Embed Size (px)
Citation preview

Schildklierlijden en diabetes
C. De Block
Oktober 2014

Content
• Fysiologie van de schildklier
• Prevalentie, diagnostiek, tekenen en behandeling van hypo-, hyperthyroidie
• Prevalentie van schildklierpathologie bij diabetes
• Glucose-ontregeling bij schildklierlijen
• Cardiovasculaire gevolgen
• Screening
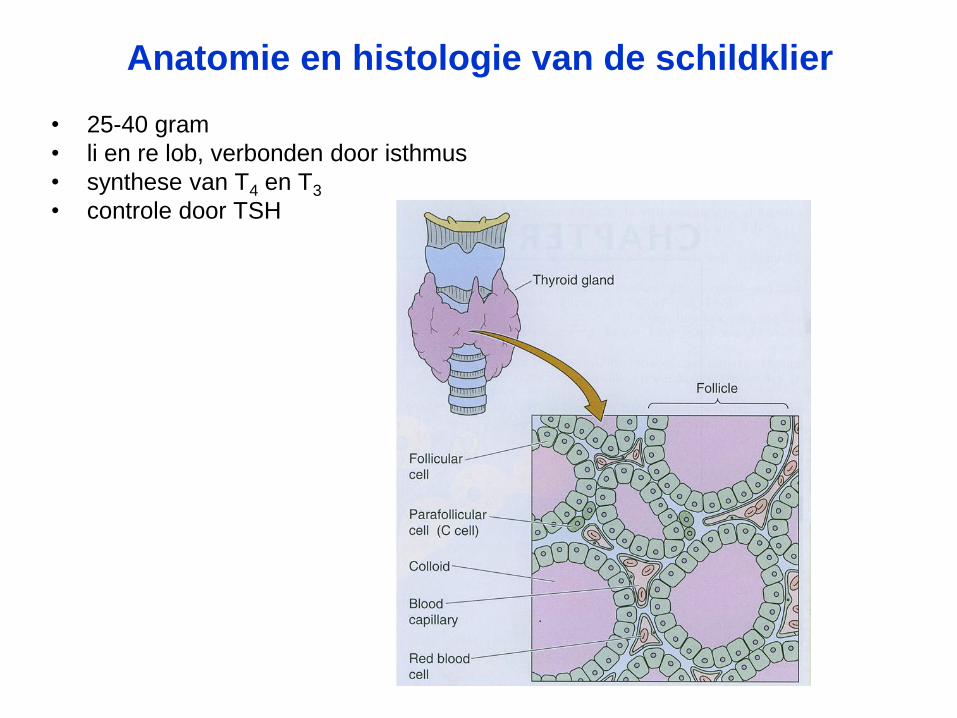
Anatomie en histologie van de schildklier
• 25-40 gram
• li en re lob, verbonden door isthmus
• synthese van T4 en T3
• controle door TSH
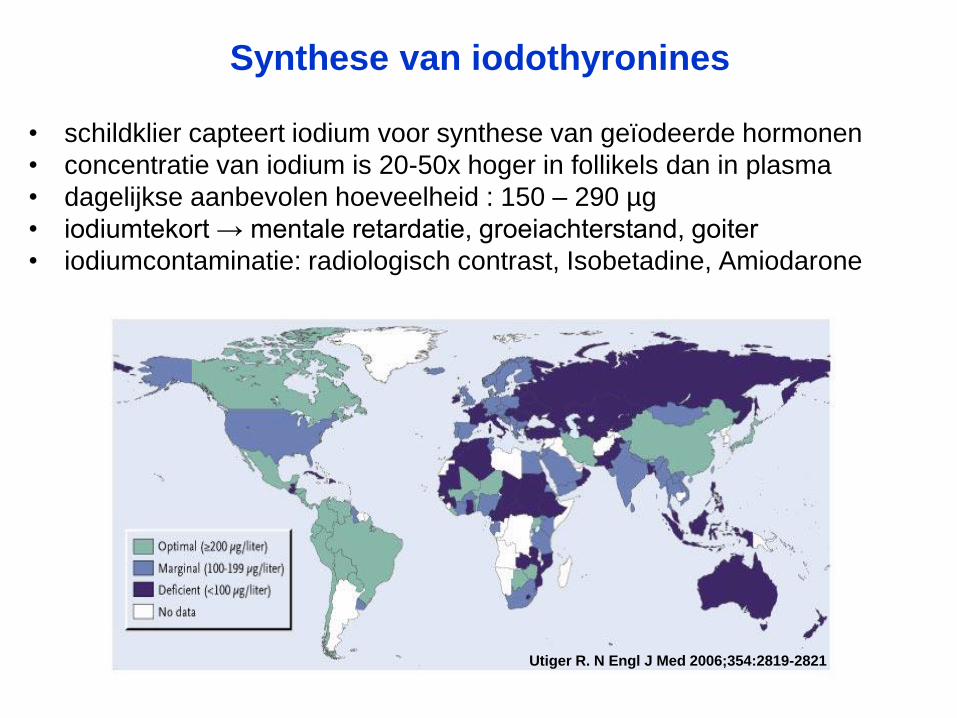
Synthese van iodothyronines
• schildklier capteert iodium voor synthese van geïodeerde hormonen
• concentratie van iodium is 20-50x hoger in follikels dan in plasma
• dagelijkse aanbevolen hoeveelheid : 150 – 290 µg
• iodiumtekort → mentale retardatie, groeiachterstand, goiter
• iodiumcontaminatie: radiologisch contrast, Isobetadine, Amiodarone
Utiger R. N Engl J Med 2006;354:2819-2821

