-
8/16/2019 Towe 2015
1/8
Adaptation of the Monetary Choice Questionnaire to
AccommodateExtreme Monetary Discounting in Cocaine Users
Sheri L. Towe and Andréa L. Hobkirk Duke University School of
Medicine
Daniel G. YeDuke University
Christina S. MeadeDuke University School of Medicine
Delay discounting, which refers to the phenomenon that rewards
decrease in subjective value as the delayassociated with their
receipt increases, is a paradigm that has been used extensively in
substance abuseresearch to understand impulsive decision making.
One common measure to assess delay discounting isthe Monetary
Choice Questionnaire (MCQ) developed by Kirby, Petry, and Bickel
(1999) . While theMCQ has great utility because of its simplicity
and brief administration time, it is possible that the MCQproduces
a ceiling effect in estimating delay discounting parameters in
highly impulsive individuals. Inthe present study, we adapted the
MCQ to attempt to address this ceiling effect by extending the
original
scale with 9 items, and we then compared scores on the original
MCQ with the extended MCQ in asample of active cocaine users. The
ceiling effect, while observed in the original MCQ scores for overa
quarter of the sample, was largely eliminated with the extended
scale. Highly impulsive participants,whose scores on the extended
scale exceeded the highest possible score on the original scale,
had higherlevels of sensation seeking compared to other
participants, but not trait impulsivity. The extended MCQmay be
useful in populations with high rates of impulsivity, where the
original measure may underes-timate discounting rates due to a
ceiling effect.
Keywords: impulsivity, delay discounting, cocaine dependence,
drug abuse
Delay discounting describes to the phenomenon that
rewardsdecrease in subjective value as the delay associated with
theirreceipt increases ( Mazur, 1987 ; Rachlin & Green, 1972
).Highly impulsive individuals exhibit high rates of delay
dis-counting in laboratory tasks, meaning that they show
preferencefor smaller, immediate rewards over larger, delayed
rewards.Research has demonstrated that higher rates of delay
discount-ing are associated with various health risk behaviors,
includingsubstance use, problematic gambling, and HIV
transmissionrisk behaviors ( Bickel & Marsch, 2001 ; Chesson et
al., 2006 ;Odum, Madden, Badger, & Bickel, 2000 ; Reynolds,
2006 ).
Delay discounting has been utilized extensively as a para-digm
for impulsivity in substance users, because increaseddelay
discounting theoretically reflects a fundamental decisionmaking
process present in substance using populations ( Reyn-olds, 2006 ).
While decision making is a complex process, partof the
phenomenology of substance dependence is thatsubstance-dependent
persons often make choices that contradicttheir stated goals. For
example, a person may commit to quit-ting smoking one day, only to
buy a pack of cigarettes thefollowing day. Delay discounting may be
a key factor in howthat decision is reached. For those with high
rates of delaydiscounting, more distal rewards, like achieving 30
days of sobriety or having funds to pay bills at the end of the
month, areunderweighted compared with immediate rewards, such as
sub-stance use.
Delay discounting has been shown to correlate with othermeasures
of impulsivity, including trait impulsivity and sensa-tion seeking
( Caswell, Bond, Duka, & Morgan, 2015 ; Koff &Lucas, 2011
). However, other research has shown weak orinconsistent
associations ( Mitchell, 1999 ; Vuchinich & Simp-son, 1998 ).
Research has demonstrated that higher delay dis-counting rates are
associated with addictive behaviors acrossmany different
substances, including nicotine, cocaine, opiates,and alcohol
compared with nondrug using controls ( MacKillopet al., 2011 ).
Cocaine users in particular have demonstratedgreater delay
discounting compared with nondrug users(Garcia-Rodriguez,
Secades-Villa, Weidberg, & Yoon, 2013 ;Heil, Johnson, Higgins,
& Bickel, 2006 ; Kirby & Petry, 2004 ).
This article was published Online First July 20, 2015.Sheri L.
Towe and Andréa L. Hobkirk, Department of Psychiatry &
Behavioral Sciences and Duke Global Health Institute, Duke
UniversitySchool of Medicine; Daniel G. Ye, Duke Global Health
Institute, DukeUniversity; Christina S. Meade, Department of
Psychiatry & BehavioralSciences and Duke Global Health
Institute, Duke University School of Medicine.
This study was funded by Grants K23-DA028660, F32-DA038519,
andT32-AI007392 from the United States National Institutes of
Health. We aregrateful to the UNC Center for AIDS Research
(P30-AI50410) for itsassistance with patient recruitment. The NIH
had no further role in studydesign, data collection, analysis and
interpretation of data, writing thereport, or in the decision to
submit the article for publication. We thank allthe men and women
who participated in this study.
Correspondence concerning this article should be addressed to
Sheri L.Towe, Duke University, Box 90519, Durham, NC 27708.
E-mail:[email protected]
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
Psychology of Addictive Behaviors © 2015 American Psychological
Association2015, Vol. 29, No. 4, 1048 –1055 0893-164X/15/$12.00
http://dx.doi.org/10.1037/adb0000101
1048
-
8/16/2019 Towe 2015
2/8
One measure that has been successfully used to assess
delaydiscounting in the laboratory is the Monetary Choice
Question-naire (MCQ; Kirby, Petry, & Bickel, 1999 ). The MCQ
asksparticipants to make 27 choices between smaller immediate
re-wards versus larger delayed rewards ( Kirby et al., 1999 ).
