Embed Size (px)
Citation preview

Review
Role of Withania somnifera (Ashwagandha) in themanagement of male infertility
Pallav Sengupta a,b, Ashok Agarwal b,*, Maria Pogrebetskaya b,c,Shubhadeep Roychoudhury b,d, Damayanthi Durairajanayagam e,Ralf Henkel f
a Department of Physiology, Faculty of Medicine, MAHSA University, Jalan SP2, Bandar Saujana Putra, 42610Jenjarom, Selangor, Malaysiab American Center for Reproductive Medicine, Cleveland Clinic, 10681 Carnegie Avenue, Cleveland, OH 44195,USAc Case Western Reserve University/University Hospitals Cleveland Medical Center, 11100 Euclid Avenue,Cleveland, OH 44106, USAd Department of Life Science and Bioinformatics, Assam University, Silchar 788011, Indiae Discipline of Physiology, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh Campus, JalanHospital, 47000 Sungai Buloh, Selangor, Malaysiaf Department of Medical Biosciences, University of the Western Cape, Bellville 7535, Cape Town, South Africa
Pallav Sengupta is a Senior Lecturer of the Department of Physiology, Faculty of Medicine at MAHSA University,Malaysia. He has a PhD in male reproductive physiology from the University of Calcutta, India and over 24 peerreviewed publications in PubMed. He is a collaborating scientist with the American Center for Reproductive Medi-cine at Cleveland Clinic.
KEY MESSAGEWithania sominifera roots improve semen quality by increasing sperm count and motility, regulating repro-ductive hormone levels and inhibiting lipid peroxidation. Proposed mechanisms underlying these effects aredirect alleviation of oxidative stress and enhancement of hormonal balance via the gamma-aminobutyric acid-like mimetic pathway. Withania sominifera could potentially supplement routine treatment of male infertility.
A B S T R A C T
To manage male infertility caused by hormonal imbalance, infections and other predicaments, multifarious treatment strategies are emerging world-
wide. Contemporary treatments, such as assisted reproductive techniques, are costly with low success rates of only 10–30%; however, herbal remedies
are gaining more attention as an alternative or supplementary therapeutic modality for male infertility. The beneficial effects induced by oral intake of
the roots of a small evergreen shrub, Withania sominifera (Ashwagandha) on semen quality of infertile men have previously been studied. Oral intake
of Ashwagandha roots has been found to inhibit lipid peroxidation, improve sperm count and motility, and regulate reproductive hormone levels. The
molecular mechanisms of these effects, however, are yet to be unveiled.
* Corresponding author.E-mail address: [email protected] (A Agarwal).
https://doi.org/10.1016/j.rbmo.2017.11.0071472-6483/© 2017 Reproductive Healthcare Ltd. Published by Elsevier Ltd. All rights reserved.

In this review, we will discuss the role of herbal medicines in male infertility; provide a detailed analysis of various human and animal studies in-
volving Withania somnifera; describe a proposed direct oxidative mechanism involving mitigation of oxidative stress as well as an indirect mechanism
consisting of a gamma-aminobutyric acid-like-mimetic pathway ameliorating hormonal balance through crosstalk among different endocrine glands
to improve male fertility; and how Withania somnifera supplementation mitigates risk factor-induced male infertility as well as ameliorates male fertility.
© 2017 Reproductive Healthcare Ltd. Published by Elsevier Ltd. All rights reserved.
Introduction
The use of herbal medicines has persisted for thousands of years,and continues to represent a considerable area of medical treat-ment in many countries, particularly in Asia, Africa and South America.In recent years, the use of traditional medicine has expanded evenin western countries, which is signified by its steadily growing ap-plication (Samy et al., 2008). Even well-known common and widelyused medicines, such as aspirin, were originally derived from plantextracts. According to an estimation by the World Health Organiza-tion, 80% of the world’s population rely on plant-derived medicinesfor their health care, most of whom are from developing countries(Gurib-Fakim, 2006).
Plants and other natural resources have always been of interestto researchers, mainly for the treatment of various medical condi-tions as well as in the development of new drugs. It is progressivelygaining importance as a mode of treatment worldwide (Kuo et al., 2017;Mills et al., 2005; Pandey et al., 2013). In India, the traditional me-dicinal system, termed Ayurveda, supplements more modern formsof medicine. Ayurveda is also described as the ‘science of life or lon-gevity’ because it offers a comprehensive system to rejuvenate thebody towards a long, healthy life through diet and nutrition (Pandeyet al., 2013). Ayurvedic medicines have been used to treat condi-tions such as diabetes, high blood pressure, gastritis as well as femaleand male reproductive health issues (Samy et al., 2008). In the MiddleEast, herbal remedies have been found to improve fertility in dia-betic and infertile males (Khaki and Ainehchi, 2017;Ouladsahebmadarek et al., 2016). Traditional Chinese medicine alsoinvolves various modalities of treatment, some of which include acu-puncture as well as the use of herbal supplements for various typesof diseases that range from minor illnesses to life-threatening con-ditions (Crimmel et al., 2001). In the USA, complementary andalternative medicine has been increasing in popularity among thegeneral population and also within the medical community. It hasbecome a multi-billion dollar industry over the past decade (Clarkeand Black, 2015).
Because of the increased popularity, much research has focusedon various medicinal uses of plants, including treatment of male in-fertility. Many herbal drugs and commonly used food-stuffs are knownto have a beneficial effect on male reproductive health, includingTribulus terrestris (Gokhru or land caltrops), Eurycoma longifolia(Tongkat Ali), Allium sativum (garlic), Allium cepa (onion), Cannabissativa (marijuana), Capsicum frutescens (chilli pepper), and Zingiberofficinale (ginger) (Henkel et al., 2014; Lohiya et al., 2016; Mansouriet al., 2016; Tambi et al., 2012). A well-known herb from India thathas been most commonly used in the treatment of male infertility formore than 3000 years is Withania somnifera, known locally knownas Aswagandha or the ‘Indian ginseng’ (Lohiya et al., 2016; Malviyaet al., 2016). Withania somnifera has been widely used for the treat-
ment of erectile dysfunction, oligozoospermia, reproductiveendocrinological problems and other male reproductive healthproblems.
Withania somnifera is reported to have several beneficial effectson male fertility, but its mode of action based on reports from humanand animal studies has not yet been properly documented. There-fore, in this review, we discuss the role of herbal medicines in maleinfertility; provide a detailed analysis of various human and animalstudies involving Withania somnifera; describe a proposed direct oxi-dative mechanism involving mitigation of oxidative stress as well asan indirect mechanism consisting of a gamma-aminobutyric acid(GABA)-like-mimetic pathway ameliorating hormonal imbalancethrough crosstalk among different endocrine glands to improve malefertility; and how Withania somnifera supplementation mitigates riskfactor-induced male infertility.
Herbal medicine and male infertility
Infertility is defined as a couple’s inability to conceive after 1 year ofproperly timed and unprotected vaginal intercourse. Worldwide, itaffects about 48.5 million couples, with the male factor infertility ac-counting for about one-half of these cases (Mascarenhas et al., 2012).The inability to conceive may cause personal and psychological stress(Dyer et al., 2004, 2005, 2009), and can also place strain on the maritalrelationship and decrease quality of life (Agarwal et al., 2014a). In ad-dition to the stress factor involved, various infertility treatments andassisted reproductive techniques are expensive and do not offer highsuccess rates, as these range only from 10–30%. Because of the con-straints of assisted reproduction techniques, patients tend to resortto alternative remedies for male infertility, including herbal treat-ment (Dabaja and Schlegel, 2014). Yet, clinicians and researchers haveonly recently begun to investigate herbal remedies as a form of treat-ment for male fertility issues.
The causes of male infertility are numerous, and may include hor-monal imbalances, infections, varicocele and sexual dysfunction. About40–50% of cases are idiopathic (Chachamovich et al., 2009). Al-though infections and varicocele are potentially treatable, theseconditions are thought to cause an increase in oxidative stress, whichmay be the molecular basis for the infertility associated with theseconditions (Agarwal et al., 2006a). Oxidative stress occurs when animbalance occurs between reactive oxygen species (ROS) and the an-tioxidant capacity of the biological system (Hall, 2015).
The high prevalence of male infertility, and the psychological tollthat it can have on a couple trying to start or expand their family, hasled to increasing use of pharmacological, surgical and alternativetherapies. The traditional treatment for male infertility is gearedtowards deciphering the underlying cause of the infertility. If a causecan be elucidated, then treatment can be further subdivided into either
312 R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6

surgical or non-surgical options. Non-surgical treatment options aremainly based on the cause of infertility (Hall, 2015). Surgical treat-ment may be necessary to correct some forms of male infertility. Itis most often used to reverse specific anatomic or pathophysiologicdefects to improve semen quality. The end goal of surgical treat-ment is to allow couples to either conceive naturally or to have anincreased chance for a successful outcome with suitable assisted re-production techniques. For example, varicoceles have been associatedwith male infertility, and can be treated surgically by various differ-ent modalities (Esteves and Agarwal, 2016). A meta-analysis byBaazeem et al. (2011) indicated that varicocelectomy generally dem-onstrates a significant improvement in sperm concentration and totaland progressive motility; however, they found no conclusive evi-dence of improvement in spontaneous pregnancy rates after varicocelerepair. In an earlier meta-analysis, our laboratory also reported that,in patients with varicocele, seminal ROS levels increase and total an-tioxidant capacity significantly decreases, leading to oxidative stress(Agarwal et al., 2006a). In turn, the oxidative stress caused by the vari-cocele triggers nuclear DNA damage in spermatozoa (Agarwal et al.,2006b). Other surgical interventions include treatment for ejacula-tory duct obstruction, orchidopexy for an undescended testis andvarious sperm retrieval options for assisted reproduction tech-niques (Walsh and Smith, 2013).
For thousands of years, various herbal medicines have been usedworldwide for the treatment of male infertility and sexual dysfunc-tion. In China, Traditional Chinese Medicine, which includesacupuncture, massage as well as herbal supplements, is commonlyused in conjunction with western medicines for infertility treatment(Crimmel et al., 2001). In a non-randomized study comprising 202 pa-tients with male infertility, men with oligozoospermia were treatedwith Sheng Jing, a herbal mixture of 15 plants twice daily for 60 days.After this treatment, the men displayed normalized levels of testos-terone, LH and FSH, decrease in sperm antibody production as wellas improvement in semen volume, sperm density and motility. Themost notable result from this study was a high pregnancy rate of 78%in the 148 couples available for follow up (Chen and Wen, 1996). InSouth Africa, a significant proportion of the population still relies ontraditional herbal remedies for their primary health care, includingthe treatment of reproductive problems such as erectile dysfunc-tion, infertility and for contraception (Abdillahi and Van Staden, 2012).Recent investigations on Typha capensis, a Southern African plant,which is growing in wetlands, and popularly called ‘love reed’, hasbeen shown to have activity to scavenge free radicals and to stimu-late testosterone secretion by Leydig cells (Henkel et al., 2012;Ilfergane and Henkel, 2017).
