Embed Size (px)
DESCRIPTION
Total Intravenous Anesthesia. อ.นพ.ธีรวัฒน์ ชลาชีวะ ภาควิชาวิสัญญีวิทยา โรงพยาบาลรามาธิบดี. Beneficial of TIVA. Decrease global warming from N 2 O Decrease pollution from volatile agents in OR Decrease risk in patients or operation : Suspected MH Air embolism Brain surgery - PowerPoint PPT Presentation
Citation preview

อ.นพ.ธี�รวั�ฒน ชลาช�วัะภาควั�ชาวั�สั�ญญ�วั�ทยาโรงพยาบาลรามาธี�บดี�
Total Intravenous Anesthesia

Beneficial of TIVA• Decrease global warming from N2O
• Decrease pollution from volatile agents in OR
• Decrease risk in patients or operation :– Suspected MH
– Air embolism
– Brain surgery
• More suitable during operation that difficult or impossible to use inhalational anesthesia effectively– Laryngoscope, bronchoscopy
– Thoracic surgery
– Gastroscopy or colonoscopy
• Decrease risk of PONV
• Ambulatory surgery
• Anesthesia in outside OR

Balanced Anesthesia
UnconsciousHypnosisAmnesia
AnalgesiaImmobility
Muscle relaxation
- IV anesthetic agents- Inhalation agents
- Opioid
- Musclerelaxants
Reflex suppression

Is the Patient Anesthethetized?How do you gauge the depth of anesthesia when using TIVA?
• Same skills are used as when administering volatile drugs.

Pharmacokinetics and TIVA
• Use of mathematics to describe
How the body “handles” particular drug

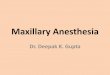
Open, three-compartment model

Organ perfusion
020Bone, ligament, cartilage
Vessel-poor
620FatFat
1950Muscle, skinMuscle
7510Brain, heart, liver, endocrine glands
Vessel-rich
CO (%)Body Mass(%)
CompositionTissue Group

Open, three-compartment model

Context Sensitive Half Time
• Time plasma concentrations take to reduce by 50% after discontinuing infusion.
• Short CSHT drugs are desired for TIVA.

Open, three-compartment model

ke0: Describing drug delivery to the effect site
the pharmacokinetic rate constant which describes the rate of equilibration between the plasma concentration and effect site.

Effector Site Delay

Effective Blood Concentration
• Potency of – Volatile drugs : MAC (anesthetic required to pr
event gross, purposeful movement in 50% of patients in response to a noxious stimulus)
– Propofol : ED50
• propofol and N2O was 4.5 mcg/ml and the ED95 was 4.7 mcg ml.
• propofol was 6.0 mcg/ml and the ED95 was 6.2 mcg/ml.

Development of delivery systems
AIMAIMmaintenance of optimum & stable anesthetic condition
1st iv. bolus injection : single, intermittent administration, iv. drip
22ndndInfusion pumpSyringe pump
33rdrdTCI

TIVA-TCI : Target Controlled Infusion
• TCI เป็�นเทคน�คท��น าเอาข้"อม#ลควัามสั�มพ�นธีข้องอ�ตราการไหลข้องยาและระดี�บยาในกระแสัเล*อดีมาค านวัณโดียเคร*�องคอมพ�วัเตอรเพ*�อควับค,มระดี�บยาในแต-ละ Compartment ให"เป็�นไป็ตามต"องการ

TIVA-TCI : Drugs suitable for
Check
wake up
time
Propof
ol Cet
1.5-2.0 µ
g/ml
=
wake up
Hypnosis Propofol
Dexmedetomidine (Etomidate not suitable due to suppressant of adrenal steroidogenesis)
AnalgesicsAlfentanilRemifentanil? fentanyl not for long infusion (Morphine not suitable )l
√
√

Propofol• เป็�นยาในกล,-ม alkylphenol ซึ่/�งเป็�นไข้ม�นในอ,ณหภ#ม�ห"อง• ป็ระกอบดี"วัย 1%propofol, 10%soybean oil as long-
chain triglycerides, 2.25%glycerol and 1.2%purified egg phosphatide ม� 0.005% disodium edetate เพ*�อ ป็0องก�น bacterial growth
• Metabolism– Rapid metabolism in liver by conjugation and
glucorodination – Renal excretion– Extrahepatic metabolism ; lung, small intestine,
kidneys

