Embed Size (px)
Citation preview
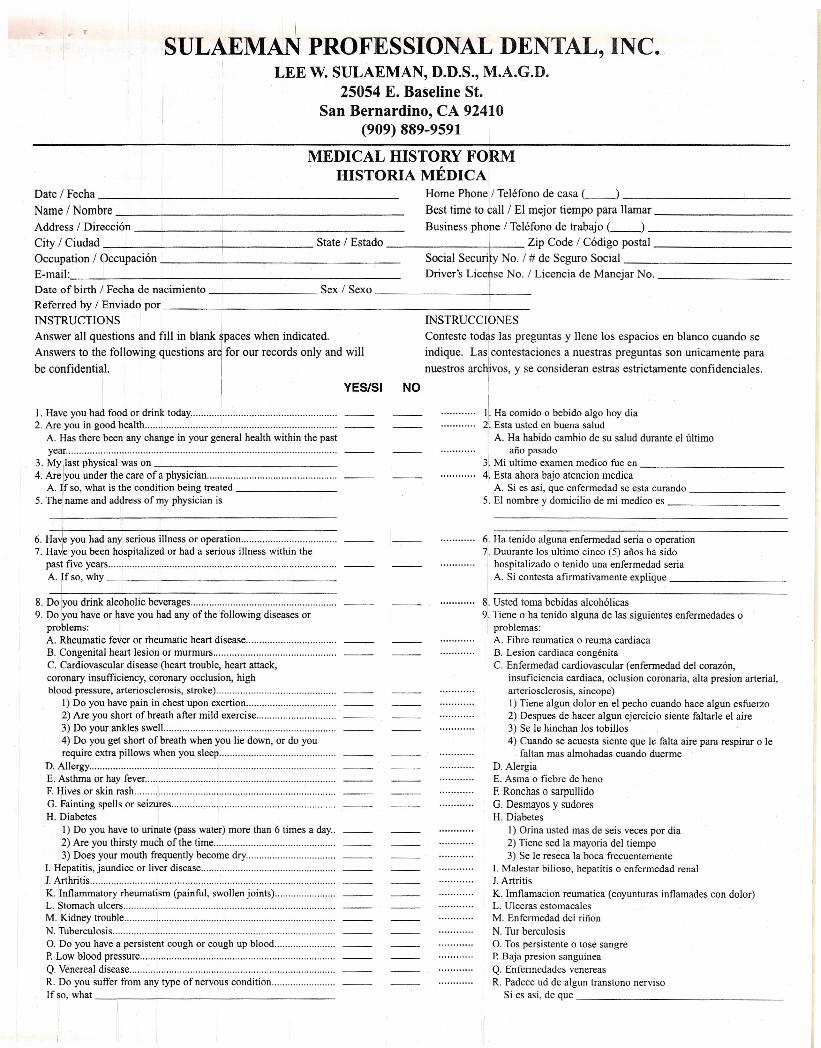
ISULAEMAN PROFESSIONAL DENTAL, INC.
I LEE W. SULAEMAN, D.D.S., M.A.G.D.25054 E. Baseline St.
Sari Bernardino, CA 92410(909) 889-9591
Date/Fecha _
Name/Nombre _
MEDICAL HISTORY FORMHISTORIA MEDICA
Home Phone / Telefono de cas a C--) _Best time to call / El mejor tiempo para llamar _
Address / Direcci6n Business phone / Telefono de trabajo C-_) _City / Ciudad I State / Estado I Zip Code / Codigo postal _
Occupation / Occupacion I Social seCUri~ No. / # de Seguro Social _
E-mail: Driver's LicenseNo./Licencia de Manejar No.
Date of birth / Fecha de nacimiento Sex / Sexo 1 _
Referred by / Enviado por IINSTRUCTIONS INSTRUCClbNES
Answer all questions and fill in blank paces when indicated. Con teste todas las preguntas y Ilene los espacios en blanco cuando se
Answers to the following questions are, for our records only and will indique. La;rcontestaciones a nuestras preguntas son unicamente para
be confidential. nuestros arch1ivos, y se consideran estras estrictamente confidenciales.