The traditional form of medicine is now also supplementing con-ventional western medicine in developed countries such as the USAand Germany, similar to how India continues to practice the Ayurvedicmedicine alongside Western medicine. According to Ayurvedic treat-ment regimen, infertile men are often given a mixture of severaldifferent plants that commonly include Mucuna pruriens (velvet bean),Withania somnifera (Indian ginseng), Tribulus terrestris (land cal-trops), Glycyrrhiza glabra (licorice), Terminalia arjuna (Arjuna tree),Phyllanthus emblica (Indian gooseberry or amla), Zingiber officinale(ginger) and Piper longum (Indian long pepper) (Samy et al., 2008).With the increasing use of complementary and alternative medi-cine, however, it is imperative to determine the efficacy and mechanismof action of such herbal supplementations.
The Center for Disease Control defines assisted reproduction tech-niques as any manipulation of both sperm and egg outside of the body
(CDC, 2007). The techniques involved include IVF, gamete intrafallopiantube transfer, zygote intrafallopian transfer, intracytoplasmic sperminjection and cryopreservation (SART, 2016). The type of assisted re-production technique used depends on the patient, and the treatmentused is based on the cause of infertility of the male, female or both,and on their own personal preferences and beliefs. The use of herbalmedicine in assisted reproduction techniques has not been as wide-spread as its use in the treatment of infertility in general. Plant-derived bioactive compounds, however, have been investigated in anumber of animal studies on cryopreservation and in humans in IVF(Mokhber Maleki et al., 2014; Sapanidou et al., 2014; Zhang et al., 2007).
The preparation of semen for assisted reproduction techniquesrequires the removal of seminal plasma, which is rich in antioxidantmolecules and enzymes. Therefore, spermatozoa, which essentiallylack their own antioxidative protection, are at an increased risk of oxi-dative damage due to oxidative stress (Agarwal et al., 2014a; Sapanidouet al., 2014). Cryopreservation of spermatozoa allows for a couple topreserve their fertility for a period of time. This technique, however,is associated with the production of ROS, which subsequently leadsto lipid peroxidation (LPO) and decreased sperm parameters (Agarwalet al., 2014b). As a result of this concern, several studies have beenconducted to determine whether the use of plant-derived antioxi-dants would improve sperm quality, such as the polyphenol-rich grapepomace extract (obtained from white grapes, species Vitis vinifera,variety Batiki Tyrnavou) and crocin (the main apocarotenoids of saffron/Crocus sativus extract) (Mokhber Maleki et al., 2014; Sapanidou et al.,2014). Grape seed extracts, which contain polyphenols, are able toneutralize ROS as can be seen in a study in which bovine sperma-tozoa were incubated with the extract and resulted in an increase inmotility and viability (Belviranli et al., 2015; Sapanidou et al., 2014).Crocin at a concentration of 1 mm caused a decrease in ROS pro-duction with subsequently lower LPO levels and increased viabilityand motility in cryopreserved bovine spermatozoa (Mokhber Malekiet al., 2014).
A human study investigated the effects of administration of aChinese herbal mixture and the subsequent results of IVF. The herbalmixture called Bushen Shengjing Decoction was administered to pa-tients with oligozoospermia and azoospermia for 2–3 months beforeICSI. Compared with the control group, the treatment group showedan increase in sperm concentration, motility and viability. In addi-tion, higher rates of fertilization and clinical pregnancy were alsoevident in the treatment group (Zhang et al., 2007). The mixture usedcontained several different herbal supplements, some of which wereshown to have antioxidant activity.
Additional studies need to be conducted to determine whether theuse of herbal supplements for assisted reproduction techniques iswarranted, and to find out what the molecular mechanisms of actionare for these supplements. It is logical to hypothesize that if suchsupplements assist with male infertility that their subsequent use withassisted reproduction techniques would also show a beneficial effect.Until such studies are conducted, it is difficult to reach a definitiveconclusion.
Withania somnifera and male infertility
Withania somnifera is commonly known as Ashwagandha in Ayurvedicmedicine, Indian ginseng, poison gooseberry or winter cherry. It is asmall evergreen shrub with long tuberous roots that belong to the
313R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6
Solanaceae (nightshade) family of plants (Figure 1). Withania somniferahas small, greenish-yellow flowers and smooth, round fruits with nu-merous seeds. This plant can be found in tropical and subtropicalareas, ranging from South Africa, Middle East India and China (Daret al., 2015). In India, Withania somnifera is grown as a medicinal crop,and either the whole plant or different parts are used for its medici-nal properties. Since antiquity, and to this day, the root of Withaniasomnifera is used as an adaptogen, diuretic, sedative, antioxidant, andaphrodisiac (Narinderpal et al., 2013). Other parts of the plant, suchas the leaves and fruits, have been used as a pain reliever, memoryenhancer, anti-neoplastic agent, anti-microbial agent, and anti-inflammatory agent (Narinderpal et al., 2013).
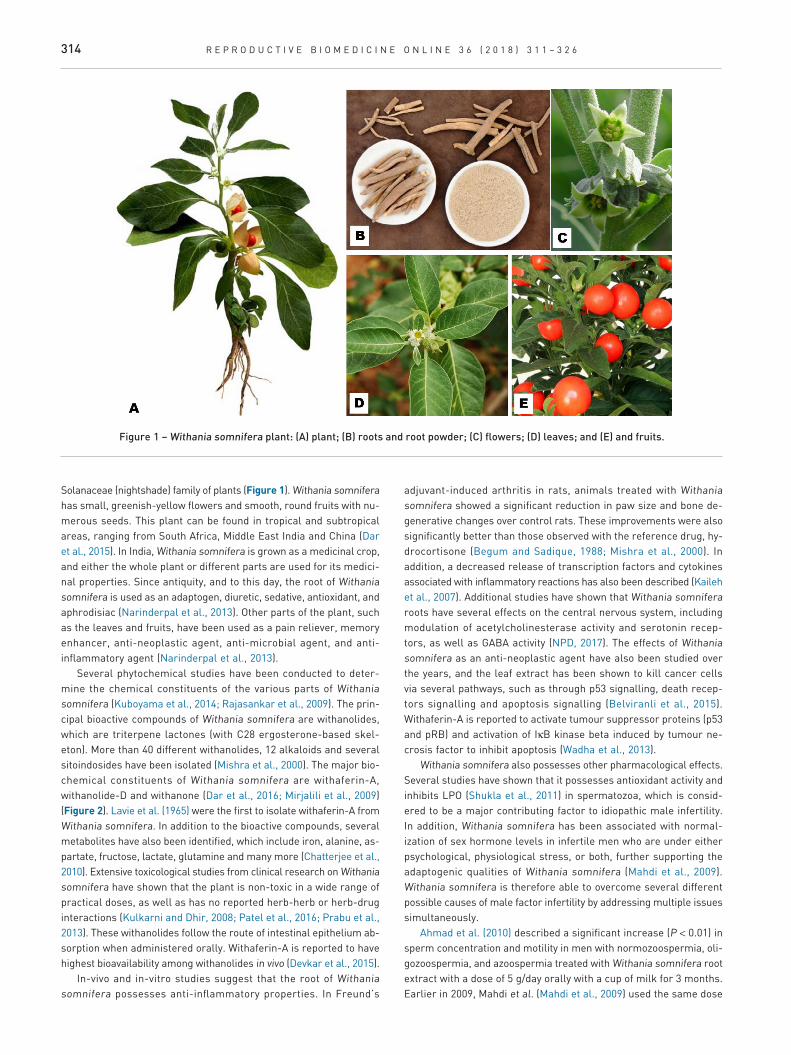
Several phytochemical studies have been conducted to deter-mine the chemical constituents of the various parts of Withaniasomnifera (Kuboyama et al., 2014; Rajasankar et al., 2009). The prin-cipal bioactive compounds of Withania somnifera are withanolides,which are triterpene lactones (with C28 ergosterone-based skel-eton). More than 40 different withanolides, 12 alkaloids and severalsitoindosides have been isolated (Mishra et al., 2000). The major bio-chemical constituents of Withania somnifera are withaferin-A,withanolide-D and withanone (Dar et al., 2016; Mirjalili et al., 2009)(Figure 2). Lavie et al. (1965) were the first to isolate withaferin-A fromWithania somnifera. In addition to the bioactive compounds, severalmetabolites have also been identified, which include iron, alanine, as-partate, fructose, lactate, glutamine and many more (Chatterjee et al.,2010). Extensive toxicological studies from clinical research on Withaniasomnifera have shown that the plant is non-toxic in a wide range ofpractical doses, as well as has no reported herb-herb or herb-druginteractions (Kulkarni and Dhir, 2008; Patel et al., 2016; Prabu et al.,2013). These withanolides follow the route of intestinal epithelium ab-sorption when administered orally. Withaferin-A is reported to havehighest bioavailability among withanolides in vivo (Devkar et al., 2015).
In-vivo and in-vitro studies suggest that the root of Withaniasomnifera possesses anti-inflammatory properties. In Freund’s
adjuvant-induced arthritis in rats, animals treated with Withaniasomnifera showed a significant reduction in paw size and bone de-generative changes over control rats. These improvements were alsosignificantly better than those observed with the reference drug, hy-drocortisone (Begum and Sadique, 1988; Mishra et al., 2000). Inaddition, a decreased release of transcription factors and cytokinesassociated with inflammatory reactions has also been described (Kailehet al., 2007). Additional studies have shown that Withania somniferaroots have several effects on the central nervous system, includingmodulation of acetylcholinesterase activity and serotonin recep-tors, as well as GABA activity (NPD, 2017). The effects of Withaniasomnifera as an anti-neoplastic agent have also been studied overthe years, and the leaf extract has been shown to kill cancer cellsvia several pathways, such as through p53 signalling, death recep-tors signalling and apoptosis signalling (Belviranli et al., 2015).Withaferin-A is reported to activate tumour suppressor proteins (p53and pRB) and activation of IκB kinase beta induced by tumour ne-crosis factor to inhibit apoptosis (Wadha et al., 2013).
Withania somnifera also possesses other pharmacological effects.Several studies have shown that it possesses antioxidant activity andinhibits LPO (Shukla et al., 2011) in spermatozoa, which is consid-ered to be a major contributing factor to idiopathic male infertility.In addition, Withania somnifera has been associated with normal-ization of sex hormone levels in infertile men who are under eitherpsychological, physiological stress, or both, further supporting theadaptogenic qualities of Withania somnifera (Mahdi et al., 2009).Withania somnifera is therefore able to overcome several differentpossible causes of male factor infertility by addressing multiple issuessimultaneously.
Ahmad et al. (2010) described a significant increase (P < 0.01) insperm concentration and motility in men with normozoospermia, oli-gozoospermia, and azoospermia treated with Withania somnifera rootextract with a dose of 5 g/day orally with a cup of milk for 3 months.Earlier in 2009, Mahdi et al. (Mahdi et al., 2009) used the same dose
Figure 1 – Withania somnifera plant: (A) plant; (B) roots and root powder; (C) flowers; (D) leaves; and (E) and fruits.