• CNS– Decrease CMRO2, CBF, ICP– Anticonvulsion– Myoclonic, hiccup
• CVS– Venous dilatation, decrease PVR &CO -->
hypotension– Greater CVS than thiopental
• Respiration– may be transient apnea– decrease TV, rate

• Age– increased sensitivity of the elderly to the effects of
propofol . ke0, hence plasma effect site equilibration has been reported not to be changed by age.
– These properties suggest that induction in elderly patients should be achieved with lower plasma concentrations than in younger adults, however it should also be titrated more slowly to avoid side effects.
Pharmacodynamic variability

• Systemic disease– It has often been assumed– patients with significant disease would require
less anaesthetic• increased central nervous system sensitivity to the
drug• increased free fraction of drug secondary to
reduced plasma protein binding (subtle pharmacokinetic changes)
Pharmacodynamic variability

ในกรณ�ไม-ใช"เคร*�อง TCI
การนำ�าสลบ ขนำาดยานำ�าสลบโดยปกติ�ใช้� 1-2.5 มก./ กก. โดย
- ในำผู้��ใหญ่� ไม�ได�ร�บยา opioid หร�อ benzodiazepine เป�นำยาpremedication ใช้� 2.25-2.5 มก./ กก.
- คนำแก�อาย!มากกว่�า 60 ป#ไม�ได�ร�บยา opioid หร�อbenzodiazepine เป�นำยา premedication ใช้� 1.75 มก./ กก.
- เด$กไม�ได�ร�บยา opioid หร�อ benzodiazepine เป�นำยาpremedication ใช้� 2-3 มก./ กก.
การป%องก�นำ hypotension ในำผู้��ป'ว่ยที่)*ป'ว่ยเร�+อร�ง หร�อผู้��ป'ว่ยที่)*มาร�บ การผู้�าติ�ดห�ว่ใจ คว่รค�อยๆให� propofol 10-30 มก. จนำกระที่�*งผู้��
ป'ว่ยสลบและคว่รให�สารนำ�+านำ�าไปก�อนำให�เพี)ยงพีอ

Maintenance dose
- ในำกรณี)ฉี)ดยาเป�นำคร�+งคราว่(intermittent bolus) ให� 10-40 มก. ที่!กๆ 2-3 นำาที่)
- ในำกรณี)หยดยาอย�างติ�อเนำ�*อง(continuous infusion) หล�งให�ยานำ�าสลบ หยดยา 140 มคก./กก./ นำาที่) เป�นำเว่ลา 10
นำาที่) ติ�อด�ว่ย 100 มคก./กก./นำาที่) โดยให�ร�ว่มก�บ fentanyl 0.02 มคก./กก./นำาที่) หร�อ alfentanil 0.25 มคก./กก./นำาที่)
ในกรณ�ไม-ใช"เคร*�อง TCI

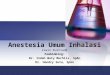
Less
Pain
With
N2OWithout N2O
Start 8 10 12
>10 mins. 5 7 9
>2 hrs. 3 5 7
Initial infusion rate 10 minSubsequence adjustmentso as to maintain a stable level of anesthesia
Not easy to control Time-consuming calculation No compensate for interrupted infusion
Delayed emergence !!!Require skill & experience
TIVA-MCI : manually-controlled infusion
“ “ are used to designate are used to designate manualmanual adjustment of adjustment of
infusion rates for anaesthesia infusion rates for anaesthesia syringe pumpssyringe pumps””

10 นาท�-2 ชม
> 2 ชม
10 นาท�แรก
10 นาท�-2 ชม
> 2 ชม
> 2 ชม10 นาท�-2 ชม
10 นาท�แรก
10 นาท�แรก
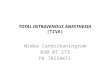
3
5
7
9
11
13Pr
opof
ol in
fusio
n ra
te (m
g/kg
/hr)
ห�ติถการที่)*ไม�ปว่ด ผู้�าติ�ดในำช้�องที่�องOpioid + N2O
ผู้�าติ�ดในำช้�องที่�องOpioid

หย!ดยาก�อนำเว่ลาที่)*ติ�องการให�ผู้��ป'ว่ยติ�*นำ
30 (20-47) นำาที่)6 ช้ม.
25 (9-43) นำาที่)5 ช้ม.
20 (8-33) นำาที่)4 ช้ม.
15 (6-23) นำาที่)3 ช้ม.
12.5 (5-20) นำาที่)2 ช้ม.
10 (4-15) นำาที่)1 ช้ม.
75. ( -412) นำาที่)30 นำาที่) 5 ( -38) นำาที่)15 นำาที่)
คว่รหย!ดยาก�อนำให�ติ�*นำระยะเว่ลาของการสลบ



