Embed Size (px)
Citation preview

Supplementazione
nutrizionale nel
paziente con BPCO
grave: nuove
prospettive
Fernando De Benedetto – Chieti
Alberobello 29.10.2016


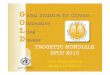
BPCO
Ipercapnia Dispnea Capacità ossidativa Ipossia Consumo O2 Infiammazione
muscolare
Fumo
Catecolamine Farmaci OCB Effetto termogenico Leptina
dell’attività
TNF
Spesa energetica Apporto energetico/consumo
DEPLEZIONE NUTRIZIONALE
European Respiratory Monograph , vol 8 Monografia 24, March 2003; pag. 11-22
Fisiopatologia della Deplezione nutrizionale

Meccanismi di alterazioni muscolari nella BPCO
AMERICAN THORACIC SOCIETYDOCUMENTS
An Official American Thoracic Society/European Respiratory Society
Statement: Update on Limb Muscle Dysfunction in Chronic Obstructive
Pulmonary Disease
François Maltais, Marc Decramer, Richard Casaburi, Esther Barreiro, Yan Burelle, Richard Debigare,
P. N. Richard Dekhuijzen, Frits Franssen, Ghislaine Gayan-Ramirez, Joaquim Gea, Harry R. Gosker, Rik Gosselink,
Maurice Hayot, Sabah N. A. Hussain, Wim Janssens, Micheal I. Polkey, Josep Roca, Didier Saey, Annemie
M. W. J. Schols, Martijn A. Spruit, Michael Steiner, Tanja Taivassalo, Thierry Troosters, Ioannis Vogiatzis, and
Peter D. Wagner; on behalf of the ATS/ERS Ad Hoc Committee on Limb Muscle Dysfunction in COPD
THIS OFFICIAL STATEMENT OF THE AMERICAN THORACIC SOCIETY (ATS) AND THE EUROPEAN RESPIRATORY SOCIETY (ERS) WAS APPROVED BY THE ATS BOARD OF
DIRECTORS, NOVEMBER 2013, AND BY THE ERS EXECUTIVE COMMITTEE, SEPTEMBER 2013
Background: Limb muscledysfunction isprevalent in chronicobstructivepulmonary disease(COPD) and it hasimportant clinicalimplications, such asreduced exercise tolerance, quality of life,and even survival. Sincetheprevious American Thoracic Society/European Respiratory Society (ATS/ERS) statement on limbmuscledysfunction, important progress hasbeen madeon thecharacterization of thisproblem and on our understanding of itspathophysiology and clinical implications.
Purpose: Thepurposeof thisdocument is to update the1999ATS/ERSstatement on limb muscledysfunction in COPD.
Methods: An interdisciplinary committeeof expertsfrom theATSand ERSPulmonary Rehabilitation and Clinical Problemsassembliesdetermined that thescopeof thisdocument should belimited tolimb muscles. Committeemembersconducted focused reviewsof theliteratureonseveral topics.A librarianalsoperformedaliteraturesearch.An ATSmethodologist provided adviceto thecommittee, ensuringthatthemethodological approach wasconsistent with ATSstandards.
Results: Weidentified important advances in our understandingof theextent and natureof thestructural alterations in limb musclesin patientswith COPD. Sincethelast update, landmark studieswerepublished on themechanismsof development of limb muscledysfunction in COPD and on thetreatment of thiscondition. Wenow haveabetter understanding of theclinical implications of limbmuscledysfunction. Although exercise training is themost potentintervention to address thiscondition, other therapies, such asneuromuscular electrical stimulation, areemerging. Assessment oflimb muscle function can identify patientswho areat increased riskof poor clinical outcomes,such asexerciseintoleranceandprematuremortality.
Conclusions: Limb muscledysfunction isakey systemicconsequenceof COPD.However, therearestill important gapsin ourknowledgeabout themechanisms of development of thisproblem.Strategies for early detection and specific treatments for thiscondition arealso needed.
Overview
Limb muscle dysfunction is an importantsystemic consequence of chronic obstructivepulmonary disease (COPD) because of itsimpact on physical activity, exercisetolerance, quality of life, and even survival inthis disease. Although some mechanismsunderlying the development of limb muscle
dysfunction have been identified (e.g.,deconditioning), much needs to be learnedabout the impact of other potentialcontributors to this clinical manifestation inCOPD. Limb muscle dysfunction can beprevented and improved, in part, withexercise training, but it is clear that noveltherapies are needed to better address thisproblem.
Thepurposeof thisdocument isto updatethe1999 American Thoracic Society/EuropeanRespiratory Society (ATS/ERS) statementon limb muscle dysfunction. We intend toprovide researchers and clinicians with therecent advances in this field, with emphasison the following areas: (1) structural andmetabolic alterations found in limb muscles,(2) consequences and clinical evaluation of
F.M. holds a CIHR/GSK Research Chair on COPD at Universite Laval. R.C. holds the Grancell/Burns Chair in the Rehabilitative Sciences. E.B.’s contribution to
this statement was supported by CIBERES, FIS 11/02029, 2009-SGR-393, SEPAR 2010, FUCAP 2011, FUCAP 2012, and Marato TV3 (MTV3-07-1010)(Spain) and by the ERS COPD Research Award 2008. M.I.P.’s contribution to this statement was supported by the NIHR Respiratory Disease Biomedical
Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London, who partially fund his salary.
Am J Respir Crit Care Med Vol 189, Iss 9, pp e15–e62, May 1, 2014
Copyright © 2014 by the American Thoracic Society
DOI: 10.1164/rccm.201402-0373ST
Internet address: www.atsjournals.org
American Thoracic Society Documents e15