Regulatie
hypofyse
schildklier
hypothalamus
TSH
TRH
T4 (T3)
+
+
-
-

Acties van schildklierhormonen
• calorigeen effect: basaal metabolisme ↑
• effect op eiwitmetabolisme– eiwitsynthese stijgt (groei !) o.i.v. T3 en T4
• effecten op het koolhydraatmetabolisme: – intestinale absorptie van glucose stijgt en
– gluconeogenese ↑ o.i.v. T3
• effecten op het vetmetabolisme: – lipolyse
Acties van schildklierhormonen
• effecten op lichaamsstelsels:
– zenuwstelsel: ontwikkeling en rijping
– cardiovasculair:
• versnelling van het hartritme,
• verhoogde output en contractiekracht van het hart;
– periferie: vasodilatatie en toename van warmteverlies (zweten)
– spijsverteringsstelsel:
• versnellen de intestinale motiliteit
– bevorderen de spiergroei
– versnellen de vorming van epifysaire beenkernen

Interpretatie van Schildklierfunctie Testen
normaal onderdrukt gestegen
normaal verhoogd verlaagd
euthyroïdie hyperthyroïdie hypothyroïdie
TSH
T4/T3

Hypothyroïdie
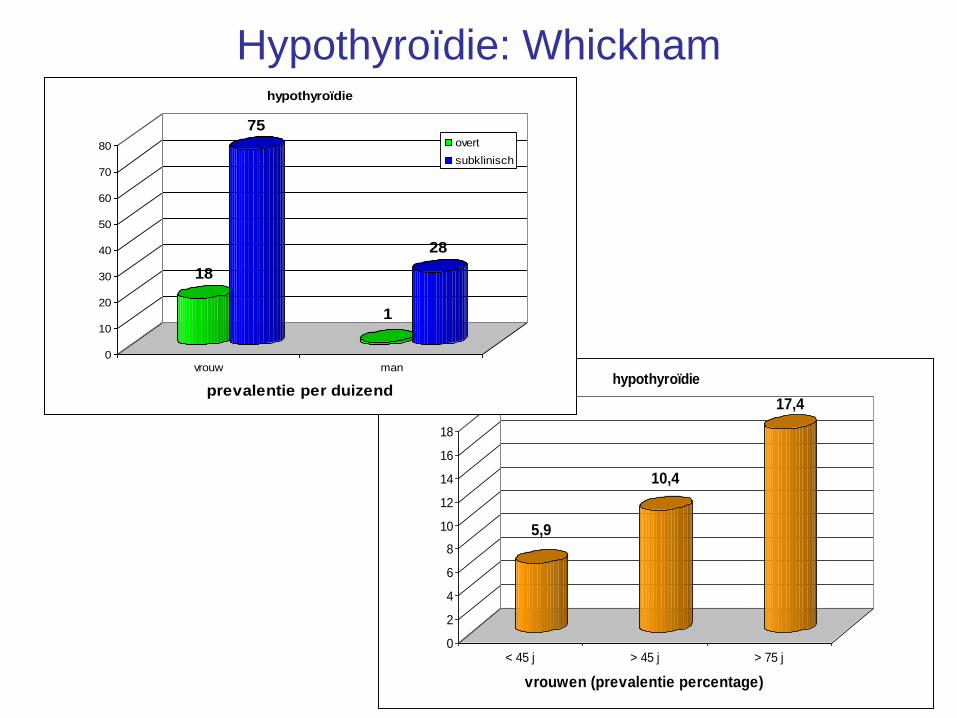
Hypothyroïdie: Whickham
5,9
10,4
17,4
0
2
4
6
8
10
12
14
16
18
< 45 j > 45 j > 75 j
vrouwen (prevalentie percentage)
hypothyroïdie
18
75
1
28
0
10
20
30
40
50
60
70
80
vrouw man
prevalentie per duizend
hypothyroïdie
overt
subklinisch