Target = ?
CP50 2.7 – 3.4 µg/ml loss of response to verbal or tactile stimuli*
Cet 2-3 µg/ml loss of eyelash reflex
Cet 4-8 µg/ml for anesthetic procedure
Intubation, LMA
* : Vuyk J et al. Anesthesiology 1992; 77: 3. Crankshaw DP et al. Anaesth Intensive Care 1994; 22: 481. Smith C et al. Anesthesiology 1994; 81: 820.
TCI –propofol concentration
Target concn based on•Level of stimulation•Drug interaction•Desired clinical endpoint•Decrement time•Intraindividual variability


•MO 5-10mg•Midazolam1-2mgPropofol TCI
•Cet 2-3 µg/ml
loss of response
Check ventilation
Muscle relaxant
Ventilate 1.0-1.5 min Cet 4-8 µg/ml
for intubation
Ventilate 1.0-1.5 minTTPE
↓Cet 2-3 µg/ml 2-3 µg/ml wait for wait for next painful stimulinext painful stimuli↑↑Cet 4-6 Cet 4-6 µg/ml µg/ml for skin incisionfor skin incision
TCI for induction & Intubation

Propofol in different lipids
• The standard propofol formulation contains 10%soybean oil as long-chain triglycerides.– Pain on injection 14.7%
• Long- and medium-chain trigycerides reduced incidence of pain on injection to 2.7%.

Propofol-related infusion syndromeHigh dose infusion >5 mg/kg/hr for > 48 hrs
Abrupt onset of profound bradycardia, metabolic acidosis lipemic plasma,
renal failure, fatty liver, rhabdomyolysis or myoglobinuria
Risk factors : poor oxygen delivery, sepsis serious cerebral injury
Monitor : acidosis, K+, renal function
symptomssymptomssymptomssymptoms

Thank you for your attention

• Preparation• 2.5% pale yellow solution pH 10 - 11• bacteriostatic• Mechanism of action• Interacts with GABA receptor-->membrane
hyperpolarization• Terminal of action• Redistribution-->ultrashort acting• Metabolism --- liver
THIOBARBITURATE(THIOPENTAL)

• Excretion--renal excretion of water-soluble
• Dose
• 3-5 mg/kg IV depending on age, ASA :
• Onset = 60 seconds
• Recovery = 5-10 mins

• Pharmacologic actions• CNS
– Decrease ICP, CMRO2, CBF– Anticonvulsant 50-100 mg IV– Cerebral protection
• Create electrical silence ;15-40 mg/kg then 2-4 mg/kg/hr
• CVS– Venous dilatation--> CO, ABP– Baroreceptor reflex– Increase HR
• CO may decrease markedly– Hypovolemia– Beta blocker– Previous heart disease
• Respiratory– Depression medullary center--> RR, TV– Apnea– Upper airway obstruction– Airway reflex
• Bronchospasm• Laryngospasm

Side Effects
• Thrombophlebitis
• Intraarterial injection-->spasm
• Allergic reaction( histamine release )
• Hypotension
• Subcutaneous injection-->necrosis
Contraindication *PORPHYRIA*

• Minor tranquilizer
• Antianxiety, sedation
• Amnesia
• Control convulsion
• Relax skeletal muscle
BENZODIAZEPINES

DIAZEPAM (Valium)
• Highly lipid soluble• Insoluble in water• Mechanism of action• Modifies GABA receptor activity• Metabolism--> hepatic• Excretion--> renal• Indication
– Premedication : 0.05-0.1 mg/kg – Induction of anesthesia :0.3-0.5 mg/kg– Intravenous sedation : 1-2 mg p.r.n. IV– Treatment of seizure

• pH<4-->Water soluble• Physiologic pH--> lipid soluble• Mechanism of action• Modifies GABA receptor activity• t 1/2 = 1 - 4 hr.• Metabolism--> hepatic• Excretion--> renal• Indication
– Premedication : 0.07-0.15 mg/kg– induction of anesthesia : 0.15-0.3 mg/kg– intravenous sedation : 0.5-1 mg repeat to effect
MIDAZOLAM (Dormicum)

