Embed Size (px)
Citation preview

MichaelJ.ZellwegerKardiologischeKlinikUSB
ISCHÄMIEDIAGNOSTIK

KernpunktedernichtinvasivenDiagnostikbeikoronarerHerzkrankheit¨ Intermediäre Vortestwahrschinlichkeit der koronaren Herzkrankheit à
Domäne der nicht - invasiven (Ischämie) Diagnostik
¨ Ergometrie versus bildgebende Diagnostik
¨ Bildgebende Methoden im Kontext
¨ Anatomie und Funktion - komplementär
¨ ein patientenorientierter, massgeschneiderter Ansatz

Brustschmerzen- istesdasHerz?
Brustschmerzen- istesdasHerz?
¨ 65j.adipöserPatient¨ Seit2TagenlinksseitigeBrustbeschwerden¨ AkzentuiertbeimLiegenaufderlinkenSeite¨ keineBegleitsymptome- gutleistungsfähig¨ AntikoagulationwegenVorhofflimmerns¨ RF:arterielleHypertonie,Diabetesmellitus

Standard
25%
25%
25%
25%
1. SofortigeHospitalisation
2. EKG,Troponin
3. UntersuchungdesPatienten
4. Nicht- invasiveIschämiediagnostik
TED-Frage:WiegehenSieweitervor?
020 000

WeitesFeldderDifferentialdiagnosen...
HämatombeispontanerBlutungunterAntikoagulation

Thoraxschmerzen inderPraxis
Diagnose Häufigkeit %
Muskuloskeletal 327 49
Kardiovaskulär 108 16
Psychogen 77 12
Respiratorisch 69 10
Gastrointestinal 55 2
Verschiedene 15 2
OhneDiagnose 21 3
Total 672 100
Verdon etal.SMW2008;138(23–24):340–347
2.7%von24620PatientenhattenThoraxschmerzen0.4%alldieserPatientenhatteneinekardiovaskuläreUrsache

Anamnese:Vor- TestWahrscheinlichkeitderkoronarenHerzkrankheit
DiamondGAetal.NEJM1979;300:1350-8Eur Heart J 2013;34:2949–3003
InvasiveAbklärung
Nicht– invasiveAbklärung
KeineweitereAbklärung

Artificial intelligence hilftbeiderBestimmungderVortest - Wahrscheinlichkeit
ZellwegerMJetal.Int JCardiol.2014Jun1;174(1
MPApre-testprobability
0.840.69
AUC
MPA:memtic pattern based algorithm, FRAM:Framingham risk score

Nicht - invasiveAbklärung derKHKbeiintermediärer Vortest - Wahrscheinlichkeit
Eur HeartJ 2013;34:2949–3003
IntermediäreVortest - Wahrscheinlichkeit
Nicht- invasiveDiagnostik:ModalitätjenachlokalerExpertiseundVerfügbarkeit
à patient tailored approach

BildgebungversusErgometrie
¨ BeiallenPatientenmöglich(pharmakologischerTest)
¨ Informationüber:
Ø LokalisationderNarben/Ischämien
Ø AusdehnungderNarben/Ischämien
Ø PumpfunktionundVoluminadesHerzens
Ø Viabilität
à HöherediagnostischeundprognostischeSicherheit

Ischämische Kaskade undDiagnostik
ZellwegerM.SwissMedWkly.2019;149:w20014

AnatomieundFunktion- komplementär
Oculo – stenotic community
hemodynamic community
Atherosclerosis/stenosis
Ischemia, scar
IntegrierteInterpretationallerverfügbarerInformationen!

VerschiedeneklinischeSzenarienAusschnittauseinemPET/CTBericht
• Ruhedurchblutung• Durchblutung unter
Stress• Pumpfunktion
• Flussraten/-reserve
• VerkalkungderGefässe
• ev.CT-Angiographie

NormaleHerzkranzgefässe,keineVerkalkungen,normaleHerzdurchblutung
AusschlusseinerkoronarenHerzerkrankung