Hypothyroïdie: Whickham
Kans om Overte Hypothyroidie te ontwikkelen bij vrouwen in 20 jaar
na initiele meting van TSH
TSH

Hypothyroïdie:
Hoog-risico groepen:
• postpartum vrouwen
• famil VG
• VG van hoofd-, nek- of schildklierbestraling of
heelkunde
• andere AIZ
• Down
• Turner

• meestal insidieus, van asymptomatisch tot een beeld met allerlei gradaties in symptomen
• goiter
• vermoeidheid
• koude-intolerantie
• gastrointestinaal:– gewichtstoename
– constipatie
• huid, haar en nagels:– droge, bleke huid
– droog, broos haar, haaruitval & broze nagels
Kliniek Hypothyroïdie:

• cardiovasculair:– bradycardie
– verminderde contractiliteit, verminderd slagvolume
– hypercholesterolemie
• zenuwstelsel:– hese stem, trage spraak
– geheugenstoornissen, moe
– vertraagde reflexen
• musculair: vertraagde contractie
Kliniek Hypothyroïdie:

Etiologie Hypothyroïdie
• primaire hypothyroïdie:
– chronische autoimmune thyroïditis: Hashimoto
– iatrogeen:
• thyreostatica,
• post thyroïdectomie,
• post radioactief iodium, bestraling
– iodium deficiëntie
– farmaca: lithium, amiodarone, interferon-α, perchloraat
– transiënte hypothyroïdie:
• pijnloze (silent, lymfocytaire) thyroïditis
• subacute granulomateuze thyroïditis (De Quervain)
• postpartum thyroïditis

Diagnose van Hypothyroïdie
• primaire hypothyroïdie
TSH + of normale T3 / T4

Autoimmune Thyroïditis (Hashimoto)
• meest voorkomende oorzaak van hypothyroïdie:
• prevalentie in alg bevolking: 0.1-10%
• destructie van follikels door lymfocytaire infiltratie
• atrofie is eindstadium na volledige destructie van goiter
• risico factoren: - genetisch (DR3, CTLA-4)
- Down syndroom, Turner syndroom
- andere AIZ
- iodium
- leeftijd (40-60 jaar)
- geslacht: V/M: 7/1
• bevestiging: - TPO-antilichamen
Hakaru Hashimoto (1881-1934)

Behandeling van Hypothyroïdie
• Levo-thyroxine
- L-Thyroxine, Elthyrone, Euthyrox, Thyrax
- ½-leven 7d = éénmalige dagelijkse inname
- perifeer omgezet in actief triiodothyronine
- 1.6-1.8 µg/ kg ideaal gewicht
- 80% resorptie
- 75-112 µg voor vrouwen / 125-200 µg voor mannen

Hyperthyroïdie

Hyperthyroïdie: prevalentie
28
2
0
5
10
15
20
25
30
vrouw man
prevalentie per duizend
overte hyperthyroïdie
Whickham-studie
2.8% van de vrouwen en 0.2% van de mannen
Prevalentie stijgt met de leeftijd

