Embed Size (px)
Citation preview
Mr Jason Smith - Consultant Surgeon
The Acute Abdomen
Jason Smith MD DMI FRCS(Gen.Surg) Consultant Surgeon
Mr Jason Smith - Consultant Surgeon
Acute Abdomen
General name for presence of signs, symptoms of inflamma4on of peritoneum
Mr Jason Smith - Consultant Surgeon
The problems of a surgeon If I operate and the problem is not surgical, pa4ent exposed to unnecessary risk, anesthe4c, etc. Risks greater with concomitant illness, older age
If I do not operate and problem is surgical, pa4ent at risk because of wrong therapy. Again the older pa4ent is under greater burden.
Risk-‐Predic4on Algorithms

Mr Jason Smith - Consultant Surgeon
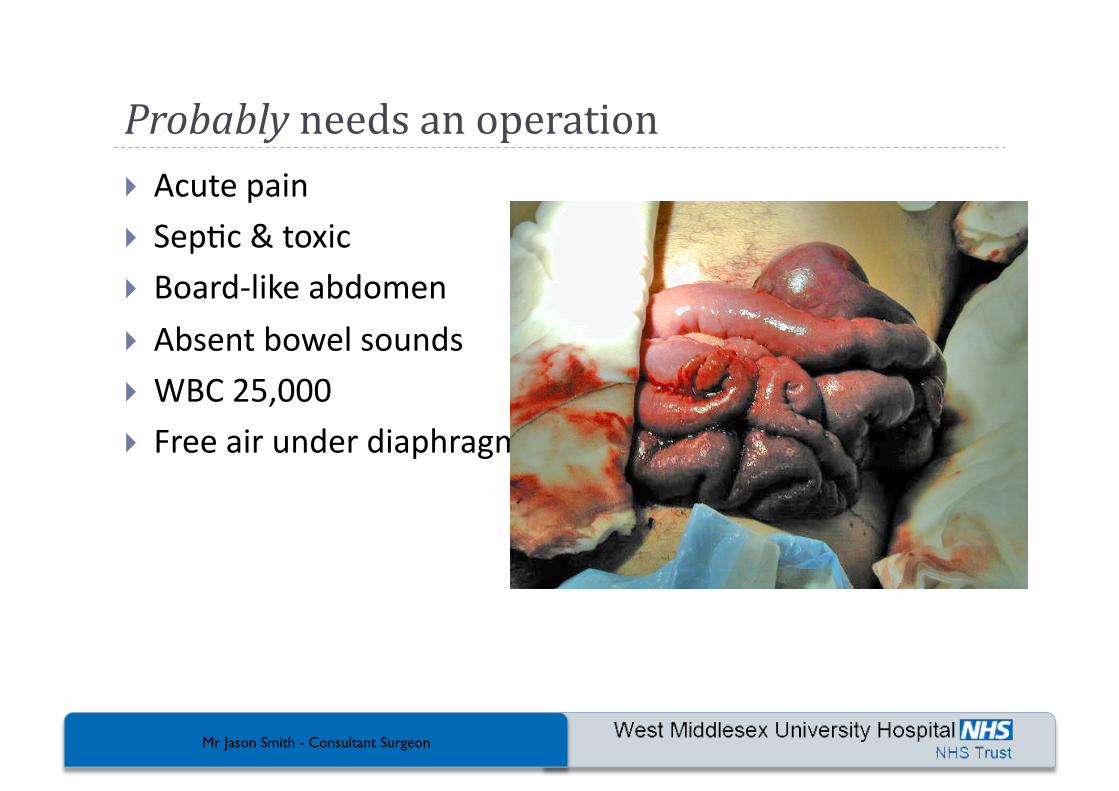
Probably needs an operation Acute pain Sep4c & toxic Board-‐like abdomen
Absent bowel sounds WBC 25,000 Free air under diaphragm
Mr Jason Smith - Consultant Surgeon
Probably doesn’t need an operation Trivial pain Robust appearance SoM abdomen with no guarding
Normal bowel sounds Normal WBC/CRP
Mr Jason Smith - Consultant Surgeon
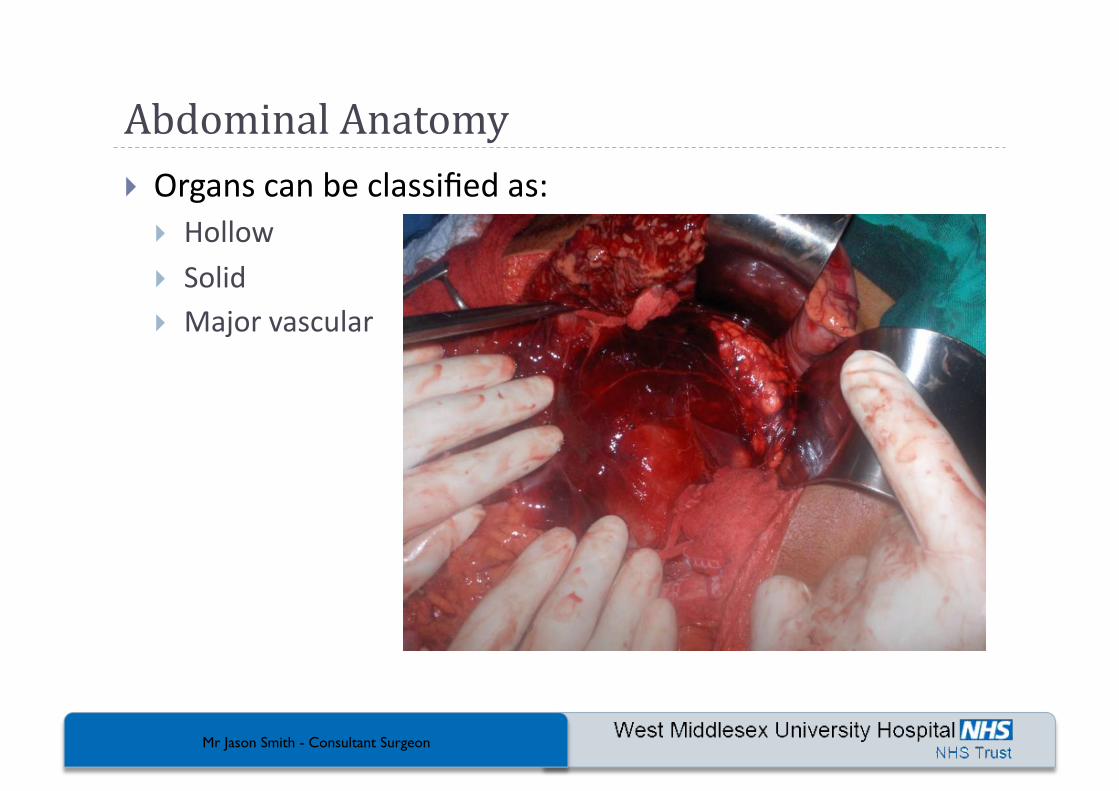
Abdominal Anatomy Organs can be classified as:
Hollow
Solid Major vascular
Mr Jason Smith - Consultant Surgeon
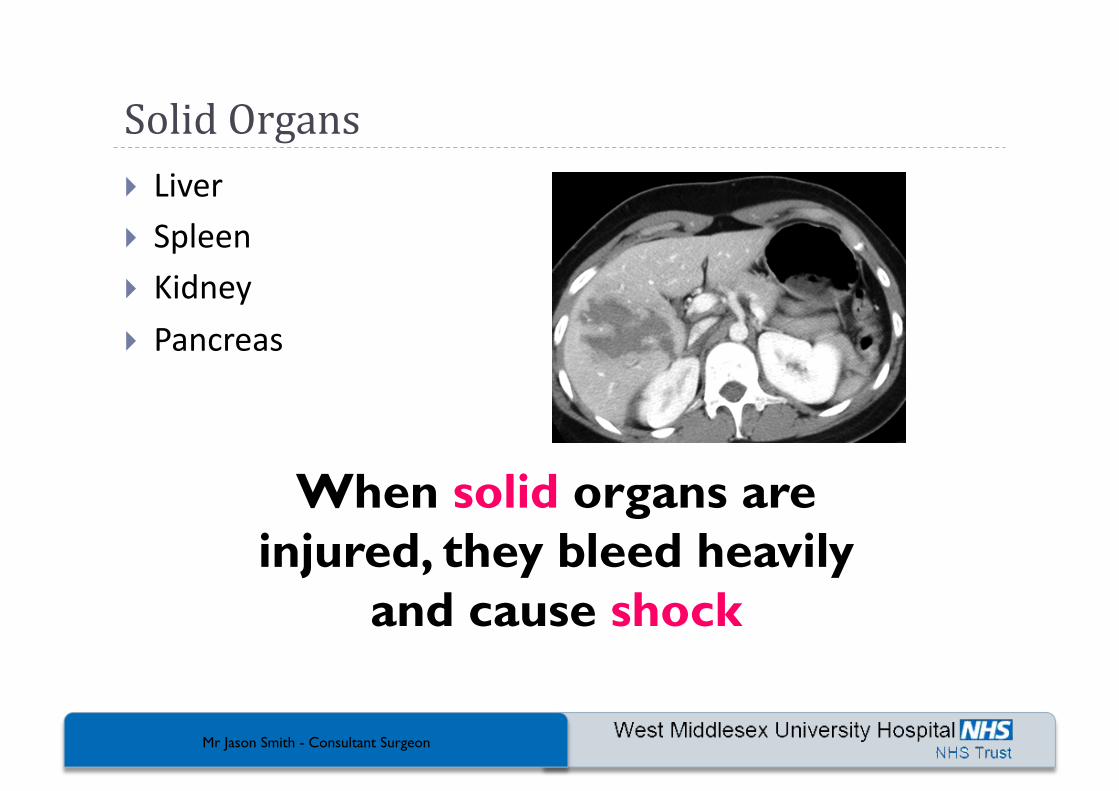
Solid Organs Liver Spleen Kidney
Pancreas
When solid organs are injured, they bleed heavily
and cause shock
Mr Jason Smith - Consultant Surgeon
Patient Assessment – Initial Views Does the pa4ent look ill, sep4c or shocked?