314 R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6
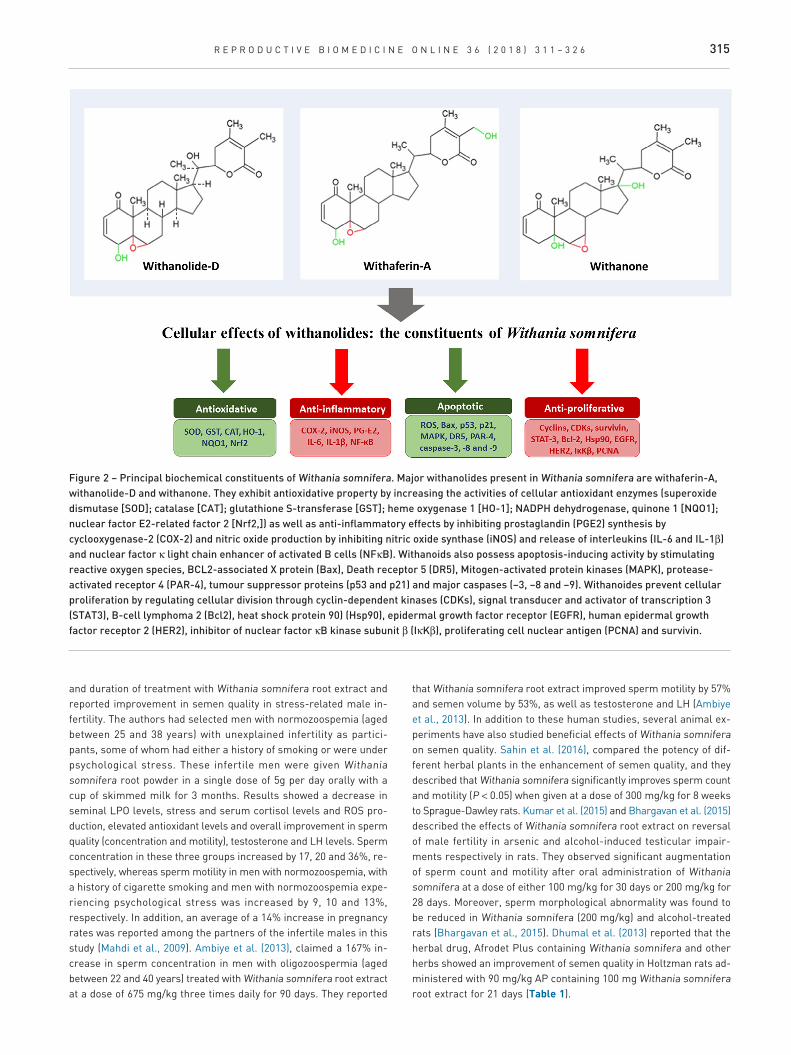
and duration of treatment with Withania somnifera root extract andreported improvement in semen quality in stress-related male in-fertility. The authors had selected men with normozoospemia (agedbetween 25 and 38 years) with unexplained infertility as partici-pants, some of whom had either a history of smoking or were underpsychological stress. These infertile men were given Withaniasomnifera root powder in a single dose of 5g per day orally with acup of skimmed milk for 3 months. Results showed a decrease inseminal LPO levels, stress and serum cortisol levels and ROS pro-duction, elevated antioxidant levels and overall improvement in spermquality (concentration and motility), testosterone and LH levels. Spermconcentration in these three groups increased by 17, 20 and 36%, re-spectively, whereas sperm motility in men with normozoospemia, witha history of cigarette smoking and men with normozoospemia expe-riencing psychological stress was increased by 9, 10 and 13%,respectively. In addition, an average of a 14% increase in pregnancyrates was reported among the partners of the infertile males in thisstudy (Mahdi et al., 2009). Ambiye et al. (2013), claimed a 167% in-crease in sperm concentration in men with oligozoospermia (agedbetween 22 and 40 years) treated with Withania somnifera root extractat a dose of 675 mg/kg three times daily for 90 days. They reported
that Withania somnifera root extract improved sperm motility by 57%and semen volume by 53%, as well as testosterone and LH (Ambiyeet al., 2013). In addition to these human studies, several animal ex-periments have also studied beneficial effects of Withania somniferaon semen quality. Sahin et al. (2016), compared the potency of dif-ferent herbal plants in the enhancement of semen quality, and theydescribed that Withania somnifera significantly improves sperm countand motility (P < 0.05) when given at a dose of 300 mg/kg for 8 weeksto Sprague-Dawley rats. Kumar et al. (2015) and Bhargavan et al. (2015)described the effects of Withania somnifera root extract on reversalof male fertility in arsenic and alcohol-induced testicular impair-ments respectively in rats. They observed significant augmentationof sperm count and motility after oral administration of Withaniasomnifera at a dose of either 100 mg/kg for 30 days or 200 mg/kg for28 days. Moreover, sperm morphological abnormality was found tobe reduced in Withania somnifera (200 mg/kg) and alcohol-treatedrats (Bhargavan et al., 2015). Dhumal et al. (2013) reported that theherbal drug, Afrodet Plus containing Withania somnifera and otherherbs showed an improvement of semen quality in Holtzman rats ad-ministered with 90 mg/kg AP containing 100 mg Withania somniferaroot extract for 21 days (Table 1).
Figure 2 – Principal biochemical constituents of Withania somnifera. Major withanolides present in Withania somnifera are withaferin-A,withanolide-D and withanone. They exhibit antioxidative property by increasing the activities of cellular antioxidant enzymes (superoxidedismutase [SOD]; catalase [CAT]; glutathione S-transferase [GST]; heme oxygenase 1 [HO-1]; NADPH dehydrogenase, quinone 1 [NQO1];nuclear factor E2-related factor 2 [Nrf2,]) as well as anti-inflammatory effects by inhibiting prostaglandin (PGE2) synthesis bycyclooxygenase-2 (COX-2) and nitric oxide production by inhibiting nitric oxide synthase (iNOS) and release of interleukins (IL-6 and IL-1β)and nuclear factor κ light chain enhancer of activated B cells (NFκB). Withanoids also possess apoptosis-inducing activity by stimulatingreactive oxygen species, BCL2-associated X protein (Bax), Death receptor 5 (DR5), Mitogen-activated protein kinases (MAPK), protease-activated receptor 4 (PAR-4), tumour suppressor proteins (p53 and p21) and major caspases (−3, −8 and −9). Withanoides prevent cellularproliferation by regulating cellular division through cyclin-dependent kinases (CDKs), signal transducer and activator of transcription 3(STAT3), B-cell lymphoma 2 (Bcl2), heat shock protein 90) (Hsp90), epidermal growth factor receptor (EGFR), human epidermal growthfactor receptor 2 (HER2), inhibitor of nuclear factor κB kinase subunit β (IκKβ), proliferating cell nuclear antigen (PCNA) and survivin.
315R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6
Table 1 – Human and animal studies that investigated the effect of Withania somnifera on semen quality improvement.
Study Study model Fertility status of model used Details of treatment Effect on semen quality Reference
Withania somnifera root extract onspermatogenic activity
Human Oligozoospermic (sperm count <20 ×106/ml)
675 mg/day in three doses for 90 days(n = 46)
Increase in sperm count, semen volume andsperm motility (P < 0.0001) on day 90 frombaseline.
Ambiye et al., 2013
Withania somnifera root powder onsemen quality in infertile men withnormozoospermia who were ‘understress’
Human Normozoospermic with eitheridiopathic infertility, underpsychological stress, or a history ofcigarette smoking
5 g/day orally for 3 months with a cupof skimmed milk (n = 20) for eachgroup)
In infertile men with normozoospermia,increase in sperm concentration comparedwith pre-treatment values (P < 0.01).In men with normozoospermia underpsychological stress, increase in spermconcentration (P < 0.01) and motility (P < 0.05)compared with pre-treatment values. In menwith normozoospermia who were cigarettesmokers, increase in sperm concentrationand motility (P < 0.05, respectively) comparedwith pre-treatment values.
Mahdi et al., 2009
Withania somnifera root extract onsemen quality in infertile men
Human Infertile men with eithernormozoospermia (sperm count >20 ×106/ml; motility >40%; normalmorphology >40%), oligozoospermia(sperm count <20 × 106/ml; motility>40%; normal morphology >40%), orasthenozoospermia (sperm count >20× 106/ml; motility <40%; normalmorphology >40%)
5 g/day orally for 3 months with a cupof milk (n = 25 for each group)
Semen volume increased in men withnormozoospermia and oligozoospermiacompared with pre-treatment values (P <0.01). Sperm concentration, motility andsperm count per ejaculate increasedsignificantly in men with normozoospermia,oligozoospermia, and asthenozoospermiacompared with pre-treatment values (P <0.01).
Ahmad et al., 2010
Ameliorative effect of Withaniasomnifera ethanolic root extract onmale reproductive system in arsenicinduced infertility
Charles Foster rats Arsenic (8 mg/kg for 45 days); inducedtesticular impairment
100 mg/kg/day orally for 30 days (n =24)
Sperm count and motility improvedsignificantly (P < 0.001; n = 6) compared withcontrol.
Kumar et al., 2015
Ethanolic Withania somnifera rootextract on reversal of semen qualityin alcohol-induced infertility
Wistar rats Alcohol-induced testicular impairment 200 mg/kg orally for 28 days Withania somnifera increased sperm count (P< 0.05) compared with control levels. Withaniasomnifera improved sperm motility (P < 0.01)and reduced sperm morphologicalabnormality (P < 0.05) in alcohol-treated rats.
Bhargavan et al., 2015
Methanol-water (70:30) Withaniasomnifera root extract on semenquality improvement compared withother herbal plants
Sprague–Dawley rats Normal rats treated with differentherbal plants
300 mg/kg orally for 8 weeks (n = 7) Withania somnifera significantly improvedsperm count (P < 0.05)
Sahin et al., 2016
Withania somnifera contained inAfrodet plus tablet on male fertility
Holtzman rats Normal adult male rats treated withAfrodet plus
90 or 180 mg/kg of Afrodet pluscontaining 100 mg Withania somniferaroot extract for 21 days
Withania somnifera (at both 90 and 180 mg/kgdoses) contained in Withania somnifera tabletimproved sperm count (P < 0.05).
Dhumal et al., 2013
316R
EP
RO
DU
CT
IVE
BIO
ME
DIC
INE
ON
LIN
E3
6(2
01
8)
31
1–
32
6

Mechanism of action of Withania somnifera
The mechanisms by which Withania somnifera is able to exert itseffects on the reproductive system and fertility can be broadly dividedinto oxidative and non-oxidative mechanisms. The oxidative mecha-nism involves modulation of antioxidant activity, along with theregulation of antioxidant enzymes and the co-factors required for theproper functioning of antioxidant enzymes. The non-oxidative mecha-nisms mainly include the effect of Withania somnifera on thehypothalamic-pituitary-gonadal (HPG) axis, as well as its anti-stress activities via the hypothalamic-pituitary-adrenal (HPA) axis. Onadministration, Withania somnifera extract is metabolized to its major
constituents: withaferin-A, withanolide-D, withanone and otherwithanolide derivatives. These biochemical constituents either act di-rectly on testicular or other male reproductive cells, or indirectly onendocrine homeostasis to improve male fertility. On the basis of thesefindings, the postulated general mechanism of action of Withaniasomnifera is presented in Figure 3.
