Embed Size (px)
Citation preview

DISCUSIÓN POSTERS: CÁNCER DE MAMA
SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
LOURDES CALVO

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
3sns
eom
Con la colaboración de:12--PE Héctor Randhall Callata Carhuapoma DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
3sns
eom
Con la colaboración de:12--PE Héctor Randhall Callata Carhuapoma DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
3sns
eom
Con la colaboración de:12--PE Héctor Randhall Callata Carhuapoma DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
DESCRIBE LA CORRRELACIÓN entre IHQ y FISH SIGUIENDO LAS GUÍAS DE ASCO/CAP DEL 2007. Serie retrospecDva de 113 pacientes .
3sns
eom
Con la colaboración de:12--PE Héctor Randhall Callata Carhuapoma DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
22% QTNA RCP: 52% HER2/CEP17> 3: 57% HER2/CEP17< 3: 42%
SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
RECOMMENDATIONS
What Is the Optimal Testing Algorithm for theAssessment of HER2 Status?
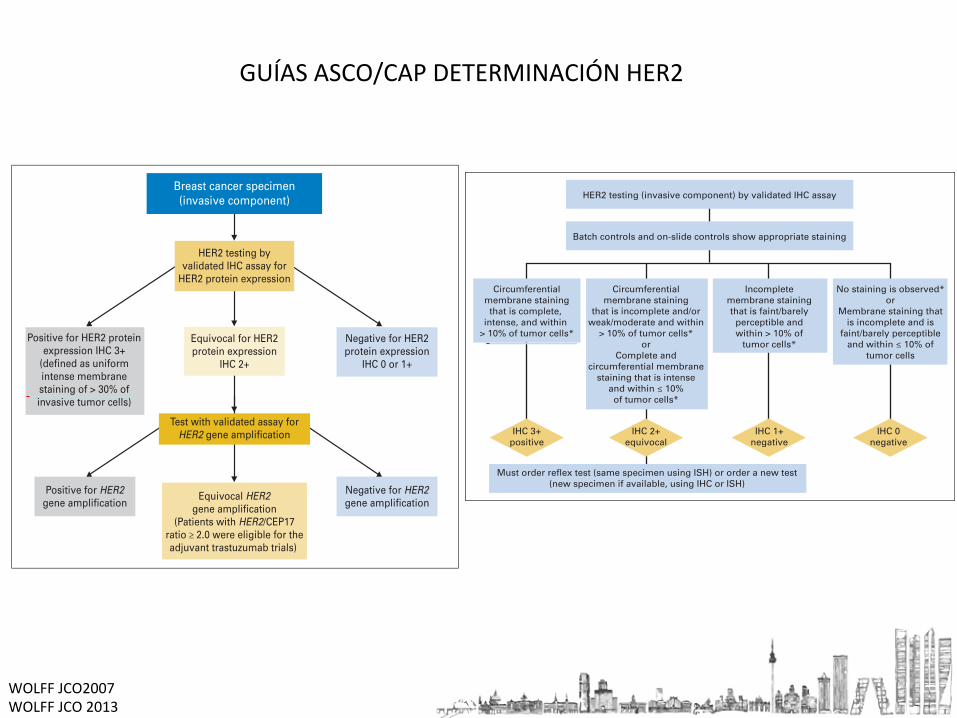
Summary and recommendations. The literature review and re-sultant panel discussion elucidated three categories of HER2 testingresults leading to different clinical decisions for patients with breastcancer. The test, regardless of method used, can be found to bepositive, equivocal, or negative. Each of these test results triggersdefined patient management algorithms as shown in Figures 1(IHC) and 2 (FISH).
In all cases, it is assumed that the test being used is accurate andreproducible based on good laboratory practices as defined later in thisarticle. In order to classify a HER2 test as either positive or negative, thelaboratory must have performed concordance testing with a validatedFISH assay and confirmed that only 5% or less of samples classified aseither positive or negative disagree with that validated assay on anongoing basis. If the laboratory cannot satisfy this criterion, it shouldnot perform HER2 testing and should send specimens to a referencelaboratory. Equivocal cases are not expected to 95% concordant,rather they should be subjected to a confirmatory test. Concordancetesting should be annually confirmed. A minority view expressedwithin the panel was that IHC is not a sufficiently accurate assay todetermine HER2 status and that FISH should be preferentially used.
It is important to note that concordance of assays does not assureaccuracy (ie, how close the measured values are to a supposed truevalue; Appendix F). Evaluating accuracy of a test requires comparisonto a gold standard. There is no gold standard at present; no assay
currently available is perfectly accurate to identify all patients expectedto benefit or not from anti-HER2 therapy.
The following definitions have been accepted for analysis ofHER2. It is critical that these analyses be conducted on the invasivecomponent of the breast cancer, because HER2 is, for unclearreasons, frequently increased (overexpressed and/or over ampli-fied) in in situ breast cancer, and the clinical implications of thisfinding are uncertain.53
Positive HER2 test. Based on a literature review of clinicaltrials, international studies and protocols, expert consensus, andUS Food and Drug Administration Panel findings, a positive HER2test is defined as either IHC result of 3! cell surface proteinexpression (defined as uniform intense membrane staining of "30% of invasive tumor cells) or FISH result of amplified HER2 genecopy number (average of " six gene copies/nucleus for test systemswithout internal control probe) or HER2/CEP 17 ratio of morethan 2.2, where CEP 17 is a centromeric probe for chromosome 17on which the HER2 gene resides. The 30% criteria for a positiveIHC is further discussed in Appendix G. The original FISH testresults were defined as either positive or negative, but an interme-diate range (from hereon referred to as equivocal range) has sincebeen described and the clinical significance of this observationremains unclear.34-36 This strategy classifies patients as havingHER2-positive disease based on positive results with either test. Itis recognized that current data are insufficient to define whetherthese patients represent true- or false-positives. Although the largeprospective randomized clinical trials of trastuzumab were notprospectively designed to answer these questions, we anticipate