Byexamining the pattern of responses, one can infer a
participant’s
rate of delay discounting or “ k value.” Kirby, Petry, and
Bickel(1999) found that MCQ scores were correlated with other
mea-sures of impulsivity such as the Barratt Impulsiveness Scale,
andmean MCQ scores were higher among the substance-users com-pared
to nondrug using controls. Additionally, research has shownthat the
scores from the MCQ correlate highly with scores fromtraditional
measures of delay discounting, such as adjusting-amount procedures
( Epstein et al., 2003 ). Taken together, thisresearch suggests
that the MCQ is a valid means of measuringdelay discounting. Given
its simplicity and brevity, the MCQ is anideal measure to
administer in time-limited research settings whereuse of lengthier
behavioral tasks to assess delay discounting is notfeasible.
Highly impulsive persons may exhibit an extreme preference
forimmediate rewards. On the MCQ, these individuals select
theimmediate reward in all 27 items, resulting in a ceiling effect.
Inthese cases, the 27-item MCQ may underestimate the rate of
delaydiscounting. This ceiling effect has been observed in prior
researchusing the MCQ with substance users. For example, in one
sampleof alcohol and cocaine users, participants always selected
theimmediate reward in approximately 22% of the MCQs adminis-tered
(Black & Rosen, 2011 ). In addition, a ceiling effect has
beenobserved in other measures of delay discounting among
highlyimpulsive samples and has been cited as a contributing factor
tospurious correlations ( Johnson, Bickel, & Baker, 2007 ;
Petry &Casarella, 1999 ; Yoon et al., 2007 ). Thus, this
ceiling effect is of concern when working with populations who
exhibit high impul-
sivity, including stimulant users who engage in high rates of
riskybehaviors.
To address this ceiling effect, we adapted the MCQ to
accom-modate extreme discounting by adding nine items to extend
thescale. The purpose of this article is to describe the
adaptationprocess and to compare performance on the original
versusadapted versions of the MCQ in a sample of cocaine users.
Method
Participants and Procedures
MCQ data was collected as part of a larger study examining
theneurocognitive effects of HIV and cocaine use ( Meade,
Towe,Skalski, & Robertson, 2015 ). The community-based sample
in-cluded 101 adult cocaine users who met the following
inclusioncriteria: (a) 4 days of cocaine use in the past month or a
positiveurine drug screen for cocaine, (b) 1 year of regular
cocaine use,and (c) lifetime cocaine dependence. Alcohol,
marijuana, andnicotine use were permitted, and current alcohol and
marijuanadependence were permitted if cocaine dependence was the
princi-pal diagnosis. For other drugs, individuals were excluded
forlifetime abuse or dependence, history of regular use, any use in
thepast year, and/or a positive drug screen. Additional
exclusioncriteria were: English nonfluency or illiteracy; ninth
gradeeducation; serious neurological disorders (e.g., seizure
disorder,
cryptococcal meningitis) or severe head trauma; severe
mentalillness; pregnancy; physical disabilities impeding
participation(e.g., blindness); and impaired mental status.
Participants were recruited from the Raleigh-Durham, NC
areabetween May, 2010 and May, 2015 via advertisements in
localnewspapers and websites, flyers, and brochures at
community-
based organizations and clinics, and participant referrals. All
po-tential participants completed a structured telephone screen
toassess preliminary eligibility (e.g., HIV infection, drug use
his-tory), and interested individuals were then invited for a
compre-hensive in-person screening.
After providing written informed consent, participants weregiven
a breathalyzer test to ensure sobriety, and they provided aurine
sample for drug and pregnancy screening. Self-reportedHIV-positive
status was verified by medical record review, andHIV-negative
status was confirmed by an OraQuick © rapid HIVtest. Participants
then completed clinical interviews and question-naires. Eligible
participants returned on another day to complete aneurocognitive
assessment that included the MCQ, additional clin-ical interviews
and questionnaires, and another urine drug test. Allquestionnaires
were computerized using audio computer-assistedself-interview
(ACASI).
Participants were paid $35 for the screening visit, regardless
of eligibility, and $65 for the neurocognitive assessment. All
proce-dures were approved by the institutional review boards at
DukeUniversity Health System and University of North Carolina
atChapel Hill.
Measures
Original Monetary Choice Questionnaire (MCQ-27).Participants are
presented with choices between smaller, immedi-ate rewards and
larger, delayed rewards (e.g., “Would you prefer
$54 today or $80 in 30 days?;” Kirby et al., 1999 ). The
MCQ-27includes a fixed set of 27 items with immediate rewards
rangingfrom $11–$78 and delayed rewards ranging from $25–$85 with
adelay of 7–186 days. Delayed rewards are grouped into
threecategories based on size, with nine items per category:
small($25–$35), medium ($50–$60), and large ($75–$85).