Skeletal muscle disfunction in COPD
Alterazioni strutturali del muscolo
• Shift delle fibre muscolari da fibre di tipo I a fibre di tipo II;
• Atrofia non omogeneamente distribuita (maggiore nei quadricipiti) rispetto ai distretti superiori;
• Correlazione inversa fra fibre di tipo I e gravità di BPCO e diretta con BMI;
• Capillarizzazione: La densità di capillari nel muscolo (numero di capillari per mm2 ) sembra ridotta anche se il rapporto fra superfici sembra mantenuto (capacità di diffusione conservata)

Bioenergetica e funzione mitocondriale
• Alterata funzione mitocondriale (alterazione o disuso?) con riduzione della funzione ossidativa muscolare;
• Evidenza di ridotta densità, ridotta funzione e ridotta tendenza genetica alla biogenesi mitocondriale nella BPCO;
• Ridotta capacità aerobica (bassa concentrazione di ATP e creatinfosfato) e preservata attività glicolitica (alta concentrazione di prodotti intermedi della glicolisi);
• Possibile ruolo dell’epigenetica (l’ipossia cellulare facilitata dalla sedentarietà determinerebbe una ridotta funzione muscolare);
• Bassa efficienza meccanica (fibre alterate) e elevata spesa energetica (catecolamine, farmaci, OCB).
Danno Ossidativo
• Dimostrato aumento dello stress ossidativo (ROS, RNS) nei pazienti con BPCO - proporzionale alla gravità del danno funzionale e al fumo- correlato al danno muscolare in termini di ridotta funzionedel muscolo e di endurance (Correlazione con aumentata proteolisi?
Correlazione con infiammazione sistemica?)

Eziologia della disfunzione muscolare

Eziologia del danno muscolare: disusoMeccanismo discusso:
• PRO: evidenze cellulari tipiche, il riallenamento all’esercizio permette una reversibilità delle alterazioni anche se non completa (verosimilmente tempi di riallenamento troppo brevi o carico non raggiungibile per limite ventilatorio);
• CONTRO: evidenza di miopatia non correlata con il grado di riduzione di attività, nel confronto con pazienti senza BPCO con riduzione di attività simile le alterazioni strutturali e funzionali muscolari sono significativamente differenti, dopo riallenamento le alterazioni strutturali rimangono nei BPCO (Shift fibre muscolari), la debolezza muscolare viene evidenziata in tutte le classi di gravità

Alterazioni funzionali: cause (1)
• Infiammazione: citochine stimolanti la via UbP attraverso l’attività transcrizionale di NfKb e FOXO, apoptosi e autofagia (solo durante riacutizzazione?);
• Stress ossidativo: aumento della proteolisi e attivazione della via UbP (NfKb e FOXO);
• Ipossia: ridotta proliferazione e differenziazione cellulare, ridotta attivita delle Kinasi di mTOR che ha un ruolo nella proteinosintesi, alterato trasporto e utilizzo di O2 aumentano lo stress ossidativo, compromissione della capacità ossidativa e della capillarizzazione;
• Ipercapnia: acidosi tessutale altera la sintesi e la degradazione delle proteine contrattili