Hyperthyroïdie:kliniek
symptomen %
• zenuwachtigheid 95
• warmte intolerantie 90
• moeheid 90
• hartkloppingen 90
• vermagering 85
• kortademigheid 75
• uitputtingsgevoel 70
• toegenomen eetlust 65
• oog klachten 55
tekens %
• tachycardie 95
• goiter 95
• zweten 95
• tremor 95
• oog tekens 70
• spierzwakte 70
• voorkamerfibrillatie 10
• versnelde spraak
• verkorte relaxatie reflexen
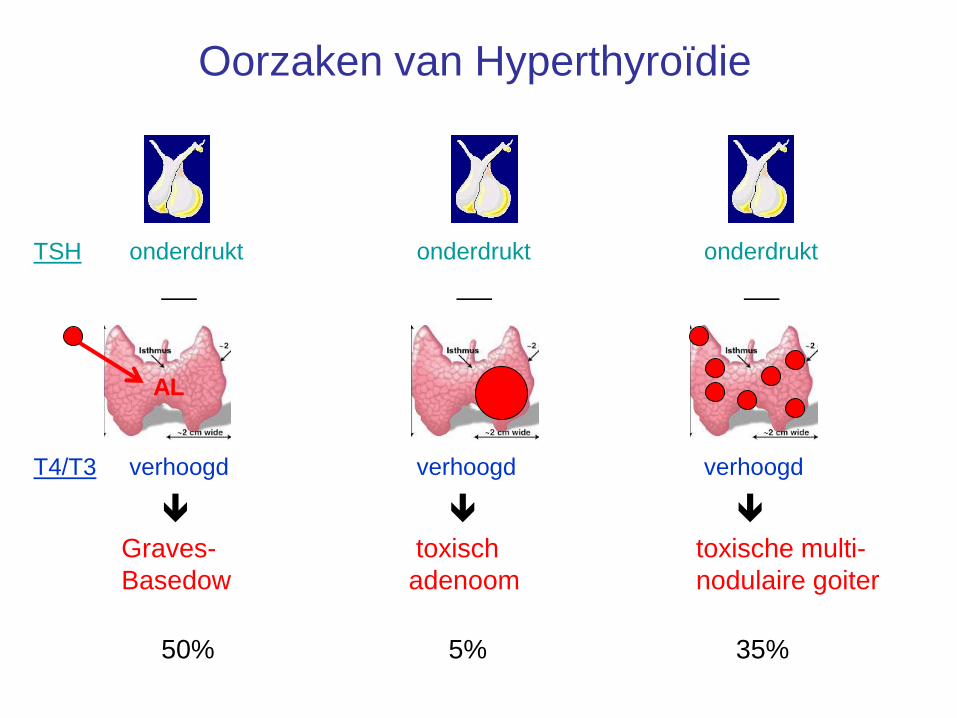
Oorzaken van Hyperthyroïdie
TSH onderdrukt onderdrukt onderdrukt
T4/T3 verhoogd verhoogd verhoogd
Graves- toxisch toxische multi-
Basedow adenoom nodulaire goiter
AL
50% 5% 35%

Oorzaken van Hyperthyroïdie
TSH onderdrukt onderdrukt onderdrukt
T4/T3 verhoogd verhoogd verhoogd
Destructie iodium- iatrogeen
Infectieus geïnduceerd
<1% 5% <1%
T4
T4T4
T4
T4
T4
I I
II I
IX

Ziekte van Graves-Basedow
• Meest frequente oorzaak van
hyperthyroïdie (50-80%)
– Prevalentie: 5% vd bevolking
– Piekincidentie: 30-40 jaar

• geslacht: vrouw/man ratio bedraagt 7/1
• leeftijd: na de puberteit
• stress
• overmaat aan iodiuminname
• associatie met andere autoimmuunziekten (autoimmune
thyroïditis, type 1 diabetes mellitus, pernicieuze anemie,
ziekte van Addison, vitiligo, …)
• genetische susceptibiliteit :
– studies met monozygote tweelingen (concordantie van 20-40%)
– HLA DR3
– CTLA-4 allelen (cytotoxic T lymphocyte-associated protein 4)
Risicofactoren Graves-Basedow
• anamnese en kliniek: hyperthyroïdie
• palpatie schildklier:
– 90% vertoont een diffuse goiter die 2-3x vergroot is
– thrill e/o souffle
• 20% vertoont oftalmopathie; 5% dermopathie (myxoedeem pretibiaal)
• Labo:
– TSH ↓, FT4 en FT3 ↑
– TSH receptor antilichamen
• bevestigen klinische diagnose
• positief in 80-90%
• blijvend hoge titers zijn predictief voor recidieve
• lage titers hebben geen prognostische waarde
– TPO antilichamen
• scintigrafie
diagnose Graves-Basedow

Kliniek en scintigrafie van de ziekte van Graves
Scintigrafie:
uitgesproken capatie thv SK,
weinig achtergrondcapatie