Call for help!
Are they lying s4ll (peritoni4s, shock),
or rolling around in agony (colic)?
Assess and manage Airway, Breathing and Circula4on as a priority (as per ALS/ATLS).
Mr Jason Smith - Consultant Surgeon
Patient Assessment – Initial Views As per ATLS, Mx occurs at the same 4me as assessment & diagnosis Large bore venflon – large vein
Oxygen
Analgesia (limited)
“Am I out of my depth?” “Do I have enough help?”
Documenta4on!! Safety -‐ you
Mr Jason Smith - Consultant Surgeon
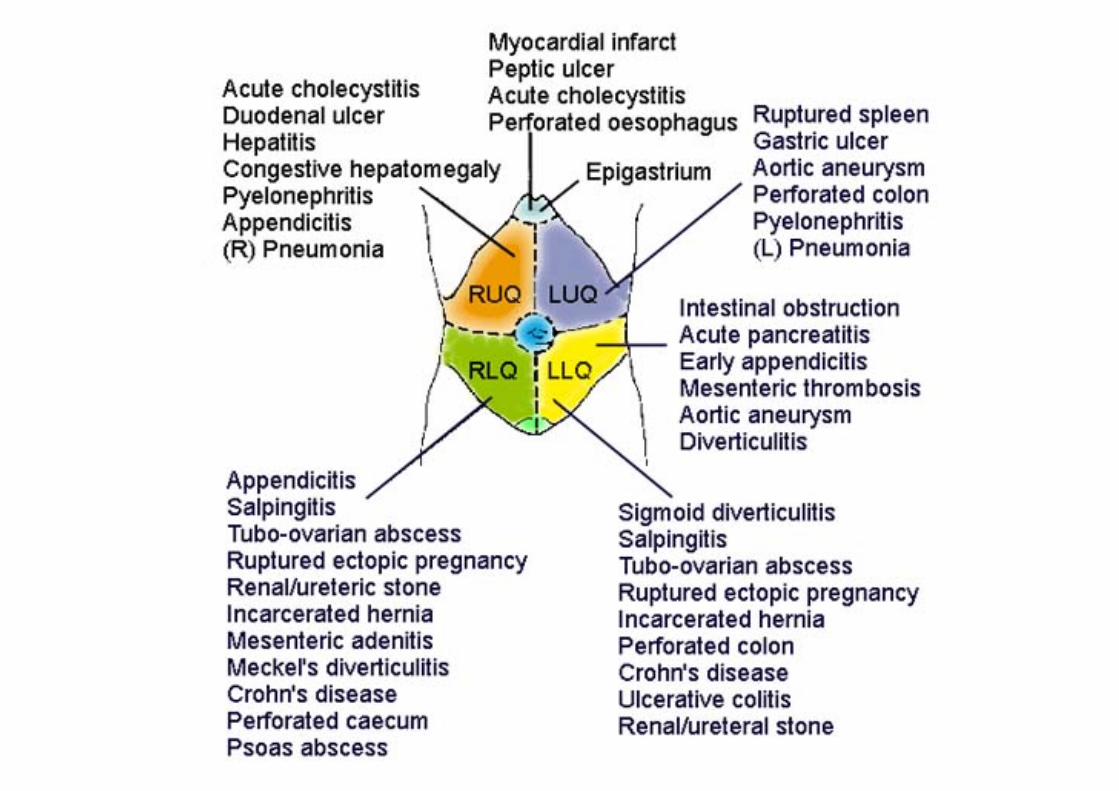
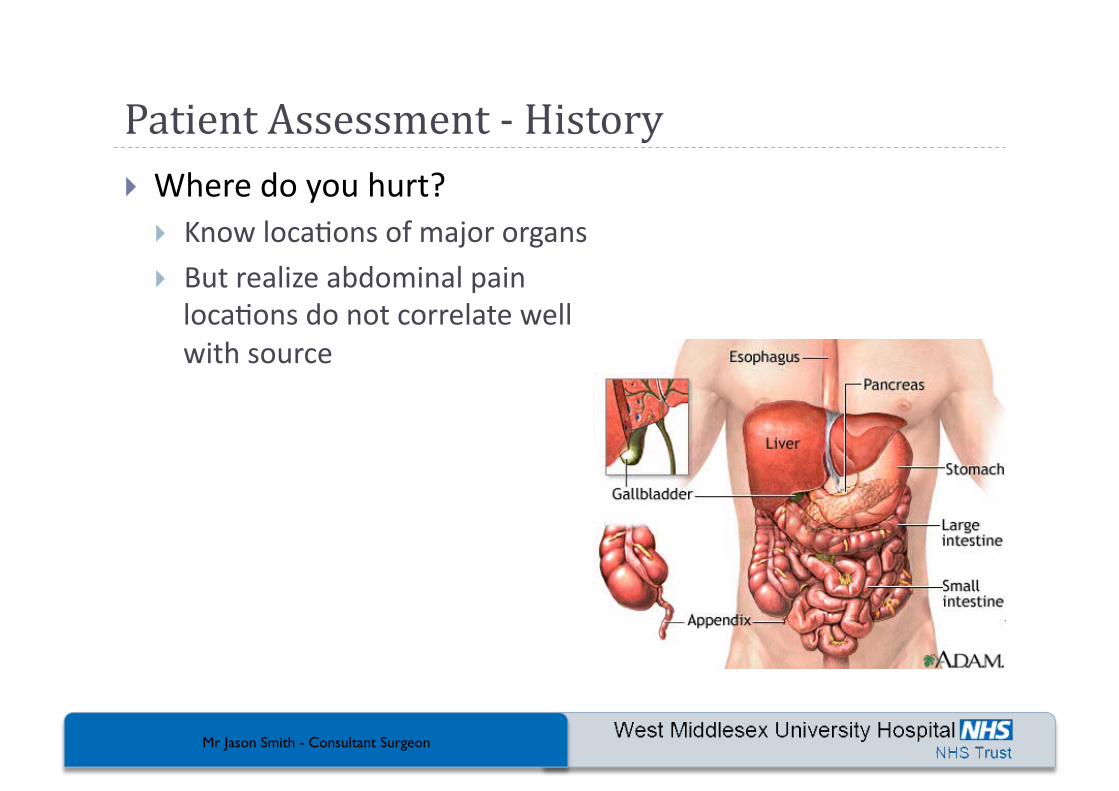
Patient Assessment -‐ History Where do you hurt?
Know loca4ons of major organs
But realize abdominal pain loca4ons do not correlate well with source
Mr Jason Smith - Consultant Surgeon
Patient Assessment -‐ History What does pain feel like?
Steady pain -‐ inflammatory process
Crampy pain -‐ obstruc4ve process
Sharp – peritoneal irrita4on
Dull – peritoneal stretching
Mr Jason Smith - Consultant Surgeon
Patient Assessment -‐ History Was onset of pain gradual or sudden? Sudden = perfora4on, hemorrhage, infarct
Gradual = peritoneal irriga4on, hollow organ distension
Mr Jason Smith - Consultant Surgeon
Patient Assessment -‐ History Does pain radiate (travel) anywhere?
Right shoulder, angle of right scapula = gall bladder
Around flank to groin = kidney, ureter Into middle of back = pancreas, duodenum
Mr Jason Smith - Consultant Surgeon
Patient Assessment -‐ History
Dura4on? <6 hour dura4on = ? surgical significance
Nausea, vomi4ng? Bloody? “Coffee Grounds”?
Any blood in GI tract = Emergency until proven otherwise
Mr Jason Smith - Consultant Surgeon
Patient Assessment -‐ History
Change in urinary habits? Urine appearance? Change in bowel habits? Appearance of bowel movements? Melena?
Mr Jason Smith - Consultant Surgeon
Patient Assessment -‐ History Regardless of underlying cause vomi4ng or diarrhea can be a problem because of associated volume loss
Everybody has pancreatitis until proven otherwise
Mr Jason Smith - Consultant Surgeon
Patient Assessment -‐ History
Females Last menstrual period?