Alterazioni funzionali: cause (2)• Ridotti livelli ormonali: ridotti livelli ematici di testosterone e
elevati di miostatina (attività inibente la proliferazione dei mioblasti)
• Sbilancio Energetico: elevato consumo energetico/ridotto apporto proteico (ridotta FM e FFM), normale consumo energetico/ridotto apporto proteico (normale FM e ridotto FFM);
• Terapia steroidea: riduce la produzione di proteine contrattili, alterazione delle fibre muscolari (trofismo per fibre II), aumenta la miostatina;
• Deficit vit D: atrofia fibre muscolari II, influenza sul trasporto di calcio,
• Sistema renina angiotensina: angiotensina II inibisce IGF1 e stimola NFKb e miostatina,
• Fumo: aumenta lo stress ossidativo e riduce fibre muscolari I
Suscettibilità muscolare alla fatica
• Afferenze nervose e drive neurologico: aumento del feedback dalle fibre muscolari durante l’esercizio;
• Flusso ematico , rilascio e estrazione di O2: aumentata richiesta e ridotta perfusione durante esercizio (fatica muscolare) spiegata solo per il 30-40% vista la scarsa risposta ad O2 terapia , ridotta capillarità;
• Funzione delle unità motorie: alterazione metabolica (aumento lattati, riduzione di fosfocreatina, alterato supporto energetico, alterazione delle proteine contrattili), ridotta capacità ossidativa, alterata produzione di energia (ridotto numero e funzione mitocondriale)
COPDSkeletal Muscle Impairment
“ a disabling systemic consequence of COPD”
- affects 20 % - 40% of patients with moderate to severe COPD
- is commonly described in locomotor muscles
- causes exercise intolerance, weakens, poor endurance and increased fatigability
- Fiber atrophy, a shift in fiber-type distribution from type I to type II/IIx
Mitochondrial abnormalities
- is strongly related to diminished quality of life and premature mortality

COPDRespiratory muscles
- the activity of the oxidative enzymes citratesynthase (CS), succinate dehydrogenase, and β-hydroxyacyl-CoA dehydrogenase is elevated in thediaphragm of patients with severe COPD in contrastwith the leg muscles
- the activity of the glycolytic enzymes hexokinaseand lactic dehydrogenase is decreased. Thisenzymatic profile is consistent with a predominanceof type I or IIa fibers reported in the diaphragms ofCOPD patients in contrast with leg muscles.
COPDRespiratory vs Skeletal muscles
The increasing in oxidative capacity andmitochondrial function in the diaphragm and inaccessory respiratory muscles are in the oppositedirection than in the quadriceps femoris and likelyreflect a “training effect” (due to the respiratoryworkload)

Energy Metabolism

Q10 (CoQ10) and Creatine
• coenzyme Q10 (CoQ10) and creatine have beenfound to affect both oxidative stress andmitochondrial function
• they may act in a synergistic manner when combined
Coenzyme Q10
its protective effects against oxidativestress and mitochondrial dysfunction have been
demonstrated inseveral in vitro and in vivo models

Coenzyme Q10
- is a component of the electron transport chain and is associated with innermitochondrial complex III protein and participates in aerobic cellular respiration
- is located in membranes in close proximity to the unsaturated lipid chains to actas a primary scavenger of free radicals
- may exert a protective effect against mitochondria mediated apoptosis and celldeath, by inhibiting the mitochondrial permeability transition pores (PTP) opening
- is a cofactor of mitochondrial uncoupling proteins and may also exert protectiveeffects by activation of these proteins, leading to a reduction in mitochondrial-freeradical generation