AlterskorrigiertleichtverkalkteHerzkranzgefässemitStenosen,ohnehämodynamische Relevanz(normaleHerzdurchblutung)
CalciumScore84
Ausschlusseinerstenosierenden koronarenHerzerkrankungà LifestyleundmedikamentöseTherapie
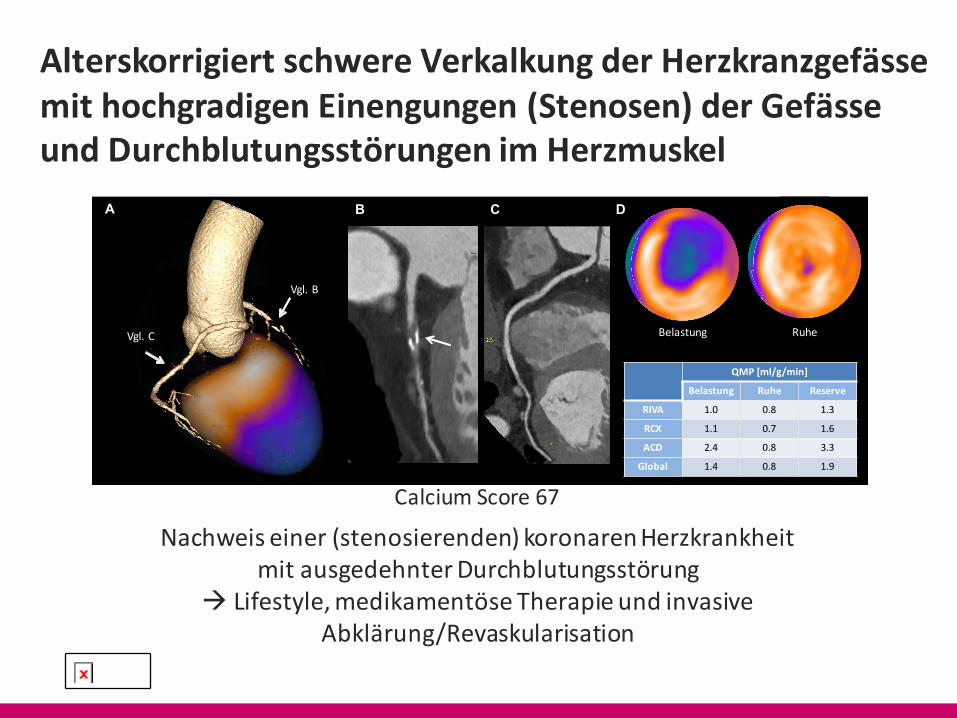
AlterskorrigiertschwereVerkalkungderHerzkranzgefässemithochgradigenEinengungen(Stenosen)derGefässeundDurchblutungsstörungenimHerzmuskel
CalciumScore67
A B C
Belastung Ruhe
QMP[ml/g/min]
Belastung Ruhe Reserve
RIVA 1.0 0.8 1.3
RCX 1.1 0.7 1.6
ACD 2.4 0.8 3.3
Global 1.4 0.8 1.9
Vgl.B
Vgl.C
D
Nachweiseiner(stenosierenden)koronarenHerzkrankheitmitausgedehnterDurchblutungsstörung
à Lifestyle,medikamentöseTherapieundinvasiveAbklärung/Revaskularisation

normaler Stresstest
≠Ausschluss koronare Herzkrankheit

normaler Stresstest
=niedrige Wahrscheinlichkeit
für eine hämodynamischrelevante Stenose
meist vereinbar mit guterPrognose
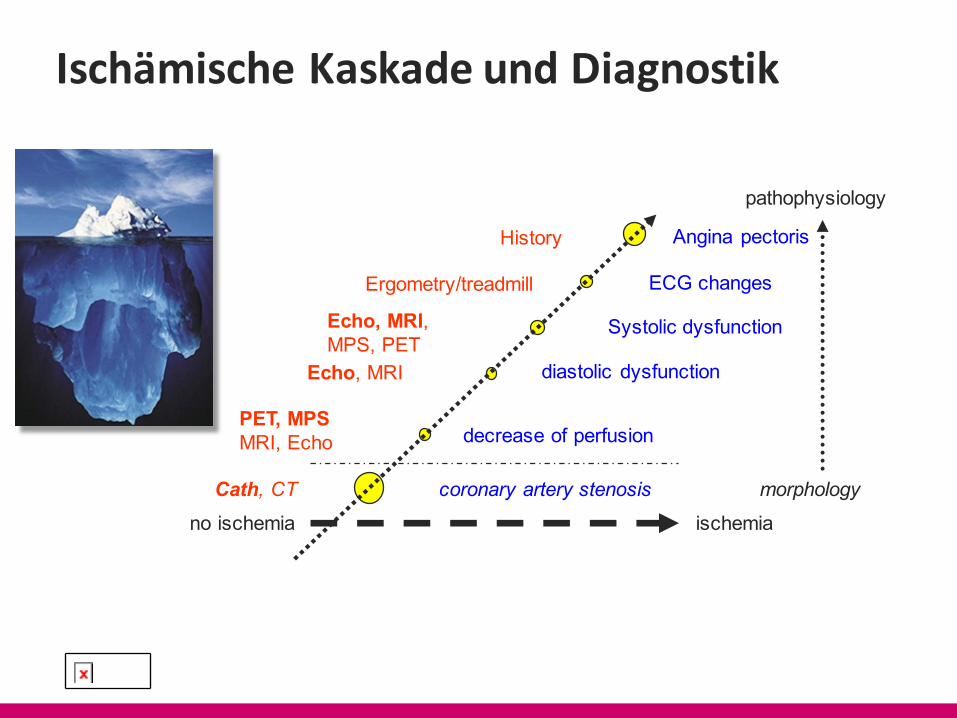
Ischämische Kaskade undDiagnostik
no ischemia
decrease of perfusion
diastolic dysfunction
ECG changes
Angina pectoris
Systolic dysfunction
History
Ergometry/treadmill
Echo, MRI,MPS, PET
Echo, MRI
PET, MPSMRI, Echo
ischemiacoronary artery stenosisCath, CT morphology
pathophysiology