As described by Kirby et al. (1999) , participants’
hyperbolicdiscount parameter ( k value) is determined by fitting
data to thefollowing discount function equation: V immediate V
delayed /(1 k D), in which V is the reward value in dollars and D
is delay indays (Mazur, 1984 ). Values of k range from 0.00016 to
0.25 for theMCQ-27, with higher values indicating a greater
preference forsmaller, immediate rewards over larger, delayed
rewards. Eachpossible k value increases by an order of
approximately 2.5,resulting in a logarithmic scale. K values are
estimated by takingthe geometric midpoint between the discount
rates associated witheach item and then examining the participant’s
pattern of re-sponses across trials to determine which k value is
most consistentwith the response pattern. By examining the pattern
of responses inthis way, one can infer a participant’s point of
indifference be-tween delayed and immediate rewards. To determine
the mostconsistent value, the proportion of a participant’s choices
that areconsistent with each k value is calculated. The k value
that yieldsthe highest proportion is the value assigned to the
participant. If two or more values have the same proportion, the
participant’sassigned k value is the geometric mean of those
values. Because
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
1049ADAPTATION OF THE MCQ FOR EXTREME DISCOUNTING
-
8/16/2019 Towe 2015
3/8
raw k values tend to be highly skewed, k values are
normalizedusing the natural logarithm transformation. K values are
alsoranked from 1 to 10. Rank 1 and Rank 10 represent the lowest
andhighest possible k values, respectively (e.g., when a
participantselects all delayed rewards or all immediate rewards
across trials),and Ranks 2 through 9 are assigned to the ranges of
discount rates
between items (e.g., values between 0.00016 to 0.00040 wereRank
2).Extended Monetary Choice Questionnaire (MCQ-36). To
expand the MCQ-27, nine items with higher associated k values
wereadded. Three new items were added to each category (small,
medium,large), resulting in 12 items per category and a total of 36
items for theMCQ-36. Additional k values for the extended scale
were computedby continuing the logarithmic scale of the original
MCQ-27, resultingin new k values of 0.625, 1.5625, and 3.90625. The
new itemsincluded delay periods lasting 1–7 days and utilized the
same threedelayed rewards as the other items in the category. The
immediatereward for each additional item was calculated based on
the standarddiscount function equation, resulting in immediate
rewards for thesenew items ranging from $5–$17. Dollar amounts were
rounded to the
nearest whole dollar, and then the exact k for that dollar
amount wascalculated with the formula. This resulted in k values
for the MCQ-36ranging from 0.00016 to 4.00. K values were also
natural log trans-formed and ranked for the MCQ-36, with ranks
ranging from 1 to 13.Table 1 shows the items included in the MCQ-36
and their calculatedk values.
The MCQ-36 was computerized using ePrime (PsychologySoftware
Tools, Inc., http://www.pstnet.com ). Choices were pre-sented in
random order, and participants indicated their responseusing a
computer mouse. Participants completed the full MCQ-36,and then
scores were generated for the original MCQ-27 and theextended
MCQ-36. Participants were told that all rewards werehypothetical,
and participants did not receive any money based ontheir
performance on the task.
Barratt Impulsiveness Scale—version 11 (BIS-11). At
theneurocognitive assessment, participants completed the
BIS-11(Patton, Stanford, & Barratt, 1995 ), which is one of the
oldest andmost widely used self-report measures of trait
impulsivity ( Stan-ford et al., 2009 ). The BIS-11 includes 30
items that describecommon impulsive or nonimpulsive behaviors and
preferences.
Table 1 Items in the Extended Monetary Choice Questionnaire
(MCQ-36)
Reward size Amount today Amount later Delay in days Calculated k
valuea
Small 34 35 186 0.00016Small 28 30 179 0.00040Small 22 25 136
0.00100Small 25 30 80 0.00250Small 19 25 53 0.00596Small 24 35 29
0.01580Small 14 25 19 0.04135Small 15 35 13 0.10256
Small 11 30 7 0.24675Small b 6 25 5 0.63333Small b 5 30 3
1.66667Small b 7 35 1 4.00000Medium 54 55 117 0.00016Medium 47 50
160 0.00040Medium 54 60 111 0.00100Medium 49 60 89 0.00252Medium 40
55 62 0.00605Medium 34 50 30 0.01569Medium 27 50 21 0.04056Medium
25 60 14 0.10000Medium 20 55 7 0.25000Medium b 12 50 5
0.63333Medium b 13 55 2 1.61538Medium b 12 60 1 4.00000Large 78 80
162 0.00016Large 80 85 157 0.00040Large 67 75 119 0.00100Large 69
85 91 0.00255Large 55 75 61 0.00596Large 54 80 30 0.01605Large 41
75 20 0.04146Large 33 80 14 0.10173Large 31 85 7 0.24885Large b 17
80 6 0.61765Large b 13 75 3 1.58974Large b 17 85 1 4.00000
a Exact values calculated using the standard discount function
equation, V immediate Vdelayed /(1 k D), in whichk represents the k
value, V is the reward value in dollars and D is delay in days. b
Item added to the MCQ-36that was not included in the MCQ-27.