Equivocal HER2gene amplification
(Patients with HER2/CEP17ratio ≥ 2.0 were eligible for theadjuvant trastuzumab trials)
Breast cancer specimen(invasive component)
HER2 testing byvalidated IHC assay for
HER2 protein expression
Equivocal for HER2protein expression
IHC 2+
Test with validated assay forHER2 gene amplification
Negative for HER2protein expression
IHC 0 or 1+
Positive for HER2gene amplification
Negative for HER2gene amplification
Positive for HER2 protein expression IHC 3+
(defined as uniform intense membrane staining of > 30% of invasive tumor cells)
Fig 1. Algorithm for immunohistochemis-try (IHC). For additional information regard-ing adjuvant trastuzumab trials see Slamonet al,19 Romond et al,21 Piccart-Gebhart etal,22 and HERA trial study.23 HER2, humanepidermal growth factor receptor 2.
Guideline for HER2 Testing in Breast Cancer
www.jco.org 125 www.asco.org on October 19, 2014 - Published by jco.ascopubs.orgDownloaded from
Copyright © 2006 by the American Society of Clinical Oncology and College of American Pathologists. All rights reserved.
Other HER2-targeted drugs (eg, the kinase inhibitor lapatinib,32
the antibody pertuzumab,33 and the antibody-drug conjugate ado-trastuzumab emtansine [T-DM1]34) have been approved for thetreatment of HER2-positive metastatic breast cancer. At the sametime, data show that lapatinib (when added to paclitaxel)35 and per-tuzumab (as a single agent)36 offer no clinical benefit in patients withHER2-negative metastatic disease. These new HER2-targeted drugsare now being tested in the adjuvant setting, including in studiesevaluating their adjuvant role alone or in dual-antibody regimenswithout concomitant or sequential chemotherapy. Compared withregimens already in use, the newer agents are as or more expensive,and they may be associated with other dose-limiting toxicities,such as skin and GI tract toxicities with lapatinib and liver toxicitieswith ado-trastuzumab emtansine.37
Therefore, the need for an updated ASCO/CAP guideline onaccurate HER2 testing to ensure that the right patient receives the righttreatment is now more critical than ever.22,24-27,38 Since the publica-tion of the 2007 HER2 testing guideline, CAP has observed a remark-able uptake of proficiency testing (Fig 4),5 with nearly 1,500laboratories currently participating. CAP has also observed fewerlaboratories experiencing deficiencies on laboratory inspection.Indirect evidence suggests that the performance of laboratoriesthat conduct HER2 testing in the United States and elsewhere isimproving.39-42 Available evidence and experience since 2007 rein-force the importance of robust validation of new assays by labora-tories before clinical implementation, as well as their ongoingmonitoring, and the value of various external quality assuranceschemes adopted in many countries.
METHODS
The HER2 testing Update Committee (Appendix Table A1, online only) metthree times via Webinars coordinated by its Steering Committee to review the
data published from January 2006 to January 2013 and to revise the recom-mendations. Additional data were gathered from in-press publications andpersonal correspondence with researchers to address the issue of mandatorytesting if a test result is 0 or 1!. Draft manuscripts were circulated by e-mail,and the Update Committee approved the final manuscript. This guideline wasreviewed by external reviewers and approved by the ASCO Clinical PracticeGuideline Committee and relevant CAP entities.
