.7% 45.3%Healthy nose 2 48.1% 51.9%
Healthy nose 3 37.5% 62.5%Healthy nose 4 57.6% 42.4%Atrophic
preop 63.8% 36.2%Atrophic postop 90.8% 9.2%
Atrophic preop and atrophic postop refer, respectively, to the
pre- andpostoperative geometries of the atrophic nose.
Fig. 7. Pressure averaged over coronal cross sections
versusdistance from nostrils in the atrophic and normal noses
studied.See Fig. 1 legend for more information on symbols.
1089ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
10/12
finding substantiates the nomenclature paradoxical for
thecomplaints of nasal congestion associated with AR and is
inagreement with rhinomanometry data collected by Moore andKern
(38) in 135 AR patients. The mean total nasal resistancein their
patients was 0.12 Pa/(ml/s), while literature reports forhealthy
subjects are on the order of 0.150.30 Pa/(ml/s) (38).The resistance
figures calculated by CFD are somewhat lower
than the ones obtained through rhinomanometry, as also foundin
other CFD studies (50). However, it should be borne in mindthat by
convention, rhinomanometry calculates nasal resistanceat a
transnasal pressure drop of 150 Pa (6). The simulationspresented in
this study were based on resting airflow rates,where the transnasal
pressure drop is considerably lower. Thenonlinear shape of the
pressure-flow curve for nasal airflowmeans that the resistance
figures calculated in this work are notdirectly comparable to
rhinomanometry. Nevertheless, bothmethods are consistent in
predicting reduced nasal resistancesfor AR patients.
The high efficiency of a healthy nasal cavity for warmingand
humidifying the inspired air is well recognized (8, 28, 29,36, 40).
The simulations presented in this study predicted thatat rest
inspired air was already within 1.5C of the mucosatemperature
(Tmucosa 32.6C) at the middle of the normalturbinate region (Fig.
3A). Due to the abnormal patency of theatrophic nose, however, air
was still 4.65.6C colder thanTmucosa (27C Tair 28C) when it reached
the samelocation before surgery. While in the normal noses air
exitedthe nasopharynx at Tair Tmucosa and with 36 g water/m
3 ofair, in the before-surgery atrophic nose air was still
3Cbelow Tmucosa and the water content was still 30 g/m
3 of air(Table 2). These predictions are consistent with
experimentalmeasurements by Drettner et al. (10), who measured
theair-conditioning capacity of normal and pathological noses
andfound that atrophic noses do not condition the air as
effectively
as normal ones. Also in agreement with our simulations,Lindemann
et al. (35) found a decreased capacity to warminspired air in
cavities widened through aggressive sinus sur-gery with resection
of the turbinates. Interestingly, dryness andcrusting are also
frequent complaints of these patients (35).
Our simulations predicted that the cavity-narrowing proce-dure
improved the air-conditioning properties of the atrophicnose. At
the nasopharynx level, air was 1.2C warmer and2.5% more humid
postoperatively (Table 2). The surgery,however, failed to restore
the normal airflow and water fluxpatterns (Figs. 2 and 4). Our
analysis of the water transport 6wk after surgery suggests that
mucus evaporation increasedpostoperatively in the left cavity
(Figs. 5 and 6; Table 3). Thisincrease was partially due to the
great imbalance in airflow
partitioning between the two cavities after surgery (Table
4).Six months after surgery, crusts were observed mostly in theleft
side, in agreement with the higher airflow and higher waterflux
calculated for this side of the nose. At that time it wasobserved
that resorption of the implant widened an anteriorconstriction that
had occurred on the right cavity due to theimplant, partially
reducing the imbalance in airflow distribu-tion between the two
cavities. However, it is unlikely that thisredistribution has been
sufficient to bring the water flux levelsback to their normal
values. Therefore, our analysis suggeststhat the surgery was not a
final cure for this patient becausewater flux through the mucosa
remained abnormally high andabnormally distributed. At the present
time, the patient reports
being satisfied with the surgical outcome because his
maincomplaint (the fetor) has resolved, although crusts are
stillpresent.
At first sight, there seems to be a contradiction between
thehigher magnitude of heat and water fluxes in the atrophic
noseand incomplete air conditioning compared with the
normalsubjects (Table 2, Fig. 5). This apparent discrepancy is
ex-
plained by the reduced surface area available for heat and
waterexchange in the atrophic nose. This effectively means
that,despite the increased levels of heat and water fluxes (per
unitarea), the overall rate of heat and moisture transfer from
tissueto air in the atrophic geometries is lower than normal,
leadingto incomplete conditioning of inspired air. This finding
sug-gests that reconstructive nasal surgeries in AR should target
toaugment the nasal surface area to avoid excessive
mucusevaporation and drying.