Anatomie/Koronarkalk(Agatston - Score)
¨ KoronarkalkistAusdruckeinerkoronarenHerzkrankheit¤ JehöherderCalciumscore,destohöherdie„Calciumlast“
¨ MarkerallerRisikofaktoren,dieaufdieKoronarien einesIndividuumsimLaufedesLebensaufdieHerzkranzgefässeeingewirkthaben¤ UnterliegtdenLimitationenderRisikoscores nicht(wieAGLA/Framingham/PROCAM)
¤ hatanerkanntenprognostischenWert
CT- Untersuchung<<1mSveinmalAtemanhaltenkeinKontrastmittelnötig

Anatomie/KoronarkalkundPrognoseüber15Jahre
ShawLJ.AnnInternMed.2015;163:14-21
3%6%
9%
14%
21%
28%
Una
djus
ted
all-c
ause
mor
talit
y
n =9715,asymptomatischCAC 0 1-10 11-100 101-399 400-999 >1000

RelevanteKoronarstenosebei„kalkfreien“Koronarien sehrunwahrscheinlich
Iwasaki et al
Can J Cardiol Vol 26 No 7 August/September 2010378
Patients with a heart rate of more than 70 beats/min received oral metoprolol 20 mg before the 64-slice CT scan. To achieve coronary vasodilation, 0.8 mg of sublingual nitroglycerin was administered before the scan.
A native scan without contrast dye was performed to determine the total calcium burden of the coronary tree (sequential scan with 32 mm × 0.6 mm collimation, tube current 60 mA at 120 kV). Contrast-enhanced CT angiography data were acquired with the use of a spiral scan with 32 mm × 0.6 mm collimation, 330 ms gantry rota-tion, a pitch of 0.2 and a tube voltage of 120 kV.
A total of 64 overlapping 0.6 mm slices per rotation were acquired with the use of a focal spot periodically moving in the longitudinal direction (z-flying focal spot).
Tube current was modulated according to the electrocardiogram, with a maximum current of 850 mA to 950 mA during a time period of approximately 330 ms centred at 375 ms before the next R wave and reduction by 80% during the remaining cardiac cycle. Contrast agent (60 mL to 70 mL; 370 mg iodine/mL) was injected intrave-nously (4.0 mL/s), followed by a 30 mL saline chaser. Transaxial images were reconstructed using an electrocardiogram-gated half-scan reconstruction algorithm (temporal resolution 164 ms) and a B30f kernel.
The 64-slice CT image interpretationCT data sets were transferred to an off-line workstation (Aquarius NetStation; Terarecon Inc, USA) for image analysis. Total calcium scores for all patients were calculated using dedicated software and were expressed as Agatston scores. The Agatston score is a commonly used scoring method that calculates the total amount of calcium on the basis of the number, areas and peak Hounsfield units (HU) of the detected calcified lesions (23).
Two reviewers independently evaluated the contrast-enhanced 64-slice CT scans with maximum-intensity and curved multiplanar reconstruction techniques along multiple longitudinal axes and
transversely. The coronary artery tree was segmented according to a modified American Heart Association classification system and the segments were evaluated visually for the presence of coronary artery stenosis (24).