Literature Search StrategyThe MEDLINE and the Cochrane Collaboration Library electronic da-
tabases were searched with the date parameters of January 2006 throughJanuary 2013 for articles in English. The MEDLINE search terms are includedin Data Supplement 3, and a summary of the literature search results isprovided in Data Supplement 4.
Inclusion and Exclusion CriteriaArticles were selected for inclusion in the systematic review of the evi-
dence if they met the following criteria : (1) the study compared, prospectivelyor retrospectively, fluorescent ISH (FISH) and immunohistochemistry (IHC)results or other tests; described technical comparisons across various assayplatforms; examined potential testing algorithms for HER2 testing; or exam-ined the correlation of HER2 status in primary versus metastatic tumors fromthe same patients; (2) the study population consisted of patients with a diag-nosis of invasive breast cancer; or (3) the primary outcomes included thenegative predictive value (NPV) or positive predictive value (PPV) of ISH andIHC assays used to determine HER2 status, alone and in combination; nega-tive and positive concordance across platforms; and accuracy in determiningHER2 status and benefit from anti-HER2 therapy and in determining sensi-tivity and specificity of individual tests. Consideration was given to studies thatdirectly compared results across assay platforms.
Studies were not limited to randomized controlled trials but also in-cluded other study types, including cohort designs, case series, evaluationstudies, and comparative studies. The Update Committee also reviewed othertesting guidelines and proficiency strategies of various US and internationalorganizations, including unpublished data. Letters, commentaries, and edito-rials were reviewed for any new information. Case reports were excluded. Theclinical questions addressed in the update are available in Data Supplement 5.
HER2 testing (invasive component) by validated IHC assay
Batch controls and on-slide controls show appropriate staining
Must order reflex test (same specimen using ISH) or order a new test(new specimen if available, using IHC or ISH)
Circumferentialmembrane stainingthat is complete,
intense, and within > 10% of tumor cells*
Circumferentialmembrane staining
that is incomplete and/orweak/moderate and within
> 10% of tumor cells*or
Complete andcircumferential membrane
staining that is intenseand within ≤ 10%of tumor cells*
Incompletemembrane stainingthat is faint/barely
perceptible andwithin > 10% of
tumor cells*
No staining is observed*or
Membrane staining thatis incomplete and is
faint/barely perceptibleand within ≤ 10% of
tumor cells
IHC 3+positive
IHC 2+equivocal
IHC 1+negative
IHC 0negative
Fig 1. Algorithm for evaluation of humanepidermal growth factor receptor 2 (HER2)protein expression by immunohistochem-istry (IHC) assay of the invasive compo-nent of a breast cancer specimen.Although categories of HER2 status byIHC can be created that are not coveredby these definitions, in practice they arerare and if encountered should be consid-ered IHC 2! equivocal. ISH, in situ hybrid-ization. NOTE: the final reported resultsassume that there is no apparent histo-pathologic discordance observed by thepathologist. (*) Readily appreciated usinga low-power objective and observedwithin a homogeneous and contiguousinvasive cell population.
Wolff et al
4000 © 2013 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
from 217.124.244.63Information downloaded from jco.ascopubs.org and provided by at Conselleria de Sanidade - SERGAS on October 19, 2014
Copyright © 2013 American Society of Clinical Oncology. All rights reserved.
GUÍAS ASCO/CAP DETERMINACIÓN HER2
WOLFF JCO2007 WOLFF JCO 2013