YES/SI NO I
I. Have you had food or drink today .2. Are you in good health .
A. Has there been any change in your general health within the pastyear .
3. My last physical was on _4. Are Iyou under the care of a physician .
A. ~f so, what is the condition being treated _5. The name and address of my physician is
II. Ha comido 0 bebido algo hoy dia'. Esta usted en buena salud
A. Ha habido cambio de su salud durante el ultimoafio pasado
3. Mi ultimo exam en medico fue en _4. Esta ahora bajo atencion medica
A. Si es asi, que enfermedad se esta curando _5. EI nombre y domicilio de mi medico es _
...1
6. Ha~e you had any serious illness or operation .
7. ::srlv~u y~:~: .~~s:.~.ta.l.iz.~~.~~.~a.d..~..~~~~.~.~.s.ill.~.~~~.~i.t~i~.~~~ .A. If so, why _
6[.Ha tenido alguna enfermedad seria 0 operation7. Duurante los ultimo cinco (5) afios ha sido
hospitalizado 0 tenido una enfermedad seriaA. Si contesta afirmativamente explique _
~:g~j~~~~~:eko~:~~I~~~e::~a;n~·~f~h~·i~·ii~~·i·~~·di~~~~~~·~~······· ...
problems:A. Rheumatic fever or rheumatic heart disease , .B. Congenital heart lesion or murmurs .C. Cardiovascular disease (heart trouble, heart attack,coronary insufficiency, coronary occlusion, highblood pressure, arteriosclerosis, stroke) .
I) Do you have pain in chest upon exertion .2) Are you short of breath after mild exercise .3) Do your ankles swell .4) Do you get short of breath when you lie down, or do yourequire extra pillows when you sleep .
D. Allergy .E. Asthma or hay fever .F. Hives or skin rash .G. Fainting spells or seizures .H. Diabetes
I) Do you have to urinate (pass water) more than 6 times a day..2) Are you thirsty much of the time .3) Does your mouth frequently become dry .
I. Hepatitis, jaundice or liver disease .1. Arthritis .K. Inflammatory rheumatism (painful, swollen joints) .L. Stomach ulcers , ' .M. Kidney trouble .N. Tuberculosis .O. Do you have a persistent cough or cough up blood , .P. Low blood pressure .Q. Venereal disease .R. Do you suffer from any type of nervous condition .Ifso,what _
8. Usted toma bebidas alcoholicas9. Tiene 0 ha tenido alguna de las siguientes enfermedades 0
I problemas:A. Fibre reumatica 0 reuma cardiacaB. Lesion cardiaca congenitaC. Enfermedad cardiovascular (enfermedad del corazon,
insuficiencia cardiaca, oclusion coronaria, alta presion arterial,arteriosclerosis, sincope)I) Tiene algun dolor en el pecho cuando hace algun esfuerzo2) Despues de hacer algun ejercicio siente faltarle el aire3) Se Ie hinchan los tobillos4) Cuando se acuesta siente que Ie falta aire para respirar 0 Ie