Coenzyme Q10
Its use in humans as a therapeutic agent was provedunsatisfactory, most likely because of its poor solubility inwater, its limited solubility in lipids, and its relatively highmolecular weight (863 g/mol), all result in poor oralbioavailability
Creatine
- has been shown to inhibit mitochondrial permeability transition and enhancemitochondrial function in stimulating mitochondrial energy production viacreatine-stimulated respiration and the adenine nucleotide translocase
- has been reported to act as an antioxidant against reactive species ions
- has been reported to enhance expression of myogenin and other myogenicregulatory factors that regulate myosin heavy chain expression
- has been found to be useful in buffering intracellular energy stores and reducingthe cellular energy deficit by improving mitochondrial function and to be effectivein attenuating the age-related decline in mitochondrial function
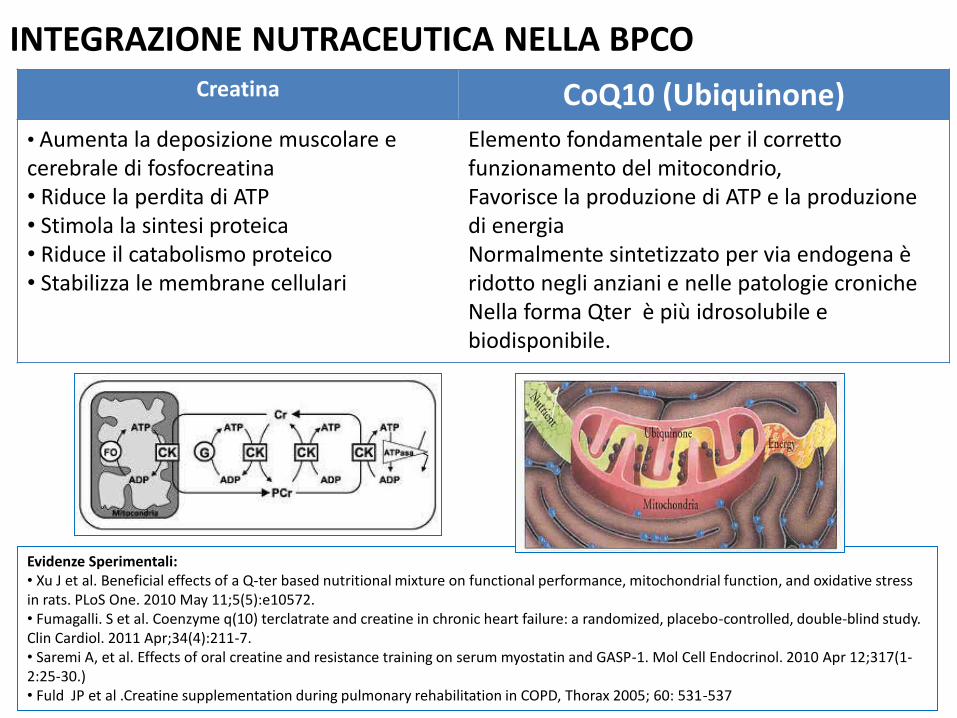
Creatina CoQ10 (Ubiquinone)
• Aumenta la deposizione muscolare e cerebrale di fosfocreatina• Riduce la perdita di ATP• Stimola la sintesi proteica• Riduce il catabolismo proteico• Stabilizza le membrane cellulari
Elemento fondamentale per il corretto funzionamento del mitocondrio, Favorisce la produzione di ATP e la produzione di energia Normalmente sintetizzato per via endogena è ridotto negli anziani e nelle patologie croniche Nella forma Qter è più idrosolubile e biodisponibile.
Evidenze Sperimentali:• Xu J et al. Beneficial effects of a Q-ter based nutritional mixture on functional performance, mitochondrial function, and oxidative stress in rats. PLoS One. 2010 May 11;5(5):e10572.• Fumagalli. S et al. Coenzyme q(10) terclatrate and creatine in chronic heart failure: a randomized, placebo-controlled, double-blind study. Clin Cardiol. 2011 Apr;34(4):211-7.• Saremi A, et al. Effects of oral creatine and resistance training on serum myostatin and GASP-1. Mol Cell Endocrinol. 2010 Apr 12;317(1-2:25-30.)• Fuld JP et al .Creatine supplementation during pulmonary rehabilitation in COPD, Thorax 2005; 60: 531-537
INTEGRAZIONE NUTRACEUTICA NELLA BPCO




To assess the physiological (exercise tolerance) and nutritional (lean mass and muscle efficiency)
effects determined by the association of Coenzyme Q10 (QTer®) and Creatine (Eufortyn® LiOs) in patients with chronic respiratory failure
due to COPD
Aim of the study

Study Design
Multicenter study, national (Italian), longitudinal, prospective, randomized, controlled, double-blind versus placebo, conducted on two parallel groups,
which expects 2 months of therapeutic treatment and 10 months of follow-up
Placebo sachets compared with Eufortyn® LiOs

Dosage
1) Active Treatment Group: 2 sachets/day containing Eufortyn® LiOs
2) Placebo Group: 2 sachets/day containing only excipients