Graves’ oftalmopathie
• Ooglidretractie
• Proptosis
• Diplopie en beperkte oogbewegingen

Graves’ oftalmopathie
• oedeem en roodheid bovenste
ooglid, conjunctivale injectie en
ernstige chemosis vh linker oog
• oedeem en retractie van het
ooglid en exoftalmie
• conjuctivale injectie en
chemosis, beperkingin
oogbeweging, N. Opticus-
neuropathie

• Antithyroïdea:
– propylthiouracyl / methimazole gedurende 4-6 weken alvorens normalisatie schildkliertesten
– nadien: “block and replace” gedurende 6-12-18 maanden• zelfde dosis antithyroïdea of afbouwend
• + levothyroxine (50-100 µg/d)
– stop wanneer TSH-R-AL negativeren
• -blokkers
- adjuvante therapie in begin fase
- propanolol (Inderal) 3-4x 40 mg/d
- metoprolol (Seloken ) 1x 100 mg/d
Medische Behandeling Graves-Basedow (II)

• 3-15 mCi
na voorbereiding met antithyroïdea
nadien antithyroïdea afbouwend
• indicaties
- recidief
- allergie op antithyroïdea
• complicaties
- recidieve hyperthyroïdie 1-10%
- permanente hypothyroïdie 80%
- exarcerbatie oftalmopathie 10%
( preventie met corticoïden)
- geen inductie maligniteit
Radio-actief I* Behandeling Graves-Basedow

• bilaterale thyroïdectomie
na voorbereiding met antithyroïdea en iodium
• indicaties
- grote goiter
- recidief
- allergie op antithyroïdea
• complicaties
- recidief hyperthyroïdie 1-10%
- permanente hypothyroïdie 80-90%
- hypoparathyroïdie 0-3%
- stemband paralyse 0-3%
Chirurgische Behandeling Graves-Basedow

Thyroïditis
Pearce EN et al. NEJM 2003
hyperthyroïdie
(1-3 maand)
hypothyroïdie
(3-8 maand)euthyroïdie

Post-partum (Lymfocytaire) Thyroïditis
• zelfde pathogenese als silencieuze lymfocytaire thyroïditis: autoimmuun
• kliniek:
- 8-10% van bevallingen
- 3-6 maanden post-partum
- beperkt gevoelige, niet-harde goiter
- positieve TPO-antilichamen
• evolutie:
- hyperthyroïdie hypothyroïdie herstel
- recidieven definitieve hypothyroïdie

SCHILDKLIER & DIABETES

Prevalentie van schildklierlijden bij
diabetes
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139

Prevalentie van schildklierlijden bij diabetes
• Schildklierlijden komt meer bij T1DM dan bij T2DM voor
• Longitudinale data tonen dat 1/3 vd T1DM patiënten een gestoorde
SK functie ontwikkelt
• Postpartum SK dysfunctie treedt op bij tot 25% vd vrouwen met
T1DM
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139
Umpierrez et al. Diab Care 2003; 26: 1181-1185. Gerstein HC. Ann Intern Med 1993; 118: 419-423.

TYPE 1 DIABETES & AUTOIMMUNITY
• Insulitis & -cell AAb (ICA, GADA, IA-2A, IAA, ZnT8 Ab)
• HLA DR/DQ : 50% of the genetic risk
• Associated organ-specific AAb: T1 DM vs non-DM
• TPO: thyroid peroxidase Ab 10-25 % 2-4 %
• PCA: parietal cell Ab 10-25 % 1.5-10 %
• EmA-IgA: anti-endomysium Ab 0.5-10 % 0-0.5 %
• AAA: anti-adrenal Ab 1.5-3 % 0-0.5 %
• ~18-20% of t1DM pts have APS
Collin 2002, De Block 2001
Betterle 1984, Bottazzo 1974, Eisenbarth 1986, Gorus 1997, Landin-Olsson 1992, Maclaren 1985

TYPE 1 DIABETES & AUTOIMMUNITY
De Block 2001 Clin Exp Immunol; De Block JCEM 2001
0
5
10
15
20
25
30
35
40
45
%
0-12 13-19 20-29 30-39 40-49 > = 50
age (y)
aTPO+ (m)
aTPO+ (f)PCA+ (m)
PCA+ (f)