Oxidative mechanisms
Reactive oxygen species are highly reactive compounds that have oneor more unpaired electrons (Griveau and Lannou, 1997) with half-
Figure 3 – The proposed mechanism of action of Withania somnifera. This herb improves both sperm quality as well as the reproductivehormonal profile by acting through direct and indirect pathways, respectively. In the direct oxidative defense pathway, Withania somniferareduces oxidative stress and improves the antioxidant potential of seminal plasma; whereas through the indirect antioxidant defensepathway, Withania somnifera prevents the stress induced cortisol-mediated decrease in testosterone level, as well as exerts an inhibitoryaction of prolactin on sperm production. These mechanisms normalize the male reproductive hormone levels and improve spermparameters to enhance male fertility. (The green arrows indicate an increase whereas the red arrows indicate a decrease). ACTH,adrenocorticotropic hormone; CAT, catalase; CRH, corticotropin-releasing hormone; GABA, gamma-aminobutyric acid; GnRH,gonadotrophin-releasing hormone; HPA, hypothalamic–pituitary–adrenal; HPG, hypothalamic-pituitary-gonadal; ROS, reactive oxygenspecies; SOD, superoxide dismutase; PRL, prolactin. (For interpretation of the references to colour in this figure legend, the reader isreferred to the Web version of this article.)
317R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6

lives in the nano- to milli-second range. Although molecular oxygenis chemically a di-radical, it is relatively inert, but reacts in certainphysiological processes with organic molecules and thus forms ROS.In normal physiological processes, energy is produced in the mito-chondria through the oxidation of biological molecules, which requireoxygen as a terminal electron acceptor. In the male germ cell, asperm-specific oxidoreductase, dependent on nicotinamide adeninedinucleotide phosphate-oxidase, is located in the midpiece of the fla-gellum (Gavella and Lipovac, 1992). A major part of ROS productionoccurs because of disruption and subsequent leakage of electronsfrom the mitochondrial electron transfer chain from Complex I or III(Finkel and Holbrook, 2000; Koppers et al., 2008). Even under normalphysiological aerobic conditions, about 1–5% of the consumed oxygenis converted into free radicals (Boveris and Chance, 1973; Chance et al.,1979), which is an unavoidable consequence of metabolism. The pro-duction of ROS via this mechanism are regarded as cytotoxicbyproducts that are involved in the cause of disease and ageing (Rahaand Robinson, 2000). Superoxide anions, which are a type of ROS,dismutate to hydrogen peroxide (Sharma and Agarwal, 1996). Hy-drogen peroxide is an oxidant that has been associated with maleinfertility since the 1940s, when John MacLeod (1943) observed a de-crease in motility when spermatozoa were incubated under high oxygentension. A small and controlled concentration of ROS, however, is re-quired for normal sperm function as ROS are also important mediatorsof signal transduction that lead to hyperactivation, capacitation andacrosome reaction (de Lamirande et al., 1997). Therefore, a deli-cate balance between ROS (oxidation) and ROS scavenging enzymesand antioxidants (reduction) must be maintained to prevent damageto the spermatozoa. This physiological damage leading to dysfunc-tion of the male germ cell is a result of the plasma membranecontaining an extraordinarily high amount of polyunsaturated fatty acids(Parks and Lynch, 1992). Elevation of ROS has been associated withdecreased sperm motility owing to cellular depletion of adenosine py-rophosphate, cellular membrane damage via LPO, and DNA damage(Agarwal et al., 2014a). In addition, ROS can directly oxidize and damagethe sperm DNA (Agarwal et al., 2014a), and also the end products ofLPO, such as malondialdehyde, 4-hydroxy-2-alkenals or 2-alkenalsare also genotoxic and mutagenic (Luczaj and Skrzydlewska, 2003).
To combat the deleterious effects of ROS, seminal plasma con-tains numerous enzymatic and non-enzymatic antioxidants (Agarwalet al., 2004). In addition, spermatozoa have, to a limited extent, an-tioxidant enzymes, including superoxide dismutase (SOD), catalaseas well as glutathione peroxidase (Agarwal et al., 2014a). Each of theenzymes have distinct functions: SOD functions by converting super-oxide anions into hydrogen peroxide and oxygen, catalase causes thedismutation of hydrogen peroxide into oxygen and water, and gluta-thione peroxidase reduces hydrogen and lipid hydroperoxides viaglutathione as an electron donor (Harris, 1992). The non-enzymaticantioxidants include substances such as ascorbic acid, alpha-tocopherol, pyruvate and glutathione (Zini and Al-Hathal, 2011).
Reactive oxygen species that are present in seminal plasmaemanate from various sources, some of which are endogenous,whereas others are exogenous. The main endogenous sources includeneutrophils, macrophages and immature spermatozoa. Exogenoussources encompass mostly environmental and lifestyle factors, suchas smoking, alcohol and radiation (Agarwal et al., 2014a). There-fore, potential treatment for male infertility owing to oxidative stressmust address the ROS themselves and the underlying cause of theirproduction. If the causes of the oxidative stress cannot be altered,however, then the treatment must be able to at least buffer it.
Several studies have looked at the effects of oral antioxidantsupplements and their effects on male factor infertility (Gharagozlooand Aitken, 2011). Simply using antioxidants, however, may not al-leviate the problem because the cause is not always known. In addition,considering that the specific balance between oxidation and reduc-tion is essential for normal sperm function, an oversupply ofantioxidants would lead to so-called ‘reductive stress’, which is asdangerous for cells and organs as oxidative stress (Castagné et al.,1999; Henkel and Solomon, 2017). This paradoxical phenomenon iscalled the ‘antioxidant paradox’, a term that was coined by Halliwell(2000). On this basis, researchers have begun to look at herbal supple-ments for the treatment of male-factor infertility.
Studies reporting the relationship between Withania somniferatreatment and oxidative parameters are presented in Table 2. Semenfrom infertile men has been found to contain decreased antioxidantactivity. For example, one of our recent studies has established thecut-off value of total antioxidant capacity of 1947 µM in seminal plasmathat can diagnose infertile males with oxidative stress (Roychoudhuryet al., 2016). Decreased antioxidant activity occurs when concentra-tions of antioxidants or functional antioxidative enzymes decrease;dysfunctional enzymes increase; or the amount of ROS increase, whichoverwhelms the natural antioxidant capacity. As mentioned, the rootpowder of Withania somnifera (5g/day), when administered daily toinfertile men with normozoospermia for 3 months, had decreased ROSproduction in the seminal plasma and improved sperm count (Shuklaet al., 2011). In several studies investigating the effects of Withaniasomnifera on semen quality in infertile males, enzymatic antioxi-dant activity was determined by measuring LPO and protein carbonylgroups in seminal plasma, which indirectly depicts the enzymatic ac-tivity of SOD and catalase. Compared with pretreatment, the amountof LPO was found to decrease after administration of Withaniasomnifera (Ahmad et al., 2010; Mahdi et al., 2009; Shukla et al., 2011),which is most likely attributed to a synergistic relationship betweenthe increase in the enzymatic activity of SOD and catalase and theinnate antioxidant activity of Withania somnifera. Therefore, com-pounds of the Withania somnifera extract are able to donate electronsand halt the destructive chain reaction of free radicals, thereby low-ering the overall ROS burden (Mishra et al., 2000).
In addition to the reduction in LPO seen in infertile men treatedwith Withania somnifera, several studies investigated the concen-tration of metals ions such as arsenic (Kumar et al., 2015), copper,zinc, iron and gold in seminal plasma, and how they were altered byWithania somnifera treatment. Zinc in conjunction with copper is re-quired as co-factors for SOD, whereas catalase and glutathioneperoxidase require iron and selenium, respectively (Shukla et al., 2011).Although gold does not participate directly with antioxidant enzymes,gold treatment has been shown to improve steroidogenesis and ga-metogenesis in immature Wistar rats. When gold chloride was injectedsub-cutaneously at a dose of 0.5 mg/kg body weight per day into im-mature rats for 26 days, plasma levels of testosterone were foundto be significantly elevated from baseline, which led researchers toconclude that this treatment is associated with a stimulatory effecton testicular function (Biswas et al., 2004). On this basis, Shukla et al.(2011) investigated the effects of Withania somnifera on combatingoxidative stress and cell death in spermatozoa, and its effects on theessential metal (copper, zinc, iron and gold) concentrations withinseminal plasma of infertile men (Shukla et al., 2011). Therefore, itis reasonable to conclude that the root extract of Withania somniferacan exert its antioxidant activity via the supplementation of co-factors that are required for the proper functioning of antioxidant
318 R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6

Table 2 – Studies that investigated the relationship between Withania somnifera (root powder given at a dose of 5 g/day for 3 months) and either pro-oxidants or antioxidants.
Study Fertility status ofparticipants
Age of theparticipants
Number of participants Results Reference
Withania somnifera effect onintracellular ROS
Normozoospermic;oligozoospermic;asthenozoospermic
Not mentioned n = 75;normozoospermic: 25; oligozoospermic:25; asthenozoospermic: 25
ROS generation was diminished in men withnormozoospermia (32.56% decrease; P < 0.05),oligozoospermia (49.76% decrease; P < 0.01) andasthenozoospermia (44.33% decrease; P < 0.01) comparedwith pretreatment.
Shukla et al., 2011
Withania somnifera and ROS inseminal plasma
Normozoospermic butinfertile
25–38 years Control (n = 60);treated group (n = 60) divided into threesub-groups:normozoospermic: 20; underpsychological stress: 20; smoker: 20;unknown cause
LPO in seminal plasma of infertile men, men withnormozoospermia who are cigarette smokers and men withnormozoospermia under psychological stress decreased by29, 27, 23% respectively, compared with baseline
Mahdi et al., 2009
Normozoospermic,oligozoospermic;asthenozoospermic
Not mentioned Control (n = 75);treated group (n = 75) divided into threesub-groups:normozoospermic: 25, oligozoospermic:25, asthenozoospermic: 25
LPO and protein carbonyl groups in seminal plasma aftertreatment reversed in men with normozoospermia,oligozoospermia, and asthenozoospermia (P < 0.01).
Ahmad et al., 2010
Withania somnifera andantioxidant vitamins
Normozoospermic;oligozoospermic
Not mentioned Control (n = 75Treated group (n = 75) divided into threesub-groups:normozoospermic: 25, oligozoospermic:25, asthenozoospermic: 25
Levels of vitamins A, E and C were reduced in all infertile menbefore and after treatment levels recovered in men withnormozoospermia (P < 0.01), oligozoospermia (P < 0.01) andasthenozoospermia (P < 0.01).
Ahmad et al., 2010
Withania somnifera andessential metalconcentration
Normozoospermic;oligozoospermic;asthenozoospermic
Not mentioned n = 75normozoospermic: 25, oligozoospermic:25, asthenozoospermic: 25
Increased the seminal plasma concentrations of Cu2+, Zn2+,Fe2+ and Au2+ in infertile men with normozoospermia (P <0.01), oligozoospermia (P < 0.01) and Fe2+, Zn2+ and Au2+ andasthenozoospermia (P < 0.01).