Noncalcified atherosclerotic plaque was defined as any discernible structure that could be clearly assignable to the vessel wall, that had a CT density of lower than the contrast-enhanced coronary lumen but greater than the surrounding connective tissue, and that could be identified in at least two independent planes (14). Standard display settings were used for the evaluation of the contrast-enhanced 64-slice CT scans (window width 800 HU; window centre 250 HU).
Two observers identified coronary segments using a modified American Heart Association classification. Segments were classified as normal (smooth parallel or tapering borders), having nonsignificant stenosis (luminal irregularities or less than 50% stenosis) or having significant stenosis.
Informed consent for the clinical procedure and research protocol was received from all studied patients. The present study was approved by an institutional review board.
Statistical analysisData are expressed as mean ± SD. Discrete variables were expressed as counts or percentages, and were compared using the χ2 or Fisher’s exact tests. The difference in the prevalence of coronary plaque between the two groups was calculated by the Mann-Whitney U test. P<0.05 was considered to be statistically significant.
RESULTSA total of 224 asymptomatic patients were identified with no CAC (n=117) and with mild CAC (n=107).
Clinical characteristics of the patients studied are shown in Table 1. Patients in the no CAC group were younger and had a lower prevalence of diabetes. Medications and laboratory data were not sig-nificantly different between the two groups.
Figure 1 shows the prevalence of noncalcified plaque in the two groups. The incidence of noncalcified plaque was 11.1% in the no CAC group and 23.4% in the mild CAC group (P=0.0142).
Figure 1) Prevalence of noncalcified plaque. CAC Coronary artery calcium
20
40
60
80
100(%)
p=0.0142
TABLE 1Clinical characteristics of patients
No CAC (n=117) Mild CAC (n=107) P
Age, years, mean ± SD 62.4±10.4 67.4±8.5 0.0003Male sex 59 (50.4) 59 (55.1) 0.9999Hypertension 51 (43.6) 60 (56.1) 0.0616Hyperlipidemia 48 (41.0) 55 (51.4) 0.1193Diabetes mellitus 19 (16.2) 36 (33.6) 0.0024Active smoker 34 (29.1) 36 (33.6) 0.4596Obesity 22 (18.8) 24 (22.4) 0.5023Therapy
Acetylsalicylic acid 21 (17.9) 20 (18.7) 0.8596Statin 40 (34.2) 35 (32.7) 0.4548ARB/ACE-I 51 (43.6) 48 (44.9) 0.6593CCB 40 (34.2) 38 (35.5) 0.7663BB 13 (11.1) 8 (7.5) 0.2467
Laboratory data, mean ± SDBS, mmol/L 7.3±3.2 8.0±3.3 0.2736HbA1c, % 6.70±1.74 6.62±1.40 0.9767TC, mmol/L 5.52±0.91 5.64±0.97 0.7046TG, mmol/L 1.64±0.96 1.98±1.01 0.1585HDL-C, mmol/L 1.45±0.41 1.38±0.34 0.4654LDL-C, mmol/L 2.84±0.60 3.78±0.92 0.2294
Data presented as n (%) unless otherwise indicated. ACE-I Angiotensin-converting enzyme inhibitor; ARB Angiotensin receptor blocker; BB Beta-blocker; BS Blood sugar; CAC Coronary artery calcium; CCB Calcium channel blocker; DM Diabetes mellitus; HbA1c Hemoglobin A1c; HDL-C High-density lipoprotein cholesterol; LDL-C Low-density lipoprotein cholesterol; TC Total cholesterol; TG Triglyceride
Iwasakietal.CanJCardiol 2010;26:377-380
224asymptomatic patients
CAC=0CAC<100
Significant stenosis0.9% 2.8%