Finally, we would like to discuss some limitations of
thisseminal investigation. First, simulations were conducted
onlyfor the inhalation part of the respiratory cycle. It is known
thatapproximately 1/3 of the heat and humidity transferred
frommucosa to inspired air is recovered during exhalation
(52).Therefore, humidity recovery during expiration needs to
beincluded in future studies to confirm that the patterns
ofincreased mucus evaporation in AR noses observed here arenot
affected. Second, the cyclic changes of flow direction andmucosal
temperature during respiration were approximated byan average,
steady-state process. Theoretical arguments sup-port this approach
with regard to the airflow patterns (31), butthe dependence of
mucosal temperature on airflow patterns isstill unclear. Recent
advances in computation capacity are justbeginning to allow the
study of time-dependent nasal airflow(26, 37), so that this
hypothesis may be tested soon.
Third, we assumed that nasal airflow is laminar in AR andnormal
noses. There is evidence that the airflow is indeed
laminar for resting flow rates in healthy noses (7, 21, 30,
31,48), but it is possible that the flow is more turbulent in the
widecavities of AR patients. To clarify this issue, the
airflowpatterns in a physical replica of the AR nose remain to
beinvestigated experimentally. The general conclusions drawn inthis
paper, however, would not change if airflow were found tobe
turbulent in the atrophic nose, since turbulence wouldincrease the
drying effect of the airflow, reinforcing the hy-pothesis that
excessive evaporation of the mucous layer playsa key role in the
pathophysiology of AR.
In conclusion, the airflow and water vapor transport
simu-lations presented in this article support the hypothesis that
ARis related to excessive evaporation of the mucous lining.
Wesuggest that three main factors contribute to increased water
flux in the mucosa of these patients. First, we found that
thelack of turbinates led to an abnormal airflow distribution.
Airflowed mainly along the top half of the nose,
substantiallyincreasing the humidification burden on this region.
Second,we found that the atrophy process reduced the surface
areaavailable for water transfer, increasing flux per unit area.
Third,we found that a unilateral obstruction concentrates air
humid-ification in the most patent side and thus contributes to
in-creased water flux in this side. Therefore, our results
suggestthat the main goals of a surgery to treat AR should be 1)
torestore the original surface area of the nose, 2) to restore
thephysiological airflow distribution, and 3) to create
symmetriccavities. These three strategies would have the overall
effect of
1090 ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
11/12
minimizing the water fluxes per unit area and reestablishing
thephysiological pattern of restricting high water fluxes to
theanterior-inferior portion of the nose. A procedure that seems
tofit these criteria is the reconstruction of the inferior and
middleturbinates (41).
APPENDIX
Description of the Computational Method
The conservation of mass and momentum for laminar,
in-compressible flow are described, respectively, by the
equations
u 0
u
t (u )u p 2u
where u u(x,y,z,t) is the velocity vector, t is time, is
fluiddensity, and is dynamic viscosity (13, 51). In our
simula-tions, we adopted 1.20 kg/m3 and 1.9 105 kg/ms(24, 40).
Heat transfer is governed by the equation of energy
conser-vation
T
t (u )T
k
cp
2T
where T T(x,y,z,t) is temperature, cp 1,005.9 J/(kg K) isthe
specific heat, and k 0.0268 W/(mK) is the thermalconductivity of
air (40). The transport of moisture from themucosa to air is
governed by the convection-diffusion equation
tcH2O (u )cH2O DH2O
2cH2O
where cH2O cH2O (x,y,z,t) is the water vapor concentration
in air and DH2O 2.6 105
m2
/s is the mass diffusivityof water vapor in air (24, 40).
Steady-state versions of these equations were solved on
adual-processor workstation (Dell Precision, Intel Xeon 3.60GHz,
3.93 GB of RAM) using Fluent 6.2.16 (Fluent, Lebanon,NH). Fluent
uses the finite volume method to solve the differ-ential equations
numerically. The segregated solver withSIMPLEC pressure-velocity
coupling and second-order, up-wind discretization were utilized for
solution of the aboveequations (14). Since the physical properties
of the air-watervapor mixture were assumed constant, an uncoupled
solutionstrategy was employed; namely, the flow field was
obtainedfirst and then the energy conservation and
convection-diffusionequations were solved.