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
1050 TOWE, HOBKIRK, YE, AND MEADE
-
8/16/2019 Towe 2015
4/8
Participants rate each items using a 4-point scale (
rarely/never ,occasionally , often , almost always/always ), and
higher scores in-dicate greater impulsiveness. All 30 items are
summed to yield atotal score, ranging from 30 to 120, and there are
six subscalesbased on first-order factors determined by a principal
componentanalysis ( Patton et al., 1995). The six subscales are
attention,
motor impulsiveness, self-control, cognitive complexity,
persever-ance, and cognitive instability.Sensation Seeking
Scale—version V (SSS-V). Participants
also completed the SSS-V ( Zuckerman, 1994 ; Zuckerman,
Eysenck,& Eysenck, 1978 ). In this 40-item, forced-choice
questionnaire, par-ticipants choose which of two statements best
applies to them. Thisinventory was developed to measure individual
differences in stimu-lation and arousal needs and is thought to
correlate with impulsivity.Reliability and construct validity for
this instrument has been well-established ( Zuckerman, 1994 ;
Zuckerman et al., 1978 ). Each state-ment is scored as either 0 or
1, and then items are summed to createa total score, ranging from 0
to 40. In addition to a total score, theSSS-V produces four
subscales that represent different dimensions of sensation seeking:
thrill and adventure seeking, experience seeking,disinhibition, and
boredom susceptibility.
Other measures. Demographic characteristics and detailed
as-sessments of substance use were completed at the screening
visit.Interviews included Module E of the Structured Clinical
Interview for DSM–IV–TR to assess for lifetime cocaine dependence
and othersubstance use disorders ( First, Spitzer, Gibbon, &
Williams, 1996 )and the Addiction Severity Index-Lite to assess
lifetime substance useand associated impairments ( McLellan et al.,
1992 ). Frequency of substance use in the past 30 days was assessed
using timeline follow-back methodology ( Robinson, Sobell, Sobell,
& Leo, 2014 ; Sobell &Sobell, 1996 ). A urine toxicology
screen for cocaine, cannabis, am-phetamine, methamphetamine,
oxycodone, methadone, other opioids(including heroin),
benzodiazepines, and barbiturates was used to
corroborate self-report. Premorbid verbal IQ was estimated using
theWechsler Test of Adult Reading (WTAR), in which participants
read50 words aloud that have atypical grapheme to phoneme
translations(Wechsler, 2001 ). Finally, participants completed a
computerizedsurvey that assessed demographics.
Participants completed the Brief Symptom Inventory 18 (BSI-18)at
the neurocognitive assessment. The BSI-18 is an 18-item
question-naire which assesses psychological distress. Participants
rate theirlevel of distress associated with 18 symptoms over the
past week using a 5-point Likert scale (0 not at all to 4 extremely
;Derogatis, 1993 ). An overall score is created by calculating the
meanof all 18 items. The HIV Risk Behavior Scale (HRBS), a brief
interview, was also completed at the neurocognitive assessment.
TheHRBS, a well-validated measure, assesses frequency of drug risk
behaviors (six items) and sex risk behaviors (six items) in the
past 30days (Darke, Hall, Heather, Ward, & Wodak, 1991 ). For
the HRBS,items are summed to create a total score.
Quality Assurance Procedures
All MCQ data were evaluated to ensure that participants
respondedin a consistent manner and appeared to understand the
task. Withineach category of delayed rewards (small, medium,
large), consistencywas evaluated by examining the highest
proportion of consistentchoices. Cases where ties resulted (e.g.,
two or more k values haveequally high proportions) were considered
indicative of potentially
inconsistent responding because a tie indicates that multiple k
valuesare equally likely to represent a participant’s true point of
indifference.While ties are generally handled by taking the
geometric mean of thek values, this method has potential for bias
when the pattern of responding is inconsistent. Therefore, we
established more rigorousstandardized criteria to evaluate when
ties result in k value estimates
that are potentially not valid. The k value within a category
wasexcluded if either of the following criteria were met: (a) there
was atie for the highest proportion between two k values and those
k valueswere separated by more than one other k value, or (b) there
was a tiebetween three or more k values for the highest proportion.
This firstcriterion was selected because the geometric mean of two
tied k values which are separated by only one other k value likely
doesclosely approximate a participant’s actual point of
indifference, butthe geometric mean of two highly discrepant k
values (i.e., separatedby more than one other k value) may not
provide as accurate anapproximation. For example, responses in the
large category for oneparticipant resulted in a two-way tie between
k values of Rank 6 andRank 10, and a geometric mean between these
two values wouldresult in a k value of Rank 8. If one of these
responses was an erroror mistake by the participant (due to lack of
comprehension orresponse imputation error), a Rank of 8 would not
be as closelyrepresentative of the participant’s actual point of
indifference. Thesecond criterion was selected because three- and
four-way ties gen-erally result in very low proportions. For
example, responses in thesmall reward category for one case
resulted in a four-way tie, witheach k value having a proportion of
0.58. When no exclusion rule wasmet, the k values within each
category were considered valid.
Cases were also evaluated for overall consistency. Cases
weremarked as overall inconsistent when either: (a) k value
proportionswere less than or equal to 0.80 in at least two
categories, (b) propor-tions in all three categories resulted in
ties, or (c) k values across twoor more categories were excluded
during scoring. These criteria were
selected because they each indicate that inconsistent responding
oc-curred across two or more reward categories. When a case
wasmarked as overall inconsistent, all k values for that case were
ex-cluded.
Using these procedures, two cases (2%) were marked as
highlyinconsistent overall and excluded from analysis, resulting in
99 caseswith valid MCQ data. In the individual reward categories
for theremaining 99 cases, no cases were marked as invalid in
small, onecase was marked as invalid in medium, and two cases were
marked asinvalid in large. For those cases, that category value was
consideredinvalid, but the other two categories were marked as
valid andtherefore the case was retained for analysis.
