Embed Size (px)
Citation preview

1

What is an Opioid? Opiates as defined from MedcineNet: A medication
or an illegal drug that is derived from the opium poppy or that mimics the effect of an opiate (a synthetic opiate). Opiate drugs are narcotic sedatives that depress activity of the central nervous system, reduce pain, and induce sleep
Opiates work by interacting with the Opioid Receptors on the nerve cells in the brain and nervous system to produce pleasurable effects and ultimately relieve pain
Some additional Info
Narcotic -refers to opioids and opioid derivatives
Oxycodone versus Oxycontin- Oxycodone is the
actual substance(opioid) in Oxycontin, Oxycontin is
a 12 hr sustained release form of oxycodone
2

Shocking Stats US Opioid Use
According to the National Survey on Drug Use and Health over 2 million Americans are
currently addicted to opioids
In 2012, 259 million prescriptions were written for opioids, which is more than enough to
give every American adult their own bottle of pills
61% of drug overdoses from 2014 were related to prescription drugs containing opioids
Direct correlation between increase in prescriptions and overdose rates
3

Chasing the Pain- How the Epidemic Started
The opioid epidemic specifically the use of Oxycontin, the largest prescribed opioid, can be attributed to three main factors:
New trend in Pain Pharmacology starting in the early 1980’s
Strategic marketing campaign lead by Purdue Pharma, the maker of
Oxycontin
Change(liberalization)in physicians prescribing habits for opioids
4

Change in Pain Pharmacology 1980’s
Historically opiates and narcotics had been prescribed primarily for cancer patients with
chronic pain
Starting in the early 1980’s shift in the usage of opiates starts to occur
Used for chronic non-cancer patients i.e.. dental pain, orthopedic pain
Two articles were posted in Medical journals in support of opioid use
New England Journal of Medicine “reported that less than one percent of patients at Boston
University Medical Center who received narcotics while hospitalized became addicted.”
Journal of Pain advocating for non-cancer patient use, “narcotics can be safely and effectively
prescribed to selected patients with relatively little risk of producing the maladaptive behaviors
which define opioid abuse.”
5

Change in Pain Pharmacology 1980’s Cont’d
“While the number of cancer patients was not likely to increase drastically
from one year to the next, if a company could expand the indications for use
of a particular{narcotic} drug, then it could boost sales exponentially without
any real change in the country's health demography.”- Mike Mariani
This atmosphere created the perfect storm for Oxycontin to hit the market
1995 FDA approves Oxycontin
Additional strengths were released to market in 1996
In 2000 a 160mg tablet was released(no longer on the market)
High dosage forms contributed to the abuse of the drug, making it easy to
crush, sniff, snort and inject for a euphoric long lasting high. Now considered
a gateway drug to heroin
6

Strategic Marketing Campaign led by Purdue Pharma
Lead by Arthur Slacker one of three owners of Purdue
Claim to fame was the Valium marketing campaign in which the drug hit $100 million in
revenue
Arthur launched a multifaceted marketing campaign of Oxycontin
From 1996-2001 Purdue Pharma held more than 40 national pain- management
conferences speaking to over 5K healthcare professionals
Creating sentiment "Forget fears about prescribing opioids to a more general pain
population. This isn’t heroin. This pill has a unique time release mechanism that means
it’s not very addictive at all.”
Collection of prescribing data for years
Purdue had collected data on physicians prescribing habits creating prescribing profiles
on individuals and physicians. Purdue used this data to target the higher prescribers .
7

Strategic Marketing Campaign led by Purdue Pharma Cont’d
Patient Starter Coupon program- gave patients free prescription for a 7-30 day
supply
A total of 34,000 coupons had been redeemed nationally according to the
Washington, DC: General Accounting Office.
Why was Oxycontin the narcotic of choice for physicians? Other Narcotics
on the market ( i.e. Percocet, Vicodin, Fentanyl)
The crux of the entire marketing campaign was the drug’s “ incredibly
low risk of addiction” as a result of the time-release formulation
Even the FDA bought into this logic, a Medical Officer from the agency
stated “Delayed absorption, as provided by OxyContin tablets is believed
to reduce the abuse liability of a drug.”
8

Examples of Purdue’s Advertisement Campaign
“Friend for life against the war on pain”
A campaign of deliberate deception?
9

Change in Physicians’ Prescribing habits Based on the intense marketing campaign which included over 20k
pain- management related workshops and lectures espousing better pain management strategies coupled with the “incredibly low risk of addiction” doctors started to write scripts for Oxycontin more regularly and more liberally
By 2001 General Account Office confirmed Oxycontin became the most frequently prescribed brand-name opioid in the United States for treating moderate to severe pain
New pattern of thinking- Get ahead of the pain instead of behind the pain
Sentiment people want physicians to treat their pain adequately using opioids. Payment for doctors being based on patient surveys motivates physicians to write for opioids
“ We have created a culture where pain medication is not expected it is demanded by the patients” – Kevin Pho, M.D.
10