Autoimmuun schildklierlijden bij T1DM
• Autoimmuun schildklierlijden (AITD) kan
voorkomen
– in associatie met enkel T1DM
– in kader van een autoimmuun polyglandulair
syndroom
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139

Autoimmuniteit bij T1DM
Barker et al. JCEM 2006

Betterle C et al., Exp Clin Immunol 2004
Autoimmune Polyendocrine Syndromes

Eisenbarth, G. S. et al. N Engl J Med 2004;350:2068-2079
Autoimmune Polyendocrine Syndromes

AITD in autoimmune disorders:
Disease or ABGeneral
populationT1 DM Coeliac disease Addison's Hypothyroidism
T1 DM
anti-islet Ab
2-3%
1-3%
xxx
85-90%12-14% 4%
Coeliac
transglutaminase Ab
0.5%
0.5-1%
1-8%
8-12%
xxx
99%5% 4%
Addison's
21-hydroxylase Ab
0.005%
0-0.6%
0.5%
0.7-3%
xxx
83-90%
Hypothyroidism 5-9% 30% 3-12% 14-21% xxx
aTPO2-10% in adults
1-4% in children
15-30% in adults
5-22% in children18% 23-40% 47-83%
Graves'
TSH Rec Ab
0.1-2%
?
6-10%
?10-20%
Pernicious anemia/
Autoimmune gastritis
2% for AIG
0.15-1% for PCA
5-10% for AIG
2-4% for PCA
PCA 2.5 - 12%15-25% in adults
10-15% in children
Table 1. Prevalence of organspecific autoantibodies and autoimmune diseases.
6% 2%
Adapted from Van den Driessche, Eenkhoorn V, Van Gaal L, De Block C; Neth J Med 2009
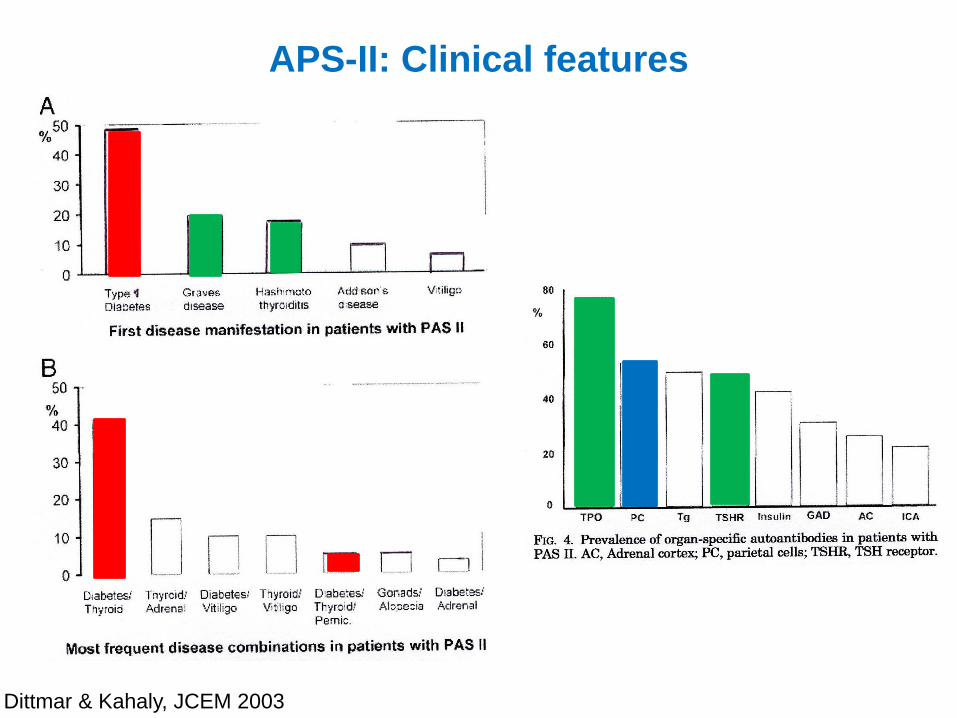
APS-II: Clinical features
Dittmar & Kahaly, JCEM 2003