Data Analysis PlanQuantitative analysis was conducted using SPSS
21.0.0
(SPSS Inc., Chicago, IL). Descriptive statistics were used
tocharacterize the sample and determine the geometric mean forthe
raw k value, mean ln k value, mean rank value, and the totalnumber
of cases with the maximum score for both the MCQ-27and MCQ-36.
Participants whose k value on the MCQ-36exceeded the maximum
possible k value of 0.25 on the MCQ-27were classified as extreme
responders. Independent sample t tests and chi-squared tests were
conducted to identify differ-ences in demographic and other
relevant variables across ex-treme responders and nonextreme
responders. Variables iden-
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
1051ADAPTATION OF THE MCQ FOR EXTREME DISCOUNTING
-
8/16/2019 Towe 2015
5/8
tified as significantly different between groups and
relevantdemographic characteristics (age, race, gender, and years
of education) were included as covariates in the remaining
anal-yses. Univariate analyses of covariance (ANCOVAs) were
per-formed to examine differences between extreme versus
nonex-treme responders on the BIS, SSS, and other relevant
variables.
Results
Participant Characteristics
The majority of participants were male (66%) and AfricanAmerican
(92%). Participants were 46.29 years old on average(SD 8.46) and
49% of the sample was HIV-positive. Approx-imately 24% of the
sample identified as gay, lesbian, or bisex-ual. Participants
reported 12.24 years of education on average(SD 2.40) and 84%
reported being unemployed. Participantshad used cocaine on average
10.50 of the past 30 days ( SD 7.64) and reported a mean of 17.80
years of regular cocaine use(SD 7.48). The vast majority (88%)
reported smoking as theirusual route of cocaine administration, and
85% of the sampletested positive for cocaine in a urine drug screen
completed onthe day the MCQ was administered.
MCQ-27 and MCQ-36 Descriptive Characteristics
Table 2 presents geometric means of raw k values, mean ln k
values, and mean rank values for the MCQ-27 and the MCQ-36overall
and within each reward category. With the extendedscale, the MCQ-36
produced higher k values than the MCQ-27overall and across each
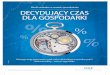
category. Figure 1 shows the number of participants with each rank
value in the MCQ-36. A total of 26participants (26%) were assigned
a k value of 0.25 in either
their overall mean or within at least one individual reward
sizecategory on the MCQ-36. Seventeen participants (17%)
wereassigned a k value of 0.25 for their overall mean k
value.Eighteen participants (18%) received a k value of 0.25 in
thesmall category, 15 (15%) in medium, and 16 (16%) in large.
Atotal of four participants (4%) were assigned the maximumpossible
k value of 4.00 in either their overall mean or within atleast one
individual reward size category. Two participants(2%) were assigned
the maximum k value of 4.00 for theiroverall mean, with two
participants (2%) receiving the maxi-mum value in the small
category, two (2%) in the mediumcategory, and four (4%) in the
large category.
Comparison of Extreme Responders to NonextremeResponders
We compared the 26 extreme responders to the 73 nonex-treme
responders on other participant and substance use char-acteristics
(e.g., occupational status, days of cocaine use) to
identify other potential control variables. A significantly
higherproportion of nonextreme responders (89%) were
unemployedcompared to extreme responders (69%) for occupational
status,
2 (1, N 99) 5.55, p .018. There was also a significantdifference
between groups on sexual orientation, 2 (1, N 99) 3.88, p .049,
such that a larger proportion (39%) of extreme responders
identified as gay, lesbian, or bisexual com-pared to nonextreme
responders (19%). There were no othersignificant differences
between groups. Therefore, in additionto age, race, gender, and
years of education, occupational statusand sexual orientation were
included as covariates in the sub-sequent ANCOVAs.
Table 3 presents the adjusted means and F values for eachANCOVA.
Several group differences were apparent on theSSS-V, with extreme
responders having higher scores overalland on the experience
seeking and disinhibition subscales. Onthe BIS-11, groups did not
significantly differ across the total orsubscale scores. Groups
also did not differ on premorbid verbalIQ, HRBS score, or BSI total
score. To reduce the risk of a TypeI error due to multiple
comparisons, we applied a familywiseBonferroni adjustment to the
significance level for theseANCOVAs so that significance levels
were set at p .003. Noresults were significant using this adjusted
significance level.Traditional p values (i.e., p .05, 0.01) are
noted in Table 3 .
Discussion
In this sample of active cocaine users, the modified
MCQ-36appeared to be successful in reducing a ceiling effect on k
scores compared with the MCQ-27. There was a clear ceilingeffect
using the original MCQ-27 items, with over a quarter of
participants producing k values that exceeded the maximumpossible k
value. This ceiling effect was reduced substantiallywith the MCQ-36
to only four participants receiving the max-imum possible k value.
Based on these results, use of theextended MCQ-36 may be warranted
in populations with highrates of impulsivity, such as
out-of-treatment cocaine users, inorder to get a more accurate
estimate of discounting parameters.