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
3sns
eom
Con la colaboración de:13--PE María José Bueno Verdejo DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
ObjeDvo: Estudiar el papel de la sintasa de ácidos grasos (FASN) en la transformación oncogénica mamaria.
• Material y Métodos: Modelo animal mul2-‐transgénico de delección condicional de FASN en ratones MMTV-‐PyMT que presentan tumores hormonoposi2vos asociados a la expresión del oncogén PyMT.
• Estudio del efecto de la Delección de FASN en la tumorogénesis mamaria comparando el crecimiento tumoral y supervivencia con y sin delección de FASN en los ratones MMTV-‐PyMT.

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
3sns
eom
Con la colaboración de:13--PE María José Bueno Verdejo DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
CONCLUSIONES EL papel limitante de FASN en la tumorogénesis mamaria podría ser una estrategia atracDva para la quimioprevención del cáncer de mama.

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
ObjeDvo: IdenDficar marcadores predicDvos de mala respuesta a QTN (RCB-‐III) y de recaída en el momento del diagnósDco.
Material y Métodos: E. RetrospecDvo 115
pacientes tratadas con Antrac y Taxanos.
Tiempo de seguimiento 150 meses. (1996-‐2011)
25 pacientes metástasis.
35 pacientes RCB-‐III (37% Metástasis).
3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
El estudio propone dos firmas predicDvas
1. FP de Quimioresistencia: OR= 29,1; S=38% y E=98%
2. FP de metástasis: OR= 14,5; S=66,6% y E=87,9%
El disponer de marcadores predicDvos de respuesta a QTNA y de supervivencia pueden ayudar a seleccionar la mejor estrategia para cada paciente.
3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
3sns
eom
Con la colaboración de:14--PE SERAFIN MORALES MURILLO DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
3sns
eom
Con la colaboración de:16--PE Katerin Ingrid Rojas Laimito DOI: 10.3252/pso.es.3snseom.2014
Mama Avanzada
ObjeDvo: Valorar la influencia de la PCR en la S tras QTNA
3sns
eom
Con la colaboración de:16--PE Katerin Ingrid Rojas Laimito DOI: 10.3252/pso.es.3snseom.2014
Mama Avanzada
3sns
eom
Con la colaboración de:16--PE Katerin Ingrid Rojas Laimito DOI: 10.3252/pso.es.3snseom.2014
Mama Avanzada
Confirma los datos de otras series de que la RPC se asocia a mayor SG y SLE.

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
3sns
eom
Con la colaboración de:15--PE ABRAHAM HERNÁNDEZ BLANQUISETT DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
Serie de 35 pacientes CMG Octubre 1990-‐Oct 2013. Grupo A: 11 pacientes CM durante la gestación
Grupo B: 24 pacientes CM en los 12 meses siguientes al parto.
No hubo diferencias significaDvas entre los grupos ni para las caracterísDcas clínico-‐patol ni para el tratamiento.
En el seguimiento 11 han recaído y 5 han muerto.
SLE: 69% y 45% a los 5 y 10 años
SG: 90,8% y 74,2% a los 5 y 10 años
CONCLUSIONES
No hubo diferencias en SLE ni en SG entre los grupos.
Alto porcentaje de afectación ganglionar à mal pronósDco.
3sns
eom
Con la colaboración de:15--PE ABRAHAM HERNÁNDEZ BLANQUISETT DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana
3sns
eom
Con la colaboración de:15--PE ABRAHAM HERNÁNDEZ BLANQUISETT DOI: 10.3252/pso.es.3snseom.2014
Mama Temprana

SIMPOSIOSEOM
03
MADRID 2014 22, 23 Y 24 OCTUBRE HOTEL NH-EUROBUILDING
PROGRAMA CIENTÍFICO
Fundación
www.seom2014.org
Declarado de interés sanitario por: Acreditado por:
21, category 1 ESMO-MORA points
3sns
eom
Con la colaboración de:17--PE Isabel Blancas López-Barajas DOI: 10.3252/pso.es.3snseom.2014
Mama Avanzada
Estudio observacional, retrospecDvo y mulDcéntrico.
OP: Evaluar respuesta a Fulvestrant 500 en SLP, en p post-‐menop con RH+ y fallo a una línea hormonal.
Material y Métodos:
Tratadas entre En 2010-‐Jun 2012.
25 centros, 263 pacientes evaluables Met viscerales: 38 (14,4%)
3sns
eom
Con la colaboración de:17--PE Isabel Blancas López-Barajas DOI: 10.3252/pso.es.3snseom.2014
Mama Avanzada
3sns
eom
Con la colaboración de:17--PE Isabel Blancas López-Barajas DOI: 10.3252/pso.es.3snseom.2014
Mama Avanzada

13/06/14 01:52Eyewitness: 12,000 light years from Earth | World news | theguardian.com
Página 1 de 2http://www.theguardian.com/world/picture/2014/mar/13/eyewitness-12000-light-years-from-earth
Search
At 1,300 times the diameter of our sun (making it an extraordinary 1.1bn miles across)and more than a million times brighter, the yellow hypergiant HR 5171 A is a genuine
Eyewitness: 12,000 light years fromEarthPhotographs from the Guardian Eyewitness series
theguardian.com, Thursday 13 March 2014 09.43 GMT
GRACIAS





























