Embed Size (px)
Citation preview
VOL. 72, NO. 5 NOTES, CASES, INSTRUMENTS 1013
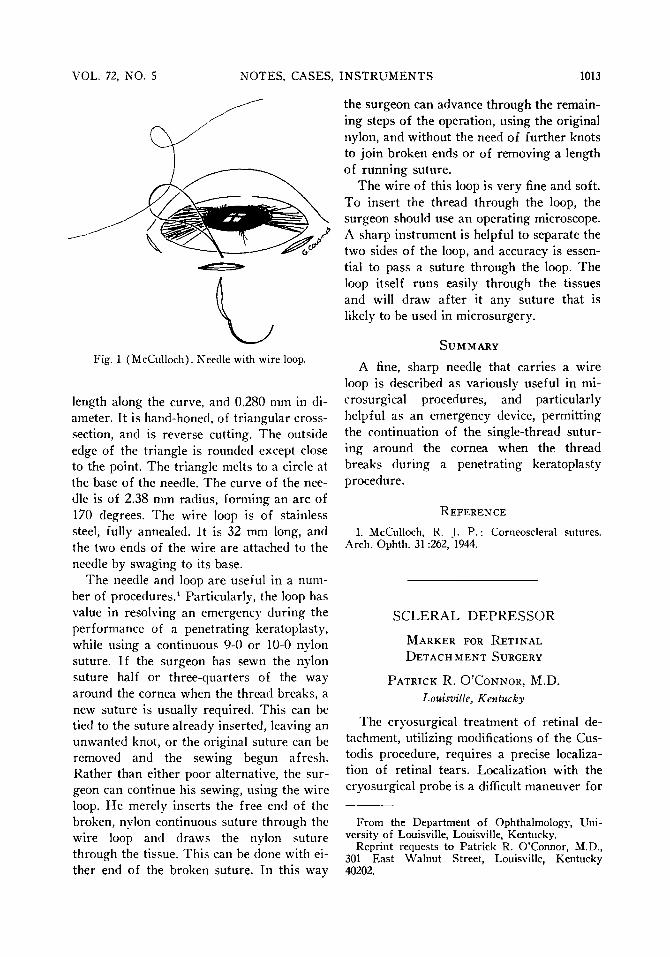
Fig. 1 (McCulloch). Needle with wire loop.
length along the curve, and 0.280 mm in diameter. It is hand-honed, of triangular cross-section, and is reverse cutting. The outside edge of the triangle is rounded except close to the point. The triangle melts to a circle at the base of the needle. The curve of the needle is of 2.38 mm radius, forming an arc of 170 degrees. The wire loop is of stainless steel, fully annealed. It is 32 mm long, and the two ends of the wire are attached to the needle by swaging to its base.
The needle and loop are useful in a number of procedures.1 Particularly, the loop has value in resolving an emergency during the performance of a penetrating keratoplasty, while using a continuous 9-0 or 10-0 nylon suture. If the surgeon has sewn the nylon suture half or three-quarters of the way around the cornea when the thread breaks, a new suture is usually required. This can be tied to the suture already inserted, leaving an unwanted knot, or the original suture can be removed and the sewing begun afresh. Rather than either poor alternative, the surgeon can continue his sewing, using the wire loop. H e merely inserts the free end of the broken, nylon continuous suture through the wire loop and draws the nylon suture through the tissue. This can be done with either end of the broken suture. In this way
the surgeon can advance through the remaining steps of the operation, using the original nylon, and without the need of further knots to join broken ends or of removing a length of running suture.
The wire of this loop is very fine and soft. To insert the thread through the loop, the surgeon should use an operating microscope. A sharp instrument is helpful to separate the two sides of the loop, and accuracy is essential to pass a suture through the loop. The loop itself runs easily through the tissues and will draw after it any suture that is likely to be used in microsurgery.
S U M M A R Y
A fine, sharp needle that carries a wire loop is described as variously useful in mi-crosurgical procedures, and particularly helpful as an emergency device, permitting the continuation of the single-thread suturing around the cornea when the thread breaks during a penetrating keratoplasty procedure.
R E F E R E N C E
1. McCulloch, R. T. P. : Corneoscleral sutures. Arch. Ophth. 31:262, "1944.
S C L E R A L D E P R E S S O R
M A R K E R FOR R E T I N A L
D E T A C H M E N T SURGERY
P A T R I C K R. O ' C O N N O R , M.D.
Louisville, Kentucky
The cryosurgical treatment of retinal detachment, utilizing modifications of the Cus-todis procedure, requires a precise localization of retinal tears. Localization with the cryosurgical probe is a difficult maneuver for
From the Department of Ophthalmology, University of Louisville, Louisville, Kentucky.
Reprint requests to Patrick R. O'Connor, M.D., 301 East Walnut Street, Louisville, Kentucky 40202.

1014 AMERICAN JOURNAL OF OPHTHALMOLOGY NOVEMBER, 1971
the inexperienced assistant because no visible lesion remains on the scleral surface after freezing.
Gass1 introduced a scleral marker in 1966. It resembled the thimble-type scleral depressor with a hollow, stainless steel tube attached to its tip after the cross bar was removed. When applied to the sclera with moderate pressure, a dark, ring-shaped impression remains for 20 seconds. The sclera is then permanently tattooed with a marking pencil. The Gass instrument was found superior to other available markers, but had several disadvantages. Even with rotation of the eye, locating posteriorly positioned tears remains a difficult exercise because the curvature of the instrument prevents its use deep within the bony orbit. The tip of the instrument does not glide smoothly over the scleral surface and is unsatisfactory when dealing with small retinal holes which require scleral indentation and a careful retinal examination prior to marking.
In order to alleviate these two problems, a new instrument was designed which
combines a scleral depressor and marker.* The marking portion incorporates the same tip found on the Gass instrument. It is mounted on a flat, straight handle to provide easy access to the posterior sclera without ocular rotation or interference from the orbital rim. Scleral marking^ of retinal tears is accomplished in the manner described for the Gass design. The smooth, round tip of the opposite end serves as a scleral depressor and avoids tissue damage during the pre-marking examination.
S U M M A R Y
To facilitate scleral marking of retinal tears in surgical treatment of retinal detachments, the Gass scleral marker was mounted on a flat, straight handle. A smooth round tip on the opposite end of the handle serves as a scleral depressor.
REFERENCE
1. Gass, J. D. M.: Scleral marker for retinal detachment surgery. Arch. Ophth. 76 :700, 1966.
* Available from Storz Instrument Company, St. Louis, Missouri.





