Shukla et al., 2011
Withania somnifera andantioxidant enzymes inseminal plasma of infertilemen
Normozoospermic butinfertile
25–38 years Control (n = 60);treated group (n = 60) divided into threesub-groups:normozoospermic: 20 under psychologicalstress, 20 under smoking, 20 underunknown cause
SOD activity in seminal plasma of men withnormozoospermia, men with normozoospermia who smoke,and men with normozoospermia under psychological stressby 8, 18 and 17%, and catalase activity by 6, 3 and 11%,respectively, compared with the pretreatment parameters.
Mahdi et al., 2009
Normozoospermic;oligozoospermic;asthenozoospermic
Not mentioned Control (n = 75); treated group (n = 75)divided into three sub-groups:normozoospermic; 25, oligozoospermic:25, asthenozoospermic: 25
SOD activity in fertile control group was 8.17 0.71 U/mgprotein, and significantly decreased (P < 0.01) in men withnormozoospermia, oligozoospermia and asthenozoospermia.Post-treatment levels increased significantly (P < 0.05)compared with controls.
Ahmad et al., 2010
Catalase activity in men with normozoospermia,oligozoospermia and infertile men with asthenozoospermiawas significantly increased after treatment (P < 0.01).
LPO, lipid peroxidation; ROS, reactive oxygen species; SOD, super oxide dismutase.
319R
EP
RO
DU
CT
IVE
BIO
ME
DIC
INE
ON
LIN
E3
6(2
01
8)
31
1–
32
6

enzymes. Hence, the ability of Withania somnifera root extract to de-crease ROS and oxidative stress experienced by spermatozoa can besurmised to stem from two mechanisms: its potent antioxidant ac-tivity as well as its ability to enhance antioxidant enzymes via thesupplementation of required co-factors (depicted as the direct effectin Figure 3).
Non-oxidative mechanisms
Apart from oxidative stress, other causes, such as hormonal imbal-ance caused by physiological or psychological causes, are also linkedto male infertility. Stress-related hormones, in particular glucocor-ticoids, have a deleterious effect on the hypothalamic–pituitary–gonadal (HPG) axis and subsequently on spermatogenesis (Chandraet al., 2012). Gonadotrophin-releasing hormone (GnRH) from the hy-pothalamus stimulates the anterior pituitary to release FSH and LH.They both subsequently act on the gonads, regulating spermatogen-esis and testosterone production. Therefore, when the HPG axis isdisrupted by hormones, such as gonadotrophin-inhibiting hormone,prolactin (PRL) and cortisol, spermatogenesis is negatively affected(Nargund, 2015). As Withania somnifera root extract is considered tobe an adaptogen, it is able to promote homeostasis within the body,by decreasing the stress response, and normalizing the levels of cor-tisol, thereby alleviating infertility to some extent. The adaptogenicqualities of Withania somnifera were demonstrated in a study thatanalysed its effects on infertile men with normozoospermia, who wereunder psychological, environmental stress (heavy smokers) or hadinfertility of unknown cause. The root powder of Withania somnifera,when administered for 3 months at a dosage of 5g per day withskimmed milk, resulted in a decrease in morning and afternoon levelsof cortisol in the experimental groups when compared with pretreat-ment levels (Mahdi et al., 2009). The normalization of the cortisol levelsin the treatment group was also accompanied by an increase in tes-tosterone and LH levels along with a decrease in FSH and PRL (Mahdiet al., 2009). These hormonal profiles were comparable to those ofthe fertile males. In addition, the above study measured pregnancyoutcomes in individuals treated with Withania somnifera, and re-vealed an average increase of 14% compared with controls. An earliersimilar study that analysed the reproductive hormonal profiles of in-fertile men after treatment with Withania somnifera root powder ata dose of 5g per day for 3 months with milk showed an increase inthe levels of testosterone and LH with an accompanying decrease inFSH and PRL (Ahmad et al., 2010). These results demonstrate thatWithania somnifera can regulate the levels of serum sex hormonesthrough manipulation of the HPG axis, thereby enhancing fertility(Table 3).
The augmentation of the HPA and the HPG axis may take placeeither at the adrenal cortex, gonads, pituitary or hypothalamic levels.Several studies have shown that Withania somnifera root powder ex-hibits its effect at the hypothalamic level (Bhattarai et al., 2010; Daret al., 2016; Kataria et al., 2015; Ray and Jha, 2001). Regulation atother sites, however, has not been analysed, and therefore cannotbe excluded. To study the effect that Withania somnifera exerts onthe hypothalamus, Kataria et al. (2015) used GnV-3 cells which areneuronal cells from GnRH clonal cell line derived from rat hypotha-lamic cells. These investigators were able to demonstrate that aqueousextract of Withania somnifera leaves stimulated GnRH neuronal ac-tivity via differentiation and upregulation of the release of GnRH (Kataria
et al., 2015). They hypothesized that an increase in GnRH neuronalactivity was caused by Withania somnifera’s GABA-mimetic activity.This hypothesis was confirmed by subsequent in-vitro studies withmice brain hypothalamic slices by the same group. Methanolic extractof Withania somnifera was shown to affect GnRH neuronal activitiesby activating GABAA receptors via direct interaction with the mem-brane, rather than through action potential-mediated mechanisms.Therefore, this extract was able to exhibit GABA-mimetic action viainteraction with the GABAA receptors. These receptors are ligand-gated Cl– channels that activate Cl– currents in GnRH neurons whenbound to GABA (Bhattarai et al., 2010). Although GABA is most com-monly considered to be an inhibitory neurotransmitter in the centralnervous system, most mature GnRH neurons showed an unusual char-acteristic, in that they are excited by GABA activation (DeFazio et al.,2002; Watanabe et al., 2014). Therefore, one could conclude thatWithania somnifera exerts its effects via regulation of GnRH neuronswithin the hypothalamus and stimulates its release, thereby induc-ing the production of downstream hormones such as LH, FSH andtestosterone. In addition, although whole root or leaf extracts wereused in these experiments, it is believed by many that the majorbioactive compounds within the plant are Withaferin A (Ray and Jha,2001) and Withanone (Dar et al., 2016).
If Withania somnifera root extract does in fact exert its effects atthe level of the hypothalamus, it would support the results that wereseen in the previous studies that reported a normalization of pitu-itary as well as gonadal hormones (Nargund, 2015). By normalizingthe pulsatile nature of GnRH, all downstream hormones would bealtered as well, leading to increased fertility (depicted as the indi-rect effect in Figure 3). In-vivo studies, however, need to be conductedto truly understand the complex mechanisms by which Withaniasomnifera functions to improve the fertility of infertile men.
Thus far, our discussion has mainly focused on sperm quality pa-rameters and hormonal balance. An additional topic that needs to beaddressed to fully comprehend the various components that inter-act with one another to aid in reproduction is the seminal plasma.Semen consists of spermatozoa that are suspended in a fluid calledthe seminal plasma. Seminal plasma is secreted by the seminalvesicles, prostate and bulbo-urethral glands. The various compo-nents of seminal plasma facilitate sperm function (Juyena and Stelletta,2012). Numerous chemical components make up seminal plasma andinclude inorganic ions, albumin, enzymes, hormones and peptides(Gershbein and Thielen, 1988). As the seminal plasma is intimatelyassociated with spermatozoa, it is safe to assume that its compo-nents have a direct effect on the viability of spermatozoa. Themetabolites of seminal plasma of fertile and infertile men have beenassessed in a number of studies, and several differences have beenhighlighted (Gershbein and Thielen, 1988). In infertile patients, theactivities of the enzymes alanine aminotransferase, lactate dehydro-genase (LDH) and isocitrate dehydrogenase were significantlydecreased compared with fertile men. In addition to the decline inthe above-mentioned enzymes, the following compounds were alsofound to decrease; glycerophosphocholine, citrate, glutamate, alanineand histidine. Levels of phenylalanine, however, were elevated in in-fertile men compared with fertile men (Gupta et al., 2013).
On the basis of these differences in the metabolites of fertile andinfertile men, Gupta et al. (2013) endeavoured to determine the ef-ficacy of Withania somnifera on seminal plasma metabolites of infertilemen by using high-resolution proton nuclear magnetic resonance spec-troscopy (Gupta et al., 2013). In their study, infertile men were treatedwith 5g per day of powdered Withania somnifera root extract for 3
320 R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6

Table 3 – Studies that investigated the relationship between Withania somnifera (root powder given at a dose of 5 g/day for 3 months) and reproductive hormone profile.
HormonesStudied
Fertility status ofparticipants
Age of theparticipants
Number of participants Results Reference
SerumTestosterone
Normozoospermic butinfertile
25–38 years Control (n = 60)Treated group (n = 60) divided into threesub-groups:normozoospermic: 20; under psychologicalstress: 20; smoker; 20; unknown cause
Pre-treatment serum T decreased among infertile men withnormozoospermia by 10% among; men with normozoospermiawho smoke by 8% and among men with normozoospermia whoare under stress by 14%. Post-treatment serum T improved by13%, 10% and 22%, respectively.
Mahdi et al., 2009
Normozoospermic;oligozoospermic;asthenozoospermic
Not mentioned Control (n = 75);treated group (n = 75) divided into threesub-groups:normozoospermic: 25; oligozoospermic: 25;asthenozoospermic: 25
Serum T post-treatment in men with normozoospermia,asthenozoospermic and oligozoospermia recovered significantly(P < 0.01) compared with pre-treatment levels.
Ahmad et al., 2010
Serum LH Normozoospermic butinfertile
25–38 years Control (n = 60);Treated group (n = 60) divided into threesub-groups:normozoospermic: 20; under psychologicalstress: 20; smoker: 20; unknown cause
Pre-treatment LH levels low: in men with normozoospermia whoare infertile 11%; in men with normozoospermia who smoke 16%;and in men with normozoospermia who are under stress 21%.Post-treatment LH increased by 5%, 14% and 22%, respectively.
Mahdi et al., 2009
Normozoospermic;oligozoospermic;asthenozoospermic
Not mentioned Control (n = 75);treated group (n = 75) divided into threesub-groups:normozoospermic: 25, oligozoospermic: 25,asthenozoospermic: 25
Serum LH after treatment in men with normozoospermia,asthenozoospermia and oligozoospermia recovered significantly(P < 0.01) compared with pre-treatment levels.
Ahmad et al., 2010
Serum prolactin Normozoospermic butinfertile
25–38 years Control (n = 60); treated group (n = 60) divided intothree sub-groups:normozoospermic: 20 under psychological stress,20 under smoking, 20 under unknown cause.
Pre-treatment prolactin levels in infertile men withnormozoospermia, men with normozoospermia who smoke; andmen with normozoospermia who are under stress was elevatedby 12, 17 and 20%. Post-treatment levels decreased by 12.5%
Mahdi et al., 2009
Normozoospermic;oligozoospermic;asthenozoospermic
Not mentioned Control (n = 75);treated group (n = 75) divided into threesub-groups:normozoospermic: 25; oligozoospermic: 25;asthenozoospermic 25.
Serum prolactin levels in men with oligozoospermia andasthenozoospermia were significantly greater then the controlgroup of fertile men; after treatment prolactin levels in men witholigozoospermia and men with asthenozoospermia significantdecreased (P < 0.05) compared with before treatment.