Table 2 Average K Values, ln K Values, and Ranks for the
Original Monetary Choice Questionnaire (MCQ-27) and Extended
MonetaryChoice Questionnaire (MCQ-36)
Reward size
K value geo. mean (95% CI) a ln k value M (SD) Ranked k value M
(SD)
MCQ-27 MCQ-36 MCQ-27 MCQ-36 MCQ-27 MCQ-36
Small N 99 0.06 [0.05, 0.08] 0.08 [0.05, 0.10] 2.76 (1.34) 2.57
(1.62) 8.08 (1.58) 8.21 (1.81)Medium N 98 0.05 [0.04, 0.06] 0.06
[0.04, 0.08] 3.00 (1.35) 2.84 (1.61) 7.82 (1.58) 7.93 (1.80)Large N
97 0.04 [0.03, 0.05] 0.05 [0.03, 0.07] 3.20 (1.38) 2.97 (1.80) 7.59
(1.63) 7.78 (2.02)Overall mean N 99 0.05 [0.04, 0.06] 0.06 [0.04,
0.08] 2.98 (1.20) 2.78 (1.51) 7.84 (1.43) 7.99 (1.69)a geo. mean
geometric mean of raw k values, 95% CI 95% confidence intervals for
each geometric mean.
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
1052 TOWE, HOBKIRK, YE, AND MEADE
-
8/16/2019 Towe 2015
6/8
There were some notable differences between extreme re-sponders
and nonextreme responders on the SSS, though thesewere not
statistically significant after correcting for multiplecomparisons
using the Bonferroni adjustment. Overall, extremeresponders had
higher levels of sensation seeking comparedwith nonextreme
responders, and showed particularly high lev-els of sensation
seeking in disinhibition and experience seeking.Disinhibition
reflects both social and sexual disinhibition that isexpressed in
substance-use behaviors and variety in sexualpartners ( Zuckerman
et al., 1978 ). Experience seeking repre-sents the pursuit of new
sensations and experiences through themind and senses, and
activities such as travel and a noncon-forming lifestyle (
Zuckerman et al., 1978 ).
There were few differences between extreme responders
andnonextreme responders on cocaine use, trait impulsivity, andmany
other participant characteristics. The lack of differenceson
cocaine use variables is very likely the result of
stricteligibility criteria for the sample related to frequency
andseverity of cocaine use. Use of these strict criteria resulted
in a
relatively homogeneous sample in terms of substance use
char-acteristics.
The findings from this study have important implications
formeasuring delay discounting in highly impulsive populations.In
our results, scores based on the MCQ-27 yielded k values
thatunderestimated delay discounting due to a ceiling effect for
alarge proportion of our participants. Other studies using
the27-item MCQ with substance users reported mean k valuessimilar
to those in the current study sample ( Gonzalez et al.,2012 ; Kirby
& Petry, 2004 ). Therefore, it is possible that othershave
found a similar ceiling effect, although it has not beenreported.
The MCQ-36 represents a way to assess a wider rangeof delay
discounting in highly impulsive individuals that cap-tures
variability that would otherwise be missed by the shorterMCQ-27.
Furthermore, while yielding a potentially more accu-rate estimate
of delay discounting, the addition of nine items inthe MCQ-36 did
not substantially increase the length of time of administration.
Future research might compare this extendedMCQ against other
validated measures of delay discounting.
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13
Ranked k values
Overall Mean
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13
Ranked k values
Large
0
5
10
15
20
25
30
35
1 2 3 4 5 6 7 8 9 10 11 12 13
Ranked k values
Medium
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13
Ranked k values
Small
Figure 1. Histograms of ranked k -values across reward
categories and by overall mean for the MCQ-36.Shaded bars represent
ranks from the original MCQ-27 items. Additional ranks from the
extended k value scaleincluded in the MCQ-36 are unshaded. MCQ-27
Original Monetary Choice Questionnaire; MCQ-36 Extended Monetary
Choice Questionnaire.
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
1053ADAPTATION OF THE MCQ FOR EXTREME DISCOUNTING
-
8/16/2019 Towe 2015
7/8
Additionally, future research could examine whether scores onthe
MCQ-36 are more predictive of risk behaviors.
ReferencesBickel, W. K., & Marsch, L. A. (2001). Toward a
behavioral economic
understanding of drug dependence: Delay discounting processes.
Addic-tion, 96, 73–86.
http://dx.doi.org/10.1046/j.1360-0443.2001.961736.x
Black, A. C., & Rosen, M. I. (2011). A money
management-based sub-stance use treatment increases valuation of
future rewards. Addictive Behaviors, 36, 125–128.
http://dx.doi.org/10.1016/j.addbeh.2010.08.014
Caswell, A. J., Bond, R., Duka, T., & Morgan, M. J. (2015).
Furtherevidence of the heterogeneous nature of impulsivity.
Personality and Individual Differences, 76, 68–74.
http://dx.doi.org/10.1016/j.paid.2014.11.059
Chesson, H. W., Leichliter, J. S., Zimet, G. D., Rosenthal, S.
L., Bernstein,D. I., & Fife, K. H. (2006). Discount rates and
risky sexual behaviorsamong teenagers and young adults. Journal of
Risk and Uncertainty, 32,217–230.
http://dx.doi.org/10.1007/s11166-006-9520-1
Darke, S., Hall, W., Heather, N., Ward, J., & Wodak, A.