De Block, C. E. M. et al. J Clin Endocrinol Metab 2008;93:363-371
Prevalence of PCA, AIF, autoimmune gastritis, and pernicious anemia in the general population and endocrine diseases
• aTPO:
– T1DM:
• subklinische SK dysfunctie: 5-20%
• manifeste hypothyroidism: 2-6%
• Hashimoto thyroiditis:
– suboptimale groei bij kinderen,
– vertraagde ontwikkeling van bot en tanden bij kinderen,
– obstipatie
– koudeintolerantie
– trage pols
– fertiliteit ↓
Dayan 1996, McKenna 1990, Mouradian 1983, Vanderpump 1995, Riley 198, De Block 2001
Hypothyroidie bij diabetes

Hypothyroidie bij diabetes
• hypoglycemierisico ↑ tgv
– ↓ hepatic glucose output
– ↓ gluconeogenese
• behandeling van hypothyroidie vermindert het hypo-risico
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139 Mohn et al. Diab Med 2002; 19: 70-73
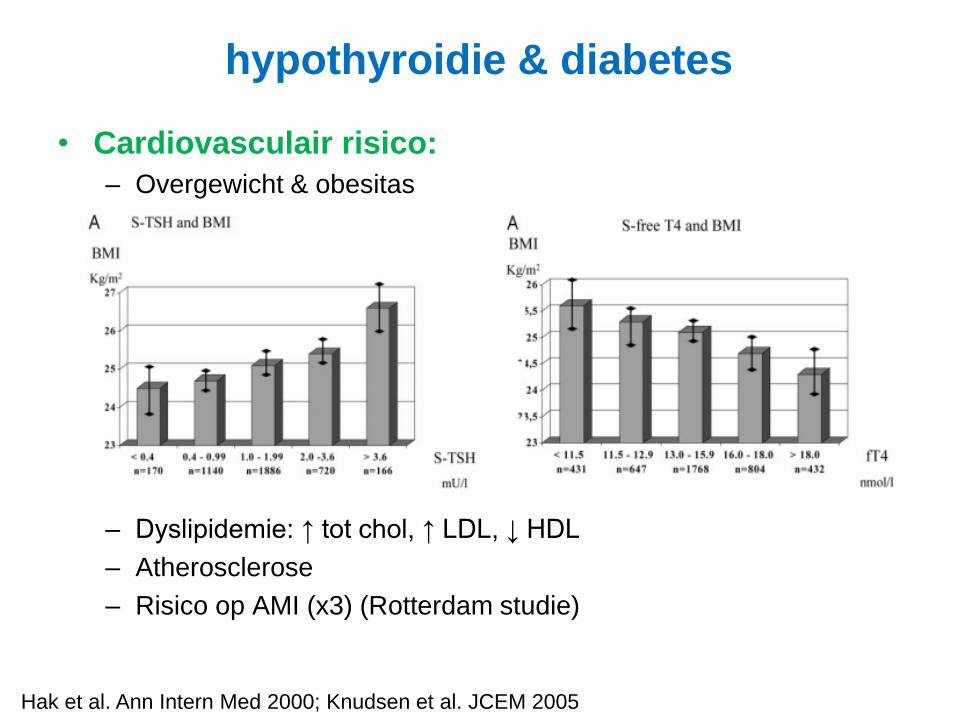
• Cardiovasculair risico:
– Overgewicht & obesitas
– Dyslipidemie: ↑ tot chol, ↑ LDL, ↓ HDL
– Atherosclerose
– Risico op AMI (x3) (Rotterdam studie)
Hak et al. Ann Intern Med 2000; Knudsen et al. JCEM 2005
hypothyroidie & diabetes