Ahmad et al., 2010
Serum FSH Normozoospermic butinfertile
25–38 years Control (n = 60);treated group (n = 60) divided into threesub-groups:normozoospermic: 20; under psychologicalstress: 20; smoker: 20 unknown cause.
Pre-treatment prolactin levels in infertile men withnormozoospermia, men with normozoospermia who smoke andmen with normozoospermic who are experiencing stress waselevated by 8, 10, 13%. Post-treatment prolactin levels decreasedby 9.5%.
Mahdi et al., 2009
Normozoospermic;oligozoospermic;asthenozoospermic
Not mentioned Control (n = 75); treated group (n = 75) divided intothree sub-groups:normozoospermic: 25; oligozoospermic: 25;asthenozoospermic: 25.
Serum FSH levels in men with oligozoospermia andasthenozoospermia were significantly greater than the controlgroup of fertile men; after treatment, FSH levels in theoligozoospermic and asthenozoospermic groups significantlydecreased (P < 0.05) compared with before treatment.
Ahmad et al., 2010
321R
EP
RO
DU
CT
IVE
BIO
ME
DIC
INE
ON
LIN
E3
6(2
01
8)
31
1–
32
6

months. The semen was then analysed for spermatozoa quality pa-rameters as well as for lactate, alanine, glutamate, glutamine, citrate,lysine, choline, glycerophosphocholine, glycine, tyrosine, histidine, phe-nylalanine and uridine concentrations. Results of these, along withthat of parameters such as sperm concentration and motility, and lipidperoxide and hormonal levels, were used to appraise the infertilitylevels of each patient before and after treatment. These metabolitesalso provided a measurement of the enzymatic activities of alaninetransaminase, aspartate transaminase, lactate dehydrogenase andisocitrate dehydrogenase, as the metabolites are the product of theenzymatic reactions. In their study, Gupta et al. (2013) were able todetermine that, after treatment, levels of the above metabolites shiftedtowards the concentration present in fertile males and suggested thatWithania somnifera can be used as an empirical treatment for theclinical management and treatment of infertility. For example, an in-crease in lactate concentration after treatment can be attributed tothe substantial amount of lactate and LDH that is found in the rootsof Withania somnifera (Chatterjee et al., 2010). Lactate is the productof a LDH-controlled reaction. It has been shown that a decrease inits enzymatic activity is associated with a decrease in sperm motilityand viability (Gershbein and Thielen, 1988). Although the research-ers were able to demonstrate that treatment with Withania somniferaaltered the composition of seminal plasma substrates and enzymes,the significance of this is not fully understood. Therefore, additionalresearch into how the various substrates and enzymes factor into theoverall picture of male reproduction would aid clinicians in develop-ing treatments for infertility and assisted reproduction techniques.
Withania somnifera reportedly increases the concentrations of es-sential metals (copper, zinc, iron and gold), which may enhance theprocess of testicular steroidogenesis to synthesize more testoster-one to stimulate testicular germ cell development by spermatogenesis(Shukla et al., 2011). Withania somnifera also improves the concen-trations of lactate, citrate, alanine, histidine and phenylalanine inseminal plasma, which may play significant roles in spermatozoa me-tabolism as well as spermatogenesis.
Amelioration of modifiable risk factors-induced maleinfertility
Male-factor infertility, solely accounting for 20–30% of infertility casesand a contributory factor in one-half of the overall infertility cases,behooves clinicians to counsel their patients in various lifestyle modi-fications that may aid in restoring fertility (Agarwal et al., 2015). Severalenvironmental and lifestyle factors have been observed to play a rolein male-factor infertility (Sengupta, 2013). Associated exposure to ciga-rette smoke, psychological stress, mobile phone usage and elevatedbody mass index (BMI) have been studied with relation to semen quality(Jurewicz et al., 2014). When obese men were compared with averagemen, the former were shown to have a threefold higher incidence ofinfertility. A BMI above 25 kg/m2 was subsequently associated with a25% reduction in both sperm count and motility (Jurewicz et al., 2014).In addition, a meta-analysis that analysed the effect tof BMI on re-productive hormones in males found a negative relationship betweentestosterone, sex hormone binding globin and free testosterone withelevated BMI (MacDonald et al., 2010). It can be extrapolated fromthese data that the higher the BMI of an individual, the greater thedecrease in sperm parameters and subsequently in fertility. There-fore, as with many other disease states, the simple act of increasing
physical activity and decreasing ones’ weight can lead to improvedfertility and decrease need for subsequent treatment. Cigarette smokingand its association with male infertility has been extensively studiedover the years. Results, however, have been contradictory where someresearchers show a negative association with sperm parameters andothers do not (Harlev et al., 2015). Smoking has been associated withan increase in ROS and leukocytospermia, both of which have beenassociated with male infertility (MacDonald et al., 2010). Cessation ofsmoking is therefore expected to aid in decreasing the oxidative stressand in improving sperm quality, and may improve fertility. Anotherfactor that should be addressed when dealing with male infertility ispsychological stress, which has been shown to affect spermatogen-esis mainly by altering testosterone levels via the HPA–HPG axis(Nargund, 2015). Counselling patients about their stress levels andits potential detrimental effects that could lead to infertility would likelyprove to be a difficult process, and should probably be reserved forclinicians who are well-trained in the area. Other factors, such as ex-posure to certain metals and environmental toxins, have also beenassociated with infertility; however, such factors would be near im-possible to alter. Therefore, some aspects of infertility can be modifiedby altering several lifestyle choices, and should be included in theoverall assessment and treatment of males who present with infertility.
Comparison of human and animal studies: anestimation of Withania somnifera dosage
As previously discussed, several studies have been conducted usingWithania somnifera root powder or root extract on antioxidative,antiproliferative as well as spermatogenic effects of the plant (Ambiyeet al., 2013; Mahdi et al., 2009; Shukla et al., 2011). Although differ-ent studies have used different doses, and there is no ‘standard dose’of Withania somnifera used in different systems, most of the studiesconducted in humans have used 5g/d as a dose (Ahmad et al., 2010;Mahdi et al., 2009; Shukla et al., 2011). Animal and in-vitro studieshave used diverse doses (Dhumal et al., 2013; Kumar et al., 2015; Sahinet al., 2016). For future research work, however, using animals asexperimental models may require a ‘standard dose’. In this aspect,the formula of dose translation based on body surface area (BSA) canbe applied (Reagan-Shaw et al., 2007). This formula uses humanequivalent dose, animal dose and animal and human Km factors (theratio of body weight and BSA). The Center of Drug Evaluation and Re-search and the Center for Biologics Evaluation and Research (2002)have suggested that the extrapolation of animal dose is correctlycarried out only through normalization to BSA.
Studies on Withania somnifera used 5g per day Withania somniferato treat the patients without clearly indicating the body weights of thesubjects, but most of them continued the treatment as a single dosefor 3 months (Mahdi et al., 2009; Shukla et al., 2011). As the partici-pants of these studies are adults, if the average weight is consideredas 70 kg for an adult human being, the human equivalent dose (mg/kg) becomes 71.43 mg/kg. If the researchers are using rats as anexperimental model (Km value 6) and converts it from human dose,the animal dose becomes 440 mg/kg (using adult human Km valueof 37). Now, an adult rat weighs about 200–500 g (average 350 g), andso the single dose for a rat will be 154.14 mg/kg. This dose is similarto the doses used in animal studies mentioned above (Dhumal et al.,2013; Kumar et al., 2015). This, however, is an initial calculation fordosage for animals with equivalent BSA, as there are several other
322 R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6

factors like age, life stages and organ of interest for treatment whichmay demand alteration of dosage in animal models. Therefore, beforecalculating the final dose of treatment, all these factors should begiven due consideration.
Future perspectives
The usage of herbal medicine for the treatment of male infertility hasincreased over the past several decades by modern day clinicians.This is simply a re-discovery of what traditional medicines have beenusing since antiquity. Numerous studies have shown the various phar-macological effects that Withania somnifera has on sperm parametersand also on sex hormones. In this review, we have attempted to providea molecular mechanism of action, to have a better understanding ofhow Withania somnifera exerts its effects. The studies conducted oninfertile males thus far, have not looked specifically at pregnancy rates,implantation rates or live birth rates. As live birth is the end-pointof fertility treatments, it should be set as a primary outcome in futurestudies. Although double-blinded, randomized, placebo-controlled trialsare considered the gold standard, it can be recognized that futurestudies should focus more on the synergistic effect, if any, of Withaniasomnifera with standard medical treatment in improving fertility. Ad-ditional studies that look at Withania somnifera and assistedreproduction techniques would be beneficial, as the use of assistedreproduction techniques in the future is likely to increase. In par-ticular, it would be interesting to observe whether the beneficialproperties of Withania somnifera persist if added to cryopreservationmedia. Despite the limited data, Withania somnifera does exhibit an-tioxidant properties, improve semen parameters and regulate sexhormones. These effects may greatly affect men seeking treatmentfor infertility, as it poses a low-cost alternative and does not yet seemto show any adverse side-effect. By combining Withania somniferawith lifestyle modification and standard medical treatment in pa-tients with infertility, the clinician may be able to maximize the chancesof a successful clinical pregnancy leading to a live birth. In the presentreview, we have only summarized the outcomes of already-publishedreports on the ‘non-toxic’ herb Withania somnifera (Kulkarni and Dhir,2008); however, we have not carried out any dose–response rela-tionship or toxicological study. Therefore, this review is unable todeclare Withania somnifera as ‘safe’ or ‘toxic’ drug. Yet, from theresults of available reports, it can be appraised that Withania somniferais beneficial for male fertility in various aspects. As treatment of pa-tients with Withania somnifera in a clinical trial showed effectiveenhancement of male fertility, it can be used as a treatment in future.
Acknowledgement
This research study was supported by funds from the American Centerfor Reproductive Medicine, Cleveland Clinic.
A R T I C L E I N F O
Article history:
Received 6 June 2017
Received in revised form 21 November 2017
Accepted 22 November 2017
Declaration: The authors report no
financial or commercial conflicts of
interest.
Keywords:
Withania somnifera
Ashwagandha
Male infertility
Semen quality
R E F E R E N C E S
Abdillahi, H.S., Van Staden, J., 2012. South African plants and malereproductive healthcare: conception and contraception. J.Ethnopharmacol. 143, 475–480.
Agarwal, A., Nallella, K.P., Allamani, S.S., Said, T.M., 2004. Role ofantioxidants in treatment of male infertility: an overview ofliterature. Reprod. Biomed. Online 8, 616–627.
Agarwal, A., Prabakaran, S., Allamaneni, S.S., 2006a. Relationshipbetween oxidative stress, variocele and infertility: a meta-analysis.Reprod. Biomed. Online 42, 630–633.
Agarwal, A., Prabakaran, S., Sikka, S.C., 2006b. Current opinions onvariocele and oxidative stress and its role in male infertility. USGenitourinary Disease. 62–68.
Agarwal, A., Durairajanayagam, D., Virk, G., du Plessis, S.S., 2014a.Sources of ROS in ART. In: Strategies to Ameliorate OxidativeStress During Assisted Reproduction, SpringerBriefs inReproductive Biology. (Chapter 2), pp. 3–32. doi:10.1007/978-3-319-10259-7_2.