(1991). Thereliability and validity of a scale to measure HIV
risk-taking behaviouramong intravenous drug users. AIDS, 5,
181–185. http://dx.doi.org/ 10.1097/00002030-199102000-00008
Derogatis, L. R. (1993). Brief symptom inventory:
Administration, scoring,and procedures manual (3rd ed.).
Minneapolis, MN: National ComputerSystems, Inc.
Epstein, L. H., Richards, J. B., Saad, F. G., Paluch, R. A.,
Roemmich, J. N.,& Lerman, C. (2003). Comparison between two
measures of delaydiscounting in smokers. Experimental and Clinical
Psychopharmacol-ogy, 11, 131–138.
http://dx.doi.org/10.1037/1064-1297.11.2.131
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B.
W. (1996).Structured clinical interview for DSM–IV Axis I
disorders, research
version, patient/non-patient edition . New York, NY: Biometrics
Re-search, New York State Psychiatric Institute.
García-Rodríguez, O., Secades-Villa, R., Weidberg, S., &
Yoon, J. H.(2013). A systematic assessment of delay discounting in
relation to
cocaine and nicotine dependence. Behavioural Processes, 99,
100–105.http://dx.doi.org/10.1016/j.beproc.2013.07.007
Gonzalez, R., Schuster, R. M., Mermelstein, R. J., Vassileva,
J., Martin,E. M., & Diviak, K. R. (2012). Performance of young
adult cannabisusers on neurocognitive measures of impulsive
behavior and their rela-tionship to symptoms of cannabis use
disorders. Journal of Clinical and Experimental Neuropsychology,
34, 962–976. http://dx.doi.org/10.1080/ 13803395.2012.703642
Heil, S. H., Johnson, M. W., Higgins, S. T., & Bickel, W. K.
(2006).Delay discounting in currently using and currently abstinent
cocaine-dependent outpatients and non-drug-using matched controls.
Addic-tive Behaviors, 31, 1290–1294.
http://dx.doi.org/10.1016/j.addbeh.2005.09.005
Johnson, M. W., Bickel, W. K., & Baker, F. (2007). Moderate
drug use anddelay discounting: A comparison of heavy, light, and
never smokers. Experimental and Clinical Psychopharmacology, 15,
187–194. http://dx.doi.org/10.1037/1064-1297.15.2.187
Kirby, K. N., & Petry, N. M. (2004). Heroin and cocaine
abusers havehigher discount rates for delayed rewards than
alcoholics or non-drug-using controls. Addiction, 99, 461–471.
http://dx.doi.org/10.1111/j.1360-0443.2003.00669.x
Kirby, K. N., Petry, N. M., & Bickel, W. K. (1999). Heroin
addicts havehigher discount rates for delayed rewards than
non-drug-using controls. Journal of Experimental Psychology:
General, 128, 78–87.
http://dx.doi.org/10.1037/0096-3445.128.1.78
Koff, E., & Lucas, M. (2011). Mood moderates the
relationship betweenimpulsiveness and delay discounting.
Personality and Individual Differ-ences, 50, 1018–1022.
http://dx.doi.org/10.1016/j.paid.2011.01.016
Table 3Comparison of Extreme Responders to Nonextreme Responders
Using ANCOVA
Adjusted means
Nonextreme responders Extreme respondersMeasure ( N 73) ( N 26)
F value
Barratt Impulsiveness ScaleBIS-11 total score 65.18 65.52 F (1,
91) .02Self-control 14.69 15.60 F (1, 91) 1.40Motor impulsiveness
14.51 13.71 F (1, 91) 1.40Attention 9.93 10.28 F (1, 91)
.29Cognitive instability 4.66 5.04 F (1, 91) 1.04Cognitive
complexity 13.16 13.12 F (1, 91) .01Perseverance 8.23 7.78 F (1,
91) .87
Sensation Seeking ScaleSSS-V total score 14.22 17.04 F (1, 91)
5.14Thrill and adventure seeking 3.23 3.52 F (1, 91) .24Experience
seeking 4.62 5.56 F (1, 91) 4.21Disinhibition 4.14 5.48 F (1, 91)
8.27Boredom susceptibility 2.23 2.47 F (1, 91) .37
Estimated premorbid verbal IQ 86.83 82.71 F (1, 90) 2.04HRBS sex
composite 3.37 4.34 F (1, 91) 1.19
BSI total score 0.49 0.53 F (1, 91) .11 Note. The covariates
included were age, race, gender, years of education, sexual
orientation, and occupationalstatus. Means presented represent the
adjusted means after controlling for all covariates in the ANCOVA.
BIS-11point scales: total, 30 –120; self-control, 6–24; motor
impulsiveness, 7–28; attention, 5–20; cognitive instability,3–12;
cognitive complexity, 5–20; perseverance, 4–16. SSS-V point scales:
total, 0–40; all subscales, 0–10.ANCOVA analysis of covariance;
SSS-V Sensation Seeking Scale - version V; HRBS HIV Risk Behavior
Scale; BSI Brief Symptom Inventory. p .05. p .01.
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
1054 TOWE, HOBKIRK, YE, AND MEADE
-
8/16/2019 Towe 2015
8/8
MacKillop, J., Amlung, M. T., Few, L. R., Ray, L. A., Sweet, L.