faltan mas almohadas cuando duermeD. AlergiaE. Asma 0 fiebre de henoF. Ronchas 0 sarpullidoG. Desmayos y sudoresH. Diabetes
I) Orina usted mas de seis veces por dia2) Tiene sed la mayoria del tiempo3) Se Ie reseca la boca frecuentemente
I. Malestar bilioso, hepatitis 0 enfennedad renalJ. ArtritisK. Imflamacionreumatica (coyunturas inflamades con dolor)L. Ulceras estomacalesM. Enfennedad del riftonN. Tur berculosisO. Tos persistente 0 tose sangreP. Baja presion sanguineaQ. Enfermedades venereasR. Padece ud de algun transtono nervi so
Si es asi, de que _
I
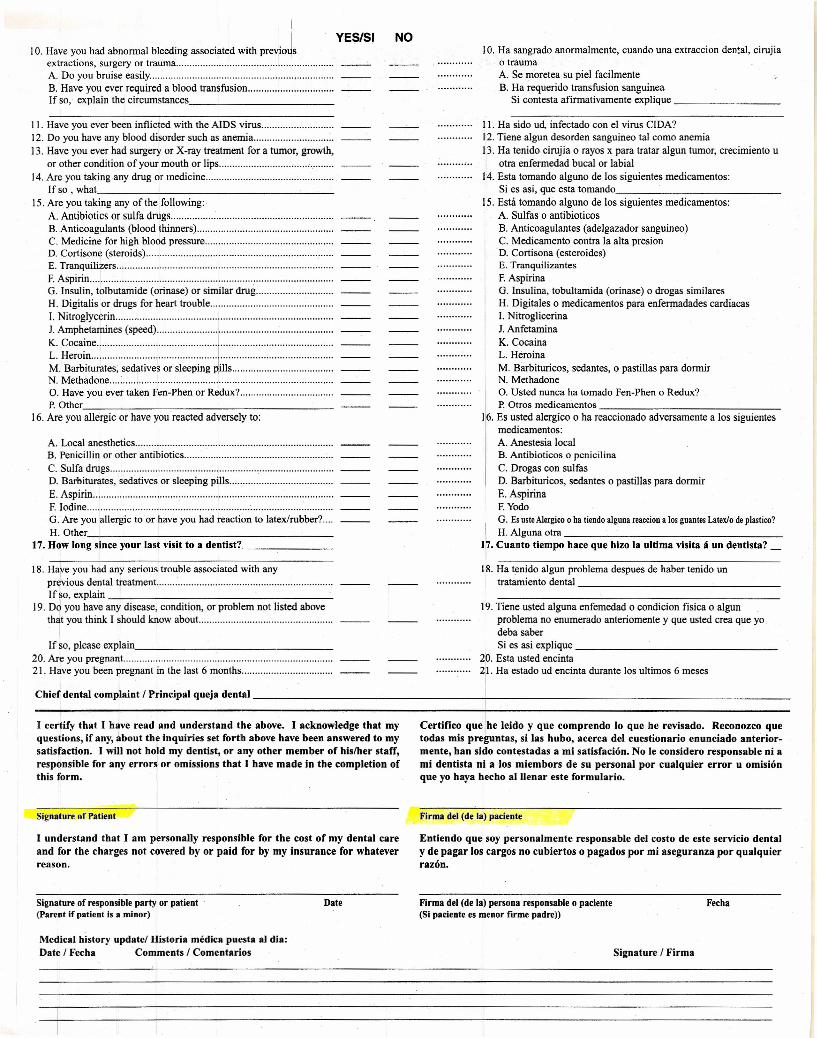
10. Have you had abnormal bleeding associated with previoJsextractions, surgery or trauma .A. Do you bruise easily .B. Have you ever required a blood transfusion .If so, explain the circumstances, _
YES/51 NO10. Ha sangrado anormalmente, cuando una extraccion dental, cirujia
o traumaA. Se moretea su piel facilmenteB. Ha requerido transfusion sanguinea
Si contesta afirmativamente explique ~ __
A. Local anesthetics .B. Penicillin or other antibiotics .C. Sulfa drugs , .D. Barbiturates, sedatives or sleeping pills .E. Aspirin .F. Iodine .G. Are you allergic to or have you had reaction to latex/rubber? .H.Other _
17. How long since your last visit to a dentist? _
II. Ha sido ud, infectado con el virus CIDA?12. Tiene algun desorden sanguineo tal como anemia13. Ha tenido cirujia 0 rayos x para tratar algun tumor, crecimiento u
otra enfermedad bucal or labial14. Esta tomando alguno de los siguientes medicamentos:
Si es asi, que esta tomando _15. Esta tomando alguno de los siguientes medicamentos:
A. Sulfas 0 antibioticosB. Anticoagulantes (adelgazador sanguineo)C. Medicamento contra la alta presionD. Cortisona (esteroides)E. TranquilizantesF. AspirinaG. Insulina, tobultamida (orinase) 0 drogas similaresH. Digitales 0 medicamentos para enfermadades cardiacasl. NitrogticerinaJ. AnfetaminaK. CocainaL. HeroinaM. Barbituricos, sedantes, 0 pastillas para dormirN. MethadoneO. Usted nunca ha tornado Fen-Phen 0 Redux?p. Otros medicamentos _
116. Es usted alergico 0 ha reaccionado adversamente a los siguientesmedicamentos:A. Anestesia localB. Antibioticos 0 penicilinaC. Drogas con sulfasD. Barbituricos, sedantes 0 pastillas para dormirE. AspirinaF. YodoG. EsusteA1ergico0 ha tiendoalguna reacciona losguantesLatexlodeplastico?I H.AIgunaotra~ _
17. Cuanto tiempo hace que hlzo la ultima vislta Ii un dentista? __
I I. Have you ever been inflicted with the AIDS virus .12. Do you have any blood disorder such as anemia .13. Have you ever had surgery or X-ray treatment for a tumor, growth,
or other condition of your mouth or lips ,.,' .14. Are you taking any drug or medicine .