Eufortyn LiOs
- The CoQ10 is rendered highly water soluble without chemicalmodification of the moiety by means of a mechano-physicalprocedure called terclatration.
- The resultant multicomposite, Q-ter, can be shown to be 3- to 5-fold more bioavailable in humans, as compared to native CoQ10
- Qter is a product covered by an international patent

Therapeutic scheme
- in addition to standard drug therapy
- maintaining the diet and the eventual rehabilitationprogram constant
- a single cycle of integrative supplementation lasting 8weeks, followed by an observational period (44 weeks) for atotal of 52 wks
Study objectives
To measure the effects of Eufortyn ® LiOs sachets (dietarysupplement with CoQ10 (QTer®) 160mg and creatine 170 mg) inCOPD patients, clinically stable, with O2 chronic insufficiency inhome therapy (O2TLT), by evaluation of:
- exercise tolerance (6MW test)- body composition (by bioelectrical impedance)- changes in quality of life
NB: Plasma concentrations of CoQ10 were analyzed before and aftertreatment with Eufortyn® LiOs in comparison with the placebo group
Primary efficacy endpoint
Improvement of exercise tolerance measured by 6MW test,performed at baseline (V1) and after the period ofintegrative supplementation (V2)

Secondary efficacy endpoints a)
1. Assessment of nutritional status after two months, versus placebo, measuredby bioelectrical impedance analysis (BIA) , performed at baseline (V1) and afterthe last observation (V2).
2. Measurements of spirometric data (FEV1, FVC, FEV1/FVC) and maximuminspiratory (MIP) and expiratory pressure (MEP) at V1 and V2.
3. Evaluation of the Wellness of Patient after 2 months of treatment (V2) bycomparison with Placebo of the value of the PGIC scale.
4. Evaluation of the components of dyspnea at rest and on exertion after 2months of treatment versus placebo, measured by scale MMRC, BDI, Borg andVAS, measured at baseline (V1) and after the last observation (V2).

Secondary efficacy endpoints b)
4. Evaluation of quality of life after 2 months of treatment, versusplacebo, measured by SGRQ index and ADL recorded at baseline(V1) and after the last observation (V2).
5. Evaluation of exacerbations and hospitalizations at the beginning(V1), after treatment (V2) and by telephone questionnaire duringfollow-up.
6. Determination, after treatment with EUFORTYN® LiOs, of baselineplasma concentrations of CoQ10 versus Placebo, measured by liquidchromatography

Tolerability end points
1. Side effects incidence
2. Overall tolerability (4 levels rating scale)
3. Exacerbation rate
4. Hospitalization rate
Centri partecipanti
• Acquaviva delle Fonti (BA) - P.Schino• Barletta (BAT) - E. Tupputi• Catania - A. Pennisi• Chieti - F. De Benedetto• Firenze - M. Pistolesi• Parma - E. Marangio• Roma - S. Valente• Sassari - P. Pirina• Scafati (SA) - M. Polverino
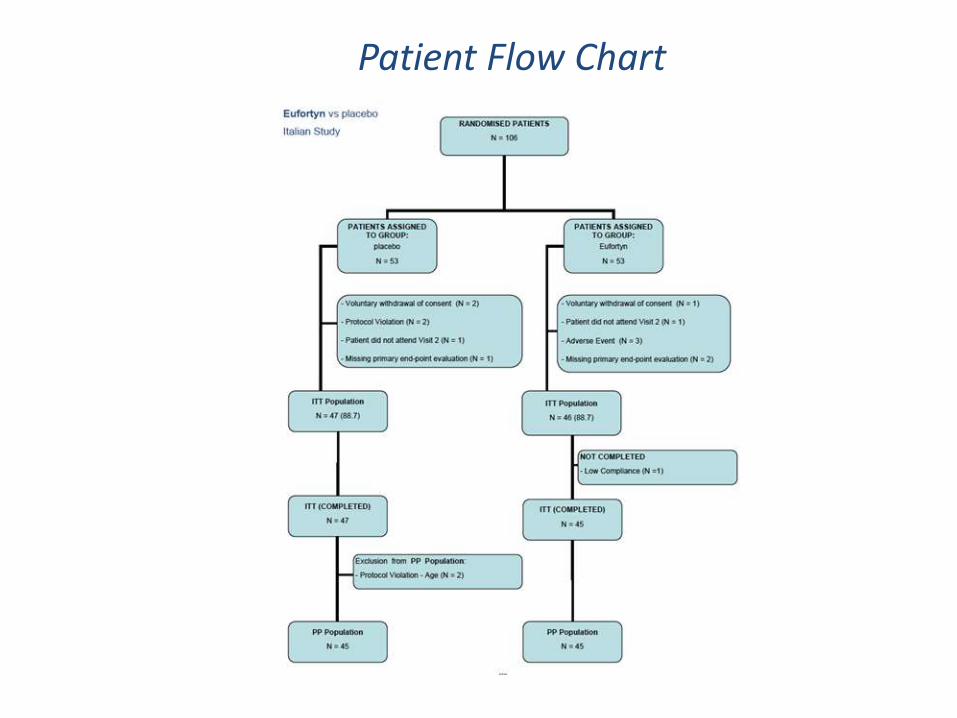
Patient Flow Chart