The Power of the Oxy Addiction The euphoric affects of Oxycontin contribute to addictive properties creating a physical
dependence that is very often unavoidable when a person is exposed to high doses of the drug for an extended period of time
The body adapts and develops a tolerance for Oxycontin making it almost impossible to stop taking them without some form of Oxycodone recovery treatment
“ He’d {the doctor} spent less than ten minutes with me. It had almost seemed too easy. I looked at the prescription, and
I noticed that my heart began to beat faster and I started to sweat. Just the mere sight of the prescription was enough to wake up the demon. I filled it on the way home. As I took the bottle out of the sack, I thought to myself “Welcome back, my friends. I’ve missed you.” It was the very beginning of the prescription so the bottle was full. I was confident that if I took two pills, I’d be able to make it up during the month. Just this once, I told myself. Then it’s back to the right dose. Yeah, sure. I spent the next couple of weeks trying desperately to keep my consumption under control. I did better on some days than others, but I was still using more than prescribed.”- Recovered Oxycontin addict
“ I needed Oxycontin to function like I needed air to breath”
“ The addiction was so strong before I knew it I was up to 80mg , running out of pills before my script, pleading desperately with my doctor for another script and making up excuses to Pharmacists for additional pills. I then resorted to the streets to get the drug”
11

Consequences for the nation & Purdue Pharma
A nation addicted to oxycontin(opioids)- increased overdoses
People dependent on the drug lead to the destruction of communities
Now taking a reactionary stance to curb the epidemic
2003 FDA issued Warning Letter to Purdue Pharma for misleading advertising claims re:
addictive potential
2007 United States V. Purdue Pharma Largest Pharmaceutical settlement in US History
Lawsuit brought against Purdue Pharma, Inc and its top executives pled guilty that it
misrepresented and misbranded the risk of addiction
Purdue paid a fine of $634 million
Purdue’s estimated sales of Oxycontin were approx $35 billion as of Q32015
Investigations relating to the trial found that Purdue had encouraged doctors to over
prescribe Oxycontin for conditions that were not classified as severe pain and misbranded
the drug as low abuse potential
12

Consequences for the nation & Purdue Pharma
13

FDA & State Governments Involvement in curbing the epidemic
Black Box Warning on Extended Release Formulation in 2002 for abuse potential
2010 Purdue released a new formulation of Oxycontin designed to be abuse deterrent
Excipients were used to give it a thicker and gooey consistency
The original formulation stopped being shipped the same year
23Mar2016 FDA now requiring all Immediate Release Opioids to carry a black box warning
“The development of abuse-deterrent opioid analgesics is a public health priority for the FDA,” said Douglas
Throckmorton, M.D.
Directed to Wholesalers practices-DEA instituted Order Monitoring Plan (OMP) for wholesalers designed to monitor
wholesalers distribution of opioids. Focus on the choke point. Easier to monitor a handful of wholesalers as oppose to
thousands of pharmacies.
Directed towards Pharmacists practices-State level-Prescription Monitoring programs (PMPs) have been implemented
& state governors looking towards strengthening prescribing laws.
PMP requires pharmacist to check database to ensure script was not filled by another physician and at any
pharmacy recently. Pharmacists due diligence before filling opioid script
States are attempting to set forth general guidelines address best practices for prescribing painkillers
14

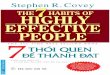
New(OP) vs. Old Oxycontin(OC) formulation- Abuse deterrent technologies added
15
Abuse deterrent polymers were used in the new formulation of Oxycontin (OP). Row #1-OP is thicker than the original (OC) formulation Row #2- Cannot be ground into a fine dust anymore Row #3- Sludgy substance not easy to inject

FDA & State Governments Involvement in curbing the epidemic
Directed towards Physicians: 16Mar2016 Center for Disease Control and Prevention released
revised guidelines for physicians(these are not binding)
"For the first time, the federal government is communicating clearly that the widespread
practice of treating common pain conditions with long-term opioids is inappropriate,"
Kolodny said. "The CDC is making it perfectly clear that medical practice needs to
change because we’re harming pain patients and fueling a public health crisis.“
New guidelines recommend physicians should prescribe for cancer-patients and or end
of life care – reverting back to original prescribing trends
Only when necessary outside of cancer patients and or end of life treatment
Give lowest amount for shortest amount of time
Do the benefits of opioids outweigh the risk for the patient ?
16