Abnormal bleeding?
In females, abdominal pain = Gynaeproblemuntil proven otherwise
In females, abdominal pain = Pregnant until proven otherwise
Mr Jason Smith - Consultant Surgeon
Physical Exam General Appearance
Lies perfectly s4ll inflamma4on, peritoni4s
Restless, writhing obstruc4on
Abdominal distension?
Ecchymosis around umbilicus, flanks?
Mr Jason Smith - Consultant Surgeon
Physical Exam
Vital signs Tachycardia ? Early shock (more important than BP)
Rapid shallow breathing peritoni4s
Young / Old patients have different responses to fluid loss
Mr Jason Smith - Consultant Surgeon
Physical Exam Palpate each quadrant
Work toward area of pain
Warmhands, gentle approach! Pa4ent on back, knee bent (helps relax)
Use child’s own hand
Note tenderness, rigidity, involuntary guarding, voluntary guarding (steth-‐test), masses
Mr Jason Smith - Consultant Surgeon
Physical Exam Bowel Sounds
Listen 1 minute in each quadrant
Listen before feeling Absent bowel sounds ileus, peritoni4s, shock
Auscultating bowel sounds has no value in trauma patients
Auscultating bowel sounds in reality is a waste of time in the acute phase
Mr Jason Smith - Consultant Surgeon
Management Airway High flow O2
An4cipate vomi4ng, appropriate clothing, bowel
An4cipate hypovolemia – hence large bore cannulae Nothing by mouth, un4l DDx established Limited analgesics
Mr Jason Smith - Consultant Surgeon
Management In adults > 30, consider possibility of referred cardiac pain.
In females, consider possible gynaeproblem, especially tubal ectopic pregnancy
Mr Jason Smith - Consultant Surgeon
Acute Abdomen -‐ Investigations Urinalysis FBC, U&E Plain AXR
(CT)
Mr Jason Smith - Consultant Surgeon
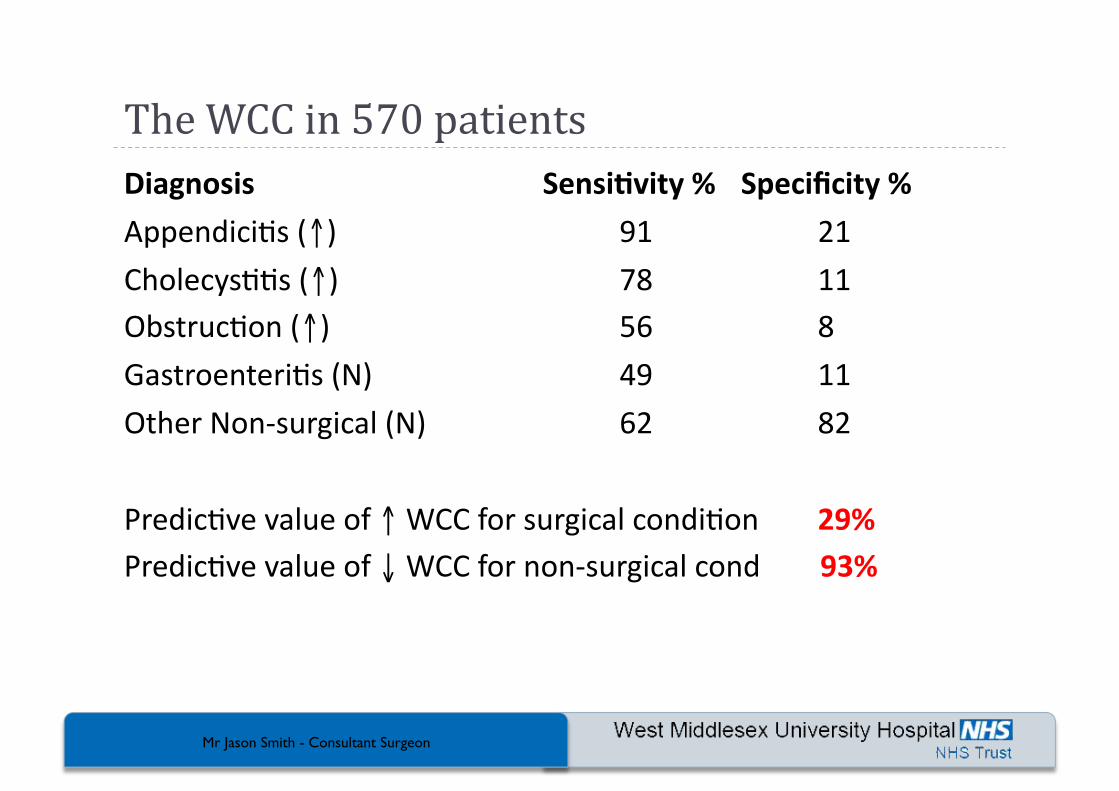
The WCC in 570 patients Diagnosis Sensi+vity % Specificity %
Appendici4s (↑) 91 21
Cholecys44s (↑) 78 11 Obstruc4on (↑) 56 8
Gastroenteri4s (N) 49 11
Other Non-‐surgical (N) 62 82
Predic4ve value of ↑ WCC for surgical condi4on 29% Predic4ve value of ↓ WCC for non-‐surgical cond 93%
Mr Jason Smith - Consultant Surgeon
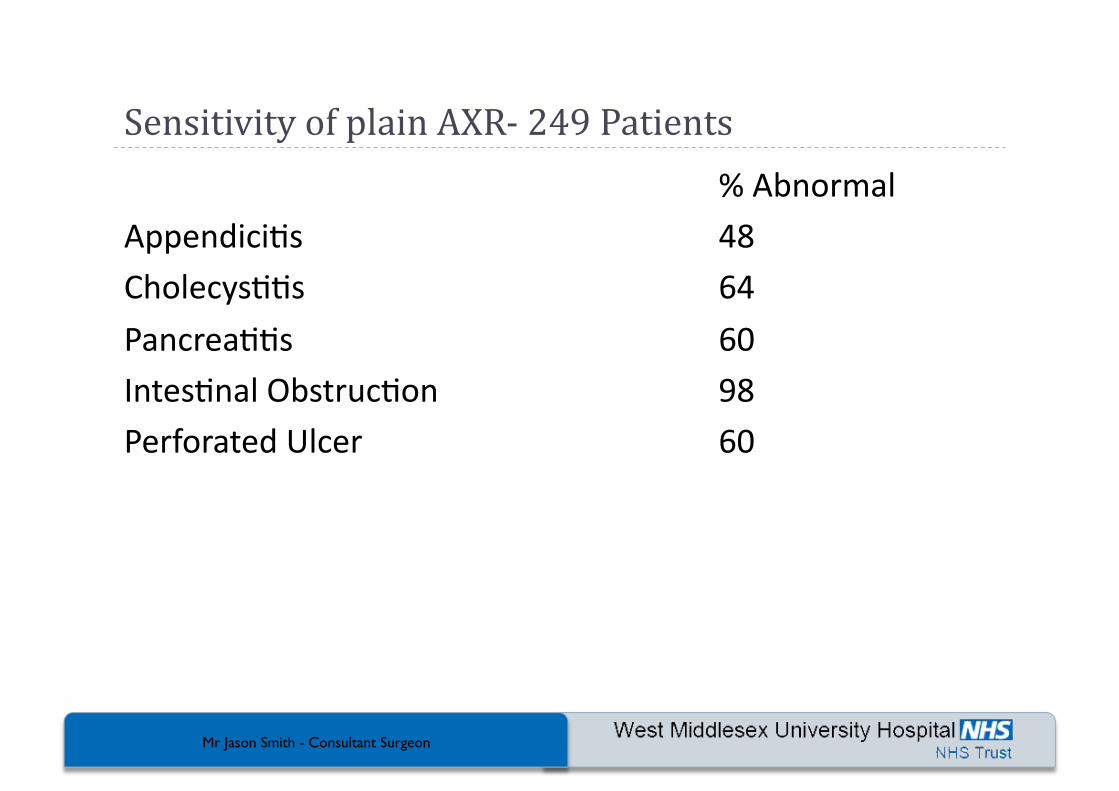
Sensitivity of plain AXR-‐ 249 Patients % Abnormal
Appendici4s 48 Cholecys44s 64
Pancrea44s 60 Intes4nal Obstruc4on 98 Perforated Ulcer 60
Mr Jason Smith - Consultant Surgeon
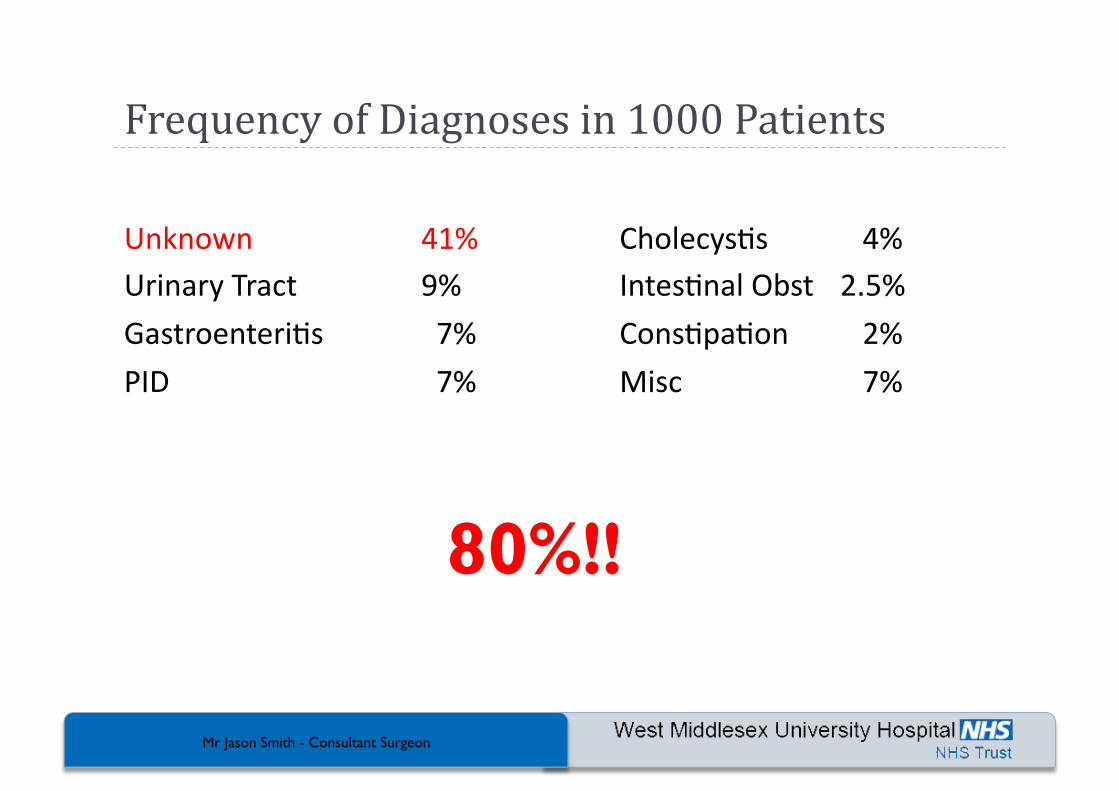
Frequency of Diagnoses in 1000 Patients
Unknown 41% Cholecys4s 4% Urinary Tract 9% Intes4nal Obst 2.5%
Gastroenteri4s 7% Cons4pa4on 2%
PID 7% Misc 7%
80%!!