Agarwal, A., Virk, G., Ong, C., du Plessis, S.S., 2014b. Effect of oxidativestress on male reproduction. World J. Mens Health 32, 1.
Agarwal, A., Mulgund, A., Hamada, A., Chyatte, M.R., 2015. A uniqueview on male infertility around the globe. Reprod. Biol. Endocrinol.26, 37.
Ahmad, M.K., Mahdi, A.A., Shukla, K.K., Islam, N., Rajender, S.,Madhukar, D., Shankwar, S.N., Ahmad, S., 2010. Withania somniferaimproves semen quality by regulating reproductive hormone levelsand oxidative stress in seminal plasma of infertile males. Fertil.Steril. 94, 989–996.
Ambiye, V.R., Langade, D., Dongre, S., Aptikar, P., Kulkarni, M., Dongre,A., 2013. Clinical evaluation of the spermatogenic activity of the rootextract of Ashwagandha (Withania somnifera) in oligospermicmales: a pilot study. Evid. Based Complement. Alternat. Med. 2013,571420.
Baazeem, A., Belzile, E., Ciampi, A., Dohle, G., Jarvi, K., Salonia, A.,Weidner, W., Zini, A., 2011. Varicocele and male factor infertilitytreatment: a new meta-analysis and review of the role of varicocelerepair. Eur. Urol. 60, 796–808.
Begum, V.H., Sadique, J., 1988. Long term effect of herbal drug Withaniasomnifera on adjuvant induced arthritis in rats. Indian J. Exp. Biol.26, 877–882.
Belviranli, M., Gokbel, H., Okudan, N., Buyukba, S., 2015. Effects ofgrape seed extract on oxidative stress and anti-oxidant defensemarkers in streptozotocin-induced diabetic rats. Turk. J. Med. Sci.45, 489–495.
Bhargavan, D., Deepa, B., Shetty, H., Krishna, A.P., 2015. The protectiveeffect of Withania somnifera against oxidative damage caused byethanol in the testes of adult male rats. Int. J. Basic Clin.Pharmacol. 4, 1104–1108.
Bhattarai, J.P., Ah Park, S., Han, S.K., 2010. The methanolic extract ofWithania somnifera ACTS on GABAA receptors in gonadotropinreleasing hormone (GnRH) neurons in mice. Phytother. Res. 24,1147–1150.
323R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6

Biswas, N.M., Chattopadhyay, A., Sarkar, M., 2004. Effects of gold ontesticular steroidogenic and gametogenic functions in immaturemale albino rats. Life Sci. 76, 629–636.
Boveris, A., Chance, B., 1973. The mitochondrial generation of hydrogenperoxide. General properties and effect of hyperbaric oxygen.Biochem. J. 134, 707–716.
Castagné, V., Lefèvre, K., Natero, R., Clarke, P.G., Bedker, D.A., 1999. Anoptimal redox status for the survival of axotomized ganglion cells inthe developing retina. Neuroscience 93, 313–320.
Center for Disease Control and Prevention (CDC). Infertility FAQs. 2017.https://www.cdc.gov/reproductivehealth/infertility. (Accessed 1 April2017).
Center of Drug Evaluation and Research and the Center for BiologicsEvaluation and Research, 2002. Estimating the safe Starting Dose inClinical Trials for Therapeutics in Adult Healthy Volunteers. U.S.Food and Drug Administration, Rockville, Maryland, USA.
Chachamovich, J., Chachamovich, E., Fleck, M.P., Cordova, F.P., Knauth,D., Passos, E., 2009. Congruence of quality of life among infertilemen and women: findings from a couple-based study. Hum. Reprod.24, 2151–2157.
Chance, B., Sies, H., Boveris, H., 1979. Hydroperoxide metabolism inmammalian organs. Physiol. Rev. 59, 527–605.
Chandra, A.K., Sengupta, P., Goswami, H., Sarkar, M., 2012. Excessivedietary calcium in the disruption of structural and functional statusof adult male reproductive system in rat with possible mechanism.Mol. Cell. Biochem. 364, 181–191.
Chatterjee, S., Srivastava, S., Khalid, A., Singh, N., Sangwan, R.S., Sidhu,O.P., Roy, R., Khetrapal, C.L., Tuli, R., 2010. Comprehensivemetabolic fingerprinting of Withania somnifera leaf and rootextracts. Phytochemistry 71, 1085–1094.
Chen, R., Wen, H., 1996. Clinical treatment of male infertility with shengjing pill. Int. J. Orient. Med. 21, 144–147.
Clarke, T., Black, L., 2015. Trends in the use of complementary healthapproaches among adults: United States, 2002–2012. Natl. HealthStat. Report. 10, 1–16.
Crimmel, A.S., Conner, C.S., Monga, M., 2001. Withered Yang: a reviewof traditional Chinese medical treatment of male infertility anderectile dysfunction. J. Androl. 22, 173–182.
de Lamirande, E., Jiang, H., Zini, A., Kodama, H., Gagnon, C., 1997.Reactive oxygen species and sperm physiology. Rev. Reprod. 2, 48–54.
Dabaja, A.A., Schlegel, P.N., 2014. Medical treatment of male infertility.Transl. Androl. Urol. 3, 9–16.
Dar, N.J., Hamid, A., Ahmad, M., 2015. Pharmacologic overview ofWithania somnifera, the Indian Ginseng. Cell. Mol. Life Sci. 72, 4445–4460.
Dar, N.J., Bhat, J.A., Satti, N.K., Sharma, P.R., Hamid, A., Ahmad, M.,2016. Withanone, an active constituent from Withania somnifera,affords protection against NMDA-induced excitotoxicity in neuron-like cells. Mol. Neurobiol. doi:10.1007/s12035-016-0044-7.
DeFazio, R.A., Heger, S., Ojeda, S.R., Moenter, S.M., 2002. Activation ofA-type gamma-aminobutyric acid receptors excites gonadotropin-releasing hormone neurons. Mol. Endocrinol. 16, 2872–2891.
Devkar, S.T., Kandhare, A.D., Sloley, B.D., Jagtap, S.D., Lin, J., Tam,Y.K., Katyare, S.S., Bodhankar, S.L., Hegde, M.V., 2015. Evaluation ofthe bioavailability of major withanolides of Withania somnifera usingan in vitro absorption model system. J. Adv. Pharm. Technol. Res. 6,159–164.
Dhumal, R., Vijaykumar, T., Dighe, V., Selkar, N., Chawda, M., Vahila, M.,Vanage, G., 2013. Efficacy and safety of a herbo-mineral ayurvedicformulation ‘Afrodet Plus’ in male rats. J. Ayurveda Integr. Med. 4,158–164.
Dyer, S., Lombard, C., Van der Spuy, Z., 2009. Psychological distressamong men suffering from couple infertility in South Africa: aquantitative assessment. Hum. Reprod. 24, 2821–2826.
Dyer, S.J., Abrahams, N., Mokoena, N.E., van der Spuy, Z.M., 2004. ‘Youare a man because you have children’: experiences, reproductivehealth knowledge and treatment-seeking behaviour among men
suffering from couple infertility in South Africa. Hum. Reprod. 19,960–967.
Dyer, S.J., Abrahams, N., Mokoena, N.E., Lombard, C.J., van der Spuy,Z.M., 2005. Psychological distress among women suffering fromcouple infertility in South Africa: a quantitative assessment. Hum.Reprod. 20, 1938–1943.
Esteves, S.C., Agarwal, A., 2016. Afterword to varicocele and maleinfertility: current concepts and future perspectives. Asian J. Androl.18, 319–322.
Finkel, T., Holbrook, N.J., 2000. Oxidants, oxidative stress and thebiology of ageing. Nature 408, 239–247.
Gavella, M., Lipovac, V., 1992. NADH-dependent oxidoreductase(diaphorase) activity and isozyme pattern of sperm in infertile men.Arch. Androl. 28, 135–141.
Gershbein, L., Thielen, D., 1988. Enzymatic and Electrolytic Profiles ofHuman Semen. Prostate 12, 263–269.
Gharagozloo, P., Aitken, R.J., 2011. The role of sperm oxidative stress inmale infertility and the significance of oral antioxidant therapy. Hum.Reprod. 26, 1628–1640.
Griveau, J.F., Lannou, D.L., 1997. Reactive oxygen species andhuman spermatozoa: physiology and pathology. Int. J. Androl. 20,61–69.
Gupta, A., Mahdi, A.A., Shukla, K.K., Ahmad, M.K., Bansal, N., Sankhwar,P., Sankhwar, S.N., 2013. Efficacy of withania somnifera on seminalplasma metabolites of infertile males: a proton NMR study at800 MHz. J. Ethnopharmacol. 149, 208–214.
Gurib-Fakim, A., 2006. Medicinal plants: traditions of yesterday anddrugs of tomorrow. Mol. Aspects Med. 27, 1–93.
Hall, J., 2015. Infertility and contraception. In: Harrison’s Principles ofInternal Medicine, ninteenth ed. McGraw-Hill, New York.
Halliwell, B., 2000. The antioxidant paradox. Lancet 355,1179–1180.
Harlev, A., Agarwal, A., Gunes, S.O., Shetty, A., du Plessis, S.S., 2015.Smoking and male infertility: an evidence-based review. World J.Mens Health 33, 143–160.
Harris, E.D., 1992. Regulation of antioxidant enzymes. J. Nutr. 122, 625–626.
Henkel, R., Solomon, M., 2017. Oxidative stress. In: Zini, A., Agarwal, A.(Eds.), A Clinicians Guide to Sperm DNA and Chromatin Damage.Springer International Publishing. Submitted.
Henkel, R., Fransman, W.O., Hipler, U.C., Wiegand, C., Schreiber, G.,Menkveld, R., Weitz, F., Fisher, D., 2012. Typha capensis(Rohrb.)N.E.Br. (bulrush) extract scavenges free radicals, inhibitscollagenase activity and affects human sperm motility andmitochondrial membrane potential in vitro – a pilot study.Andrologia 44 (Suppl. 1), 287–294.
Henkel, R.R., Wang, R., Bassett, S., Chen, T., Liu, N., Zhu, Y., Tambi, M.I.,2014. Eurycoma longifolia (Tongkat Ali) as a potential herbalsupplement for physically active male and female seniors – a pilotstudy. Phytother. Res. 28, 544–550.
Ilfergane, A., Henkel, R., 2017. Effect of Typha capensis rhizome extractF1 fraction on cell viability, apoptosis induction and testosteroneproduction in TM3-Leydig cells. Andrologia 2017, doi:10.1111/and.12854. Epub ahead of print.
Jurewicz, J., Radwan, M., Sobala, W., Ligocka, D., Radwan, P.,Bochenek, M., Hanke, W., 2014. Lifestyle and semen quality:role of modifiable risk factors. Syst. Biol. Reprod. Med. 60,43–51.
Juyena, N.S., Stelletta, C., 2012. Seminal plasma: an essential attributeto spermatozoa. J. Androl. 33, 536–551.