• CNS– Decrease CMRO2, CBF– HR increase due to drug induce vagolysis– Anxiolysis, amnesia (dose related)– Anticonvulsant properties
• CVS– Slight decrease SVR, BP
• Respiratory– Dose related respiratory depression – Respiratory response to CO2 decrease– Lower incidence of apnea– Careful titration
BENZODIAZEPINES

• Central acting benzodiazepine antagonist• Dose 0.25 - 0.5 mg.• Onset in 30 - 60 sec.• Duration 1 hr.• Liver metabolized• Side effects• dizziness, anxiety, nausea, vomiting,
agitation
FLUMAZENIL (Anexate)

• Preparation• Water soluble, racemic mixture• Mechanism of action• Act on NMDA receptor• Act on opioid and cholinergic receptor• Causes dissociation• Metabolism-- hepatic• Norketamine--1/5 potency of ketamine• Excretion--renal
KETAMINE

• Indications– induction of anesthesia
– sole anesthesia
– premedication
• DOSE– 1-2 mg/kg IV induction– 3-5 mg/kg IM induction– 0.2-0.8 mg/kg IV sedation-->5-20 mcg/kg/min– 15-45 mcg/kg/min with O2/N2O maintenance

• CNS– Increase CMRO2, CBF, ICP– Amnesia, analgesia
• CVS– Increase MAP, CO, HR– If cathecholamine depletion or autonomic – block--> depress myocardium
• Respiration– Bronchodilation--sym mediated– Relative preservation of laryngeal reflexs

• 2,6 di-isopropylphenol; 1% solution in
• egg white lecithin emulsion
• Mechanism
• May be at GABA receptor
• Metabilism--liver
• Excretion--renal
PROPOFOL (Dripivan)

• CNS– Decrease CMRO2, CBF, ICP– Anticonvulsion– Myoclonic, hiccup
• CVS– Venous dilatation, decrease PVR &cardiac – depression--> hypotension– Greater CVS than thiopental
• Respiration– may be transient apnea– decrease TV, rate

• Indication– Induction of anesthesia– Sole anesthetic for short procedure – Treatment of seizures
• Dose– 2-2.5 mg/kg IV induction– 100-200 mcg/kg/min maintenance– 25-100 mcg/kg/min sedation

ETOMIDATE
• Mechanism– May act at GABA receptor at reticular
activating system
• Metabolism--hepatic• Excretion--renal• Dose
– 0.2-0.4 mg/kg IV induction– onset 30-60 sec.– Recovery = 5 mins

• CNS– may increase EEG activity in those with – epilepsy– Myoclonic movement (pretreat c opioid )– CBF, ICP, CMRO2 decrease– CPP maintained– Enhance SSEP response
• CVS-- STABLE• Respiration
– Transient apnea– Decrease rate and TV
• Disadvantage ; Adrenocortical suppression


OPIOIDS
• Agonist
• Partial agonist
• Agonist -antagonist
• Antagonist

• Agonist Morphine CodeinePethidine
SufentanylFentanyl
Alfentanyl
• Partial agonist Buprenorphine• Agonist - antagonist Pentazocine,
Nalbuphine, Nalorphine
• Antagonist Naloxone

• Benefits– Good analgesia (dull pain)– Sedation, euphoria– Antitussive
• Indications – Premedication– Supplement anesthesia– Sole anesthesia– Analgesia
• Acute postoperative pain• Cancer pain

Side effects
• Nausea and vomiting• Pruritus• Visceral smooth
muscle– Constipation– Biliary spasm– Ureteral spasm
• CVS– Hypotension– Bradycardia
• RR and response• to PaCO2• Chest wall rigidity• Urinary retension• Histamine release

MORPHINE
• Supraspinal analgesia
• Increase pain threshold
• Sedation, euphoria
• Pruritus, urinary difficulty
• Histamine release
• Spasm of sphincter of oddi
• Anti - tussive
• Dose related resp. depression

PETHIDINE
• Potency 1/10 of MOSO4
• Equianalgesic dose : same effect of resp. depression
• Shorter duration of action
• Atropine - like effects : HR,bronchodilatation, mydriasis
• Active metabolites NorpethidineNorpethidine
• CNS excitement, agitation seizures

FENTANYL
• Potency = 100 times MOSO4
• Rapid onset, short duration
• No histamine release
• Bradycardia
• Truncal rigidity

NALOXONE
• Pure opioid antagonis
• Dose 1 - 4 mcg/kg
• Duration 30 - 45 min
• Caution > close observe for – recurrent sedation/depression– increase sympathetic outflow– reverse analgesia + resp. depression