Mr Jason Smith - Consultant Surgeon
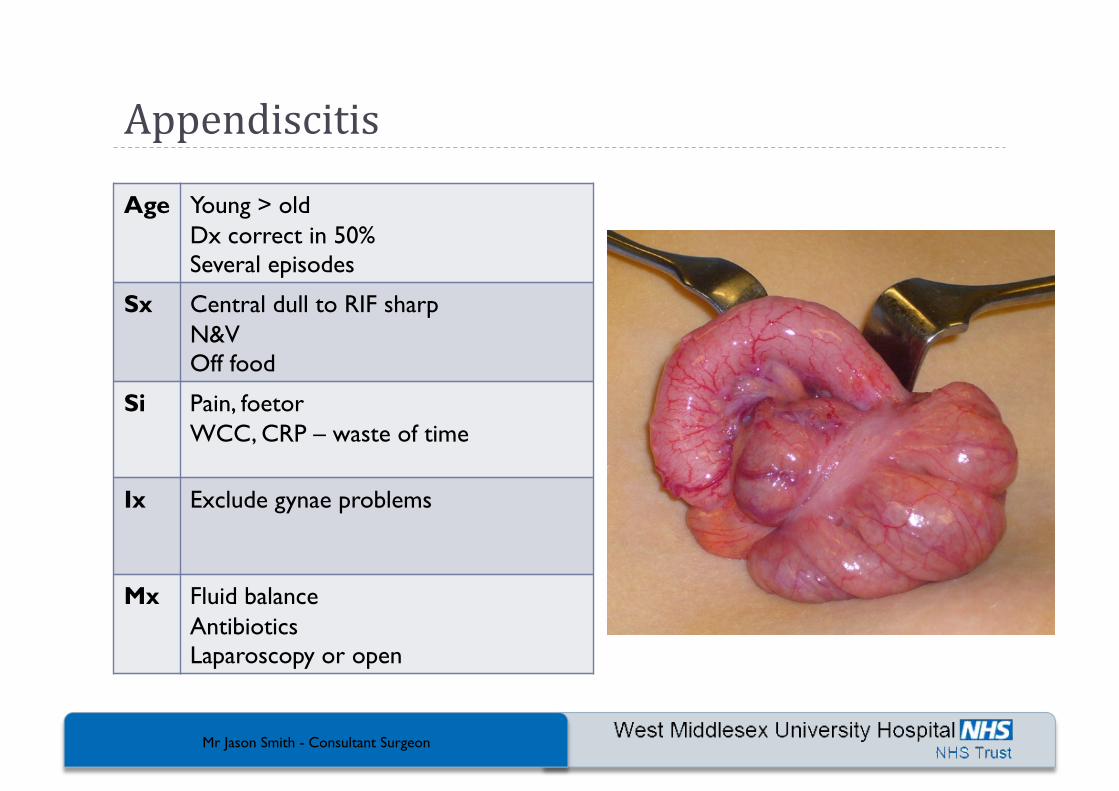
Appendiscitis
Age Young > old Dx correct in 50% Several episodes
Sx Central dull to RIF sharp N&V Off food
Si Pain, foetor WCC, CRP – waste of time
Ix Exclude gynae problems
Mx Fluid balance Antibiotics Laparoscopy or open
Mr Jason Smith - Consultant Surgeon
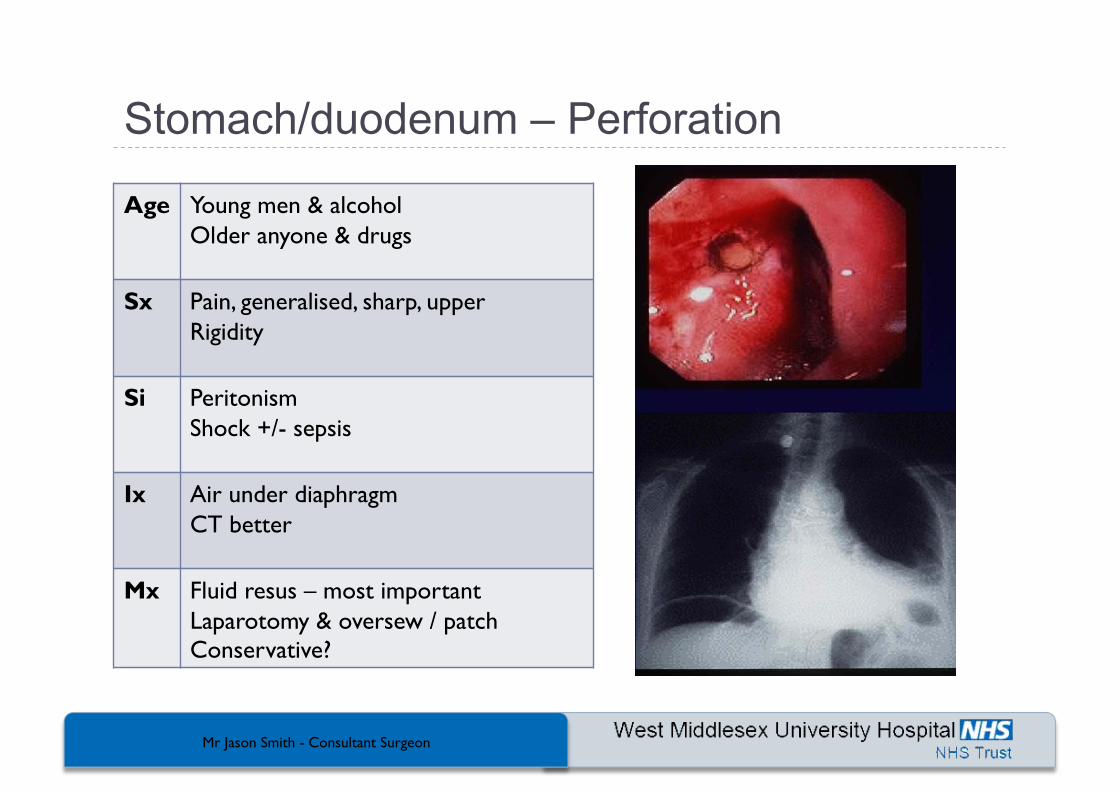
Stomach/duodenum – Perforation
Age Young men & alcohol Older anyone & drugs
Sx Pain, generalised, sharp, upper Rigidity
Si Peritonism Shock +/- sepsis
Ix Air under diaphragm CT better
Mx Fluid resus – most important Laparotomy & oversew / patch Conservative?