Patient Characteristics a)
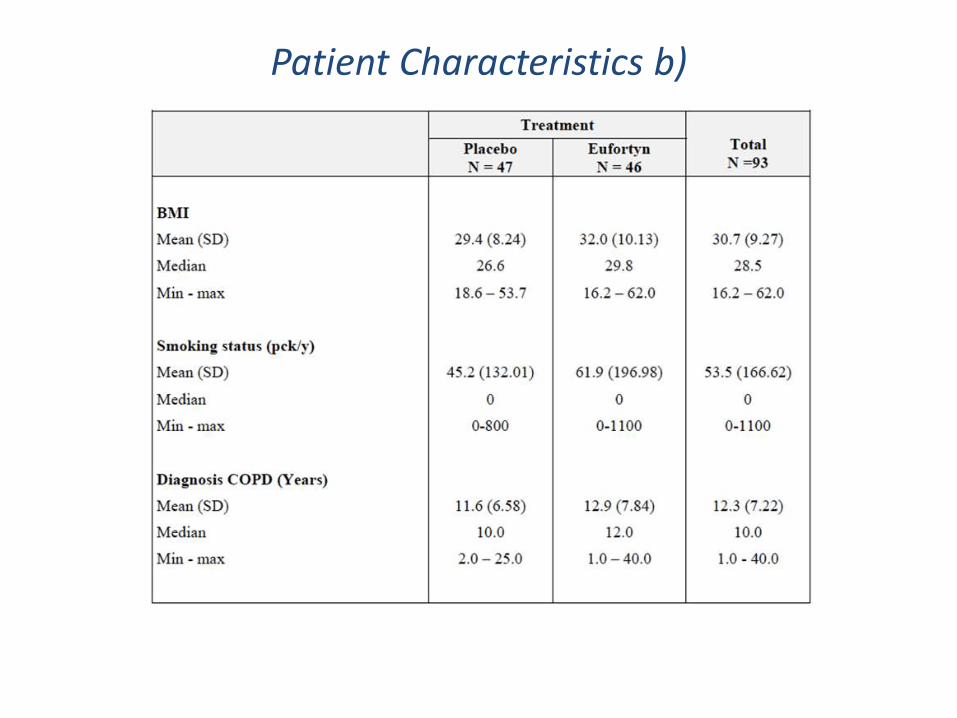
Patient Characteristics b)

History

Arterial Blood Gases
Results
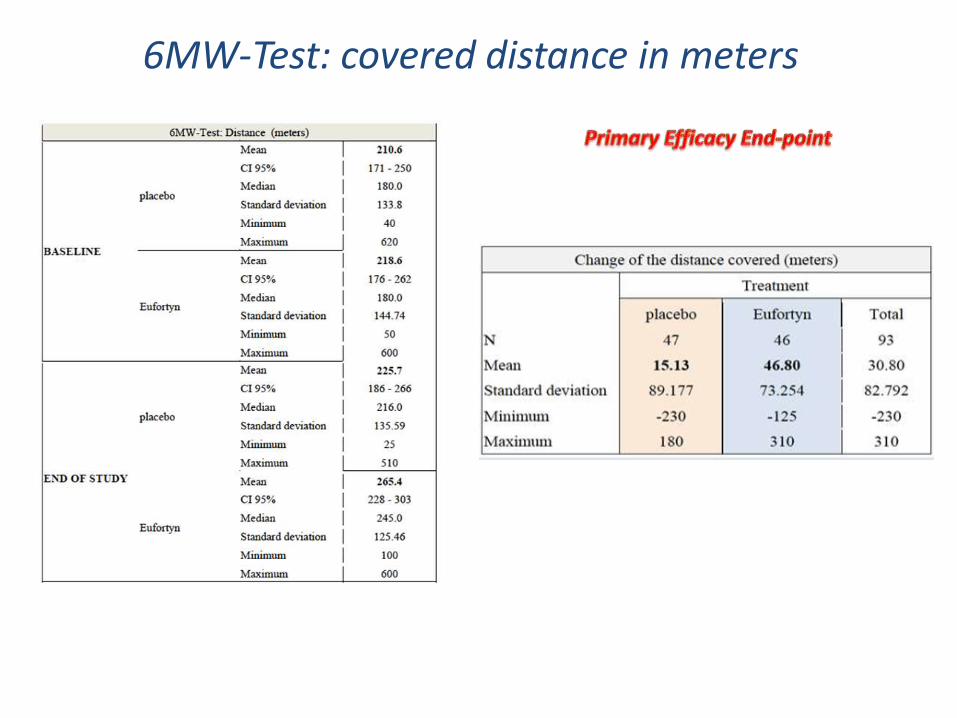
6MW-Test: covered distance in meters