Kaileh, M., Vanden Berghe, W., Heyerick, A., Horion, J., Piette, J., Libert,C., De Keukeleire, D., Essawi, T., Haegeman, G., 2007. Withaferin astrongly elicits IkappaB kinase beta hyperphosphorylationconcomitant with potent inhibition of its kinase activity. J. Biol.Chem. 282, 4253–4264.
Kataria, H., Gupta, M., Lakhman, S., Kaur, G., 2015. Withania somniferaaqueous extract facilitates the expression and release of GnRH: invitro and in vivo study. Neurochem. Int. 89, 111–119.
324 R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6

Khaki, A., Ainehchi, N., 2017. Herbal medicine and sexual behavior indiabetic patients. Int. J. Womens Health Reprod. Sci. 5, 1–2.
Koppers, A.J., De Iuliis, G.N., Finnie, J.M., McLaughlin, E.A., Aitken, R.J.,2008. Significance of mitochondrial reactive oxygen species in thegeneration of oxidative stress in spermatozoa. J. Clin. Endocrinol.Metab. 93, 3199–3207.
Kuboyama, T., Tohda, C., Komatsu, K., 2014. Effects of Ashwagandha(roots of Withania somnifera) in neurodegenerative diseases. Biol.Pharm. Bull. 37, 892–897.
Kulkarni, S.K., Dhir, A., 2008. Withania somnifera: an IndianGinseng. Prog. Neuropsychopharmacol Biol. Psychiatry 32,1093–1105.
Kumar, A., Kumar, R., Rahman, M.S., Iqubal, M.A., Anand, G., Niraj, P.K.,Ali, M., 2015. Phytoremedial effect of Withania somnifera againstarsenic-induced testicular toxicity in Charles foster rats. Avicenna J.Phytomed. 5, 355–364.
Kuo, Y.T., Liao, H.H., Chiang, J.H., Wu, M.Y., Chen, B.C., Chang, C.M.,Yeh, M.H., Chang, T.T., Sun, M.F., Yeh, C.C., Yen, H.R., 2017.Complementary chinese herbal medicine therapy improves survivalof patients with pancreatic cancer in taiwan: a nationwidepopulation-based cohort study. Integr. Cancer Ther.1534735417722224.
Lavie, D., Glotter, E., Shvo, Y., 1965. Constituents of Withaniasomifera Dun III. The side chain of Withaferin A. J. Org. Chem. 30,1774–1778.
Lohiya, N.K., Balasubhramaniyam, K., Ansari, S., 2016. Indian folkloremedicine in managing men’s health and wellness. Andrologia 48,894–907.
Luczaj, W., Skrzydlewska, E., 2003. DNA damage caused by lipidperoxidation products. Cell. Mol. Biol. Lett. 8, 391–413.
MacDonald, A.A., Herbison, G.P., Showell, M., Farquhar, C.M., 2010. Theimpact of body mass index on semen parameters and reproductivehormones in human males: a systematic review with meta-analysis.Hum. Reprod. Update 16, 293–311.
MacLeod, J., 1943. The role of oxygen in the metabolism and motility ofhuman spermatozoa. Am. J. Physiol. 138, 512–518.
Mahdi, A.A., Shukla, K.K., Ahmad, M.K., Rajender, S., Shankhwar, S.N.,Singh, V., Dalela, D., 2009. Withania somnifera improves semenquality in stress-related male fertility. Evid. Based Complement.Alternat. Med. 576962, 1–9.
Malviya, N., Malvia, S., Jain, S., Vyas, S., 2016. A review of the potentialof medicinal plants in the management and treatment of malesexual dysfunction. Andrologia 48, 880–893.
Mansouri, E., Keshtkar, A., Khaki, A.A., Khaki, A., 2016. Antioxidanteffects of allium cepa and cinnamon on sex hormones and serumantioxidant capacity in female rats exposed to power frequencyelectric and magnetic fields. Int. J. Womens Health Reprod. Sci. 4,141–145.
Mascarenhas, M.N., Flaxman, S.R., Boerma, T., Vanderpoel, S., Stevens,G.A., 2012. National, regional, and global trends in infertilityprevalence since 1990: a systematic analysis of 277 health surveys.PLoS Med. 9, e1001356.
Mills, E., Cooper, C., Seely, D., Kanfer, I., 2005. African herbal medicinesin the treatment of HIV: Hypoxis and Sutherlandia. An overview ofevidence and pharmacology. Nutr. J. 4, 19.
Mirjalili, M.H., Moyano, E., Bonfill, M., Cusido, R.M., Palazon, J., 2009.Steroidal lactones from Withania somnifera, an ancient plant forNovel medicine. Molecules 14, 2373–2393.
Mishra, L.C., Singh, B.B., Dagenais, S., 2000. Scientific basis for thetherapeutic use of Withania somnifera (ashwagandha): a review.Altern. Med. Rev. 5, 334–346.
Mokhber Maleki, E., Eimani, H., Bigdeli, M.R., Ebrahimi, B., Shahverdi,A.H., Golkar Narenji, A., Abedi, R., 2014. A comparative study ofsaffron aqueous extract and its active ingredient, crocin on the invitro maturation, in vitro fertilization, and in vitro culture of mouseoocytes. Taiwan. J. Obstet. Gynecol. 53, 21–25.
Nargund, V.H., 2015. Effects of psychological stress on male fertility.Nat. Rev. Urol. 12, 373–382.
Narinderpal, K., Junaid, N., Raman, B., 2013. A review onpharmacological profile of Withania somnifera (Ashwagandha). Res.Rev. 2, 6–14.
Ashwagndha: Natural Product Database (NPD). Lexi-Comp. Inc.http://naturaldatabase.therapeuticresearch.com/nd/Search.aspx?cs=&s=ND&pt=9&Product=Ashwaganda&btnSearch.x=0&btnSearch.y=0. (Accessed 25 May 2017).
Ouladsahebmadarek, E., Giasi, G.S., Khaki, A., Ahmadi, Y., Farzadi, L.,Ghasemzadeh, A., Hajizade, K., 2016. The effect of compound herbalremedy used in male infertility on spermatogenesis and pregnancyrate. Int. J. Womens Health Reprod. Sci. 4, 185–188.
Pandey, M.M., Rastogi, S., Rawat, A.K.S., 2013. Indian traditionalAyurvedic system of medicine and nutritional supplementation.Evidence-based Compl Alt Med 376327.
Parks, J.E., Lynch, D.V., 1992. Lipid composition and thermotropic phasebehavior of boar, bull, stallion, and rooster sperm membranes.Cryobiology 29, 255–266.
Patel, S.B., Rao, N.J., Hingorani, L.L., 2016. Safety assessment ofWithania somnifera extract standardized for Withaferin A: acute andsub-acute toxicity study. J. Ayurveda Integr. Med. 7, 30–37.
Prabu, P.C., Panchapakesan, S., Raj, C.D., 2013. Acute andsub-acute oral toxicity assessment of the hydroalcoholic extract ofWithania somnifera roots in Wistar rats. Phytother. Res. 27, 1169–1178.
Raha, S., Robinson, B.H., 2000. Mitochondria, oxygen free radicals andaging. Trends Biochem. Sci. 25, 502–508.
Rajasankar, S., Manivasagam, T., Sankar, V., Prakash, S., Muthuswamy,R., Krishnamurti, A., Surendran, S., 2009. Withania somnifera rootextract improves catecholamines and physiological abnormalitiesseen in Parkinson’s diseade model mouse. J. Ethnopharmacol. 125,369–373.
Ray, S., Jha, S., 2001. Production of Withaferin A in shoot cultures ofWithania somnifera. Planta Med. 67, 432–436.
Reagan-Shaw, S., Nihal, M., Ahmad, N., 2007. Dose translation fromanimal to human studies revisited. FASEB J. 22, 659–661.
Roychoudhury, S., Sharma, R., Sikka, S., Agarwal, A., 2016. Diagnosticapplication of total antioxidant capacity in seminal plasma to assessoxidative stress in male factor infertility. J. Assist. Reprod. Genet.33, 627–635.
Sahin, K., Orhan, C., Akdemir, F., Tuzcu, M., Gencoglu, H., Sahin, N.,Turk, G., Yilmaz, I., Ozercan, I.H., Juturu, V., 2016. Comparativeevaluation of the sexual functions and NF-KB and Nrf2 pathways ofsome aphrodisiac herbal extracts in male rat. BMC Complement.Altern. Med. 16, 318.
Samy, R.P., Pushparaj, P.N., Gopalakrishnakone, P., 2008. Acompilation of Bioactive Compounds from Ayurveda. Bioinformation3, 100–110.
Sapanidou, V.G., Margaritis, I., Siahos, N., Arsenopoulos, K., Dragatidou,E., Taitzoglou, I.A., Zervos, I.A., Theodoridis, A., Tsantarliotou, M.P.,2014. Antioxidant effect of a polyphenol-rich grape pomace extracton motility, viability and lipid peroxidation of thawed bovinespermatozoa. J. Biol. Res. (Thessalon.) 21, 19.
SART: Assisted Reproductive Technologies (Internet).http://www.sart.org/affiliates/sart/detail-sart.aspx?id=1908.(Accessed 29 January 2016).
Sengupta, P., 2013. Environmental and occupational exposure of metalsand their role in male reproductive functions. Drug Chem. Toxicol.36, 353–368.
Sharma, R.K., Agarwal, A., 1996. Role of reactive oxygen species in maleinfertility. Urology 48, 835–850.
Shukla, K.K., Mahdi, A.A., Mishra, V., Rajender, S., Sankhwar, S.N.,Patel, D., Das, M., 2011. Withania somnifera improves semen qualityby combating oxidative stress and cell death and improving essentialmetal concentrations. Reprod. Biomed. Online 22, 421–427.
Tambi, M.I., Imran, M.K., Henkel, R.R., 2012. Standardized water-soluble extract of Eurycoma longifolia, Tongkat Ali, as testosteronebooster for managing men with late-onset hypogonadism?Andrologia 44 (Suppl. 1), 226–230.
325R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6
Wadha, R., Singh, R., Gao, R., Shah, N., Widodo, N., Nakamoto, T.,Ishida, Y., Terao, K., Kal, S.C., 2013. Water extract ofAshwagandha leaves has anticancer activity: identification of anactive comopent and its mechanism of action. PLoS ONE 8,e77189.
Walsh, T., Smith, J.F., 2013. Male infertility. In: Smith & Tanagho’sGeneral Urology, eighteenth ed. Mcgraw-Hill, New York. (Chapter44).
Watanabe, M., Fukuda, A., Nabekura, J., 2014. The role of GABA in theregulation of GnRH neurons. Front. Neurosci. 8, 387.
Zhang, H., Zhao, H., Zhang, A., 2007. Male infertility with severeoligospermatism and azoospermia treated by Bushen ShengjingDecoction combined with intracytoplasmic sperm injection.Zhongguo Zhong Xi Yi Jie He Za Zhi 27, 972–975.
Zini, A., Al-Hathal, N., 2011. Antioxidant therapy in male infertility: factor fiction? Asian J. Androl. 13, 374–381.
326 R E P R O D U C T I V E B I O M E D I C I N E O N L I N E 3 6 ( 2 0 1 8 ) 3 1 1 – 3 2 6