Mr Jason Smith - Consultant Surgeon
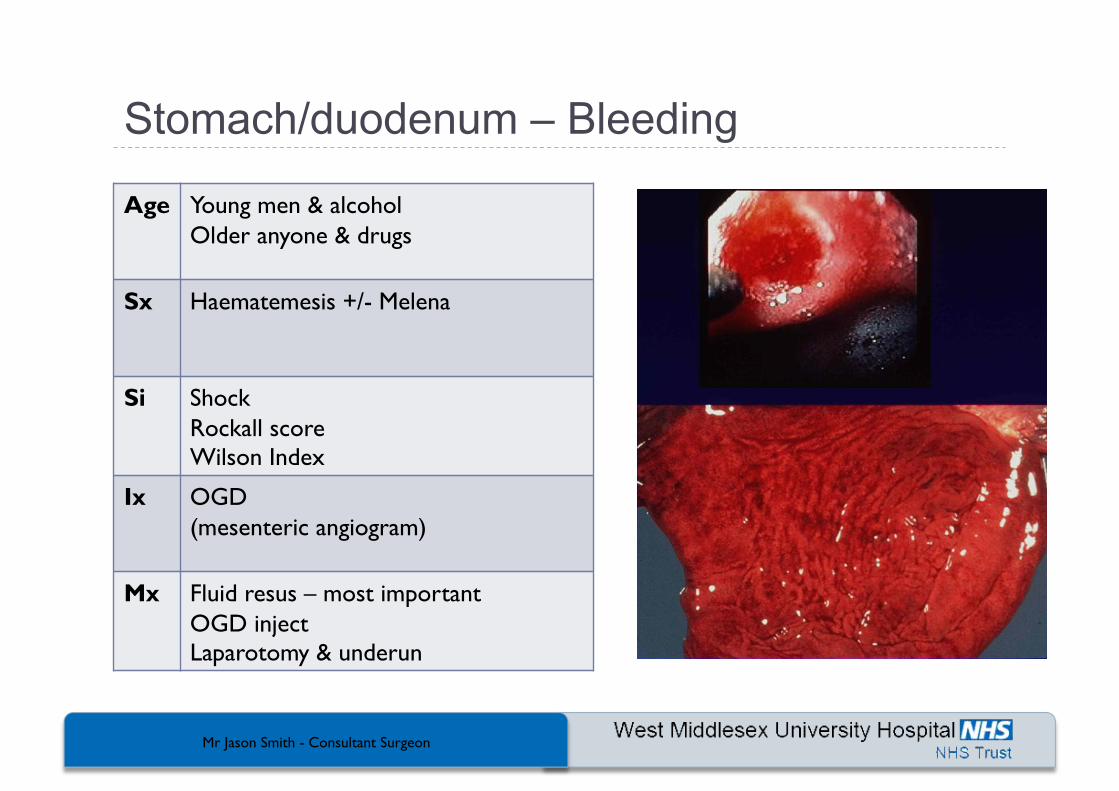
Age Young men & alcohol Older anyone & drugs
Sx Haematemesis +/- Melena
Si Shock Rockall score Wilson Index
Ix OGD (mesenteric angiogram)
Mx Fluid resus – most important OGD inject Laparotomy & underun
Mr Jason Smith - Consultant Surgeon
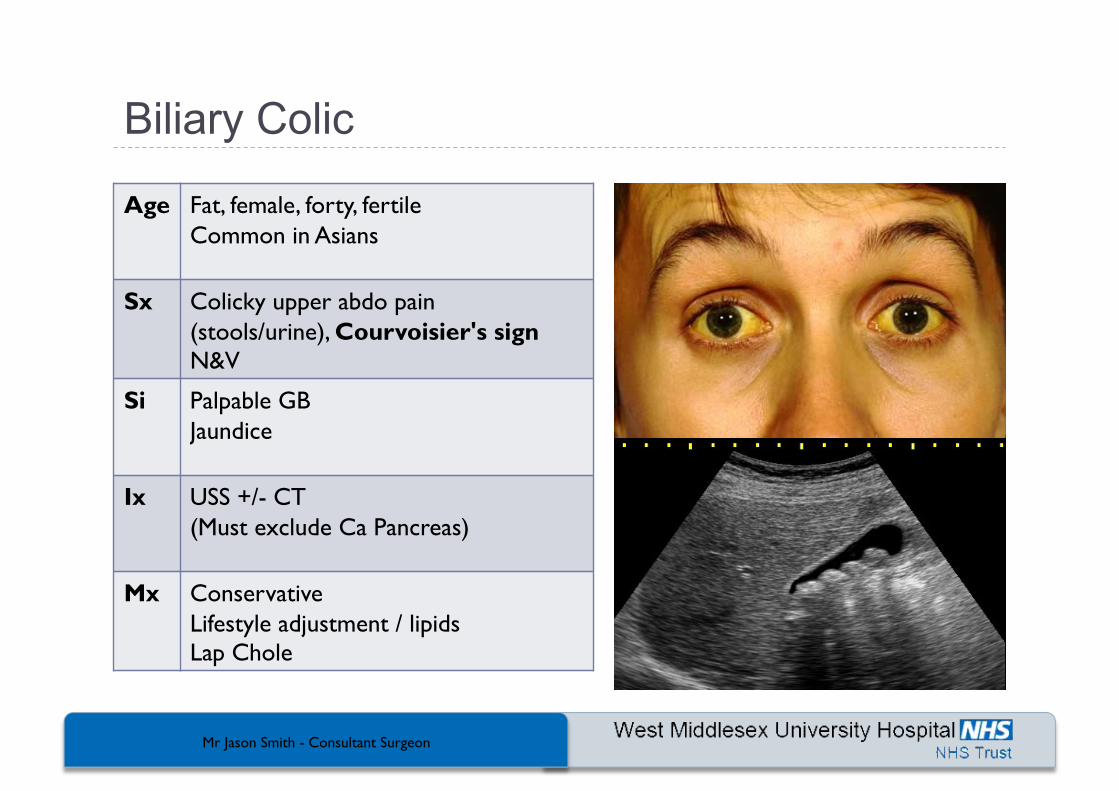
Age Fat, female, forty, fertile Common in Asians
Sx Colicky upper abdo pain (stools/urine), Courvoisier's sign N&V
Si Palpable GB Jaundice
Ix USS +/- CT (Must exclude Ca Pancreas)
Mx Conservative Lifestyle adjustment / lipids Lap Chole
Mr Jason Smith - Consultant Surgeon
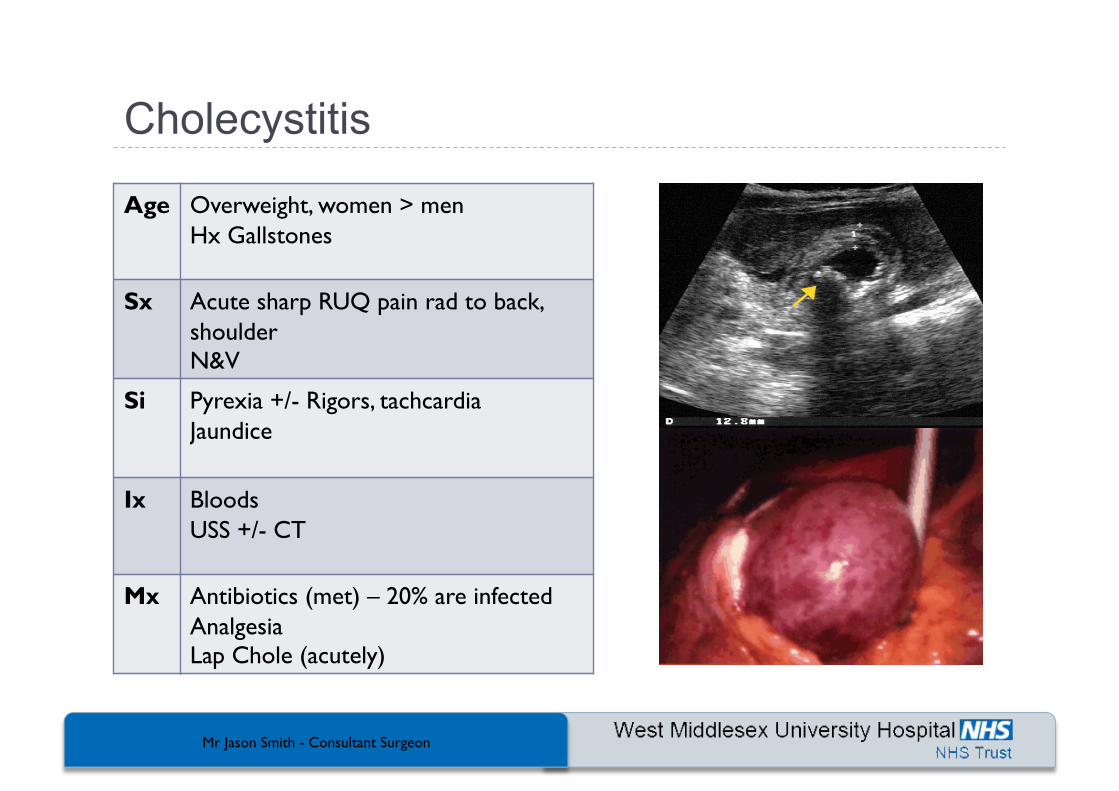
Age Overweight, women > men Hx Gallstones
Sx Acute sharp RUQ pain rad to back, shoulder N&V
Si Pyrexia +/- Rigors, tachcardia Jaundice
Ix Bloods USS +/- CT
Mx Antibiotics (met) – 20% are infected Analgesia Lap Chole (acutely)