H., &Munafò, M. R. (2011). Delayed reward discounting and
addictive be-havior: A meta-analysis. Psychopharmacology, 216,
305–321. http://dx.doi.org/10.1007/s00213-011-2229-0
Mazur, J. E. (1984). Tests of an equivalence rule for fixed and
variablereinforcer delays. Journal of Experimental Psychology:
Animal Behav-ior Processes, 10, 426–436.
http://dx.doi.org/10.1037/0097-7403.10.4.426
Mazur, J. E. (1987). An adjusting procedure for studying delayed
rein-forcement. In M. L. Commons, J. E. Mazur, J. A. Nevin, &
H. Rachlin(Eds.), The effect of delay and of intervening events on
reinforcement value (pp. 55–73). Hillsdale, NJ: Erlbaum, Inc.
McLellan, A. T., Kushner, H., Metzger, D., Peters, R., Smith,
I., Grissom,G., . . . Argeriou, M. (1992). The fifth edition of the
Addiction SeverityIndex. Journal of Substance Abuse Treatment, 9,
199–213.
Meade, C. S., Towe, S. L., Skalski, L. M., & Robertson, K.
R. (2015).Independent effects of HIV infection and cocaine
dependence on neu-rocognitive impairment in a community sample
living in the southernUnited States. Drug and Alcohol Dependence,
149, 128–135.
http://dx.doi.org/10.1016/j.drugalcdep.2015.01.034
Mitchell, S. H. (1999). Measures of impulsivity in cigarette
smokers andnon-smokers. Psychopharmacology, 146, 455–464.
http://dx.doi.org/ 10.1007/PL00005491
Odum, A. L., Madden, G. J., Badger, G. J., & Bickel, W. K.
(2000). Needlesharing in opioid-dependent outpatients:
Psychological processes under-lying risk. Drug and Alcohol
Dependence, 60, 259–266.
http://dx.doi.org/10.1016/S0376-8716(00)00111-3
Patton, J. H., Stanford, M. S., & Barratt, E. S. (1995).
Factor structure of the Barratt impulsiveness scale. Journal of
Clinical Psychology, 51,768–774.
http://dx.doi.org/10.1002/1097-4679(199511)51:6
768::AID-JCLP2270510607 3.0.CO;2-1
Petry, N. M., & Casarella, T. (1999). Excessive discounting
of delayedrewards in substance abusers with gambling problems. Drug
and Alco-hol Dependence, 56, 25–32.
http://dx.doi.org/10.1016/S0376-8716(99)00010-1
Rachlin, H., & Green, L. (1972). Commitment, choice and
self-control. Journal of the Experimental Analysis of Behavior, 17,
15–22. http://dx.doi.org/10.1901/jeab.1972.17-15
Reynolds, B. (2006). A review of delay-discounting research with
humans:Relations to drug use and gambling. Behavioural
Pharmacology, 17,651–667.
http://dx.doi.org/10.1097/FBP.0b013e3280115f99
Robinson, S. M., Sobell, L. C., Sobell, M. B., & Leo, G. I.
(2014).Reliability of the Timeline Followback for cocaine,
cannabis, and cig-arette use. Psychology of Addictive Behaviors,
28, 154–162. http://dx.doi.org/10.1037/a0030992
Sobell, L. C., & Sobell, M. B. (1996). Timeline follow-back
user’s guide: A calendar method for assessing alcohol and drug use
. Toronto, Canada:Addiction Research Foundation.
Stanford, M. S., Mathias, C. W., Dougherty, D. M., Lake, S. L.,
Anderson,N. E., & Patton, J. H. (2009). Fifty years of the
Barratt ImpulsivenessScale: An update and review. Personality and
Individual Differences,47, 385–395.
http://dx.doi.org/10.1016/j.paid.2009.04.008
Vuchinich, R. E., & Simpson, C. A. (1998). Hyperbolic
temporal discount-ing in social drinkers and problem drinkers.
Experimental and ClinicalPsychopharmacology, 6, 292–305.
http://dx.doi.org/10.1037/1064-1297.6.3.292
Wechsler, D. (2001). Wechsler Test of Adult Reading (WTAR)
manual . SanAntonio, TX: Harcourt Assessment.
Yoon, J. H., Higgins, S. T., Heil, S. H., Sugarbaker, R. J.,
Thomas, C. S.,& Badger, G. J. (2007). Delay discounting
predicts postpartum relapse tocigarette smoking among pregnant
women. Experimental and ClinicalPsychopharmacology, 15, 176–186.
http://dx.doi.org/10.1037/1064-1297.15.2.186
Zuckerman, M. (1994). Behavioral expressions and biosocial bases
of sensation seeking . New York, NY: Cambridge University
Press.
Zuckerman, M., Eysenck, S., & Eysenck, H. J. (1978).
Sensation seekingin England and America: Cross-cultural, age, and
sex comparisons. Journal of Consulting and Clinical Psychology, 46,
139–149. http://dx.doi.org/10.1037/0022-006X.46.1.139
Received April 8, 2015Revision received May 8, 2015
Accepted May 9, 2015
Thisarticleisintendedsolelyforthepersonaluseoftheindividualuserandisnottobedisseminatedbroadly.
1055ADAPTATION OF THE MCQ FOR EXTREME DISCOUNTING