For the healthy-nose meshes (106 tetrahedral cells), Fluenttook2
h to solve the flow field (450 iterations) and 7 minto solve the
heat/water transport equations (25 iterations).The atrophic-nose
meshes required typically twice as manyiterations/CPU time to
converge, despite having approximatelythe same number of cells.
Convergence was confirmed bysmall residuals (continuity: 103;
velocities: 5 105;energy equation: 3 107; convection diffusion
equation:7 106) and by monitoring the flow rate, temperature, andRH
at the outlet surface for stabilization.
RH is the ratio of the partial pressure of water vapor
actuallypresent in the mixture (pH2O) to the water vapor pressure
ofsaturated air at the same temperature (pH2O,s). The latter is
calculated in Fluent from experimental data, while the formeris
obtained in Fluent from the water concentration in air(cH2O) using
the ideal-gas law pH2O RTcH2O/MMH2O, whereR 8.31 Pa m3/(mol K) is
the universal gas constant andMMH2O 0.018 kg/mol is the molecular
mass of water. Ourboundary condition of 100% RH at the walls (at
32.6C) wasdefined as cH2O Wall 0.03694 kg/m
3. For the inlet, 50% RH (at
20C) corresponds to cH2O Inlet 0.00869 kg/m3
. The out-flow boundary condition in Fluent imposes ( Tn) 0 and(
cH2O n) 0 at the outlet, where n is a unit vector normal tothe
surface. Any backflow at the outlet was assumed to be at32.6C and
100% RH.
Fluent 6.2 does not provide the option of plotting species
flux[fluxH2O DH2O (n cH2O)Wall] through the domain walls.Therefore,
a user-defined function was written in Fluent tomake the water flux
data available as a user-defined memoryvariable. To take into
account that water evaporation increasesthe heat lost by the nasal
mucosa, heat flux (fluxheat) wascomputed from
fluxheat k T fluxH2OH
where H 2.411 106
J/kg is the latent heat of evaporationof water at nasal-tissue
temperature (40).
ACKNOWLEDGMENTS
We thank Jeffry Schroeter, Kambiz Nazridoust, Mel Andersen,
DarinKalisak, Rebecca Segal, David Wexler, Maurlio N. Vieira, and
RonaldDickman for contributions to this research. We are also
grateful to Dr. UedsonTazinaffo and to the Hospital Madre Teresa
(Belo Horizonte, Brazil) for kindlyproviding the CT scans used in
this study.
GRANTS
This work was made possible by a postdoctoral grant from CNPq,
Brazil,and the financial support of the American Chemistry Council
to The HamnerInstitutes for Health Sciences (previously CIIT
Centers for Health Research).
REFERENCES
1. Anand CS, Agrawal SR. A histopathological study in atrophic
rhinitis.J Indian Med Assoc 59: 278281, 1972.
2. Annals of the International Commission on Radiological
Protection24. Human Respiratory Tract Model for Radiological
Protection (ICRPPublication 66). Oxford: Pergamon, 1994.
3. Bailie N, Hanna B, Watterson J, Gallagher G. An overview of
numer-ical modelling of nasal airflow. Rhinology 44: 5357,
2006.
4. Boyce J, Eccles R. Do chronic changes in nasal airflow have
anyphysiological or pathological effect on the nose and paranasal
sinuses? Asystematic review. Clin Otolaryngol 31: 1519, 2006.
5. Bunnag C, Jareoncharsri P, Tansuriyawong P, Bhothisuwan
W,Chantarakul N. Characteristics of atrophic rhinitis in Thai
patients at theSiriraj Hospital. Rhinology 37: 125130, 1999.
6. Calhoun KH, House W, Hokanson JA, Quinn FB. Normal
nasalairway-resistance in noses of different sizes and shapes.
Otolaryngol Head
Neck Surg 103: 605609, 1990.7. Chung SK, Son YR, Shin SJ, Kim
SK. Nasal airflow during respiratorycycle. Am J Rhinol 20: 379384,
2006.
8. Cole P. Modification of inspired air. In: The Nose: Upper
Airway Phys-iology and the Atmospheric Environment, edited by
Proctor DF, AndersenIB. Amsterdam, The Netherlands: Elsevier
Biomedical, 1982, p. 351375.
9. Donko T, K ovacs M , Magyar T. The effect of atrophic
rhinitis (AR) onthe weight-gain of swine. Agriculturae Conspectus
Scientificus 68: 161164, 2003.