Mr Jason Smith - Consultant Surgeon
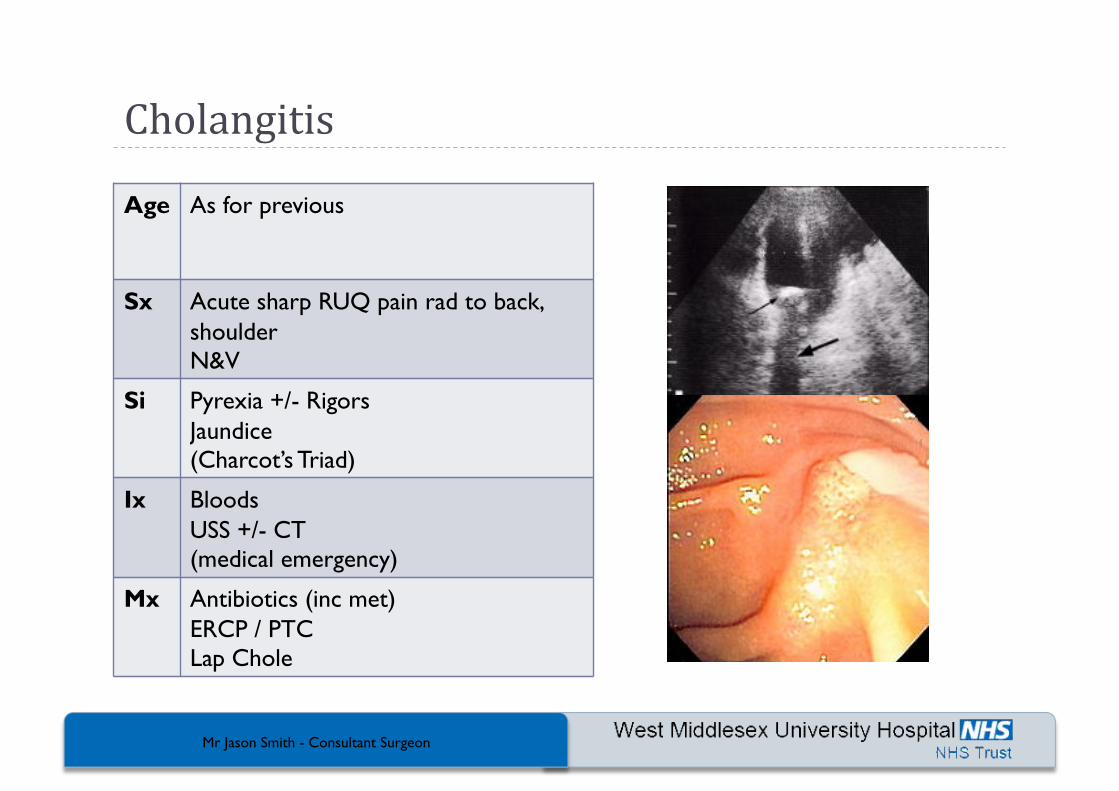
Cholangitis
Age As for previous
Sx Acute sharp RUQ pain rad to back, shoulder N&V
Si Pyrexia +/- Rigors Jaundice (Charcot’s Triad)
Ix Bloods USS +/- CT (medical emergency)
Mx Antibiotics (inc met) ERCP / PTC Lap Chole
Mr Jason Smith - Consultant Surgeon
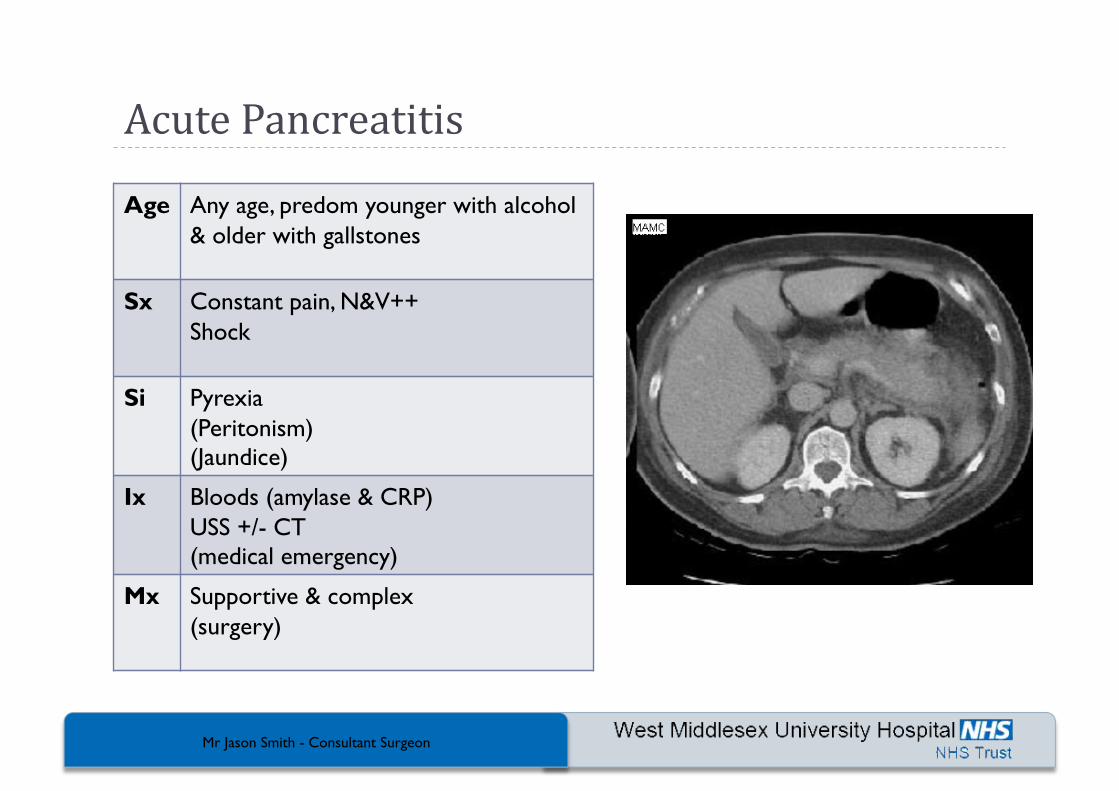
Acute Pancreatitis
Age Any age, predom younger with alcohol & older with gallstones
Sx Constant pain, N&V++ Shock
Si Pyrexia (Peritonism) (Jaundice)
Ix Bloods (amylase & CRP) USS +/- CT (medical emergency)
Mx Supportive & complex (surgery)
Mr Jason Smith - Consultant Surgeon
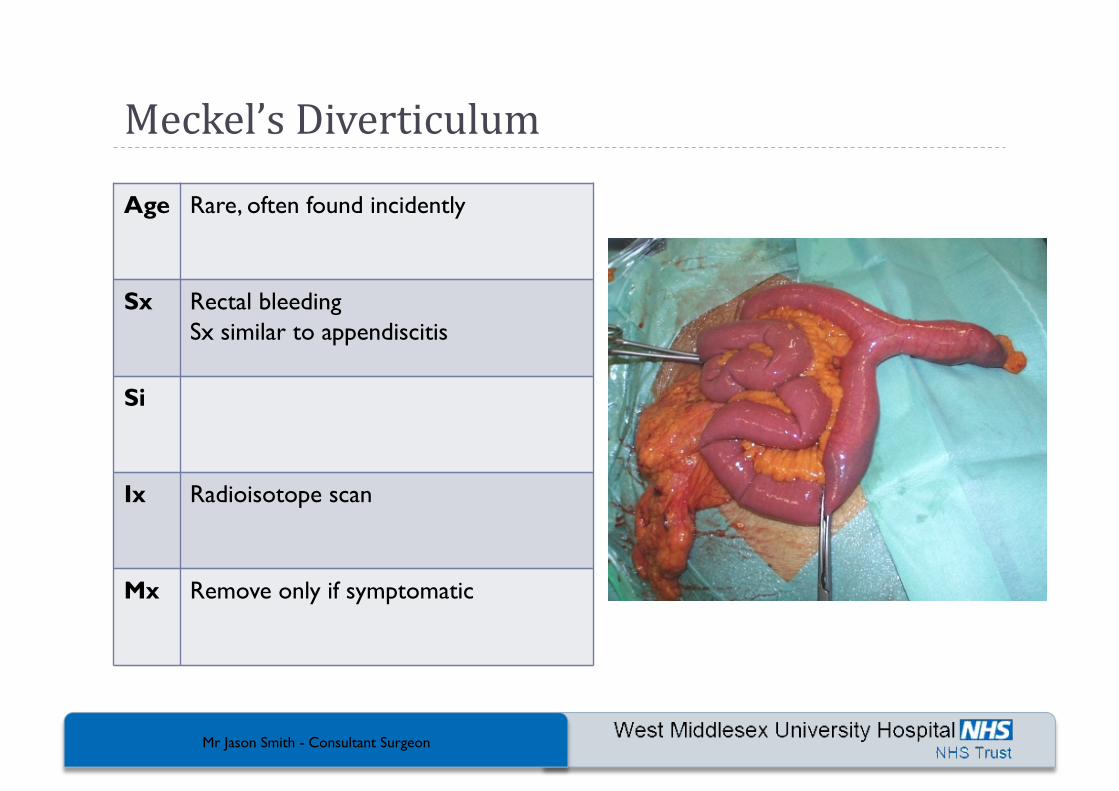
Meckel’s Diverticulum
Age Rare, often found incidently
Sx Rectal bleeding Sx similar to appendiscitis
Si
Ix Radioisotope scan
Mx Remove only if symptomatic
Mr Jason Smith - Consultant Surgeon
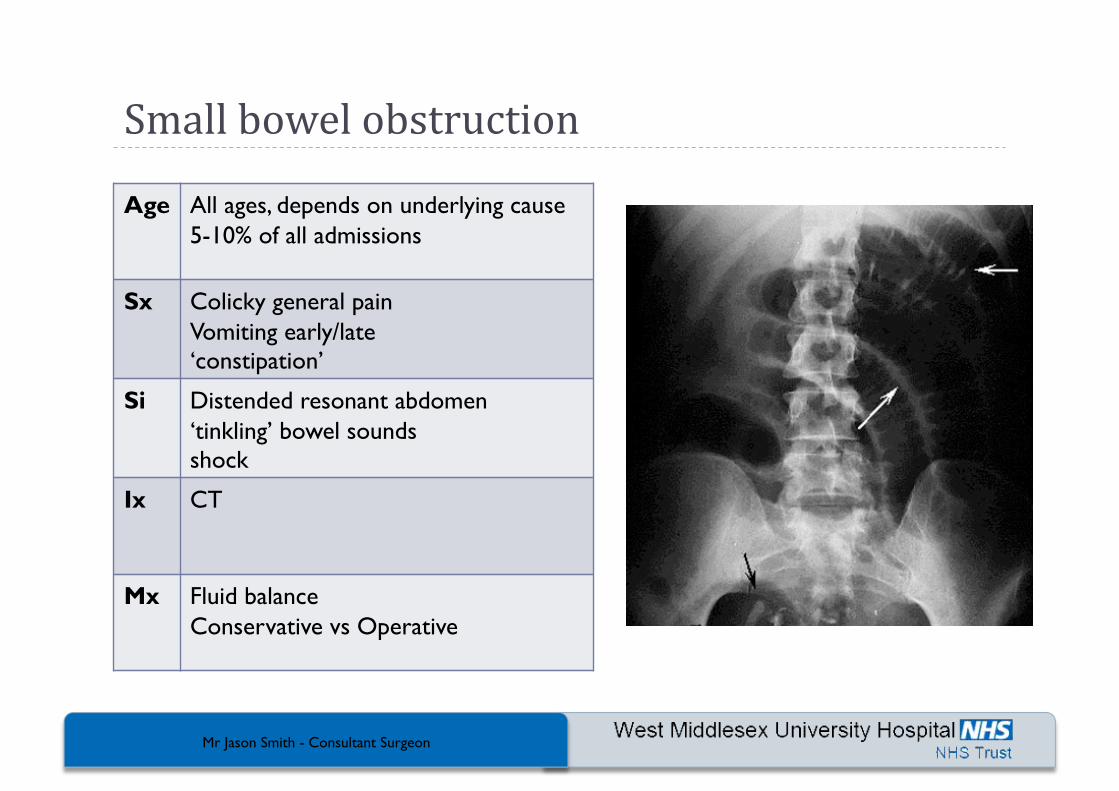