17
FDA & State Governments Involvement in curbing the epidemic Cont’d
Directed to Sponsors: Agency has held several forums to better understand the extent of the opioid abuse and public health concerns
2015 FDA Guidance Document published to develop abuse- deterrent technologies
Science of abuse deterrent technologies is relatively new, FDA maintain “flexible , adaptive approach in evaluating abuse deterrent technologies”
Guidance outlines FDA’s recommendation on including abuse-deterrent technologies are part of opioid drug formulation –helpful for opioid innovators
Examining the drugs abuse potential in in vitro studies, understanding the drugs potential to be manipulated and abused. These results will impact what other preclinical and clinical testing is required
In Vivo- Examine the PK and PD profiles if the drug is taken in true form vs. manipulated form
Clinical Abuse Deterrent study- How attractive is the formulation for abuses and how will it be abused?
PostMarket studies- Evaluate how effective are drugs with abuse- deterrent technologies in reducing abuse
Examples of Opioids Deterrent formulations
Use of chemical barriers- making the pill hard to crush, chewing or grinding, change properties of the drug if abuse is attempted ie product turns into a paste
Antagonistic combinations- If the drug is not taken as directed ( crushed, chewed, injected) antagonistic affects will be come active reducing the euphoric feeling
Aversion – Substances can be combined to produce an unpleasant effect if the dosage form is manipulated prior to ingestion or a higher dosage than directed is used

FDA Opioid Action Plan – February 2016
18
1. Expand use of advisory committees-Expert advisory committee will be required to meet anytime a
opioid with non- abuse deterrent technologies is up for approval
2 . Develop warnings and safety information for immediate-release (IR) opioid labeling-
Additional warnings to be added to the label, provide more info so doctors can prescribe
appropriately
3. Strengthen postmarket requirements- Better understanding of the long-term impact of opioid use
and insight into misuses
4. Update Risk Evaluation and Mitigation Strategy (REMS) Program-Increase training for prescribes
on pain management
5. Expand access to abuse-deterrent formulations (ADFs) to discourage abuse- Further explore
abuse –deterrent formulations
6. Support better treatment- More access to overdose treatment medications i.e. Naxolone OTC
7. Reassess the risk-benefit approval framework for opioid use-Upcoming Adcom to discuss opioid
impact on public health

FDA & State Governments Involvement in curbing the epidemic
19

Additional Affects from Opioid Epidemic
The opioid epidemic has spawned the development of new categories of drugs to treat the addiction and side effects of the opioid narcotics:
Suboxone (buprenorphine/naloxone) an opioid drug that has a "ceiling effect" that binds to opiate receptors in a way that mitigates withdrawal symptoms without producing the high risk of overdose has become a mainstay in treating opiate addiction
Evivo (naloxone) injections are now being used to treat and reverse acute overdose symptoms. In many cases they are prescribed for patients taking high doses of opiates just to have available for a caretaker to administer in the event of an inadvertent overdose
Movantik(naloxegol) has been developed to combat a common side effect with opiates referred to as opioid induced constipation or OIC
20

Moral Dilemma Measuring a subjective symptom- Pain is not a vital sign or a
diagnosed diseased
Prescribing for people truly in pain without supporting addiction – Regulate abuse without while assessing legitimate uses
Look to other solutions to manage the pain, i.e. physical therapy
Managing Physicians’ autonomy to prescribe- New York Time’s article “The American Medical Association says the decision to prescribe drugs should “stay in the hands of physicians. Of course, doctors should have discretion to make medical decisions, including what drugs to use, but state governments also have a duty to protect people by placing sensible limits on the use of risky substances.”
21

References Prescription Drugs: OxyContin Abuse and Diversion and Efforts to Address the
Problem. Washington, DC: General Accounting Office; December 2003. Publication GAO-04-110
The Promotion and Marketing of OxyContin: Commercial Triumph, Public Health Tragedy
Centers for Disease Control and Prevention. (2014). Opioid Painkiller Prescribing, Where You Live Makes a Difference. Atlanta, GA: Centers for Disease Control and Prevention.
National Institute on Drug Abuse. (2015). Drugs of Abuse: Opioids. Bethesda, MD: National Institute on Drug Abuse
How the American opiate epidemic was started by one pharmaceutical company Author Mike Mariani
Who Is Responsible for the Pain-Pill Epidemic? Author Celine Gounder
MedicneNet
American Society of Addiction Medicine- Opioid Addiction 2016 Facts & Figures
FDA Guidance Document- Abuse-Deterrent Opioids Evaluation and Labeling
Governors Unite in the War Against Opioids- New York Times Author Editorial Board
USA Today- Doctors Told to stop prescribing opiates for chronic pain 22

Questions?
23