10. Drettner B, Falck B, Simon H. Measurements of
air-conditioning capac-ity of nose during normal and pathological
conditions and pharmacolog-ical influence. Acta Otolaryngol 84:
266277, 2000.
11. Dutt SN, Kameswaran M. The aetiology and management of
atrophicrhinitis. J Laryngol Otol 119: 843852, 2005.
12. Eccles R. Nasal airflow in health and disease. Acta
Otolaryngol 120:580595, 2000.
1091ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www.jap.org
-
7/28/2019 RINITIS ATROFICA 4
12/12
13. Faber TE. Fluid Dynamics for Physicists. Cambridge, UK:
CambridgeUniv. Press, 1995.
14. Fluent 6.2. Users Guide. Lebanon, NH: Fluent, 2004.15. Frame
EM, Gufler H, Henninger W, Gasteiner J. Diagnosis of atrophic
rhinitis in a Simmental heifer by computed tomography. Vet Rec
146:558560, 2000.
16. Garcia GJM. Topics in Biophysics: Bone Allometry, the BS
Model forBiological Evolution, and the Nasal Airflow in Humans [In
Portuguese](PhD thesis). Belo Horizonte, Brazil: Universidade
Federal de MinasGerais, 2005.
17. Girardin M, Bilgen E, Arbour P. Experimental study of
velocity fieldsin a human nasal fossa by laser anemometry. Ann Otol
Rhinol Laryngol92: 231236, 1983.
18. Girgis IH. Surgical treatment of ozena by dermofat graft. J
Laryngol Otol80: 615627, 1966.
19. Gray RFE, Barton RPE, Wright JLW, Dilly PN, Moss RF.
Primaryatrophic rhinitis: a scanning electron microscopic (SEM)
study. J LaryngolOtol 94: 985992, 1980.
19a.Guilmette RA, Cheng YS, Griffith WC. Characterising the
variability inadult human nasal airway dimensions. Ann Occup Hyg
41, Suppl 1:491496, 1997.
20. Gupta SC. Septoplasty in unilateral atrophic rhinitis with
deviated nasalseptum. J Laryngol Otol 99: 163165, 1985.
21. Hahn I, Scherer PW, Mozell MM. Velocity profiles measured
forair-flow through a large-scale model of the human nasal cavity.
J Appl
Physiol 75: 22732287, 1993.22. Haight JSJ, Cole P. The site and
function of the nasal valve. Laryngo-scope 93: 4955, 1983.
23. Han-Sen C. The ozena problem. Clinical analysis of atrophic
rhinitis in100 patients. Acta Otolaryngol 93: 461464, 1982.
24. Hinds WC. Aerosol Technology: Properties, Behavior, and
Measurementof Airborne Particles. New York: Wiley, 1999.
25. Hirschberg A, Roithmann R, Parikh S, Miljeteig SH, Cole P.
Theairflow resistance profile of healthy nasal cavities. Rhinology
33: 1013,1995.
26. Ishikawa S, Nakayama T, Watanabe M, Matsuzawa T.
Visualization offlow resistance in physiological nasal respiration:
Analysis of velocity andvorticities using numerical simulation.
Arch Otolaryngol 132: 12031209,2006.
27. Jackson LE, Koch RJ. Controversies in the management of
inferiorturbinate hypertrophy: a comprehensive review. Plast
Reconstr Surg 103:300312, 1999.
28. Keck T, Leiacker R, Riechelmann H, Rettinger G. Temperature
profilein the nasal cavity. Laryngoscope 110: 651654, 2000.
29. Keck T, Leiacker R, Heinrich A, Kuhnemann S, Rettinger G.
Humid-ity and temperature profile in the nasal cavity. Rhinology
38: 167171,2000.
30. Kelly JT, Prasad AK, Wexler AS. Detailed flow patterns in
the nasalcavity. J Appl Physiol 89: 323337, 2000.
31. Keyhani K, Scherer PW, Mozell MM. Numerical simulation of
airflowin the human nasal cavity. J Biomech Eng 117: 429441,
1995.
32. Krametter R, Hassan J, Mayrhofer E, Baumgartner W.
Atrophicrhinitis in sheep in Austria. Vet Rec 154: 147148,
2004.
33. Lang J. Clinical Anatomy of the Nose, Nasal Cavity and
ParanasalSinuses. New York: Thieme Medical, 1989.