6MW-Test (ANCOVA analysis)
Delta difference between treatments of the change of covered distance in meters (Estimated marginal means, 95% CI)
p = 0,035
Threshold for clinically important change in 6MWD?

l’American Thoracic Society ha emanato delle Linee Guida a tal proposito. La distanza considerata clinicamente significativa è 54 metri (17)Haggerty MC, Stockdale-Woolley R, ZuWallack R. Functional status in pulmonary rehabilitation participants. J Cardiopulm Rehabil 1999;19:35-42.
Minimal important difference for the 6MWD
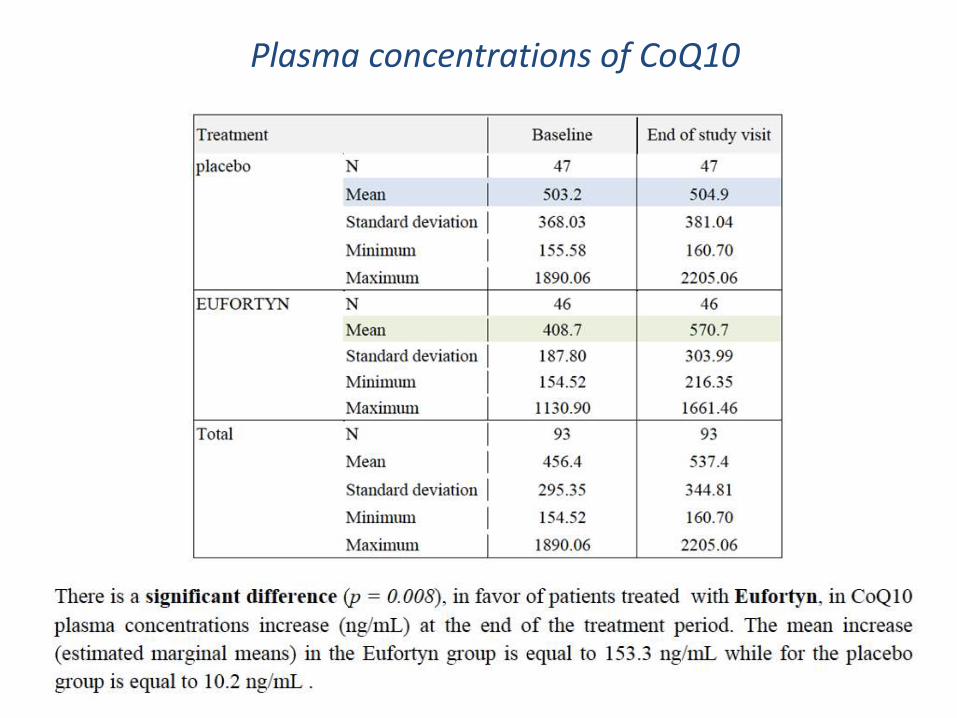
Plasma concentrations of CoQ10

Change of plasma concentration (ng/mL) of CoQ10 by treatment group, (ITT Population, N = 93)
p = 0.008
Conclusion
The supplementation with the association ofCoenzyme Q10(QTer®) and creatine (Eufortyn®
LiOs) significantly improved exercise tolerance insevere COPD patients with chronic hypoxemicrespiratory failure on long term oxygen therapy