Ifso,what. ~~_
15. Are you taking any of the following:A. Antibiotics or sulfa drugs .B. Anticoagulants (blood thinners) .C. Medicine for high blood pressure .D. Cortisone (steroids) .E. Tranquilizers .F. Aspirin .G. Insulin, tolbutamide (orinase) or similar drug .H. Digitalis or drugs for heart trouble .I. Nitroglycerin .
~.~~~:~~~~~.(S~.~~~~ : : !.. : :..:..::::::::::::::::::::::::::~.~:~~~~;~~;··~~d~~i·~~~·~~·~i~~~i·~·~·Jii~·.·.·.·.·.·.:::..:::::::::::::::::::::::::N. Methadone : ~f .O. Have you ever taken Fen-Phen or Redux? .p. Other _
16. Are you allergic or have you reacted adversely to:
18. Hare you had any serious trouble associated with anypr~vious dental treatment... .Ifso, explain _
19. oJ you have any disease, condition, or problem not listed aboveth~t you think I should know about... .
18. Ha tenido algun problema despues de haber tenido untratamiento dental _
If so, please explain -.,. _20. Are you pregnant.. .21. Have you been pregnant in the last 6 months .
19. Tiene usted alguna enfemedad 0 condicion fisica 0 algunproblema no enumerado anteriomente y que usted crea que yodeba saberSi es asi explique _
20. Esta usted encinta21. Ha estado ud encinta durante los ultimos 6 meses
Chief dental complaint! Principal queja dental +- _
I certify that I have read and understand the above. I acknowledge that myquestions, if any, about the inquiries set forth above have been answered to mysatisfaction. I will not hold my dentist, or any other member of hislher staff,responsible for any errors or omissions that I have made in the completion ofthis form.
Certifico que Ihe leido y que comprendo 10 que herevisado. Reconozco quetodas mis preguntas, si las hubo, acerca del cuestionario enunciado anterior-mente, han sido contestadas a mi satisfacien, No Ie considero responsable ni ami dentista ni a los miembors de su personal por cualquier error u omlsienque yo haya hecho allJenar este formulario.
Signature of Patient Firma del (de la) paciente
I understand that I am personally responsible for the cost of my dental careand for the charges not covered by or paid for by my insurance for whateverreason.
Entiendo que soy personal mente responsable del costo de este servicio dentaly de pagar los cargos no cubiertos 0 pagados por mi aseguranza por qualquierrazen,
Signature of responsible party or patient(Parent if patient is a minor)
Date Firma del (de la) persona responsable 0 paciente(Si paciente es menor firme padre»
Fecha
Medical history update! Historia medica puesta al dia:Date! Fecha Comments! Comentarios Signature! Firma





