NormalesCoronar - CTschliesst koronareHerzkrankheitpraktischaus
“warranty period” of a normal scan. These dataextend to other methods of stress testing (SE, cardiacmagnetic resonance, and positron emission tomog-raphy), with the literature supporting the prognosticimportance not only of functional capacity, but alsoof the results of imaging (33).
The prognostic utility of CCTA has also beenextensively studied. In the CONFIRM (Coronary CTAngiography Evaluation for Clinical Outcomes Inter-national Multicenter) study (34), increasing extent,severity, and location of CAD predicted adverse out-comes. CCTA may identify very low-risk individuals—incremental to clinical scoring systems and CAD riskfactors—and improves prediction, discrimination, andreclassification of these individuals as higher risk inthe presence of CAD (35). Conversely, a large evidencebase supports the benign outcome of patients without
evidence of CAD by CCTA, with annualized eventrates of 0.01% to 0.24% (36). Similar data have beenobtained in patients undergoing CCTA for the evalu-ation of possible acute coronary syndrome (ACS) (36).These data highlight the importance of the NPV byCCTA, not only to rule out obstructive CAD, but alsoto effectively rule out future adverse events with along-term ($5-year) “warranty period.” CCTA’s ac-curacy for the exclusion of CAD allows ICA to berestricted to patients with CT evidence of CAD.
Whereas the assessment of decision making afterthe results of functional testing suggests that it israrely on the basis of risk (37), this problem may bemore marked with CCTA. In a comparative analysisof outcomes after CT and stress testing in a largeMedicare population, the provision of anatomic datawas associated with an increased likelihood of sub-sequent cardiac catheterization, percutaneous coro-nary intervention, and coronary artery bypass graftsurgery with CCTA compared with SPECT, andconsequently with higher costs (38). CCTA use wasassociated with a lower likelihood of hospitalizationfor acute MI (0.19% vs. 0.43%; adjusted OR: 0.60; 95%CI: 0.37 to 0.98; p ¼ 0.04), but no difference in overallmortality.
IDENTIFICATION OF INDIVIDUALS WHO
WILL AND WILL NOT BENEFIT FROM
CORONARY REVASCULARIZATION
Coronary revascularization decisions should not besolely on the basis of anatomic stenosis (39,40).Former comparisons between anatomic (ICA) andfunctional approaches showed that interventionswere twice as likely once the coronary anatomy wasknown (2). In contrast, failure to identify perfusion orwall motion abnormalities, preserved exercise ca-pacity, and lack of ST-segment abnormality are allfunctional testing results pointing to low risk. Inseveral large observational studies, revascularizationwas associated with more favorable outcomes in in-dividuals with a significant amount of ischemia(>12.5%), and with better outcomes in individualswith limited ischemia with medical therapy (41).
In contrast, moderate (40% to 70%) stenosescorrelate poorly with the presence and degree ofimpaired coronary vasodilator reserve (42). Approxi-mately 20% of patients with apparently significantstenoses are identified as having normal FFR, and13% of those thought to have nonsignificant stenoseshave abnormal flow reserve (43). The absence of thisfunctional information is a potential limitation forCCTA and argues for the use of ischemia-based eval-uations to guide revascularization decisions.
TABLE 3 Diagnostic Testing and Angiographic Findings in Patients UndergoingCoronary Angiography*
Noninvasive Tests(n ¼ 387,633)
Obstructive CAD(n ¼ 173,448)
Nonobstructive CAD(n ¼ 214,185) p Value
Standard exercise stress test 37,969 (9.8) 17,016 (9.8) 20,953 (9.8) 0.77
Stress echocardiogram 44,829 (11.6) 19,651 (11.3) 25,178 (11.8) <0.001
Stress testing with SPECT 302,651 (78.1) 134,670 (77.6) 167,981 (78.4) <0.001
Stress testing with CMR 2926 (0.8) 1331 (0.8) 1595 (0.7) 0.42
CCTA 8323 (2.1) 5791 (3.3) 2532 (1.2) <0.001
Values are n (%). *From the NCDR database (4).
CCTA ¼ coronary computed tomographic angiography; CMR ¼ cardiac magnetic resonance; NCDR ¼ NationalCardiovascular Database Registry; other abbreviations as in Table 1.
FIGURE 1 Sensitivity, Specificity, and Predictive Value ofCCTA in 3 Prospective Multicenter Trials of the DiagnosticPerformance of CCTA
100
80
60
40
20
0Sensitivity Specificity PPV NPV
ACCURACY (230, 13% prevalence)EUROPE (360, 68% prevalence)MEDIC (415, 20-80% risk)
The predictive value of a negative test is uniformly very high.ACCURACY ¼ Assessment by Coronary Computed TomographicAngiography of Individuals Undergoing Invasive Coronary Angi-ography; CCTA ¼ coronary computed tomographic angiography;EUROPE ¼ European study (18); MEDIC ¼ Multicenter Evaluationof Coronary Dual-Source CT angiography in patients with inter-mediate Risk of Coronary Artery Stenoses; NPV ¼ negative pre-dictive value; PPV ¼ positive predictive value.
Marwick et al. J A C C V O L . 6 5 , N O . 2 5 , 2 0 1 5
Gatekeeper to the Catheterization Laboratory J U N E 3 0 , 2 0 1 5 : 2 7 4 7 – 5 6
2750
Marwick etal.J Am Coll Cardiol 2015;65:2747–56