Small bowel obstruction
Age All ages, depends on underlying cause 5-10% of all admissions
Sx Colicky general pain Vomiting early/late ‘constipation’
Si Distended resonant abdomen ‘tinkling’ bowel sounds shock
Ix CT
Mx Fluid balance Conservative vs Operative
Mr Jason Smith - Consultant Surgeon
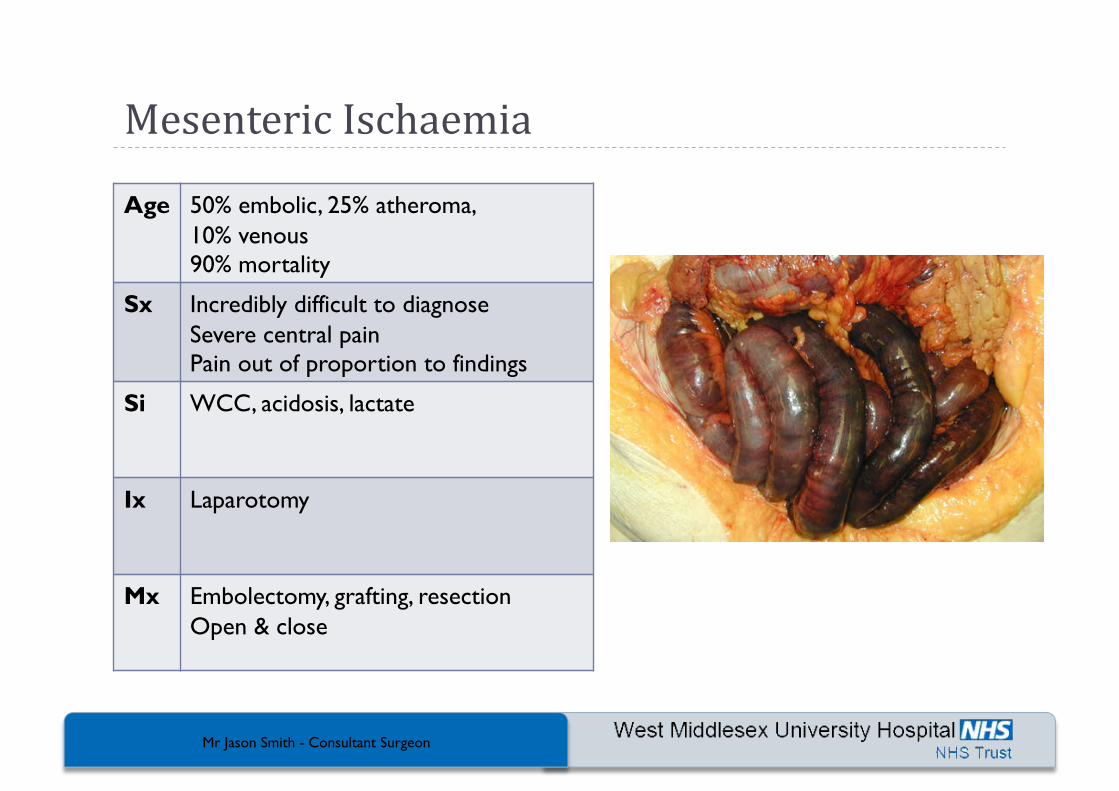
Mesenteric Ischaemia
Age 50% embolic, 25% atheroma, 10% venous 90% mortality
Sx Incredibly difficult to diagnose Severe central pain Pain out of proportion to findings
Si WCC, acidosis, lactate
Ix Laparotomy
Mx Embolectomy, grafting, resection Open & close

Mr Jason Smith - Consultant Surgeon
Acute Diverticulitis
Age 10% at 40yrs 60% by 80yrs Sx common in middle age/elderly
Sx Usually LIF pain +/- constipation +/- rectal bleeding
Si Tenderness Fever, tachycardia Raised WCC & CRP
Ix Ba enema / flexi CT
Mx Antibiotics, lifestyle 2 strikes and its out!