34. Lindemann J, Leiacker R, Rettinger G, Keck T. Nasal mucosal
tem-perature during respiration. Clin Otolaryngol 27: 135139,
2002.
35. Lindemann J, Leiacker R, Sikora T, Rettinger G, Keck T.
Impact ofunilateral sinus surgery with resection of the turbinates
by means ofmidfacial degloving on nasal air conditioning.
Laryngoscope 112: 20622066, 2002.
36. Lindemann J, Keck T, Wiesmiller K, Sander B, Brambs HJ,
RettingerG, Pless D. A numerical simulation of intranasal air
temperature duringinspiration. Laryngoscope 114: 10371041,
2004.
37. Lindemann J, Brambs HJ, Keck T, Wiesmiller KM, Rettinger
G,Pless D. Numerical simulation of intranasal airflow after radical
sinussurgery. Am J Otolaryngol 26: 175180, 2005.
38. Moore EJ, Kern EB. Atrophic rhinitis: a review of 242 cases.
Am JRhinol 15: 355361, 2001.
39. Mygind N, Pedersen M, Nielsen MH. Morphology of the upper
airwayepithelium. In:The Nose: Upper Airway Physiology and the
Atmospheric
Environment, edited by Proctor DF, Andersen IB. Amsterdam, The
Neth-erlands: Elsevier Biomedical, 1982, p. 7197.
40. Naftali S, Schroter RC, Shiner RJ, Elad D. Transport
phenomena in thehuman nasal cavity: a computational model. Ann
Biomed Eng 26: 831839, 1998.
41. Rice DH. Rebuilding the inferior turbinate with
hydroxyapatite cement.Ear Nose Throat J 79: 276277, 2000.
42. Schreck S, Sullivan KJ, Ho CM, Chang HK. Correlations
between flowresistance and geometry in a model of the human nose. J
Appl Physiol 75:17671775, 1993.
43. Segal RA, Kepler GM, Kimbell JS. Correlation of nasal
surface-area-
to-volume ratio with predicted inhaled gas uptake efficiency in
humans.ToxicolSci 78(1-S), Abstract No. 2107 (2004 Itinerary
Planner). Balti-more, MD: Society of Toxicology, 2004.
44. Shehata MA. Atrophic rhinitis. Am J Otolaryngol 17: 8186,
1996.45. Simmen D, Scherrer JL, Moe K, Heinz B. A dynamic and
direct
visualization model for the study of nasal airflow. Arch
Otolaryngol 125:10151021, 1999.
46. Sinha SN, Sardana DS, Rajvanshi VS. A nine years review of
273 casesof atrophic rhinitis and its management. J Laryngol Otol
91: 591600,1977.
47. Ssali CL. Atrophic rhinitis. A new curative surgical
treatment (middleturbinectomy). J Laryngol Otol 87: 397403,
1973.
48. Subramaniam RP, Richardson RB, Morgan KT, Kimbell JS,
Guil-mette RA. Computational fluid dynamics simulations of
inspiratory air-flow in the human nose and nasopharynx. Inhal
Toxicol 10: 91120, 1998.
49. Wachsberger A. A new technic in the surgical treatment of
ozena. ArchOtolaryngol 19: 370382, 1934.
50. Wexler D, Segal R, Kimbell J. Aerodynamic effects of
inferior turbinatereduction. Arch Otolaryngol Head Neck Surg 131:
11021107, 2005.
51. White FM. Fluid Mechanics. New York: McGraw-Hill, 2008.52.
Wolf M, Naftali S, Schroter RC, Elad D. Air-conditioning
characteris-
tics of the human nose. J Laryngol Otol 118: 8792, 2004.53.
Yokley TR. The Functional and Adaptive Significance of
Anatomical
Variation in Recent and Fossil Human Nasal Passages (PhD
thesis).Durham, NC: Duke University, 2006.
54. Young A. Closure of the nostrils in atrophic rhinitis. J
Laryngol Otol 81:515524, 1967.
55. Young A. Closure of the nostrils in atrophic rhinitis. J
Laryngol Otol 85:715718, 1971.
56. Zhao K, Scherer PW, Hajiloo SA, Dalton P. Effect of anatomy
onhuman nasal air flow and odorant transport patterns: implications
forolfaction. Chem Senses 29: 365379, 2004.
1092 ATROPHIC RHINITIS AND AIR CONDITIONING
J Appl Physiol VOL 103 SEPTEMBER 2007 www jap org