• Cardiovasculair risico:
– Endotheeldysfunctie
– Diastolische hypertensie
– Cardiovasculaire pathologie
Cappola et al. JAMA 2006
hypothyroidie & diabetes
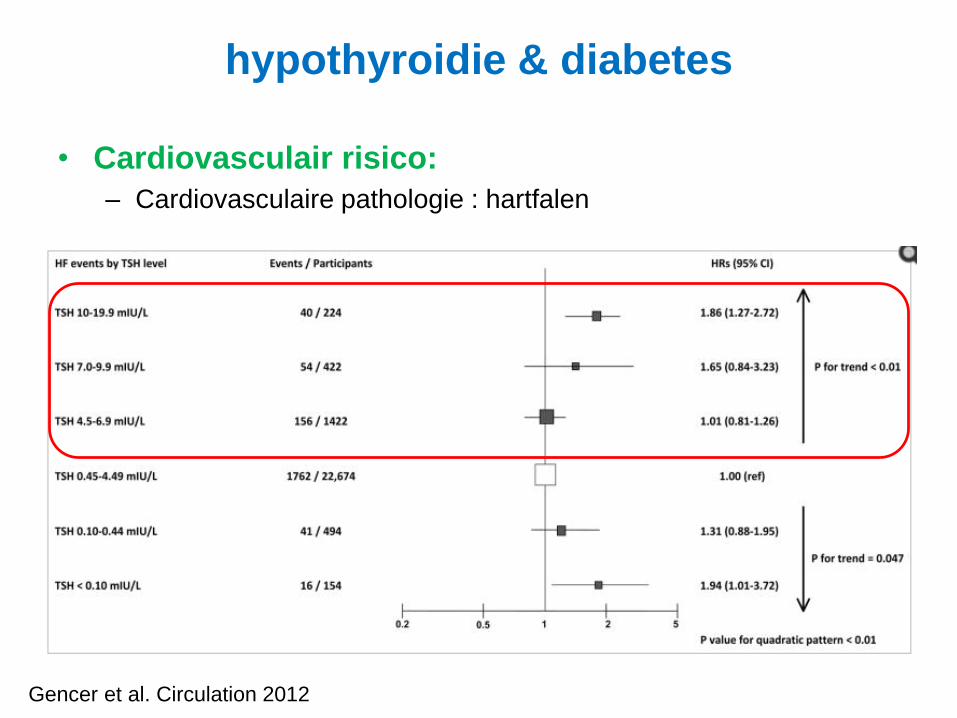
• Cardiovasculair risico:
– Cardiovasculaire pathologie : hartfalen
Gencer et al. Circulation 2012
hypothyroidie & diabetes

• Cardiovasculair risico:
Kahaly & Dilman; Endo Rev 2005
hypothyroidie & diabetes

Hyperthyroidie bij diabetes
• Ziekte van Graves - Basedow:
– gewichtsverlies
– warmte-intolerantie
– tremor
– zwakte
– uitputting
– exophtalmie
– moeilijker glycemiecontrole
– cardiale problemen
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139

Hyperthyroidie bij diabetes
• Glycemieregeling:
– Hyperthyroidie verergert de glucose intolerantie oiv:
• ↑ intestinale absorptie van glucose
• ↑ glucose productie: gluconeogenesis & glycogenolysis,
• ↓ insulinesensitiviteit
• ↑ renale klaring van insuline
• ↑ hepatic glucose output
• ↑ lipolyse
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139 Potenza et al. Endocr Pract 2009

• Cardiovasculair risico:
– tachycardie
– 10-15% : VKF → cave CVA
Kahaly & Dilman; Endo Rev 2005
hyperthyroidie & diabetes

• Cardiovasculair risico:
– voorkamerfibrillatie
Boelaert & Franklyn, J Endocrinol 2005
hyperthyroidie & diabetes

• Cardiovasculair risico:
– Cardiovasculaire pathologie : hartfalen
Gencer et al. Circulation 2012
hyperthyroidie & diabetes

• Cardiovasculair risico:
– Cardiovasculaire pathologie : mortaliteit bij ouderen
Parle et al. Lancet 2001
hyperthyroidie & diabetes

Screenen ?
• Geen consensus over noodzaak tot screenen voor SK
pathologie in de routine diabeteszorg
• Welke test gebruiken om te screenen ?
• Wanneer screenen ?
• Hoe frequent screenen, met welke intervallen ?

Aanbevelingen
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139

Aanbevelingen
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139
AITD in T1DM
• Current recommendations from the American Diabetes Association
are to screen T1DM patients for dysthyroidism using TSH &
antibodies at onset of diabetes, or in case of symptoms of hypo-or
hyperthyroidism, and TSH every 1 to 2 years thereafter.
• Since patients who are TPO antibody positive have an 18-fold
increased risk of developing thyroid disease than patients who are
TPO antibody negative, we and others suggests to screen T1DM
patients using TPO autoantibodies, TSH and T4 levels at onset of
T1DM and yearly thereafter.
Van den Driessche, Eenkhoorn V, Van Gaal L, De Block C; Neth J Med 2009

Aanbevelingen
Kadiyala et al. Int J Clin Pract 2010; 64: 1130-1139

If it were not for the
variability among
individuals, Medicine might
aswell be a Science and not
an Art
Sir William Osler, 1892

Thank you for your attention





