Mr Jason Smith - Consultant Surgeon
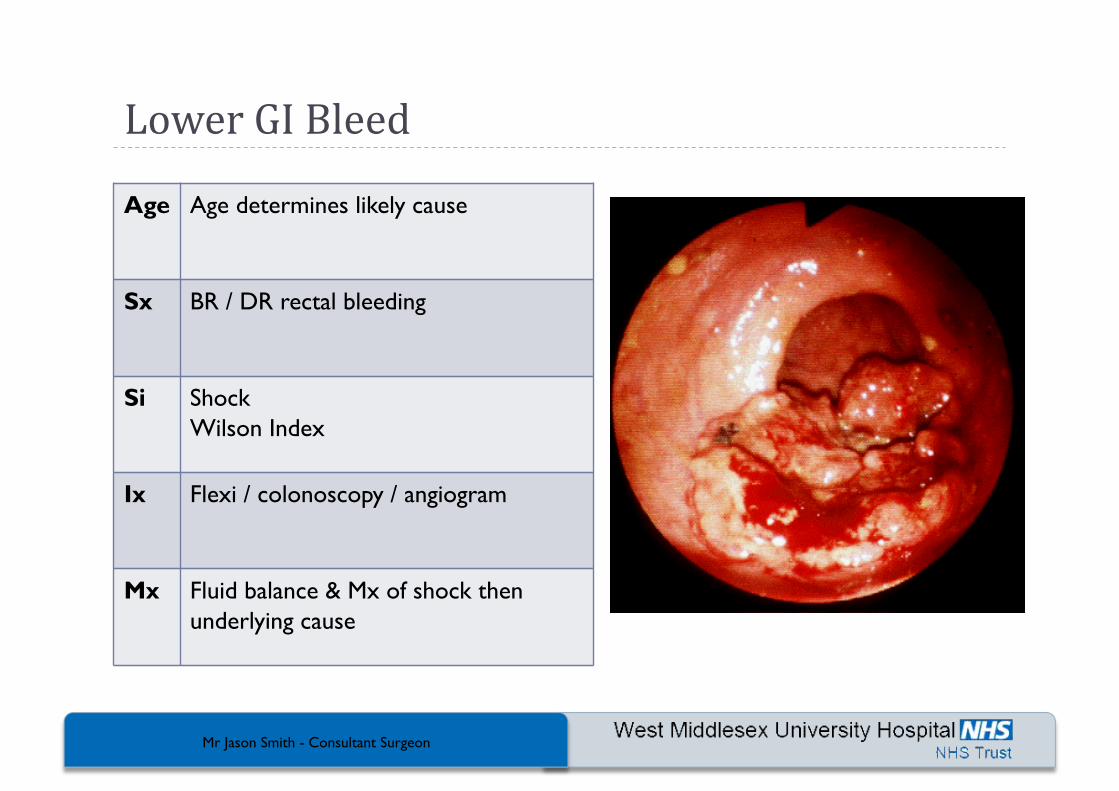
Lower GI Bleed
Age Age determines likely cause
Sx BR / DR rectal bleeding
Si Shock Wilson Index
Ix Flexi / colonoscopy / angiogram
Mx Fluid balance & Mx of shock then underlying cause
Mr Jason Smith - Consultant Surgeon
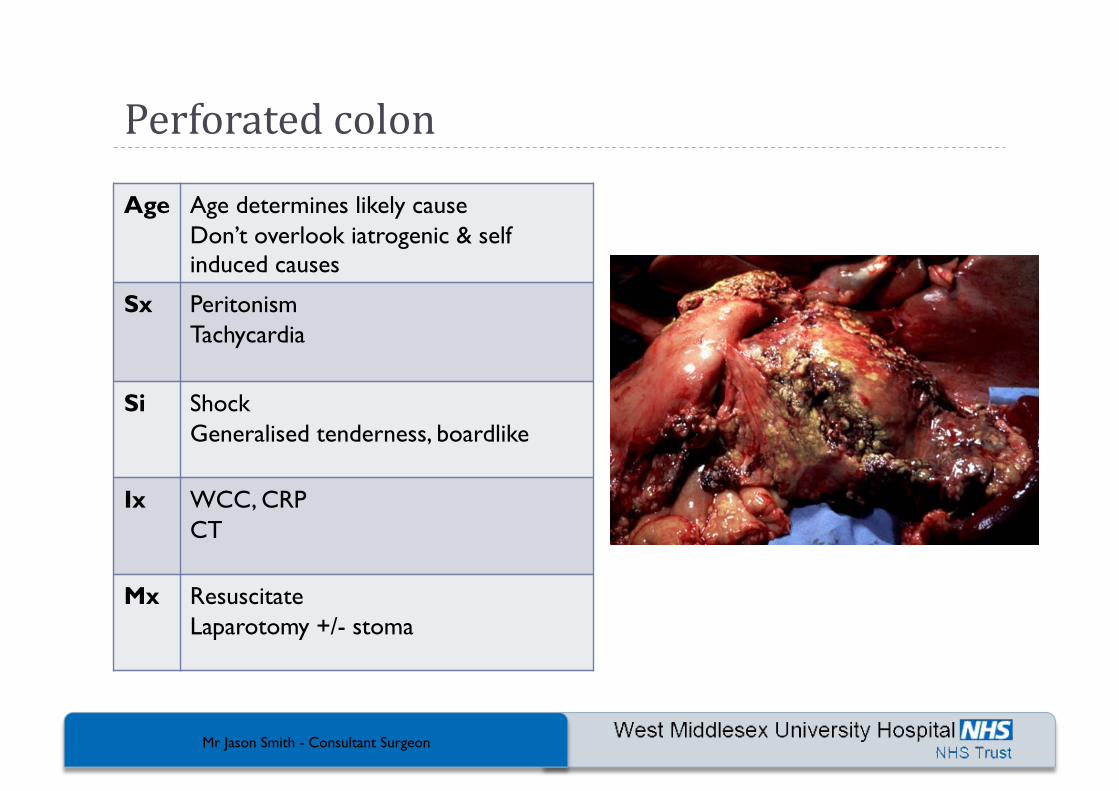
Perforated colon
Age Age determines likely cause Don’t overlook iatrogenic & self induced causes
Sx Peritonism Tachycardia
Si Shock Generalised tenderness, boardlike
Ix WCC, CRP CT
Mx Resuscitate Laparotomy +/- stoma
Mr Jason Smith - Consultant Surgeon
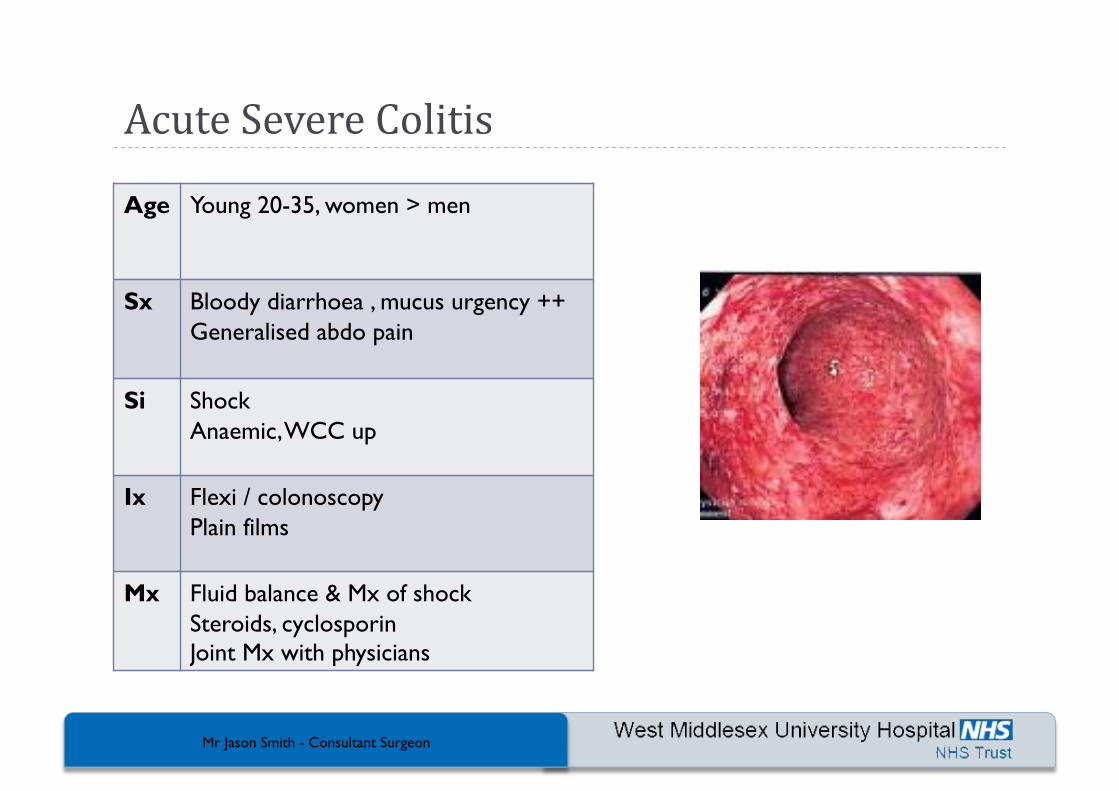
Acute Severe Colitis
Age Young 20-35, women > men
Sx Bloody diarrhoea , mucus urgency ++ Generalised abdo pain
Si Shock Anaemic, WCC up
Ix Flexi / colonoscopy Plain films
Mx Fluid balance & Mx of shock Steroids, cyclosporin Joint Mx with physicians
Mr Jason Smith - Consultant Surgeon 11/98 medslides.com 44
Acute Abdominal Pain Non-‐surgical Emergencies Mesenteric Adeni4s Acute Enteric Infec4ons Acute Enteric Poisonings
Inflammatory Bowel Disease Pancrea44s (usually)
Mr Jason Smith - Consultant Surgeon 11/98 medslides.com 45
Acute Abdominal Pain Metabolic Causes Diabe4c Ketoacidosis Heavy Metal Poisoning Acute Porphyria
Sickle Cell Crisis





















![Acute Abdomen PRESENTATION (Ingles)[1]](https://img.pdfslide.tips/doc/110x75/577cda511a28ab9e78a55ce5/acute-abdomen-presentation-ingles1.jpg)