PatientenohneMyokardnarbeundohneIschämiehabeneinesehrgutePrognose
100
99.75
99.5
99.25
99
Übe
rlebe
nsra
te
Iskander Gibbons Shaw Shaw Meta - analysis12 000 4649 8411 4726 29 786
Shawetal.JNucl Med 2003;44:134–139
„Garantieperiode“starkabhängigvonFaktorenwievorbekannterKHK,Diabetes,etc.
MPSDaten

Bei einer Ischämie >10%desMyokards profitierenPatienten prognostisch voneiner Revaskularisation
log
Haz
ard
Rat
io0
12
34
56
% Total Myocardium Ischemic
0 12.5% 25% 32.5% 50%
MedicalRx
Revasc*
*
*p<0.001
†Adjusted for clinical, hx, stressSPECT and referral data
Hachamovitch etal.Circulation 2003;107:2900-2906
10 % myocardium
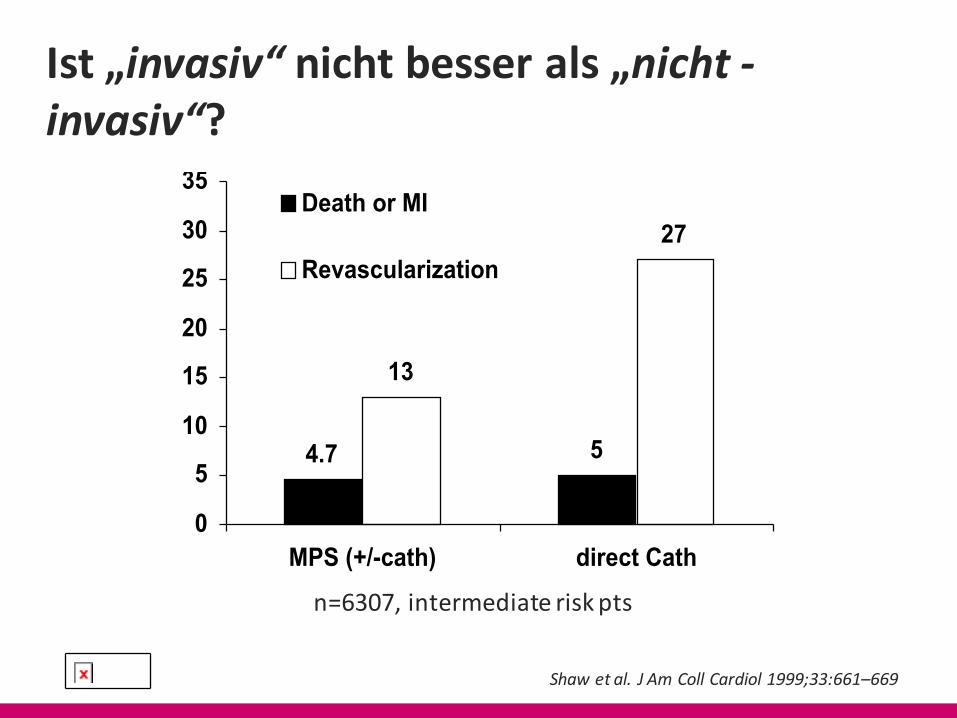
Ist„invasiv“ nichtbesserals„nicht-invasiv“?
4.7 5
13
27
0
5
10
15
20
25
30
35
MPS (+/-cath) direct Cath
Death or MI
Revascularization
Shawetal.JAmColl Cardiol 1999;33:661–669
n=6307,intermediaterisk pts

NutzenderStatintherapie inRelationzurKoronarverkalkung
Mitchell,J.D.etal.JAmColl Cardiol.2018;72(25):3233–42

Zusammenfassend¨ Anamnese: Vortest - Wahrscheinlichkeit à Intermediär à nicht -
invasive (Ischämie-) diagnostik
¨ Bildgebende Methoden gegenüber der Ergometrie zu bevorzugen
¨ Angina pectoris und Ischämie sind die Spitze des Eisbergs -
Gefässverkalkungen, Risikofaktoren ?
¨ Funktion und Anatomie ergeben komplementäre Informationen
¨ Ein patientenorientierter, massgeschneiderter Ansatz,
in Abstimmung mit lokaler Verfügbarkeit und Expertise